
Cross-Sectional Study on the Comparative Assessment of Mandibular Anesthesia (Inferior Alveolar Nerve Blockage) Manual Skills Shaping among Dentists on Plastic and Biomaterial Models


 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
- IIMT more than 155 points means a high level of stress, indicates a condition maladaptation and mental discomfort, the need to use a wide a range of means and methods for reducing neuropsychic tension, psychological relief, and changes in the style of thinking and life.
- IIMT in the range of 155–100 points means an average level of stress.
- Low-stress level (IIMT less than 99 points) indicates a state of psychological adaptation to workloads.
- to have filled and signed informed consent;
- dental specialists (students of dentistry faculty or practicing dentists);
- to have Lemyr-Tessier-Fillion PSM-25 test score more than 155.
- the participants wish to exclude their data;
- to have Lemyr-Tessier-Fillion PSM-25 test score less than 155.
- outcomes—marks for all 8 questions of Lickert scale from 1 to 5 mean;
- exposures—training course in IANB for dentists (two ways: cadavers and plastic models);
- potential confounders—the presence of previous successful experience in IANB in clinical practice (these participants were not included in final sample size of our research), gender, and age (participants were balanced according PSM-25, in this case these confounders had minimal effect);
- possible effect modifiers were not found.
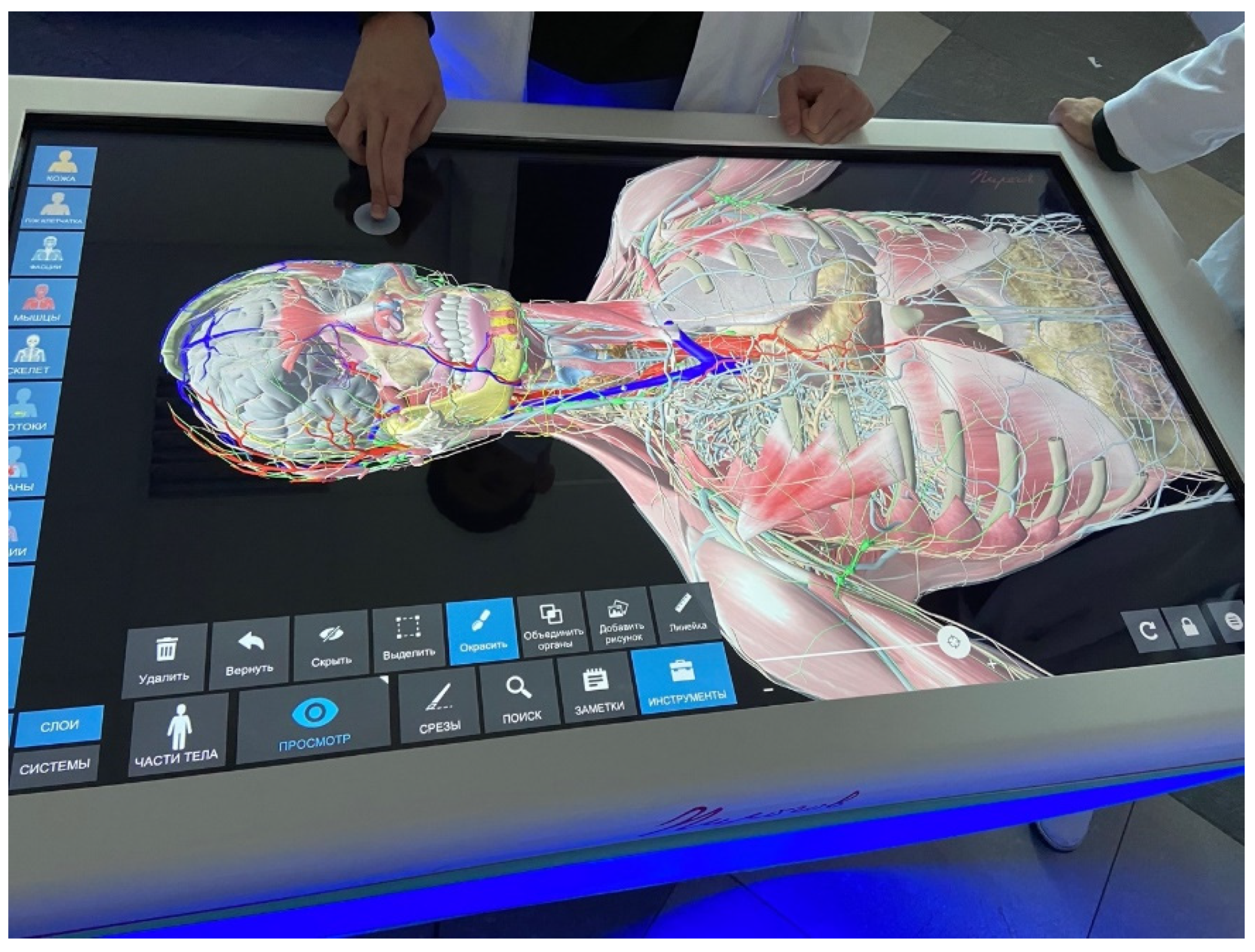
- Short lecture on clinical and anatomical guidelines for IANB: clinical anatomy of the maxillofacial area was presented at the interactive anatomical table «Pirogov» (LLC “Development”, Samara, Russia (Figure 1).
