
Implementation of a Full Digital Workflow by 3D Printing Intraoral Splints Used in Dental Education: An Exploratory Observational Study with Respect to Students’ Experiences
 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
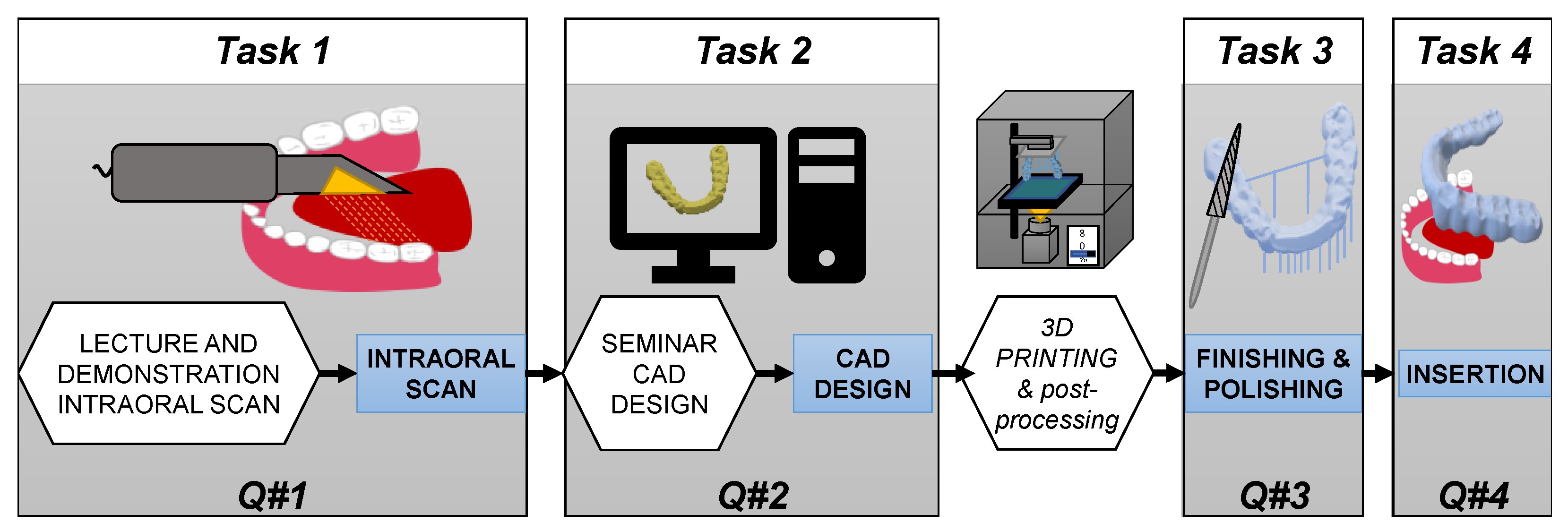
2.2. Study Design
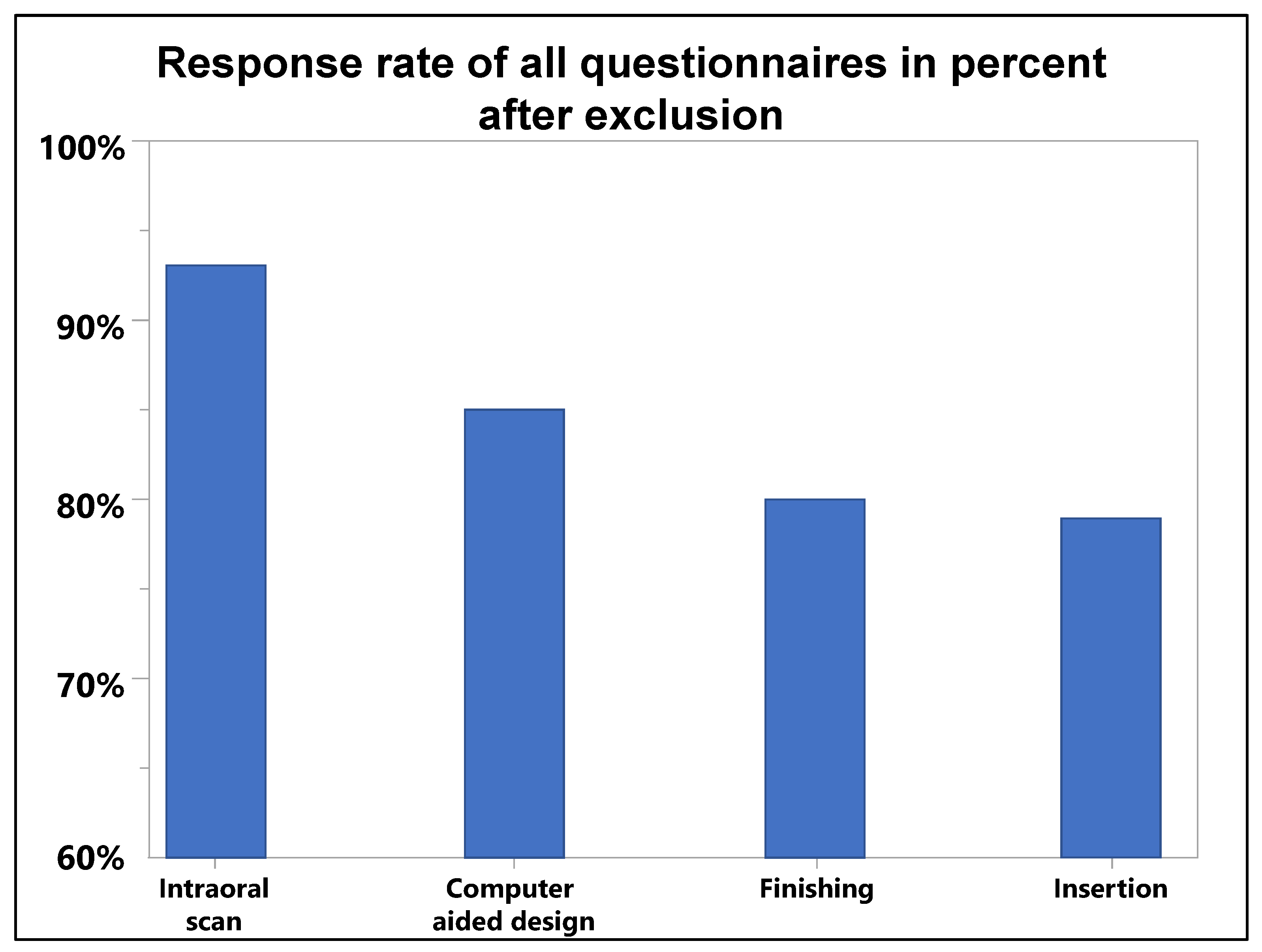
2.3. Questionnaires for the Evaluation of the Tasks
2.4. Task 1: Intraoral Scanning
2.5. Task 2: Computer-Aided Design (CAD)
2.6. Computer-Aided Manufacturing
2.7. Tasks 3 and 4: Finishing and Insertion
2.8. Data Acquisition
2.9. Data Validation and Statistical Analysis
3. Results
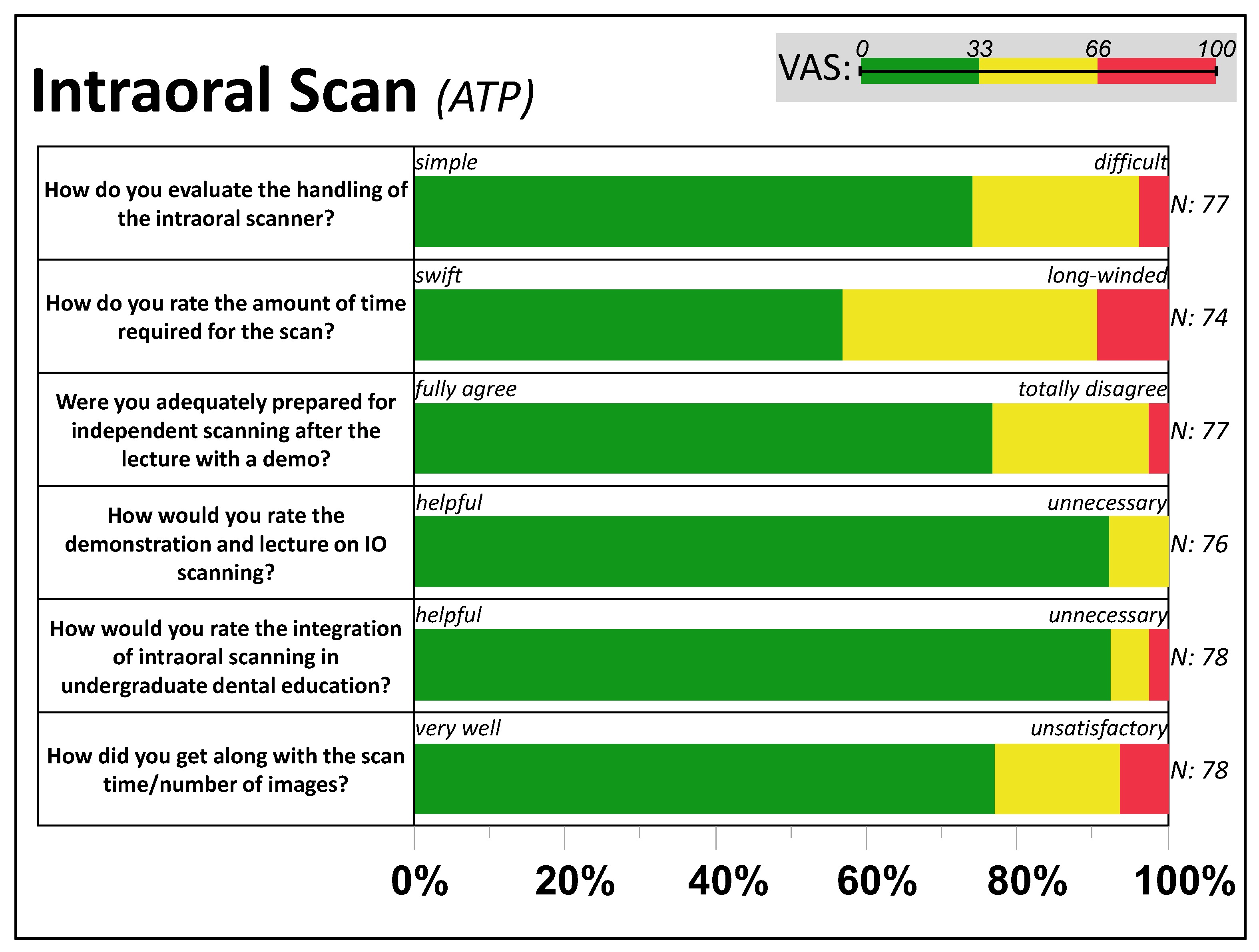
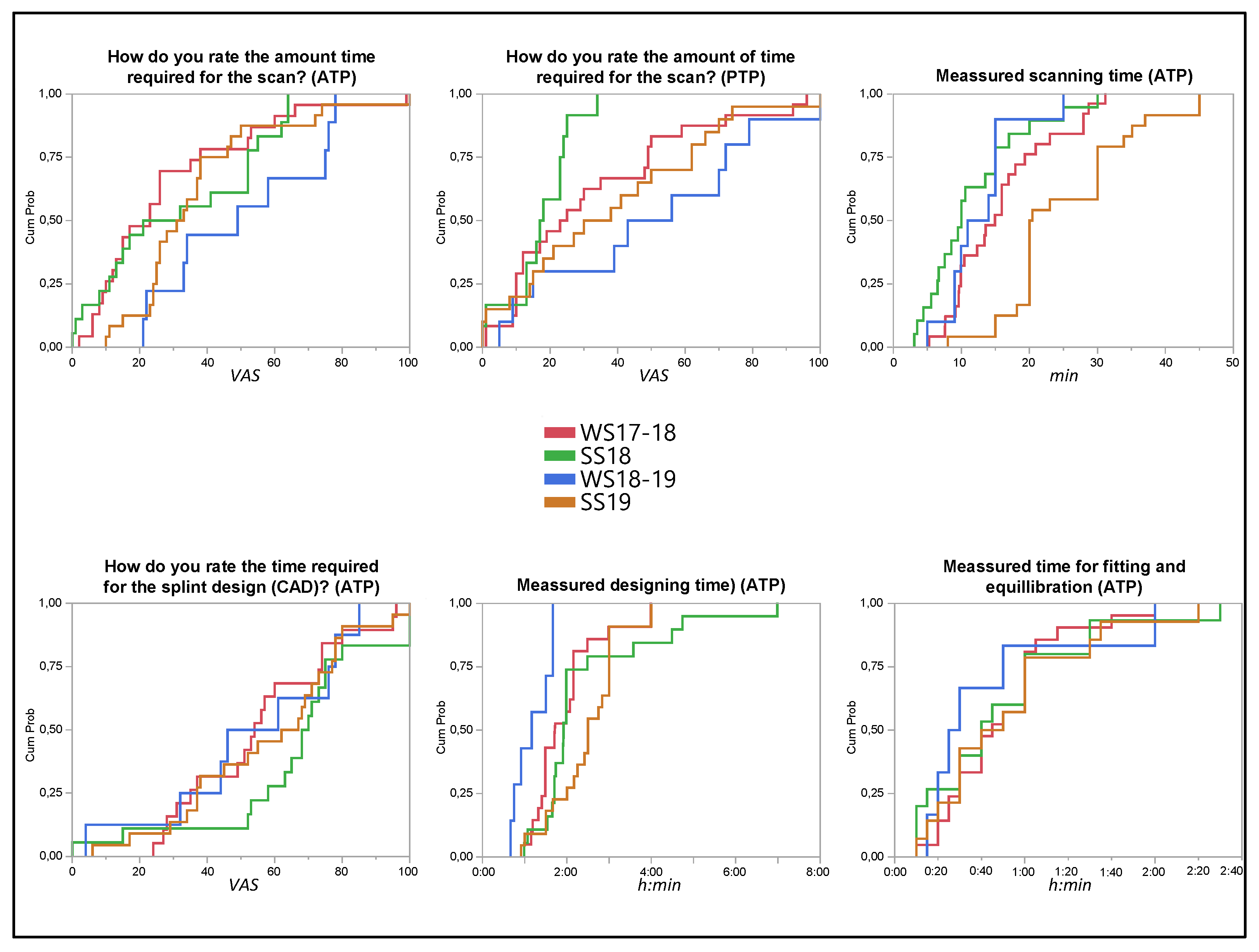
3.1. Feedback from Task 1: Intraoral Scan
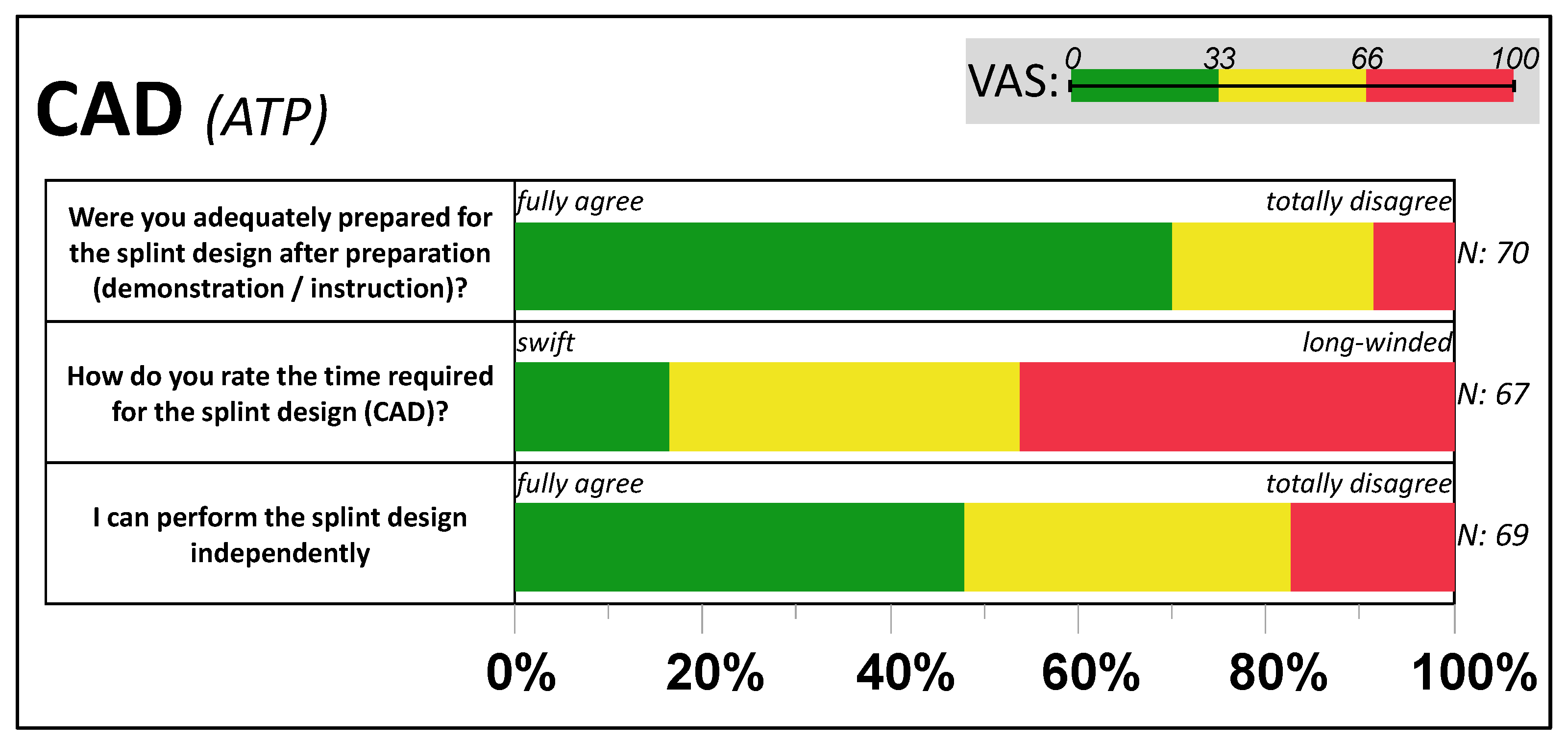
3.2. Feedback from Task 2: Computer-Aided Design
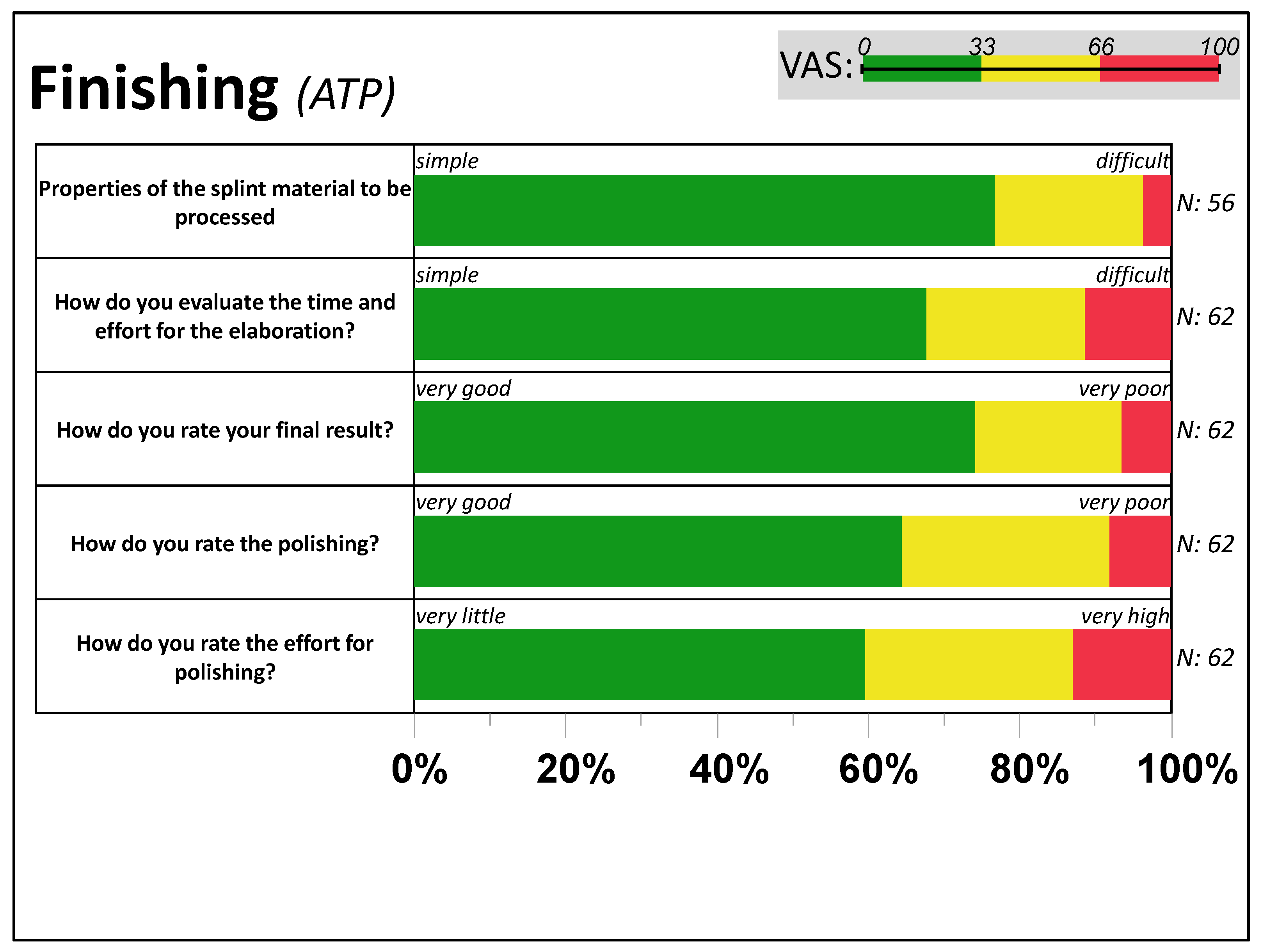
3.3. Feedback from Task 3: Finishing
3.4. Feedback from Task 4: Insertion
3.5. Reflection of the Workflow/General Preferences
3.6. Longitudinal Observation of the Item Reproducibility
3.7. Control for Individual Resources and Preferences
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Revilla-Leon, M.; Frazier, K.; da Costa, J.B.; Kumar, P.; Duong, M.L.; Khajotia, S.; Urquhart, O.; Council on Scientific, A. Intraoral scanners: An American Dental Association Clinical Evaluators Panel survey. J. Am. Dent. Assoc. 2021, 152, 669–670.e662. [Google Scholar] [CrossRef] [PubMed]
- Rekow, E.D. Digital dentistry: The new state of the art—Is it disruptive or destructive? Dent. Mater. 2020, 36, 9–24. [Google Scholar] [CrossRef] [PubMed]
- van der Zande, M.M.; Gorter, R.C.; Wismeijer, D. Dental practitioners and a digital future: An initial exploration of barriers and incentives to adopting digital technologies. Br. Dent. J. 2013, 215, E21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schweiger, J.; Edelhoff, D.; Beuer, F.; Stimmelmayr, M.; Güth, J. Analog versus digital—Update Zahntechnik. Die Quintessenz 2017, 68, 979–992. [Google Scholar]
- Mormann, W.H. The evolution of the CEREC system. J. Am. Dent. Assoc. 2006, 137, 7S–13S. [Google Scholar] [CrossRef]
- Kramer Fernandez, P.; Kuscu, E.; Weise, H.; Engel, E.M.; Spintzyk, S. Rapid additive manufacturing of an obturator prosthesis with the use of an intraoral scanner: A dental technique. J. Prosthet. Dent. 2022, 127, 189–193. [Google Scholar] [CrossRef]
