

Descriptive Study of Oral Health in an Indigenous Child Population of Baka Pygmies in Cameroon
 ,
,  ,
,
Abstract
:1. Introduction
1.1. Oral Health in Cameroon
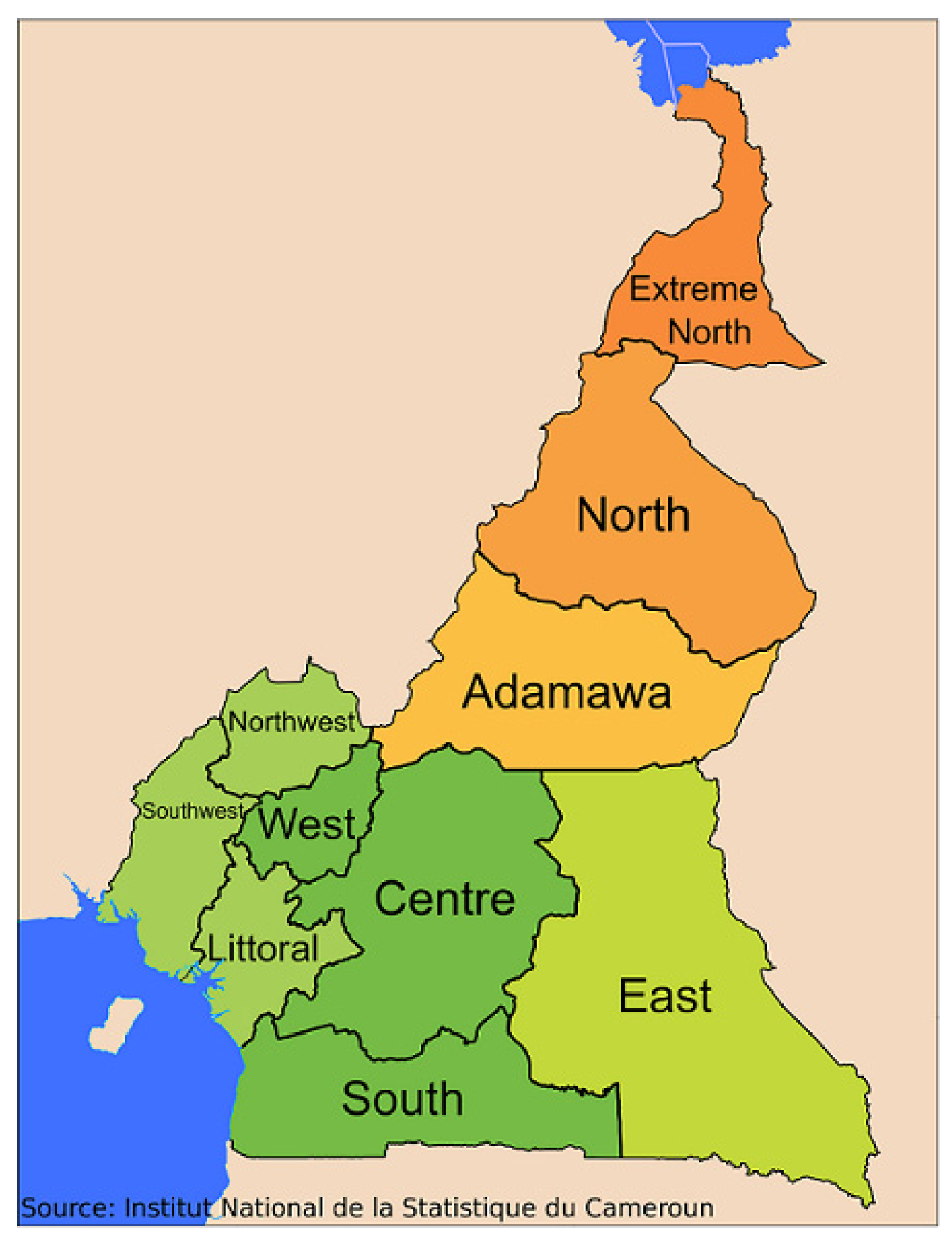
1.2. The Baka Pygmies
2. Materials and Methods
2.1. Design and Sampling
2.2. Study Variables
2.3. Statistical Analysis
3. Results
3.1. Sociodemographic Data
3.2. Daily Diet and Oral Hygiene Habits
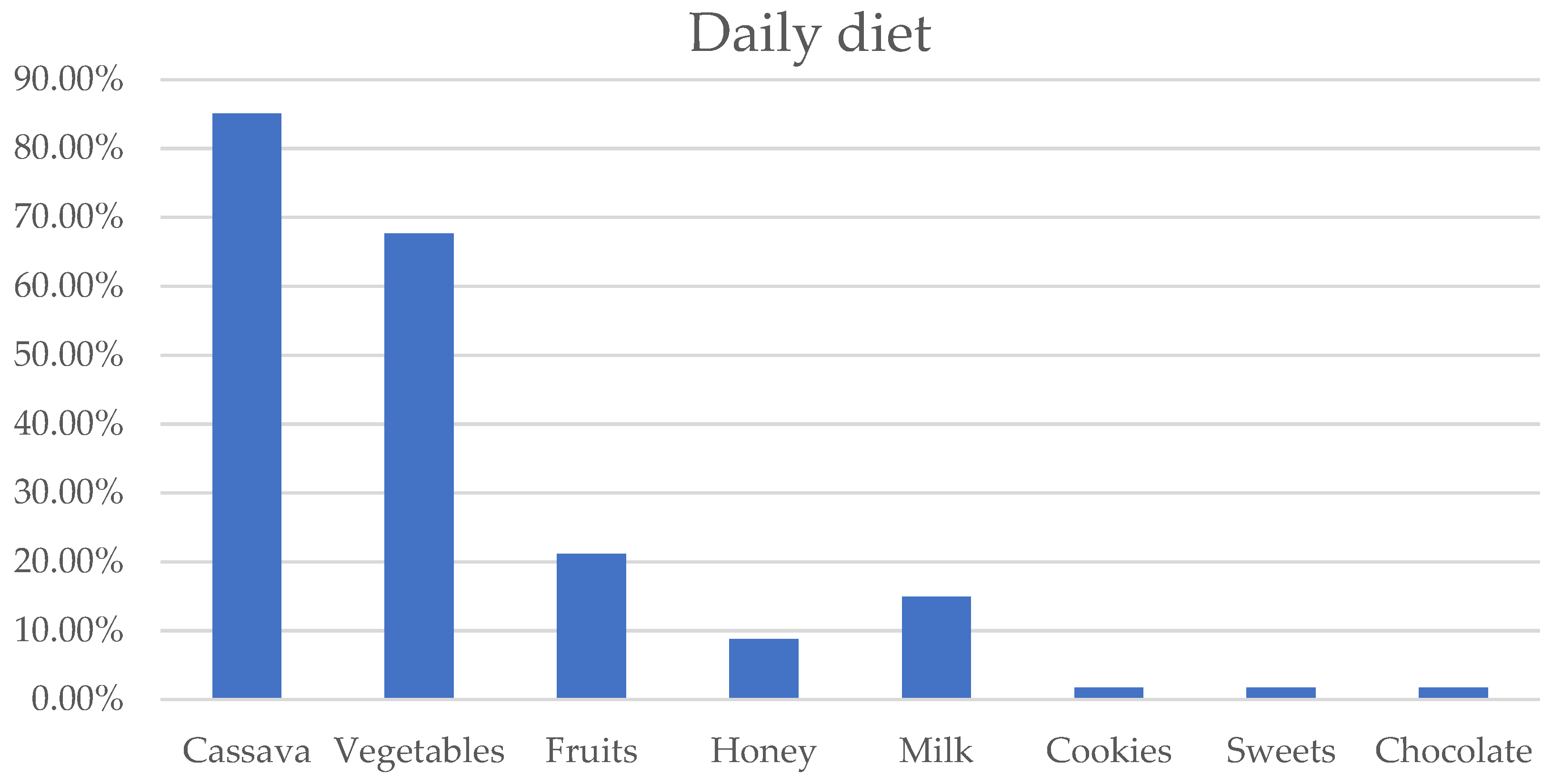
3.2.1. Daily Diet
3.2.2. Oral Hygiene Habits
3.3. Access to Oral Health Services
Dental Visits Received, Place of Visits, and Who Conducted Them
3.4. Interventions
3.5. Frequency of Dental Visits
3.6. Pathologies
3.6.1. Periodontal Status
3.6.2. Dental Caries
3.6.3. Other Oral Pathologies
4. Discussion
4.1. Sociodemographic Data
4.2. Diet
4.3. Oral Hygiene Habits
4.4. Access to Oral Health Services
4.5. Pathologies
4.5.1. Caries Prevalence and DMFT/dft
4.5.2. Periodontal Status
