
Accuracy of Intraoral Scanner for Recording Completely Edentulous Arches—A Systematic Review

 , and
, and
Abstract
:1. Introduction
2. Material and Methods
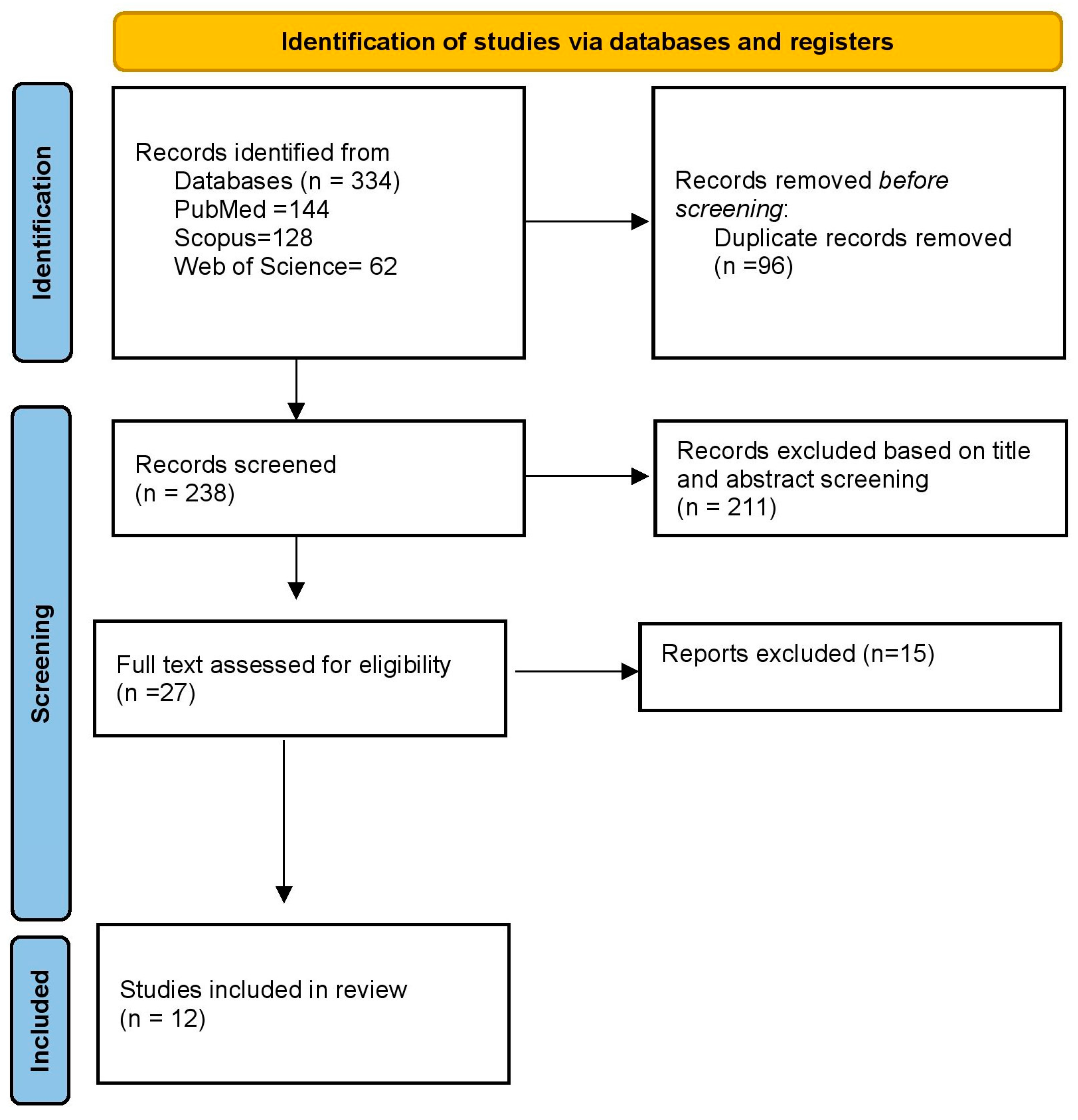
2.1. Study Selection
2.2. Risk of Bias Assessment
2.3. Data Extraction
3. Results
3.1. Risk of Bias Assessment
3.2. Characteristics of Clinical Studies
3.3. Characteristics of In Vitro Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jacobson, T.E.; Krol, A.J. A Contemporary Review of the Factors Involved in Complete Denture Retention, Stability, and Support. Part I: Retention. J. Prosthet. Dent. 1983, 49, 5–15. [Google Scholar] [CrossRef]
- Addison, P.I. Application of Mucostatic Principles to Full Denture Construction. N. Y. J. Dent. 1947, 17, 135–145. [Google Scholar] [PubMed]
- Rao, S.; Chowdhary, R.; Mahoorkar, S. A Systematic Review of Impression Technique for Conventional Complete Denture. J. Indian. Prosthodont. Soc. 2010, 10, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Devan, M.M. Basic Principles in Impression Making. 1952. J. Prosthet. Dent. 2005, 93, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Beresin, V.E.; Schiesser, F.J. The Neutral Zone in Complete Dentures. J. Prosthet. Dent. 1976, 36, 356–367. [Google Scholar] [CrossRef] [PubMed]
- Mehra, M.; Vahidi, F.; Berg, R.W. A Complete Denture Impression Technique Survey of Postdoctoral Prosthodontic Programs in the United States. J. Prosthodont. 2014, 23, 320–327. [Google Scholar] [CrossRef]
- Chaffee, N.R.; Cooper, L.F.; Felton, D.A. A Technique for Border Molding Edentulous Impressions Using Vinyl Polysiloxane Material. J. Prosthodont. 1999, 8, 129–134. [Google Scholar] [CrossRef]
- Giachetti, L.; Sarti, C.; Cinelli, F.; Russo, D.S. Accuracy of Digital Impressions in Fixed Prosthodontics: A Systematic Review of Clinical Studies. Int. J. Prosthodont. 2020, 33, 192–201. [Google Scholar] [CrossRef]
- Manisha, J.; Srivastava, G.; Das, S.S.; Tabarak, N.; Choudhury, G.K. Accuracy of Single-Unit Ceramic Crown Fabrication after Digital versus Conventional Impressions: A Systematic Review and Meta-Analysis. J. Indian Prosthodont. Soc. 2023, 23, 105–111. [Google Scholar]
- Ahlholm, P.; Sipilä, K.; Vallittu, P.; Jakonen, M.; Kotiranta, U. Digital Versus Conventional Impressions in Fixed Prosthodontics: A Review. J. Prosthodont. 2018, 27, 35–41. [Google Scholar] [CrossRef]
- Kawai, Y.; Muarakami, H.; Feine, J.S. Do Traditional Techniques Produce Better Conventional Complete Dentures than Simplified Techniques? A 10-Year Follow-up of a Randomized Clinical Trial. J. Dent. 2018, 74, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral Scanners in Dentistry: A Review of the Current Literature. BMC Oral. Health 2017, 17, 149. [Google Scholar] [CrossRef] [PubMed]
- Patzelt, S.B.M.; Vonau, S.; Stampf, S.; Att, W. Assessing the Feasibility and Accuracy of Digitizing Edentulous Jaws. J. Am. Dent. Assoc. 2013, 144, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Gan, N.; Xiong, Y.; Jiao, T. Accuracy of Intraoral Digital Impressions for Whole Upper Jaws, Including Full Dentitions and Palatal Soft Tissues. PLoS ONE 2016, 11, e0158800. [Google Scholar] [CrossRef]