- Unkovskiy, A.; Wahl, E.; Zander, A.T.; Huettig, F.; Spintzyk, S. Intraoral scanning to fabricate complete dentures with functional borders: A proof-of-concept case report. BMC Oral Health 2019, 19, 46. [Google Scholar] [CrossRef] [Green Version]
- Rekow, D. Computer-aided design and manufacturing in dentistry: A review of the state of the art. J. Prosthet. Dent. 1987, 58, 512–516. [Google Scholar] [CrossRef]
- Bandiaky, O.N.; Le Bars, P.; Gaudin, A.; Hardouin, J.B.; Cheraud-Carpentier, M.; Mbodj, E.B.; Soueidan, A. Comparative assessment of complete-coverage, fixed tooth-supported prostheses fabricated from digital scans or conventional impressions: A systematic review and meta-analysis. J. Prosthet. Dent. 2020, 127, 71–79. [Google Scholar] [CrossRef]
- Abdel-Azim, T.; Rogers, K.; Elathamna, E.; Zandinejad, A.; Metz, M.; Morton, D. Comparison of the marginal fit of lithium disilicate crowns fabricated with CAD/CAM technology by using conventional impressions and two intraoral digital scanners. J. Prosthet. Dent. 2015, 114, 554–559. [Google Scholar] [CrossRef]
- Malaguti, G.; Rossi, R.; Marziali, B.; Esposito, A.; Bruno, G.; Dariol, C.; Di Fiore, A. In vitro evaluation of prosthodontic impression on natural dentition: A comparison between traditional and digital techniques. Oral Implantol. 2016, 9, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Seelbach, P.; Brueckel, C.; Wostmann, B. Accuracy of digital and conventional impression techniques and workflow. Clin. Oral Investig. 2013, 17, 1759–1764. [Google Scholar] [CrossRef] [PubMed]
- Winkler, J.; Gkantidis, N. Trueness and precision of intraoral scanners in the maxillary dental arch: An in vivo analysis. Sci. Rep. 2020, 10, 1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kihara, H.; Hatakeyama, W.; Komine, F.; Takafuji, K.; Takahashi, T.; Yokota, J.; Oriso, K.; Kondo, H. Accuracy and practicality of intraoral scanner in dentistry: A literature review. J. Prosthodont. Res. 2020, 64, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Tomita, Y.; Uechi, J.; Konno, M.; Sasamoto, S.; Iijima, M.; Mizoguchi, I. Accuracy of digital models generated by conventional impression/plaster-model methods and intraoral scanning. Dent. Mater. J. 2018, 37, 628–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Memari, Y.; Mohajerfar, M.; Armin, A.; Kamalian, F.; Rezayani, V.; Beyabanaki, E. Marginal Adaptation of CAD/CAM All-Ceramic Crowns Made by Different Impression Methods: A Literature Review. J. Prosthodont. 2019, 28, e536–e544. [Google Scholar] [CrossRef] [PubMed]
