

Marginal Fit of Porcelain Laminate Veneer Materials under Thermocycling Condition: An In-Vitro Study
 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Tooth Collection and Grouping
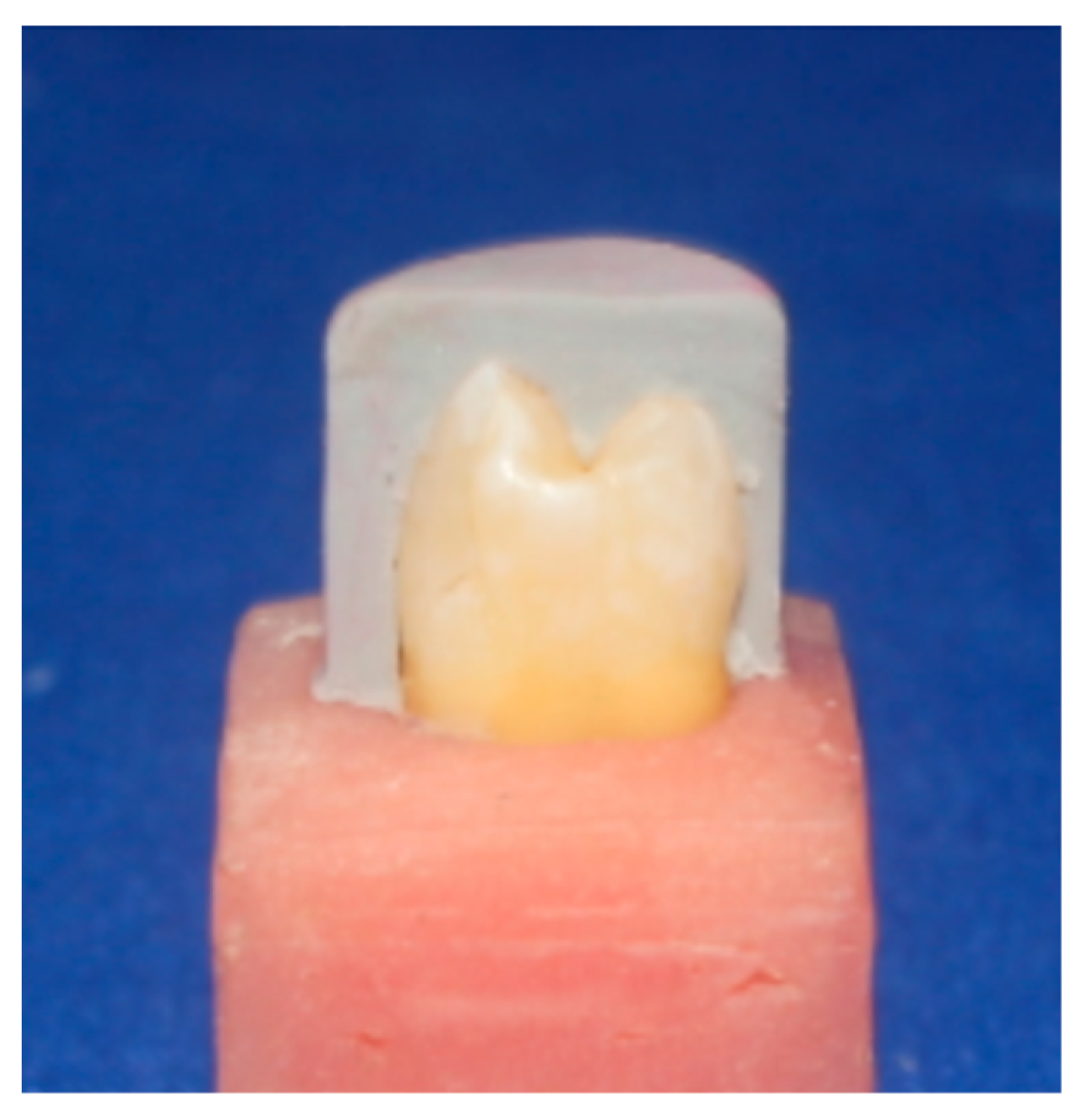
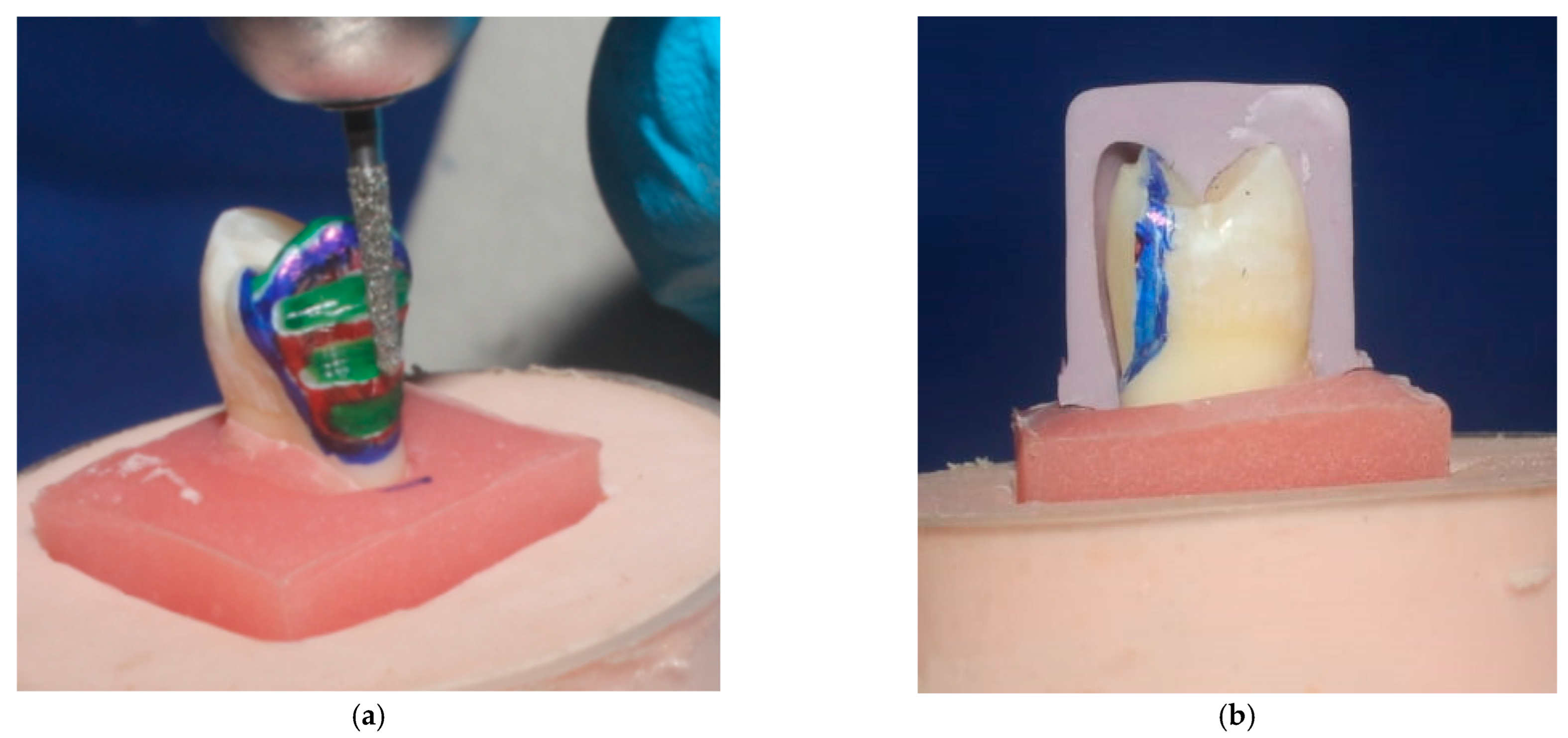
2.2. Veneer Preparation Procedure
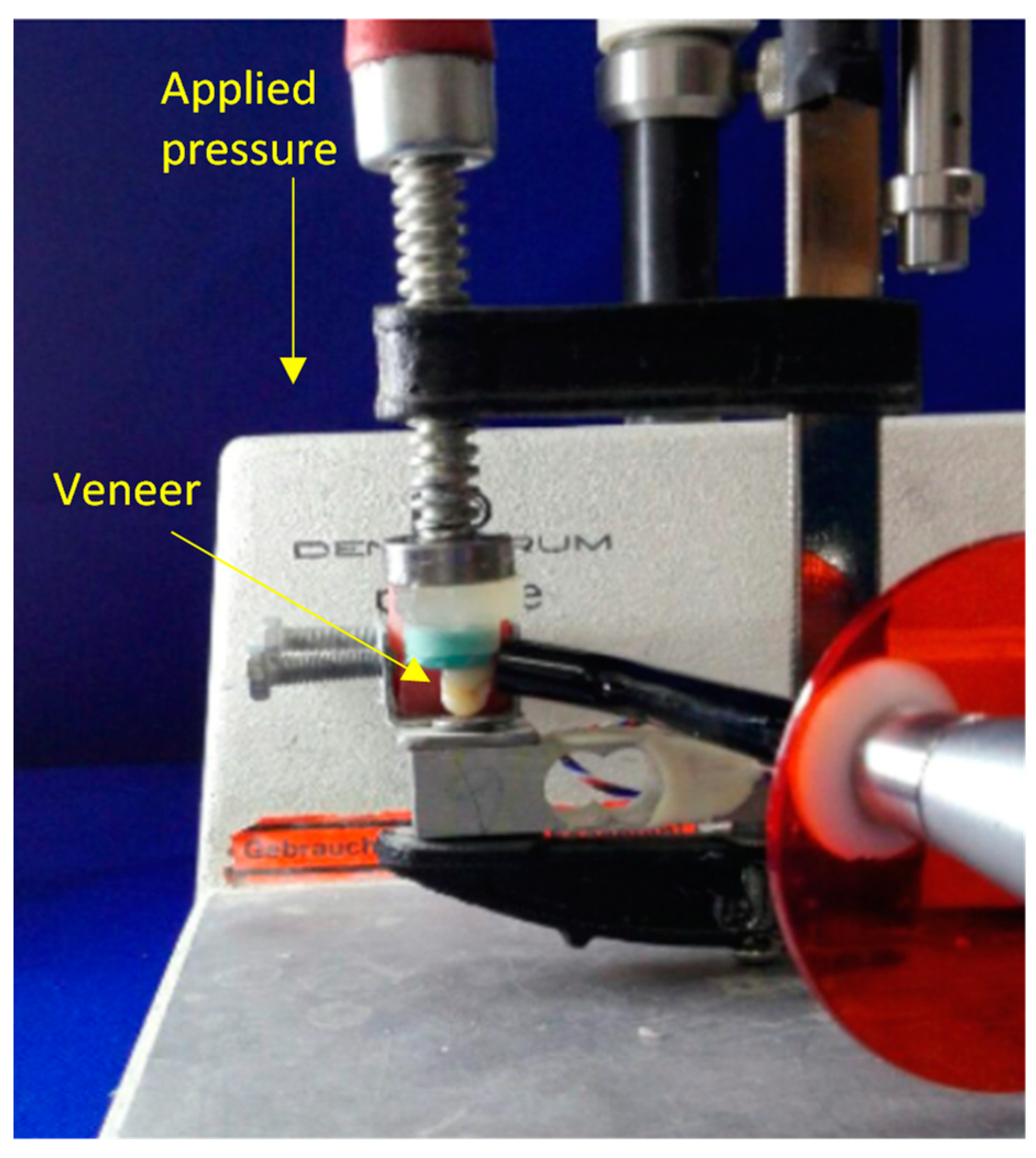
2.3. Cementation of Veneer
2.4. Thermocycling Procedure
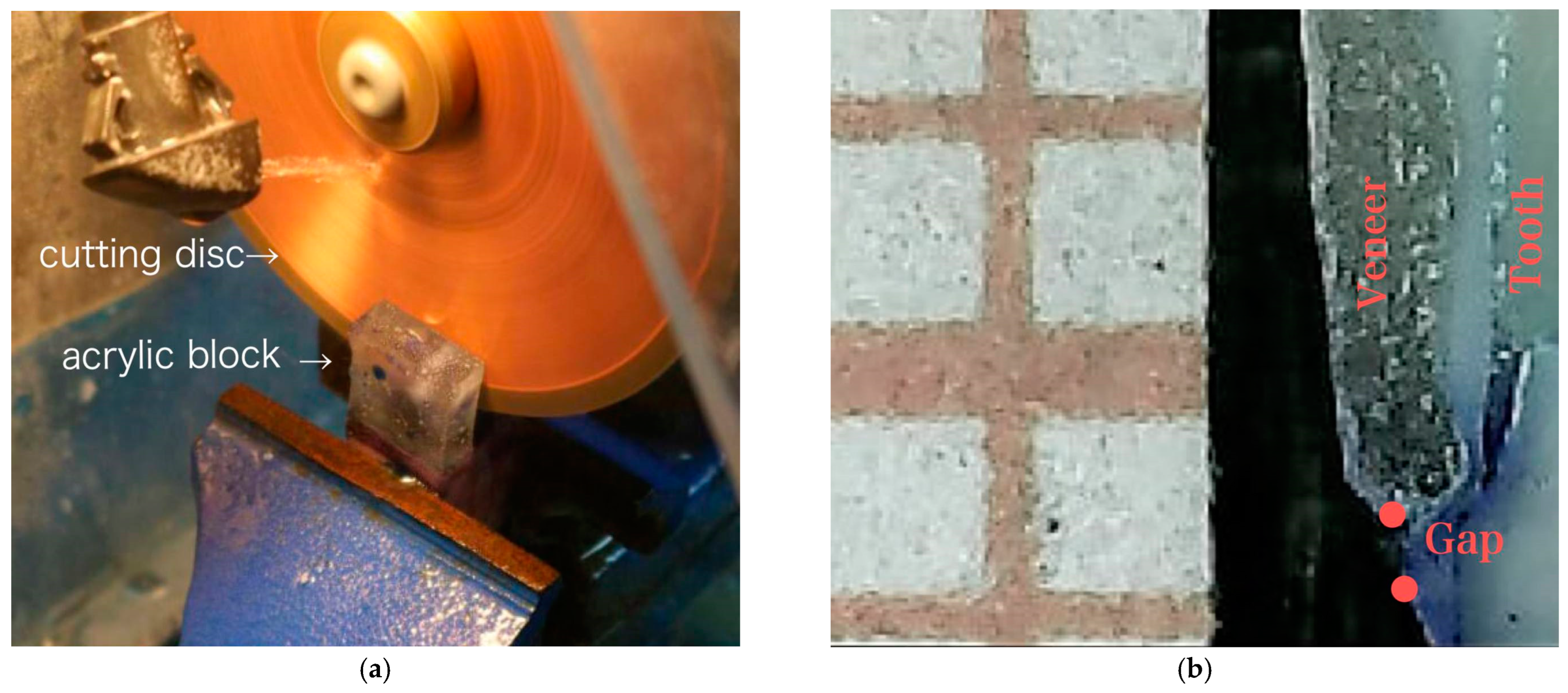
2.5. Marginal Fit Evaluation Procedure
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Calamia, J.R.; Calamia, C.S. Porcelain Laminate Veneers: Reasons for 25 Years of Success. Dent. Clin. N. Am. 2007, 51, 399–417. [Google Scholar] [CrossRef]
- Terta, H.S.; Dündarb, M.; Öztürka, B. The effect of various preparation designs on the survival of porcelain laminate veneers. Margin 2009, 26, 38. [Google Scholar]
- Fasbinder, D.J.; Dennison, J.B.; Heys, D.; Neiva, G. A Clinical Evaluation of Chairside Lithium Disilicate CAD/CAM Crowns. J. Am. Dent. Assoc. 2010, 141, 10S–14S. [Google Scholar] [CrossRef]
- Hanoon, Z.A.; Aljuboury, M.R. Microleakage of Two Porcelain Laminate Veneer Materials with Different Types of Class V Cavity Restoration (A Comparative In-vitro Study). Int. J. Med. Res. Health Sci. 2018, 7, 71–76. [Google Scholar]