- Local anesthesia landmarks were explained at the skull: these landmarks are usually used during IANB. In presented study, the following technique was used: the condyle process, the angle of the mandible and the anterior edge of the mandible branch are determined by palpation. A triangle is formed between these points, in the middle of which the middle finger of the hand is moved, the location of which is projected onto the mandibular foramen.
- On a plastic model in the position of the open mouth, the participants palpate a standard protrusion simulating bone landmarks and perform an injection from the opposite side of the found point. The participants were asked to use a standardized model for performing IANB (Energiyalab, Moscow, Russia). This model is equipped with a cartridge dental syringe with a needle, a lithium battery, an electrical wiring system, and sensors built into the model. If the technique is performed correctly, a green light signal lights up; if it is incorrect, a red light signal lights up (Figure 2).
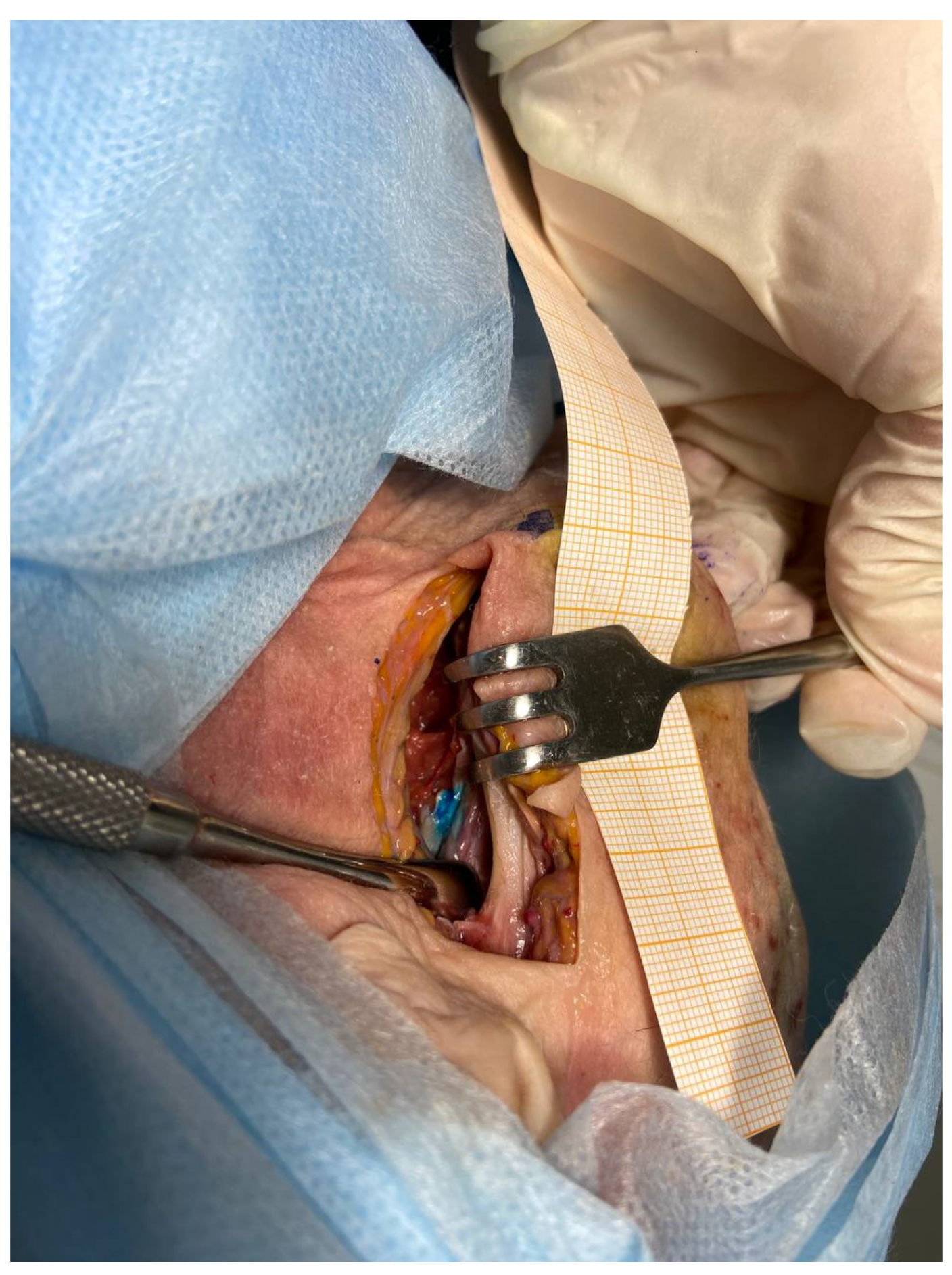
- In the group where the training was provided on the cadavers, the participants determined individual guidelines according to which local anesthesia was performed. Then, the mouth was opened on the cadavers and fixed with a mouth expander. The participants performed intraoral palpation to clarify the injection point and injected from the opposite side in the direction of the finger installed outside the mandible branch. When the inner surface of the mandible branch was reached, an aspiration test was performed an, if not - a local anesthetic solution is injected at a rate of 1 mL per minute.
3. Results
- there was a statistically significant higher rate for satisfaction with participation in the training for cadaver education (9.5 times, p-value < 0.001);
- realization of expectations with training for cadaver was seven times more for cadaver education (p-value < 0.001);
- training organization satisfaction level was 1.2 times higher for cadaver education (p-value > 0.05, with Yates correction);
- education methodology satisfaction was 1.4 times higher for cadaver course (p-value < 0.001);
- expectations with education methodology were 2.2 times higher for cadaver course participants (p-value < 0.001);
- educational value of education methodology was 1.9 times higher for cadaver training (p-value < 0.001);
- manual-skill shaping by education methodology was 3.4 times higher for cadaver IANB training (p-value < 0.001);
- tutor satisfaction was 2 times higher for cadaver-training skills than for plastic models (p-value < 0.001).