- Fang, J.-H.; An, X.; Jeong, S.-M.; Choi, B.-H. Digital Intraoral Scanning Technique for Edentulous Jaws. J. Prosthet. Dent. 2018, 119, 733–735. [Google Scholar] [CrossRef]
- Lee, J.-H. Improved Digital Impressions of Edentulous Areas. J. Prosthet. Dent. 2017, 117, 448–449. [Google Scholar] [CrossRef]
- Goodacre, B.J.; Goodacre, C.J. Using Intraoral Scanning to Fabricate Complete Dentures: First Experiences. Int. J. Prosthodont. 2018, 31, 166–170. [Google Scholar] [CrossRef]
- Lo Russo, L.; Salamini, A. Single-Arch Digital Removable Complete Denture: A Workflow That Starts from the Intraoral Scan. J. Prosthet. Dent. 2018, 120, 20–24. [Google Scholar] [CrossRef]
- Goodacre, B.J.; Goodacre, C.J.; Baba, N.Z. Using Intraoral Scanning to Capture Complete Denture Impressions, Tooth Positions, and Centric Relation Records. Int. J. Prosthodont. 2018, 31, 377–381. [Google Scholar] [CrossRef]
- D’Arienzo, L.F.; D’Arienzo, A.; Borracchini, A. Comparison of the Suitability of Intra-Oral Scanning with Conventional Impression of Edentulous Maxilla in Vivo. A Preliminary Study. J. Osseointegration 2018, 10, 115–120. [Google Scholar]
- Chebib, N.; Kalberer, N.; Srinivasan, M.; Maniewicz, S.; Perneger, T.; Müller, F. Edentulous Jaw Impression Techniques: An in Vivo Comparison of Trueness. J. Prosthet. Dent. 2019, 121, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Park, C.; Yang, H.-S.; Lim, H.-P.; Yun, K.-D.; Ying, Z.; Park, S.-W. Comparison of Different Impression Techniques for Edentulous Jaws Using Three-Dimensional Analysis. J. Adv. Prosthodont. 2019, 11, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Lo Russo, L.; Caradonna, G.; Troiano, G.; Salamini, A.; Guida, L.; Ciavarella, D. Three-Dimensional Differences between Intraoral Scans and Conventional Impressions of Edentulous Jaws: A Clinical Study. J. Prosthet. Dent. 2020, 123, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Hack, G.; Liberman, L.; Vach, K.; Tchorz, J.P.; Kohal, R.J.; Patzelt, S.B.M. Computerized Optical Impression Making of Edentulous Jaws—An In Vivo Feasibility Study. J. Prosthodont. Res. 2020, 64, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Kalberer, N.; Chebib, N.; Wachter, W.; Lee, H.; Müller, F.; Srinivasan, M. In Silico Evaluation of the Peripheral and Inner Seals in Complete Denture Master Impressions Using a Custom-Developed 3D Software. Clin. Oral. Investig. 2021, 25, 125–132. [Google Scholar] [CrossRef]
- Chebib, N.; Imamura, Y.; El Osta, N.; Srinivasan, M.; Müller, F.; Maniewicz, S. Fit and Retention of Complete Denture Bases: Part II—Conventional Impressions versus Digital Scans: A Clinical Controlled Crossover Study. J. Prosthet. Dent. 2022. [Google Scholar] [CrossRef] [PubMed]
- Al Hamad, K.Q.; Al-Kaff, F.T. Trueness of Intraoral Scanning of Edentulous Arches: A Comparative Clinical Study. J. Prosthodont. 2023, 32, 26–31. [Google Scholar] [CrossRef]
- Braian, M.; Wennerberg, A. Trueness and Precision of 5 Intraoral Scanners for Scanning Edentulous and Dentate Complete-Arch Mandibular Casts: A Comparative in Vitro Study. J. Prosthet. Dent. 2019, 122, 129–136.e2. [Google Scholar] [CrossRef]