- Serag, M.; Nassar, T.A.; Avondoglio, D.; Weiner, S. A Comparative Study of the Accuracy of Dies Made from Digital Intraoral Scanning vs. Elastic Impressions: An In Vitro Study. J. Prosthodont. 2018, 27, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Wesemann, C.; Muallah, J.; Mah, J.; Bumann, A. Accuracy and efficiency of full-arch digitalization and 3D printing: A comparison between desktop model scanners, an intraoral scanner, a CBCT model scan, and stereolithographic 3D printing. Quintessence Int. 2017, 48, 41–50. [Google Scholar] [CrossRef]
- Prager, M.C.; Liss, H. Assessment of Digital Workflow in Predoctoral Education and Patient Care in North American Dental Schools. J. Dent. Educ. 2020, 84, 350–357. [Google Scholar] [CrossRef]
- Schlenz, M.A.; Michel, K.; Wegner, K.; Schmidt, A.; Rehmann, P.; Wostmann, B. Undergraduate dental students’ perspective on the implementation of digital dentistry in the preclinical curriculum: A questionnaire survey. BMC Oral Health 2020, 20, 78. [Google Scholar] [CrossRef] [Green Version]
- Zitzmann, N.U.; Kovaltschuk, I.; Lenherr, P.; Dedem, P.; Joda, T. Dental Students’ Perceptions of Digital and Conventional Impression Techniques: A Randomized Controlled Trial. J. Dent. Educ. 2017, 81, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Zitzmann, N.U.; Matthisson, L.; Ohla, H.; Joda, T. Digital Undergraduate Education in Dentistry: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 3269. [Google Scholar] [CrossRef] [PubMed]
- Schwindling, F.S.; Deisenhofer, U.K.; Porsche, M.; Rammelsberg, P.; Kappel, S.; Stober, T. Establishing CAD/CAM in Preclinical Dental Education: Evaluation of a Hands-On Module. J. Dent. Educ. 2015, 79, 1215–1221. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, K.E.; Wang, T.; Li, K.Y.; Luk, W.K.; Burrow, M.F. Performance and perception of dental students using three intraoral CAD/CAM scanners for full-arch scanning. J. Prosthodont. Res. 2019, 63, 167–172. [Google Scholar] [CrossRef]