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramazani, N.; Iranmanesh, S.M. Dental Students’ Preference with Regard to Tactile or Visual Determination of Injection Site for an Inferior Alveolar Nerve Block in Children: A Crossover Randomized Clinical Trial. J. Dent. 2016, 13, 40–48. [Google Scholar]
- Jadu, F.M.; Jan, A.M.; Mohamed, K.M.; Abdel-Alim, H.M.; Bayoumi, A.M. Impact of Methods for Teaching Inferior Alveolar Nerve Block Anesthesia on Dental Students’ Efficiency. World J. Dent. 2019, 10, 374–378. [Google Scholar] [CrossRef]
- Senese, O.; Blaise, K. Risks posed by bilateral inferior alveolar nerve block: Myth or reality? Adv. Oral Maxillofac. Surg. 2021, 2, 100042. [Google Scholar] [CrossRef]
- Antanavičienė, G.; Zaleckytė, M.; Narbutaitė, J. Stress and associated factors among dentists. Stomatologija 2020, 22, 44–48. [Google Scholar] [PubMed]
- Vasil’ev, Y.L.; Rabinovich, S.A.; Dydykin, S.S.; Bogoyavlenskaya, T.A.; Kashtanov, A.D.; Kuznetsov, A.I. Evaluation of dentists regulatory systems stress during the provision of dental care according to pulse oximetry data. Stomatologiya 2020, 99, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Rabinovich, S.A.; Razumova, S.N.; Vasil’ev, Y.L. Functional cardiovascular assessment in dentists performing local anesthesia in out-patient settings. Stomatologiya 2017, 96, 20–22. [Google Scholar] [CrossRef] [PubMed]
- Nicola, S.; Virag, I.; Stoicu-Tivadar, L. VR Medical Gamification for Training and Education. Stud. Health Technol. Inform. 2017, 236, 97–103. [Google Scholar]
- Mazgelytė, E.; Rekienė, V.; Dereškevičiūtė, E.; Petrėnas, T.; Songailienė, J.; Utkus, A.; Chomentauskas, G.; Karčiauskaitė, D. Effects of Virtual Reality-Based Relaxation Techniques on Psychological, Physiological, and Biochemical Stress Indicators. Healthcare 2021, 9, 1729. [Google Scholar] [CrossRef]
- Meese, M.M.; O’Hagan, E.C.; Chang, T.P. Healthcare Provider Stress and Virtual Reality Simulation: A Scoping Review. Simul. Healthc. 2021, 16, 268–274. [Google Scholar] [CrossRef]
- Liaw, S.Y.; Sutini Chua, W.L.; Tan, J.Z.; Levett-Jones, T.; Ashokka, B.; Te Pan, T.L.; Lau, S.T.; Ignacio, J. Desktop Virtual Reality Versus Face-to-Face Simulation for Team-Training on Stress Levels and Performance in Clinical Deterioration: A Randomised Controlled Trial. J. Gen. Intern. Med. 2022, 1, 1–7. [Google Scholar] [CrossRef]
- Wong, G.; Apthorpe, H.C.; Ruiz, K.; Nanayakkara, S. A Tale of Two Teaching Methods: Students’ Clinical Perspectives on Administering Dental Local Anesthetics. J. Dent. Educ. 2020, 84, 166–175. [Google Scholar] [CrossRef]