- Osnes, C.A.; Wu, J.H.; Venezia, P.; Ferrari, M.; Keeling, A.J. Full Arch Precision of Six Intraoral Scanners in Vitro. J. Prosthodont. Res. 2020, 64, 6–11. [Google Scholar] [CrossRef]
- Zarone, F.; Ruggiero, G.; Ferrari, M.; Mangano, F.; Joda, T.; Sorrentino, R. Comparison of Different Intraoral Scanning Techniques on the Completely Edentulous Maxilla: An in Vitro 3-Dimensional Comparative Analysis. J. Prosthet. Dent. 2020, 124, e1–e762. [Google Scholar] [CrossRef]
- Mennito, A.S.; Evans, Z.P.; Nash, J.; Bocklet, C.; Lauer Kelly, A.; Bacro, T.; Cayouette, M.; Ludlow, M.; Renne, W.G. Evaluation of the Trueness and Precision of Complete Arch Digital Impressions on a Human Maxilla Using Seven Different Intraoral Digital Impression Systems and a Laboratory Scanner. J. Esthet. Restor. Dent. 2019, 31, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Deferm, J.T.; Schreurs, R.; Baan, F.; Bruggink, R.; Merkx, M.A.W.; Xi, T.; Bergé, S.J.; Maal, T.J.J. Validation of 3D Documentation of Palatal Soft Tissue Shape, Color, and Irregularity with Intraoral Scanning. Clin. Oral. Investig. 2018, 22, 1303–1309. [Google Scholar] [CrossRef] [PubMed]
- Peroz, S.; Peroz, I.; Beuer, F.; Sterzenbach, G.; von Stein-Lausnitz, M. Digital versus Conventional Complete Dentures: A Randomized, Controlled, Blinded Study. J. Prosthet. Dent. 2022, 128, 956–963. [Google Scholar] [CrossRef] [PubMed]
- Tasaka, A.; Uekubo, Y.; Mitsui, T.; Kasahara, T.; Takanashi, T.; Homma, S.; Matsunaga, S.; Abe, S.; Yoshinari, M.; Yajima, Y.; et al. Applying Intraoral Scanner to Residual Ridge in Edentulous Regions: In Vitro Evaluation of Inter-Operator Validity to Confirm trueness. BMC Oral. Health 2019, 19, 264. [Google Scholar] [CrossRef]
- Schimmel, M.; Akino, N.; Srinivasan, M.; Wittneben, J.-G.; Yilmaz, B.; Abou-Ayash, S. Accuracy of Intraoral Scanning in Completely and Partially Edentulous Maxillary and Mandibular Jaws: An in Vitro Analysis. Clin. Oral. Investig. 2021, 25, 1839–1847. [Google Scholar] [CrossRef]
- Mai, H.Y.; Mai, H.-N.; Lee, C.-H.; Lee, K.-B.; Kim, S.-Y.; Lee, J.-M.; Lee, K.-W.; Lee, D.-H. Impact of Scanning Strategy on the Accuracy of Complete-Arch Intraoral Scans: A Preliminary Study on Segmental Scans and Merge Methods. J. Adv. Prosthodont. 2022, 14, 88–95. [Google Scholar] [CrossRef]
- Kontis, P.; Güth, J.-F.; Schubert, O.; Keul, C. Accuracy of Intraoral Scans of Edentulous Jaws with Different Generations of Intraoral Scanners Compared to Laboratory Scans. J. Adv. Prosthodont. 2021, 13, 316–326. [Google Scholar] [CrossRef]
- Ender, A.; Attin, T.; Mehl, A. In Vivo Precision of Conventional and Digital Methods of Obtaining Complete-Arch Dental Impressions. J. Prosthet. Dent. 2016, 115, 313–320. [Google Scholar] [CrossRef]
- Tao, C.; Zhao, Y.J.; Sun, Y.C.; Heng, M.D.; Xie, Q.F.; Pan, S.X. Accuracy of Intraoral Scanning of Edentulous Jaws with and without Resin Markers. Chin. J. Dent. Res. 2020, 23, 265–271. [Google Scholar]
- Stefanelli, L.V.; Franchina, A.; Pranno, A.; Pellegrino, G.; Ferri, A.; Pranno, N.; Di Carlo, S.; De Angelis, F. Use of Intraoral Scanners for Full Dental Arches: Could Different Strategies or Overlapping Software Affect Accuracy? Int. J. Environ. Res. Public Health 2021, 18, 9946. [Google Scholar] [CrossRef]