- An, H.; Langas, E.E.; Gill, A.S. Effect of scanning speed, scanning pattern, and tip size on the accuracy of intraoral digital scans. J. Prosthet. Dent. 2022. [Google Scholar] [CrossRef]
- Mennito, A.S.; Evans, Z.P.; Lauer, A.W.; Patel, R.B.; Ludlow, M.E.; Renne, W.G. Evaluation of the effect scan pattern has on the trueness and precision of six intraoral digital impression systems. J. Esthet. Restor. Dent. 2018, 30, 113–118. [Google Scholar] [CrossRef]
- Moon, Y.G.; Lee, K.M. Comparison of the accuracy of intraoral scans between complete-arch scan and quadrant scan. Prog. Orthod. 2020, 21, 36. [Google Scholar] [CrossRef]
- Kernen, F.; Schlager, S.; Seidel Alvarez, V.; Mehrhof, J.; Vach, K.; Kohal, R.; Nelson, K.; Flugge, T. Accuracy of intraoral scans: An in vivo study of different scanning devices. J. Prosthet. Dent. 2021, 128, 1303–1309. [Google Scholar] [CrossRef]
- Resende, C.C.D.; Barbosa, T.A.Q.; Moura, G.F.; Tavares, L.D.N.; Rizzante, F.A.P.; George, F.M.; Neves, F.D.D.; Mendonca, G. Influence of operator experience, scanner type, and scan size on 3D scans. J. Prosthet. Dent. 2021, 125, 294–299. [Google Scholar] [CrossRef]
- Al Hamad, K.Q. Learning curve of intraoral scanning by prosthodontic residents. J. Prosthet. Dent. 2020, 123, 277–283. [Google Scholar] [CrossRef]
- Roth, I.; Czigola, A.; Joos-Kovacs, G.L.; Dalos, M.; Hermann, P.; Borbely, J. Learning curve of digital intraoral scanning—An in vivo study. BMC Oral Health 2020, 20, 287. [Google Scholar] [CrossRef]
- Pillai, S.; Upadhyay, A.; Khayambashi, P.; Farooq, I.; Sabri, H.; Tarar, M.; Lee, K.T.; Harb, I.; Zhou, S.; Wang, Y.; et al. Dental 3D-Printing: Transferring Art from the Laboratories to the Clinics. Polymers 2021, 13, 157. [Google Scholar] [CrossRef] [PubMed]
- von See, C. Additive Verfahren in der Zahnmedizin. ZWR Dtsch. Zahnärzteblatt 2019, 128, 440–445. [Google Scholar] [CrossRef]
- Huettig, F.; Krämer-Fernandez, P.; Unkovskiy, A.; Spintzyk, S. 3-D-Druck in der prothetischen Zahnmedizin: Wo stehen wir? ZWR Dtsch. Zahnärzteblatt 2020, 129, 642–650. [Google Scholar] [CrossRef]
- Revilla-Leon, M.; Meyer, M.J.; Zandinejad, A.; Ozcan, M. Additive manufacturing technologies for processing zirconia in dental applications. Int. J. Comput. Dent. 2020, 23, 27–37. [Google Scholar]