- Holmes, J.R.; Bayne, S.C.; Holland, G.A.; Sulik, W.D. Considerations in measurement of marginal fit. J. Prosthet. Dent. 1989, 62, 405–408. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, M.S.; Windeler, A.S. An investigation of dental luting cement solubility as a function of the marginal gap. J. Prosthet. Dent. 1991, 65, 436–442. [Google Scholar] [CrossRef]
- Wolfart, S.; Wegner, S.M.; Al-Halabi, A.; Kern, M. Clinical evaluation of marginal fit of a new experimental all-ceramic system before and after cementation. Int. J. Prosthodont. 2003, 16, 587–592. [Google Scholar] [PubMed]
- Pak, H.-S.; Han, J.-S.; Lee, J.-B.; Kim, S.-H.; Yang, J.-H. Influence of porcelain veneering on the marginal fit of Digident and Lava CAD/CAM zirconia ceramic crowns. J. Adv. Prosthodont. 2010, 2, 33–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felton, D.A.; Kanoy, B.E.; Bayne, S.C.; Wirthman, G.P. Effect of in vivo crown margin discrepancies on periodontal health. J. Prosthet. Dent. 1991, 65, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Reich, S.; Gozdowski, S.; Trentzsch, L.; Frankenberger, R.; Lohbauer, U. Marginal Fit of Heat-pressed vs CAD/CAM Processed All-ceramic Onlays Using a Milling Unit Prototype. Oper. Dent. 2008, 33, 644–650. [Google Scholar] [CrossRef] [Green Version]