4.5.3. Other Pathologies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Petersen, P.E.; Bourgeois, D.; Ogawak, H.; Estupinan-day, S.; Ndiaye, C. Policy and Practice The global burden of oral diseases and risks to oral health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar]
- Parker, E.J.; Jamieson, L.M.; Broughton, J.; Albino, J.; Lawrence, H.P.; Roberts-thomson, K. The oral health of Indigenous children: A review of four nations. J. Paediatr. Child Health 2010, 46, 483–486. [Google Scholar] [CrossRef] [PubMed]
- Josefczyk, M. The State of Oral Health on the African Continent. Oral Heal Africa. Senior. Honors Thesis, Liberty University, Lynchburg, VA, USA, 16 September 2015. [Google Scholar]
- Da Silveira Moreira, R. Epidemiology of Dental Caries in the World. In Oral Health Care—Pediatric, Research, Epidemiology and Clinical Practices; InTech: London, UK, 2012; pp. 149–168. [Google Scholar] [CrossRef]
- Petersen, P.E. The World Oral Health Report 2003 WHO Global Oral Health Programme. Community Dent Oral Epidemiol. Community Dent. Oral Epidemiol. 2003, 31, 3–23. [Google Scholar] [CrossRef]
- González Alarcón, D. Estudio De La Eficacia De La Aplicación Única De La Solución De Fluoruro Diamínico De Plata Y El Barniz De Fluoruro Sódico En La Remineralización De La Lesión De Caries De La Población Infantil Camerunesa Tras 42 Meses De Seguimiento. Ph.D. Thesis, Universidad de Sevilla, Sevilla, Spain, 28 September 2017. [Google Scholar]
- Chidzonga, M.M.; Carneiro, L.C.; Kalyanyama, B.M.; Kwamin, F. Determinants of Oral Diseases in the African and Middle East Region Determinants of Oral Diseases in the African and Middle East Region. Adv. Dent. Res. 2015, 27, 26–31. [Google Scholar] [CrossRef]
- WHO. WHO Promoting Oral Health in Africa. 2016. Available online: http://www.who.int/oral_health/publications/promoting-oral-health-africa/en/%0A (accessed on 18 June 2023).