- Anadioti, E.; Musharbash, L.; Blatz, M.B.; Papavasiliou, G.; Kamposiora, P. 3D printed complete removable dental prostheses: A narrative review. BMC Oral Health 2020, 20, 343. [Google Scholar] [CrossRef]
- Salmi, M.; Paloheimo, K.S.; Tuomi, J.; Ingman, T.; Makitie, A. A digital process for additive manufacturing of occlusal splints: A clinical pilot study. J. R. Soc. Interface 2013, 10, 20130203. [Google Scholar] [CrossRef]
- Berntsen, C.; Kleven, M.; Heian, M.; Hjortsjo, C. Clinical comparison of conventional and additive manufactured stabilization splints. Acta Biomater. Odontol. Scand. 2018, 4, 81–89. [Google Scholar] [CrossRef]
- Shaheen, E.; Sun, Y.; Jacobs, R.; Politis, C. Three-dimensional printed final occlusal splint for orthognathic surgery: Design and validation. Int. J. Oral Maxillofac. Surg. 2017, 46, 67–71. [Google Scholar] [CrossRef]
- Huettig, F.; Kustermann, A.; Kuscu, E.; Geis-Gerstorfer, J.; Spintzyk, S. Polishability and wear resistance of splint material for oral appliances produced with conventional, subtractive, and additive manufacturing. J. Mech. Behav. Biomed. Mater. 2017, 75, 175–179. [Google Scholar] [CrossRef]
- Dedem, P.; Turp, J.C. Digital Michigan splint—From intraoral scanning to plasterless manufacturing. Int. J. Comput. Dent. 2016, 19, 63–76. [Google Scholar] [PubMed]
- Gratton, D.G.; Kwon, S.R.; Blanchette, D.R.; Aquilino, S.A. Performance of two different digital evaluation systems used for assessing pre-clinical dental students’ prosthodontic technical skills. Eur. J. Dent. Educ. 2017, 21, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Hamil, L.M.; Mennito, A.S.; Renne, W.G.; Vuthiganon, J. Dental students’ opinions of preparation assessment with E4D compare software versus traditional methods. J. Dent. Educ. 2014, 78, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- Marti, A.M.; Harris, B.T.; Metz, M.J.; Morton, D.; Scarfe, W.C.; Metz, C.J.; Lin, W.S. Comparison of digital scanning and polyvinyl siloxane impression techniques by dental students: Instructional efficiency and attitudes towards technology. Eur. J. Dent. Educ. 2017, 21, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Douglas, R.D.; Hopp, C.D.; Augustin, M.A. Dental students’ preferences and performance in crown design: Conventional wax-added versus CAD. J. Dent. Educ. 2014, 78, 1663–1672. [Google Scholar] [CrossRef] [PubMed]