- Boeddinghaus, M.; Breloer, E.S.; Rehmann, P.; Wöstmann, B. Accuracy of single-tooth restorations based on intraoral digital and conventional impressions in patients. Clin. Oral Investig. 2015, 19, 2027–2034. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, S.; Shinya, A.; Kuroda, S.; Gomi, H. The accuracy of the CAD system using intraoral and extraoral scanners for designing of fixed dental prostheses. Dent. Mater. J. 2017, 36, 402–407. [Google Scholar] [CrossRef]
- Tabata, L.F.; de Lima Silva, T.A.; de Paula Silveira, A.C.; Ribeiro, A.P.D. Marginal and internal fit of CAD-CAM composite resin and ceramic crowns before and after internal adjustment. J. Prosthet. Dent. 2020, 123, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Neves, F.D.; Prado, C.J.; Prudente, M.S.; Carneiro, T.A.; Zancope, K.; Davi, L.R.; Mendonca, G.; Cooper, L.F.; Soares, C.J. Micro-computed tomography evaluation of marginal fit of lithium disilicate crowns fabricated by using chairside CAD/CAM systems or the heat-pressing technique. J. Prosthet. Dent. 2014, 112, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- de Paula Silveira, A.C.; Chaves, S.B.; Hilgert, L.A.; Ribeiro AP, D. Marginal and internal fit of CAD-CAM-fabricated composite resin and ceramic crowns scanned by 2 intraoral cameras. J. Prosthet. Dent. 2017, 117, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Mathew, C.; Mathew, S.; Karthik, K. A review on ceramic laminate veneers. J. Indian Acad. Dent. Spec. Res. 2010, 1, 33–37. [Google Scholar]