- Passos, L.; Meiga, S.; Brigagão, V.; Street, A. Impact of Different Scanning Strategies on the Accuracy of Two Current Intraoral Scanning Systems in Complete-Arch Impressions: An in Vitro Study. Int. J. Comput. Dent. 2019, 22, 307–319. [Google Scholar] [PubMed]
- Li, J.; Moon, H.S.; Kim, J.-H.; Yoon, H.-I.; Oh, K.C. Accuracy of Impression-Making Methods in Edentulous Arches: An in Vitro Study Encompassing Conventional and Digital Methods. J. Prosthet. Dent. 2021, 128, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Baghani, M.T.; Shayegh, S.S.; Johnston, W.M.; Shidfar, S.; Hakimaneh, S.M.R. In Vitro Evaluation of the Accuracy and Precision of Intraoral and Extraoral Complete-Arch Scans. J. Prosthet. Dent. 2021, 126, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Gutmacher, Z.; Kelly, A.; Renne, W.; Hoover, M.; Mennito, A.; Teich, S.; Cayouette, M.; Ludlow, M. Evaluation of the Accuracy of Multiple Digital Impression Systems on a Fully Edentulous Maxilla. Quintessence Int. 2021, 52, 488–495. [Google Scholar] [PubMed]
- Lo Russo, L.; Caradonna, G.; Salamini, A.; Guida, L. A single procedure for the registration of maxillo-mandibular relationships and alignment of intraoral scans of edentulous maxillary and mandibular arches. J. Prosthodont. Res. 2020, 64, 55–59. [Google Scholar] [CrossRef]
- Dong, J.; Zhang, F.-Y.; Wu, G.-H.; Zhang, W.; Yin, J. Measurement of Mucosal Thickness in Denture-Bearing Area of Edentulous Mandible. Chin. Med. J. 2015, 128, 342–347. [Google Scholar] [CrossRef]
- Jacob, H.B.; Wyatt, G.D.; Buschang, P.H. Reliability and Validity of Intraoral and Extraoral Scanners. Prog. Orthod. 2015, 16, 38. [Google Scholar] [CrossRef]


{kind=link}
| Focused Question | In Fully Edentulous Patients, What Is the Accuracy of IOS Compared to Conventional Impression Techniques in the Form of Trueness and Precision for Complete Dentures? | |
|---|---|---|
| PICO | Population | Fully edentulous patient (((edentulous arch) OR (edentulous jaw [MeSH Terms])) OR (jaw edentulous [MeSH Terms])) OR (edentulous ridge). |
| Intervention | Edentulous impression with an IOS ((((digital impression) OR (intraoral scanner)) OR (optical impression)) OR (digital scan)) OR (intraoral scan). | |
| Comparison | Conventional impression techniques (((dental impression technique [MeSH Terms]) OR (conventional impression)) OR (conventional technique)) OR (elastomers, silicone [MeSH Terms]). | |
| Outcome | Accuracy in the form of trueness and precision for complete dentures ((((data accuracy [MeSH Terms]) OR (accuracy)) OR (precision)) OR (trueness)) OR (3D comparison). | |
| Search Strategy | Pubmed | (((((edentulous arch) OR (edentulous jaw[MeSH Terms])) OR (jaw edentulous[MeSH Terms])) OR (edentulous ridge)) AND (((((digital impression) OR (intraoral scanner)) OR (optical impression)) OR (digital scan)) OR (intraoral scan))) AND ((((dental impression technique[MeSH Terms]) OR (conventional impression)) OR (conventional technique)) OR (elastomers, silicone[MeSH Terms]))) AND (((((data accuracy[MeSH Terms]) OR (accuracy)) OR (precision)) OR (trueness)) OR (3D comparison)). |