- Unkovskiy, A.; Schmidt, F.; Beuer, F.; Li, P.; Spintzyk, S.; Kraemer Fernandez, P. Stereolithography vs. Direct Light Processing for Rapid Manufacturing of Complete Denture Bases: An In Vitro Accuracy Analysis. J. Clin. Med. 2021, 10, 1070. [Google Scholar] [CrossRef]
- Zimmermann, M.; Mormann, W.; Mehl, A.; Hickel, R. Teaching dental undergraduate students restorative CAD/CAM technology: Evaluation of a new concept. Int. J. Comput. Dent. 2019, 22, 263–271. [Google Scholar]
- Tan, Y.Y.; Ho, T.K.; Goo, C.L. Effect of training on time efficiency and marginal adaptation of computer-aided design/computer-aided manufacturing crowns among dental students. Eur. J. Dent. Educ. 2022, 26, 468–474. [Google Scholar] [CrossRef]
- Kurz, M.; Attin, T.; Mehl, A. Influence of material surface on the scanning error of a powder-free 3D measuring system. Clin. Oral Investig. 2015, 19, 2035–2043. [Google Scholar] [CrossRef] [Green Version]
- Mays, K.A.; Levine, E. Dental Students’ Self-Assessment of Operative Preparations Using CAD/CAM: A Preliminary Analysis. J. Dent. Educ. 2014, 78, 1673–1680. [Google Scholar] [CrossRef]
- Lenherr, P.; Marinello, C.P. prepCheck computer-supported objective evaluation of students preparation in preclinical simulation laboratory. Swiss Dent. J. 2014, 124, 1085–1092. [Google Scholar] [PubMed]
- Prakash, K.S.; Nancharaih, T.; Rao, V.V.S. Additive Manufacturing Techniques in Manufacturing—An Overview. Mater. Today Proc. 2018, 5, 3873–3882. [Google Scholar] [CrossRef]
- Faludi, J.; Bayley, C.; Bhogal, S.; Iribarne, M. Comparing environmental impacts of additive manufacturing vs traditional machining via life-cycle assessment. Rapid Prototyp. J. 2015, 21, 14–33. [Google Scholar] [CrossRef]
- Lutz, A.M.; Hampe, R.; Roos, M.; Lumkemann, N.; Eichberger, M.; Stawarczyk, B. Fracture resistance and 2-body wear of 3-dimensional-printed occlusal devices. J. Prosthet. Dent. 2019, 121, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Grymak, A.; Waddell, J.N.; Aarts, J.M.; Ma, S.; Choi, J.J.E. Evaluation of wear behaviour of various occlusal splint materials and manufacturing processes. J. Mech. Behav. Biomed. Mater. 2022, 126, 105053. [Google Scholar] [CrossRef] [PubMed]