- Saker, S.; Özcan, M. Marginal discrepancy and load to fracture of monolithic zirconia laminate veneers: The effect of preparation design and sintering protocol. Dent. Mater. J. 2021, 40, 331–338. [Google Scholar] [CrossRef]
- Chieffi, N.; Chersoni, S.; Papacchini, F.; Vano, M.; Goracci, C.; Davidson, C.L.; Tay, F.R.; Ferrari, M. The effect of application sustained seating pressure on adhesive luting procedure. Dent. Mater. 2007, 23, 159–164. [Google Scholar] [CrossRef]
- Zortuk, M.; Bolpaca, P.; Kilic, K.; Ozdemir, E.; Aguloglu, S. Effects of Finger Pressure Applied by Dentists during Cementation of All-Ceramic Crowns. Eur. J. Dent. 2010, 04, 383–388. [Google Scholar] [CrossRef] [Green Version]
- Kunii, J.; Hotta, Y.; Tamaki, Y.; Ozawa, A.; Kobayashi, Y.; Fujishima, A.; Miyazaki, T.; Fujiwara, T. Effect of Sintering on the Marginal and Internal Fit of CAD/CAM-fabricated Zirconia Frameworks. Dent. Mater. J. 2007, 26, 820–826. [Google Scholar] [CrossRef] [Green Version]
- Good, M.-L.; Mitchell, C.A.; Pintado, M.R.; Douglas, W.H. Quantification of all-ceramic crown margin surface profile from try-in to 1-week post-cementation. J. Dent. 2009, 37, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Aboushelib, M.N.; Elmahy, W.A.; Ghazy, M.H. Internal adaptation, marginal accuracy and microleakage of a pressable versus a machinable ceramic laminate veneers. J. Dent. 2012, 40, 670–677. [Google Scholar] [CrossRef] [PubMed]