- Moussa, R.; Alghazaly, A.; Althagafi, N.; Eshky, R.; Borzangy, S. Effectiveness of Virtual Reality and Interactive Simulators on Dental Education Outcomes: Systematic Review. Eur. J. Dent. 2022, 16, 14–31. [Google Scholar] [CrossRef]
- Collaço, E.; Kira, E.; Sallaberry, L.H.; Queiroz, A.C.M.; Machado, M.A.A.M.; Crivello, O., Jr.; Tori, R. Immersion and haptic feedback impacts on dental anesthesia technical skills virtual reality training. J. Dent. Educ. 2021, 85, 589–598. [Google Scholar] [CrossRef]
- Huri, G.; Gülşen, M.R.; Karmış, E.B.; Karagüven, D. Cadaver versus simulator based arthroscopic training in shoulder surgery. Turk. J. Med. Sci. 2021, 51, 1179–1190. [Google Scholar] [CrossRef]
- Stefanidis, D.; Yonce, T.C.; Green, J.M.; Coker, A.P. Cadavers versus pigs: Which are better for procedural training of surgery residents outside the OR? Surgery 2013, 154, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra, D.; Markus, A.F. Emerging simulation technologies in global craniofacial surgical training. J. Oral Biol. Craniofac. Res. 2021, 11, 486–499. [Google Scholar] [CrossRef]
- Meneas, C.G.; Abro, S.; Yangni-Angate, K.H. Training in cardiac surgery using human cadavers: Effectiveness of “Silent Teachers”. J. Card. Surg. 2019, 34, 181–185. [Google Scholar] [CrossRef]
- Haji, Z.; Arif, A.; Jamal, S.; Ghafoor, R. Augmented reality in clinical dental training and education. J. Pak. Med. Assoc. 2021, 71 (Suppl. S1), S42–S48. [Google Scholar]
- Joshi, A.; Kale, S.; Chandel, S.; Pal, D.K. Likert Scale: Explored and Explained. Curr. J. Appl. Sci. Technol. 2015, 7, 396–403. [Google Scholar] [CrossRef]
- Chu, A.K.; Law, R.W.; Greschner, J.M.; Hyer, C.F. Effectiveness of the cadaver lab in podiatric surgery residency programs. J. Foot Ankle Surg. 2020, 59, 246–252. [Google Scholar] [CrossRef]
- Leszczynski, P.; Charuta, A.; Zacharuk, T. Cadaver as an educational tool increasing the effectiveness of Combat Application Tourniquet use in extremity injuries. Ulus Travma Acil Cerrahi Derg. 2021, 27, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Estai, M.; Bunt, S. Best teaching practices in anatomy education: A critical review. Ann. Anat. 2016, 208, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Sawhney, C.; Lalwani, S.; Ray, B.R.; Sinha, S.; Kumar, A. Benefits and pitfalls of cadavers as a learning tool for ultrasound-guided regional anesthesia. Anesth. Essays Res. 2017, 11, 3–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Hu, J. A review of haptic simulator for oral and maxillofacial surgery based on virtual reality. Expert Rev. Med. Devices 2018, 15, 435–444. [Google Scholar] [CrossRef]