- Wesemann, C.; Spies, B.C.; Sterzenbach, G.; Beuer, F.; Kohal, R.; Wemken, G.; Krugel, M.; Pieralli, S. Polymers for conventional, subtractive, and additive manufacturing of occlusal devices differ in hardness and flexural properties but not in wear resistance. Dent. Mater. 2021, 37, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Reymus, M.; Stawarczyk, B. In vitro study on the influence of postpolymerization and aging on the Martens parameters of 3D-printed occlusal devices. J. Prosthet. Dent. 2021, 125, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Schmeiser, F.; Baumert, U.; Stawarczyk, B. Two-body wear of occlusal splint materials from subtractive computer-aided manufacturing and three-dimensional printing. Clin. Oral Investig. 2022, 26, 5857–5866. [Google Scholar] [CrossRef]
- Kuscu, E.; Klink, A.; Spintzyk, S.; Kraemer Fernandez, P.; Huettig, F. Bonding Interface and Repairability of 3D-Printed Intraoral Splints: Shear Bond Strength to Current Polymers, with and without Ageing. Materials 2021, 14, 3935. [Google Scholar] [CrossRef]
- Kordass, B. Editorial: Integration of CAD/CAM into dental education/Neue Approbationsordnung bietet Chancen für frühe CAD/CAM-Qualifikation. Int. J. Comput. Dent. 2019, 22, 303–304. [Google Scholar]
- Son, K.; Lee, K.B. Prediction of learning curves of 2 dental CAD software programs, part 2: Differences in learning effects by type of dental personnel. J. Prosthet. Dent. 2020, 123, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Burhardt, L.; Livas, C.; Kerdijk, W.; van der Meer, W.J.; Ren, Y. Treatment comfort, time perception, and preference for conventional and digital impression techniques: A comparative study in young patients. Am. J. Orthod. Dentofacial. Orthop. 2016, 150, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Burzynski, J.A.; Firestone, A.R.; Beck, F.M.; Fields, H.W., Jr.; Deguchi, T. Comparison of digital intraoral scanners and alginate impressions: Time and patient satisfaction. Am. J. Orthod. Dentofacial. Orthop. 2018, 153, 534–541. [Google Scholar] [CrossRef]
- Gallardo, Y.R.; Bohner, L.; Tortamano, P.; Pigozzo, M.N.; Lagana, D.C.; Sesma, N. Patient outcomes and procedure working time for digital versus conventional impressions: A systematic review. J. Prosthet. Dent. 2018, 119, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Mangano, A.; Beretta, M.; Luongo, G.; Mangano, C.; Mangano, F. Conventional vs. Digital Impressions: Acceptability, Treatment Comfort and Stress Among Young Orthodontic Patients. Open Dent. J. 2018, 12, 118–124. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| WORKFLOW | Company, City, Country | Technology | Specification, Software Version |