- Anadioti, E. Internal and Marginal Fit of Pressed and Cad Lithium Disilicate Crowns Made from Digital and Conventional Impressions; The University of Iowa: Iowa City, IA, USA, 2013. [Google Scholar] [CrossRef]
- Bakar, W.Z.W.; Chee, H.T.; Ab Ghani, Z.; Amaechi, B.T. Comparison of composite resin and porcelain inlays for restoration of noncarious cervical lesions: An In vitro study. Dent. Res. J. 2018, 15, 215–219. [Google Scholar] [CrossRef]
- Al-Hawwaz, Z.M.; Ibraheem, A.F. Marginal and internal fitness of full contour CAD/CAM fabricated zirconia crowns using different digital intra-oral scanners (an in vitro study). JPAM 2018, 12, 839–844. [Google Scholar] [CrossRef]
- Gresnigt, M.M.M.; Kalk, W.; Ozcan, M. Randomized Clinical Trial of Indirect Resin Composite and Ceramic Veneers: Up to 3-year Follow-up. J. Adhes. Dent. 2013, 15, 181–190. [Google Scholar] [CrossRef]
- Pedroche, L.O.; Bernardes, S.R.; Leão, M.P.; Kintopp, C.C.D.A.; Correr, G.; Ornaghi, B.P.; Gonzaga, C.C. Marginal and internal fit of zirconia copings obtained using different digital scanning methods. Braz. Oral Res. 2016, 30, e113. [Google Scholar] [CrossRef] [Green Version]
- Fadhil, N.H.; Khaliq, A.G.A.; Najim, B.E.-S.; DS, M.I.A. Evaluation of Marginal and Internal Adaptation of CAD/CAM and Pressable Ceramic Veneers of Different Preparation Designs Using Silicone Replica Technique:(A Comparative In Vitro Study). Int. J. Sci. Res. 2017, 6, 2222–2227. [Google Scholar]