- Ahlgren, M.; Funk, T.; Marimo, C.; Ndiaye, C.; Alfvén, T. Management of noma: Practice competence and knowledge among healthcare workers in a rural district of Zambia. Glob. Health Action 2017, 10, 1340253. [Google Scholar] [CrossRef] [PubMed]
- Gezimu, W.; Demeke, A.; Duguma, A. Noma—A neglected disease of malnutrition and poor oral hygiene: A mini-review. SAGE Open Med. 2022, 10, 20503121221098110. [Google Scholar] [CrossRef]
- Farley, E.; Mehta, U.; Srour, M.L.; Lenglet, A. Noma (cancrum oris): A scoping literature review of a neglected disease (1843 to 2021). PLoS Neglected Trop. Dis. 2021, 15, e0009844. [Google Scholar] [CrossRef]
- Khammissa, R.A.G.; Lemmer, J.; Feller, L. Noma staging: A review. Trop. Med. Health 2022, 50, 40. [Google Scholar] [CrossRef]
- Bedi, R.; Scully, C. Manson’s Tropical Infectious Diseases, 23rd ed.; Elsever: Amsterdam, Netherlands, 2014; pp. 1073–1083. [Google Scholar] [CrossRef]
- Tobin, A.O.; Ajayi, I.O. Common oral conditions and correlates: An oral health survey in Kwara State Nigeria. BMC Res. Notes 2017, 10, 568. [Google Scholar] [CrossRef]
- Bolivar, I.; Whiteson, K.; Stadelmann, B.; Baratti-Mayer, D.; Gizard, Y.; Mombelli, A.; Pittet, D.; Schrenzel, J. The Geneva Study Group on Noma (GESNOMA) Bacterial Diversity in Oral Samples of Children in Niger with Acute Noma, Acute Necrotizing Gingivitis, and Healthy Controls. PLoS Neglected Trop. Dis. 2012, 6, e1556. [Google Scholar] [CrossRef]
- Petersen, P.E.; Ogawa, H. The global burden of periodontal disease: Towards integration with chronic disease prevention and control. Periodontology 2000 2012, 60, 15–39. [Google Scholar] [CrossRef] [PubMed]
- Ngapeth-Etoundi, M. Projet Pilote D’intégration Des Soins Bucco-Dentaires Dans Les Soins De Sante Primaire Au Cameroun. Proj. Pilot. 1989, 3, 1–10. [Google Scholar]
- Lolita, Y.M.; Michael, A.A.; Hubert, N.; Florence, D.; Jacques, B. Oral Health Status of the Elderly at Tonga, West Region, Cameroon. Int. J. Dent. 2015, 2015, 820416. [Google Scholar] [CrossRef]
- Blaise, N.-Y.H. Oral health assessment of urban and rural dwellers in Bafia-Cameroon. Int. J. Sci. Res. Arch. 2021, 1, 17–28. [Google Scholar] [CrossRef]
- Šimková, P.G.; Weber, G.W.; Rozzi, F.V.R.; Slimani, L.; Sadoine, J.; Fornai, C. Morphological variation of the deciduous second molars in the Baka Pygmies. Sci. Rep. 2021, 11, 16480. [Google Scholar] [CrossRef]
- Molloumba, F.; Bossalil, F.; Molloumba, P.; Bamengozi, J. Conséquences à long terme des mutilations dentaires chez les Bantous et Pygmées au nord-ouest du Congo-Brazzaville Consequences of dental mutilations in the long term among Bantous and Pygmies in the north-western part of Congo-Brazzaville. Actes. Société Française D’histoire De L’art Dent. 2009, 47–50. [Google Scholar]
- Pemunta, N.V. Factors Impeding Social Service Delivery among the Baka Pygmies of Cameroon. J. Progress. Hum. Serv. 2019, 30, 211–238. [Google Scholar] [CrossRef]
- Funk, S.M.; Guerra, B.P.; Zamora, A.B.; Ickowitz, A.; Poni, N.A.; Abdou, M.A.; Sibama, Y.H.; Penda, R.; Brull, G.R.; Abossolo, M.; et al. Understanding Growth and Malnutrition in Baka Pygmy Children. Hum. Ecol. 2020, 48, 293–306. [Google Scholar] [CrossRef]
- Tiwari, T.; Jamieson, L.; Broughton, J.; Lawrence, H.; Batliner, T.; Arantes, R.; Albino, J. Reducing Indigenous Oral Health Inequalities: A Review from 5 Nations. J. Dent. Res. 2018, 97, 869–877. [Google Scholar] [CrossRef]
- WHO. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Burbano, H.; Rebollo, L.; Cacho, J.L.; Vadillo, P.L.; de Guzmán, M.M.; de la Figuera, G.; García, R.G. Experiencias con Bombas de Mecate en tres Escuelas del Subdepartamento de Bengbis, Provincia del Sur, Camerún. Available online: http://polired.upm.es/index.php/distecd/article/view/2509 (accessed on 18 June 2023).