|---|---|---|---|
| Intraoral scan | 3Shape, Kopenhagen, Denmark | Ultrafast optical sectioning | Trios 3 color, Pod Version, Ver: Trios 2015-1 |
| CAD | exocad, Darmstadt, Germany | Dental CAD Designer with Bite Splint Module | DentalCAD 2016.10, Ver: Valetta 2.2, Matera 2.3 |
| CAM prestage | Autodesk, California, USA | Slicing software for additive manufacturing | Netfabb Premium 2018 Netfabb Premium 2019 |
| Additive manufacturing | W2P Engineering, Vienna, Austria | DLP, 385 nm, Flex-Vat | Solfex 650, Solflex 170 |
| VOCO, Cuxhaven, Germany | Resin: Dimethacrylat | V-Print Ortho |
| Task | N | 25th Percentile (h:m:s) | Median (h:m:s) | 75th Percentile (h:m:s) | Mean (min) | SD | Min. (min) | Max. (min) |
|---|---|---|---|---|---|---|---|---|
| #1 intraoralscan | 78 | 00:09:54 | 00:15:00 | 00:21:30 | 17.5 | 9.5 | 3 | 45 |
| #2 splint design | 69 | 01:30:00 | 02:00:00 | 02:38:00 | 132 | 65 | 40 | 420 |
| #3 finishing | - | not evaluated | ||||||
| #4 fitting of splint | 56 | 00:25:00 | 00:40:00 | 01:00:00 | 49 | 33 | 10 | 150 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kraemer-Fernandez, P.; Spintzyk, S.; Wahl, E.; Huettig, F.; Klink, A. Implementation of a Full Digital Workflow by 3D Printing Intraoral Splints Used in Dental Education: An Exploratory Observational Study with Respect to Students’ Experiences. Dent. J. 2023, 11, 5. https://doi.org/10.3390/dj11010005
Kraemer-Fernandez P, Spintzyk S, Wahl E, Huettig F, Klink A. Implementation of a Full Digital Workflow by 3D Printing Intraoral Splints Used in Dental Education: An Exploratory Observational Study with Respect to Students’ Experiences. Dentistry Journal. 2023; 11(1):5. https://doi.org/10.3390/dj11010005
Chicago/Turabian StyleKraemer-Fernandez, Pablo, Sebastian Spintzyk, Ebru Wahl, Fabian Huettig, and Andrea Klink. 2023. "Implementation of a Full Digital Workflow by 3D Printing Intraoral Splints Used in Dental Education: An Exploratory Observational Study with Respect to Students’ Experiences" Dentistry Journal 11, no. 1: 5. https://doi.org/10.3390/dj11010005