- Lone, M.; McKenna, J.P.; Balta, J.Y.; O’Mahony, S.M.; Cryan, J.F.; Downer, E.J.; Toulouse, A. Assessment of thiel-embalmed cadavers as a teaching tool for oral anatomy and local anesthesia. J. Dent. Educ. 2017, 81, 420–426. [Google Scholar] [CrossRef]
- Kennel, L.; Martin, D.M.A.; Shaw, H.; Wilkinson, T. Learning anatomy through Thiel- vs. formalin-embalmed cadavers: Student perceptions of embedding methods and effect on functional anatomy knowledge. Anat. Sci. Educ. 2018, 11, 166–174. [Google Scholar] [CrossRef]
- Sankova, M.V.; Kytko, O.V.; Vasil’ev, Y.L.; Aleshkina, Y.O.; Diachkova, Y.E.; Darawsheh, H.M.; Kolsanov, A.V.; Dydykin, S.S. Medical Students’ Reactive Anxiety as a Quality Criterion for Distance Learning during the SARS-COV-2 Pandemic. Emerg. Sci. J. 2021, 5, 86–93. [Google Scholar] [CrossRef]
- Feigl, G.; Sammer, A. The influence of dissection on clinical anatomical knowledge for surgical needs. Surg. Radiol. Anat. 2022, 44, 9–14. [Google Scholar] [CrossRef]
- Asante, E.A.; Maalman, R.S.; Ali, M.A.; Donkor, Y.O.; Korpisah, J.K. Perception and Attitude of Medical Students towards Cadaveric Dissection in Anatomical Science Education. Ethiop. J. Health Sci. 2021, 31, 867–874. [Google Scholar] [CrossRef]
- Hocine, M.N.; Bouziad, K.A.; Légeron, P.; Dab, W.; Saporta, G. How to identify and prioritize psychosocial factors impacting stress level. PLoS ONE 2016, 11, e0157078. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scale | “Excellent”, n (%) | “Good”, n (%) | “Satisfactory”, n (%) | “Satisfactory”, n (%) | “Poor”, n (%) |
|---|---|---|---|---|---|
| Satisfaction with participation in the program | 164 (54.8%) | 117 (39.1%) | 18 (6%) | 0 | 0 |
| Expectations with training | 192 (64.2%) | 92 (30.8%) | 15 (5%) | 0 | 0 |
| Training organization satisfaction | 137 (45.8%) | 147 (49.2%) | 15 (5%) | 0 | 0 |
| Education methodology satisfaction | 149 (49.8%) | 146 (48.8%) | 4 (1.3%) | 0 | 0 |
| Expectations with education methodology | 254 (74.9%) | 28 (9.4%) | 17 (5.7%) | 0 | 0 |
| Educational value of education methodology | 224 (74.9%) | 75 (25.1%) | 0 | 0 | 0 |
| Manual-skill shaping by education methodology | 239 (79.9%) | 60 (20.1%) | 0 | 0 | 0 |
| Tutor satisfaction | 253 (84.6%) | 46 (15.4%) | 0 | 0 | 0 |
| Scale | “Excellent”, n (%) | “Good”, n (%) | “Satisfactory”, n (%) | “Poor”, n (%) | “Awful”, n (%) |
|---|---|---|---|---|---|
| Satisfaction with participation in the training | 17 (5.7%) | 248 (82.9%) | 34 (11.4%) | 0 | 0 |
| Expectations with training | 27 (9.1%) | 259 (86.6%) | 13 (4.3%) | 0 | 0 |
| Training organization satisfaction | 113 (37.7%) | 170 (56.6%) | 15 (5.1%) | 1 (0.6%) | 0 |
| Education methodology satisfaction | 107 (35.7%) | 150 (50.3%) | 42 (14%) | 0 | 0 |