- Nke, N.J. Gestion des écosystèmes forestiers par les Pygmées Bakola/Bagielli et voisins Bantu au Sud Ouest du Cameroun face à l’exploitation néolibérale. Ph.D. Thesis, Université catholique de Louvain, Ottignies-Louvain-la-Neuve, Belgium, 2014. [Google Scholar]
- Dapi, L.N.; Nouedoui, C.; Janlert, U.; Håglin, L. Adolescents’ food habits and nutritional status in urban and rural areas in Cameroon, Africa’. Scand J Nutr. 2005, 49, 151–158. [Google Scholar] [CrossRef]
- Mennen, L.; Mbanya, J.; Cade, J.; Balkau, B.; Sharma, S.; Chungong, S.; Cruickshank, J. The habitual diet in rural and urban Cameroon. Eur. J. Clin. Nutr. 2000, 54, 150–154. [Google Scholar] [CrossRef]
- Okolo, S.; Chukwu, G.; Egbuonu, I.; Ezeogu, F.; Onwuanaku, C.; Adeleke, O.; Hassan, A.; Ngoe-Nesoah, A. Oral hygiene and nutritional status of children aged 1–7 years in a rural community. Ghana Med. J. 2006, 40, 22–25. [Google Scholar]
- Tchoumba, B. Indigenous and Tribal Peoples and Poverty Reduction Strategies in Cameroon. Available online: http://www.ilo.org/global/standards/lang--en/index.htm (accessed on 18 June 2023).
- Azodo, C.C.; Agbor, A.M. Gingival health and oral hygiene practices of schoolchildren in the North West Region of Cameroon. BMC Res. Notes 2015, 8, 385. [Google Scholar] [CrossRef]
- Mots, V. Le brossage dentaire: Quelle méthode ? Toothbrushing: Which methods to use ? Rev. Odont. Stomat. 2011, 40, 239–260. [Google Scholar]
- Agbor, A.M.; Azodo, C.C.; Naidoo, S. Ritual tooth modification among the Baka pygmies in Cameroon. Odontostomatol. Trop. 2015, 38, 21–30. [Google Scholar]
- Agbor, A.; Azodo, C.; Naidoo, S. The Oral Health workforce in Cameroon; the past, the present and the future. Afr. J. Oral Health 2018, 7, 11. [Google Scholar] [CrossRef]
- Ndiaye, C. Oral health in the African region: Progress and perspectives of the regional strategy. Afr. J. Oral Health 2005, 2, 2–9. [Google Scholar] [CrossRef]
- Kutesa, A.; Kasangaki, A.; Nkamba, M.; Muwazi, L.; Okullo, I.; Rwenyonyi, C.M. Prevalence and factors associated with dental caries among children and adults in selected districts in Uganda. Afr. Health Sci. 2016, 15, 1302–1307. [Google Scholar] [CrossRef]
- Gonçalves, M.; Cavalcanti, L.C.; Firmino, R.T.; Ribeiro, G.L.; Granville-Garcia, A.F.; Menezes, V.A. Dental caries experience among indigenous children and adolescents. J. Oral Sci. 2015, 57, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Gilli, M.; Maringer, D.; Schumann, E. Basic Methods. Numer. Methods Optim. Financ. 2011, 287–336. [Google Scholar]



{kind=link}
{kind=link}
| Frequency | Percentage | ||
|---|---|---|---|