| Database Search | MEDLINE (PubMed), Scopus, and Web of Science (WOS). | |
| Criteria | D’Arienzo [20] | Chebib [21] | Jung [22] | Lo Russo [23] | Hack [24] | Kalberer [25] | Chebib [26] | Alhamad [27] | Patzelt [13] | Brian [28] | Osnes [29] | Zarone [30] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Was the range of the edentulous mucosa representative of what will be identified clinically? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 2. | Were criteria for selection clearly described? | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 |
| 3. | Control method likely to correctly classify the target condition | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 4. | The timelapse between the reference method and test method is short enough so the target tissue does not change | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 |
| 5. | Did the whole sample receive the verification? | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| 6. | Edentulous mucosa received the same control method regardless of the test method | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 7. | Was the control method independent of the test method? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 8. | Test method execution described in detail | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 9. | Execution of the control method described in detail | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 10. | Test results deciphered without knowledge of the control method results | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 11. | Control method results deciphered without knowledge of the test method results | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 12. | Intermediate test results reported | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| 13. | Withdrawal from the study explained | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| Total | 12 | 10 | 10 | 9 | 12 | 10 | 11 | 11 | 10 | 9 | 10 | 10 |
| Author | Reason for Exclusion |
|---|---|
| Mennito et al. [31] | Study performed on cadaveric maxilla. |
| Gan et al. [14] | A completely dentulous arch was studied. |
| Deferm et al. [32] | Interobserver validity was studied. |
| Peroz et al. [33] | Oral-health-related quality of life was evaluated. |
| Tasaka et al. [34] | Interoperator validity was assessed. |
| Schimmel et al. [35] | Analyzed the influence of operator’s experience on accuracy. |
| Mai et al. [36] | Segmental scan and merge methods were studied. |
| Kontis et al. [37] | Compared intraoral scans with laboratory scan of impressions and casts. |
| Ender et al. [38] | Complete dentition was present. |
| Tao et al. [39] | Accuracy comparison with and without resin markers. |
| Stefanelli et al. [40] | Compared scanning strategy. |
| Passos et al. [41] | Different intraoral scanners are compared. |
| Li et al. [42] | Compared the accuracy by using PEEK based scanning aid. |
| Baghani et al. [43] | Completely dentulous arch studied. |
| Gutmacher et al. [44] | Study performed on cadaveric maxilla. |