| Expectations with education methodology | 118 (39.4%) | 154 (51.4%) | 15 (4.9%) | 12 (4.3%) | 0 |
| Educational value of education methodology | 117 (39.1%) | 169 (56.6%) | 13 (4.3%) | 0 | 0 |
| Manual-skill shaping by education methodology | 71 (23.7%) | 228 (76.3%) | 0 | 0 | 0 |
| Tutor satisfaction | 128 (46%) | 161 (54%) | 0 | 0 | 0 |
| Questions | Comparison Group M ± SD Median Min–Max | Main Group M ± SD Median Min–Max | Significance of Differences (Mann–Whitney Test), Significance Level |
|---|---|---|---|
| Satisfaction with participation in the program | 3.93 ± 0.41 4 3–5 | 4.49 ± 0.61 4.4 3–5 | p < 0.001 |
| Expectations with training | 4.05 ± 0.36 4 3–5 | 4.59 ± 0.59 4.4 3–5 | p < 0.001 |
| Education methodology satisfaction | 4.22 ± 0.67 4 3–5 | 4.48 ± 0.53 4.4 3–5 | + p < 0.001 |
| Expectations regarding educational methods | 4.26 ± 0.74 4 2–5 | 4.79± 0.53 4.5 3–5 | p < 0.001 |
| Training organization satisfaction | 4.31 ± 0.59 4 2–5 | 4.41 ± 0.59 4.4 3–5 | p > 0.05 |
| Educational value of education methodology | 4.35 ± 0.56 4 3–5 | 4.75 ± 0.43 4.5 4–5 | p < 0.001 |
| Manual-skill shaping by education methodology | 4.24 ± 0.43 4.4 4–5 | 4.8 ± 0.4 4.5 4–5 | p < 0.001 |
| Educator satisfaction | 4.46 ± 0.5 4.4 4–5 | 4.85 ± 0.36 4.5 4–5 | p < 0.001 |
| General satisfaction | 33.94 ± 1.87 32 26–38 | 37.16 ± 2.01 35.5 31–40 | p < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vasil’ev, Y.; Diachkova, E.; Darawsheh, H.; Kashtanov, A.; Molotok, E.; Volel, B.; Batov, A.; Kytko, O.; Saleev, R.; Saleeva, G.; et al. Cross-Sectional Study on the Comparative Assessment of Mandibular Anesthesia (Inferior Alveolar Nerve Blockage) Manual Skills Shaping among Dentists on Plastic and Biomaterial Models. Dent. J. 2022, 10, 124. https://doi.org/10.3390/dj10070124
Vasil’ev Y, Diachkova E, Darawsheh H, Kashtanov A, Molotok E, Volel B, Batov A, Kytko O, Saleev R, Saleeva G, et al. Cross-Sectional Study on the Comparative Assessment of Mandibular Anesthesia (Inferior Alveolar Nerve Blockage) Manual Skills Shaping among Dentists on Plastic and Biomaterial Models. Dentistry Journal. 2022; 10(7):124. https://doi.org/10.3390/dj10070124
Chicago/Turabian StyleVasil’ev, Yuriy, Ekaterina Diachkova, Hadi Darawsheh, Artem Kashtanov, Ekaterina Molotok, Beatrice Volel, Artem Batov, Olesya Kytko, Rinat Saleev, Gulshat Saleeva, and et al. 2022. "Cross-Sectional Study on the Comparative Assessment of Mandibular Anesthesia (Inferior Alveolar Nerve Blockage) Manual Skills Shaping among Dentists on Plastic and Biomaterial Models" Dentistry Journal 10, no. 7: 124. https://doi.org/10.3390/dj10070124