| Gender | Female | 51 | 57.88% |
| Male | 69 | 42.51% | |
| Age range | [5–6] | 106 | 88.38% |
| [11–12] | 14 | 11.62% | |
| Study level | CPC (Community Preschool Center) | 80 | 66.60% |
| SIL (1st grade) | 17 | 14.40% | |
| CP (2nd elementary) | 4 | 3.33% | |
| CE1(3rd grade) | 5 | 4.18% | |
| CE2 (4th grade) | 2 | 1.74% | |
| Non-schooling | 12 | 9.75% |
| Camp | Frequency | Percentage | Camp | Frequency | Percentage |
|---|---|---|---|---|---|
| Adjap Mintom | 13 | 10.83% | Belleville | 5 | 4.17% |
| Doum | 12 | 10.00% | Opkweng | 4 | 3.33% |
| Mfem | 10 | 8.33% | Assock | 4 | 3.33% |
| Akonetié | 9 | 7.50% | Meyos Mintom | 3 | 2.50% |
| Akom | 8 | 6.67% | Ndibot | 3 | 2.50% |
| Bemba2 | 8 | 6.67% | Bifilon | 3 | 2.50% |
| Minkoo | 7 | 5.83% | Mebane3 | 3 | 1.67% |
| Mveng | 7 | 5.83% | Niabibete | 3 | 1.67% |
| Zoulabot | 7 | 5.83% | Mebane2 | 1 | 0.83% |
| Miata | 6 | 5.00% | Mekas | - | - |
| Alouma | 6 | 5.00% | Nkolasseck | - | - |
| Age Range | Total | ||
|---|---|---|---|
| [5–6] (n = 27)% | [11–12] (n = 10)% | (n = 37)% | |
| Toothbrushing frequency | |||
| 3 times a day | (12) 44.4% | (3) 30% | (15) 40.5% |
| Twice a day | (1) 3.7% | (4) 40% | (5) 13.5% |
| Once a day | (4) 14.8% | (2) 20% | (6) 16.2% |
| Sometimes | (10) 37.0% | (1) 10% | (11) 29.7% |
| Toothbrushing technique | |||
| Vertical | (1) 3.7% | - | (1) 2.7% |
| Horizontal | (26) 96.2% | (10) 100% | (26) 97.29% |
| Mixed | - | - | - |
| Circular | - | - | - |
| Instruments used | |||
| Toothbrush | (27) 100% | (10) 100% | (37) 100% |
| Coal | - | - | - |
| Fingers | (1) 3.7% | (4) 40% | (5) 13.5% |
| Sticks | - | - | |
| Toothbrushing aids | |||
| Dentifrice | (22) 81.48% | (10) 100% | (32) 91.4% |
| Soap | (4) 14.8% | (4) 40% | (8) 21.6% |
| Salt | (3) 11.1% | (4) 40% | (7) 19.0% |
| Coal/ashes | (1) 3.7% | (2) 20% | (3) 8.1% |
| Nothing | (21) 7.7% | (9) 90.0% | (30) 81.1 |
| Frequency | Percentage | ||
|---|---|---|---|
| Visits (n = 120) | Visits received | 17 | 13.7% |
| No visits | 103 | 86.3% | |
| Place of visits (n = 17) | School | 12 | 70.1% |
| Camp | 7 | 43.2% | |
| Hospital | - | - | |
| Who conducted it? (n = 17) | NGO | 17 | 100% |
| Dentists of public services | - | - |
| Interventions | [5–6] (n = 14)% | [11–12] (n = 3)% | Females (n = 9)% | Males (n = 8)% |
|---|---|---|---|---|
| Oral hygiene training | (3) 23.6% | (1) 33.3% | (3) 33.33% | (1) 12.5% |
| Tartrectomy | (1) 8.2% | - | (1) 11.11% | - |
| Sealants, fluoridation | (7) 52.9% | (2) 67.5% | (3) 33.33% | (6) 75% |
| Others (tooth extractions, etc.) | (3) 23.4% | - | (2) 22.22% | (1) 12.5% |
| Age Range | Gender | |||
|---|---|---|---|---|