| Author Year | Country | Sample Size | Intra Oral Scanner | Laboratory Scanner | Jaws | Conventional Impression Type | Scanned Surface | Accuracy Evaluation Method | Aligning Software | Mean Difference (mm) | Mean RMS and Standard Deviation (mm) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| D’Arienzo et al., 2018 [20] | Italy | 4 | Trios 3 | NR | Maxilla | Dental cast obtained from an alginate impression. | Complete edentulous jaw. | Superimposition against 3D model obtained from lab scanner. | 3D Reshaper 2017 | 0.219 to 0.347 | NR |
| Chebib et al., 2019 [21] | Switzerland | 12 | Trios 3 | Iscan D103i (Imetric 3D) | Maxilla | ZOE impression (reference scan). Alginate PVS. PVS relined with ZOE (PVSM). | Complete impression surface and five different areas. Midpalatal raphe, peripheral border, inner seal, residual ridge, PPS | Superimposition against 3D model obtained from lab scanner. | Geomagic Control X64 | NR | 0.70 ± 0.18 |
| Jung et al., 2019 [22] | Republic of Korea | 5 | CS3500 Carestream | D700, 3Shape | Maxilla and mandible | Dental cast obtained from border-molded PVS impression. | maxilla. Midpalatal raphe, hard palate, residual ridge, soft palate. Mandible: residual ridge, buccal shelf. | Superimposition against 3D model obtained from lab scanner. | Geomagic control 2014 | Maxilla—0.09 ± 0.08 Mandible—0.04 ± 0.05 | NR |
| Lo Russo et al., 2020 [23] | Italy | 10 maxilla and 10 mandibles | Trios 3 | NR | Maxilla and mandible | Polysulfide impression. | Complete edentulous jaw. | Superimposition against 3D model obtained from IOS. | Geomagic wrap 2017 | Maxilla—0.11 ± 0.09 Mandibular—0.26 ± 0.29 (Trimmed scans) Maxilla—0.03 ± 0.03 Mandibular—0.02 ± 0.07 | NR |
| Hack et al., 2020 [24] | USA | 27 maxilla and 5 mandibles | Lava COS True Definition (3M ESPE) | D700 version 2013 3Shape | Maxilla and mandible | Border-molded PVS impression, stone cast obtained from an impression. | Complete edentulous jaws. | Conventional impressions and the resulting stone casts were digitized and superimposed over the optical impressions. | Geomagic Qualify 2013 | Overall—0.363 ± 0.143 Maxilla—0.308 ± 0.050 Mandible—0.532 ± 0.119 | NR |
| Kalberer et al., 2020 [25] | Switzerland | 12 | Trios 3 | Iscan D103i (Imetric 3D) | Maxilla | Border-molded ZOE impression. Alginate PVS. PVS relined with ZOE. | Anterior region, buccal region, and PPS region. | Three selected reference points to superimpose the impression. Only border extension (vertical) and seal (horizontal) were assessed. | Custom-made 3D comparison software | NR | Overall vertical discrepancy 1.95 ± 0.76 Overall horizontal discrepancy 2.23 ± 0.55 |
| Chebib et al., 2022 [26] | Switzerland | 20 | Trios 3 | Iscan D103i (Imetric 3D) | Maxilla | Scan of definitive cast obtained from border-molded ZOE impression. | Complete edentulous jaws. | Superimposition against 3D model obtained from lab scanner. | Geomagic control X 2020 | NR | 0.45 ± 0.11 |
| Al hamad 2023 [27] | Jordan | 21 | Trios 4 | Ceramill® map400 | Maxilla and mandible | Border-molded PVS impression. | Complete edentulous jaws. | Superimposition against 3D model obtained from lab scanner. | Geomagic Control X; 2020 | NR | Maxillary 0.92 ± 0.24 Mandibular 1.38 ± 0.29 |