| [5–6] (n = 14)% | [11–12] (n = 3)% | Females (n = 9)% | Males (n = 8)% | |
| Frequency of dental visits | ||||
| Once | (5) 35.71% | (3) 100.0% | (6) 66.66% | (2) 25% |
| More than twice | (9) 64.3% | - | (3) 33.33% | (6) 75% |
| Date of last visit | ||||
| More than 6 months | (1) 7.14% | - | (1) 11.11% | - |
| More than one year | (9) 64.3% | (3) 100.0% | (8) 88.88% | (4)50% |
| I do not know | (4) 28.57% | - | - | (4) 50% |
| No Bleeding | Bleeding | Calculus | |||||
|---|---|---|---|---|---|---|---|
| Age range | Frequency | Percentage | Frequency | Percentage | Frequency | Percentage | p value |
| [5–6] | 13 | 12.26% | 93 | 87.74% | 28 | 26.4% | |
| 0.018 * | |||||||
| [11–12] | 2 | 12 | 85.7% | 8 | 56.6% | ||
| 14.3% | |||||||
| Females | 6 | 10.15% | 45 | 76.27% | 15 | 29.5% | |
| Gender | 0.944 | ||||||
| Males | 9 | 14.75% | 60 | 98.36% | 21 | 30.1% | |
| TOTAL | 15/120 | 13% | 105/120 | 87% | 36/120 | 30% | |
| Gender | Age Range | ||||
|---|---|---|---|---|---|
| Prevalence (n = 120)% | Males (n = 69)% | Females (n = 51)% | [5–6] (n = 106)% | [11–12] (n = 14)% | |
| Illness | |||||
| Wounds, scars | (1) 0.83% | (1) 2.2% | - | (1) 2.2% | - |
| Noma | - | - | (1) 2.2% | (1) 1% | - |
| Tumors | (4) 3.9% | (4) 3.9% | - | (2) 3.0% | (2) 14.28% |
| Total | (5) 4.7% | (5) 7.2% | - | (3) 2.83% | (2) 14.28% |
| Mucosal lesions | |||||
| NG | (5) 4.16% | (3) 4.6% | (2) 4.1% | (4) 4.0% | (1) 7.1% |
| Abscess | (4) 3.33% | (3) 4.6% | (1) 2.0% | (4) 3.5% | - |
| Others (recessions) | (3) 2.5% | (3) 4.2% | - | (3) 2.8% | - |
| Total | (12) 10% | (9) 13.2% | (3) 6.1% | (11) 10.3% | (1) 7.1% |
| (75) 62.5% | (47) 67.1% | (28) 56.2% | (72) 67.7% | (3) 22% | |
| Dental Mutilation | - | - | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poni, N.A.; Ribas-Pérez, D.; Flores-Fraile, J.; Hernández-Franch, P.V.; Rodríguez-Menacho, D.; Castaño-Séiquer, A. Descriptive Study of Oral Health in an Indigenous Child Population of Baka Pygmies in Cameroon. Dent. J. 2023, 11, 237. https://doi.org/10.3390/dj11100237
Poni NA, Ribas-Pérez D, Flores-Fraile J, Hernández-Franch PV, Rodríguez-Menacho D, Castaño-Séiquer A. Descriptive Study of Oral Health in an Indigenous Child Population of Baka Pygmies in Cameroon. Dentistry Journal. 2023; 11(10):237. https://doi.org/10.3390/dj11100237
Chicago/Turabian StylePoni, Nicias Afoumpam, David Ribas-Pérez, Javier Flores-Fraile, Paloma Villalva Hernández-Franch, Diego Rodríguez-Menacho, and Antonio Castaño-Séiquer. 2023. "Descriptive Study of Oral Health in an Indigenous Child Population of Baka Pygmies in Cameroon" Dentistry Journal 11, no. 10: 237. https://doi.org/10.3390/dj11100237