| Author Year | Country | Sample Size (Per Scanner) | Scanner | Reference Scanner | Jaws | Surface Scanned | Accuracy Evaluation Method | Aligning Software | Result (Values in µm) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Patzelt et al., 2013 [13] | USA | 20 | 1. CEREC AC Bluecam 2. Lava COS 3. iTero, 4. Zfx IntraScan | Activity 101, smart Optics | Maxilla and mandible | Complete edentulous jaw. | Superimposition against 3D model obtained from laboratory scanner. | Geomagic Qualify 2012 | Maxillary | Trueness | Precision |
| CEREC AC Bluecam | 591.8 | 332.4 | |||||||||
| Lava COS | 52.9 | 30.8 | |||||||||
| iTero (3S) | 144.2 | 178.5 | |||||||||
| iTero (DW) | 139.5 | 166.8 | |||||||||
| Zfx IntraScan | 283.8 | 425.3 | |||||||||
| Mandibular | Trueness | Precision | |||||||||
| CEREC AC Bluecam | 558.4 | 698.0 | |||||||||
| Lava COS | 44.1 | 21.6 | |||||||||
| iTero (3S) | 191.5 | 197.9 | |||||||||
| iTero (DW217.3) | 154.7 | 217.3 | |||||||||
| Zfx IntraScan | 253.8 | 319.4 | |||||||||
| Braian and Wennerberg 2019 [28] | Sweden | 15 | 1. Omnicam 2. Itero 3. Planmeca 4. Carestream CS3600 5. TRIOS 3 | NR | Mandible | Complete edentulous jaw. | Measurement of distance between markers in edentulous arch and comparison with the reference data. | No aligning software used | Trueness | Precision | |
| Omnicam | 193 | 299 | |||||||||
| Itero | 81 | 85 | |||||||||
| Planmeca | 145 | 441 | |||||||||
| CarestreamCS3600 | 181 | 247 | |||||||||
| TRIOS 3 | 36 | 94 | |||||||||
| Osnes et al., 2020 [29] | Italy | 5 | 1. True Definition 2. Planmeca 3. Omnicam 4. Dental wings 5. Trios 3 6. Aadva | NR | Maxilla | Complete edentulous jaws. | Superimposition of 3D data within each group to assess precision. | Custom-made software | Mean deviations | ||
| True Definition | 250 | ||||||||||
| Planmeca | 870 | ||||||||||
| Omnicam | 320 | ||||||||||
| Dental wings | 970 | ||||||||||
| Trios 3 | 260 | ||||||||||
| Aadva | 30 | ||||||||||
| Zarone et al., 2020 [30] | Italy | 10 | Trios 3 | ATOS core 80 | Maxilla | Complete edentulous, smooth, and wrinkled model. | Superimposition against 3D model obtained from lab scanner. | Geomagic Control X | Trueness | Precision | |
| WT/BP | 48.7 | 46.7 | |||||||||
| WT/SS | 65.9 | 53.6 | |||||||||
| WT/PB | 109.7 | 90 | |||||||||
| ST/BP | 48.1 | 46 | |||||||||
| ST/SS | 56.4 | 76 | |||||||||
| ST/PB | 61.1 | 52.9 | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Srivastava, G.; Padhiary, S.K.; Mohanty, N.; Molinero-Mourelle, P.; Chebib, N. Accuracy of Intraoral Scanner for Recording Completely Edentulous Arches—A Systematic Review. Dent. J. 2023, 11, 241. https://doi.org/10.3390/dj11100241
Srivastava G, Padhiary SK, Mohanty N, Molinero-Mourelle P, Chebib N. Accuracy of Intraoral Scanner for Recording Completely Edentulous Arches—A Systematic Review. Dentistry Journal. 2023; 11(10):241. https://doi.org/10.3390/dj11100241
Chicago/Turabian StyleSrivastava, Gunjan, Subrat Kumar Padhiary, Neeta Mohanty, Pedro Molinero-Mourelle, and Najla Chebib. 2023. "Accuracy of Intraoral Scanner for Recording Completely Edentulous Arches—A Systematic Review" Dentistry Journal 11, no. 10: 241. https://doi.org/10.3390/dj11100241