- Cherukara, G.; Seymour, K.; Samarawickrama, D.; Zou, L. A study into the variations in the labial reduction of teeth prepared to receive porcelain veneers—A comparison of three clinical techniques. Br. Dent. J. 2002, 192, 401. [Google Scholar] [CrossRef]
- Mizrahi, B. Porcelain veneers: Techniques and precautions. Wear 2007, 1, 4. [Google Scholar]
- Radz, G.M. Minimum Thickness Anterior Porcelain Restorations. Dent. Clin. N. Am. 2011, 55, 353–370. [Google Scholar] [CrossRef]
- Lesage, B. Establishing a classification system and criteria for veneer preparations. Compend. Contin. Educ. Dent. 2013, 34, 104–107. [Google Scholar] [PubMed]
- Khaliq, A.G.A.; Al-Rawi, I.I. Fracture strength of laminate veneers using different restorative materials and techniques (A comparative in vitro study). J. Baghdad Coll. Dent. 2014, 26, 1–8. [Google Scholar] [CrossRef]
- Touati, B.; Miara, P.; Nathanson, D. Esthetic dentistry and ceramic restorations. Br. Dent. J. 1999, 186, 533. [Google Scholar]
- Archangelo, C.M.; Rocha, E.P.; Anchieta, R.B.; Martin, M.; Freitas, A.C.; Ko, C.-C.; Cattaneo, P.M. Influence of buccal cusp reduction when using porcelain laminate veneers in premolars. A comparative study using 3-D finite element analysis. J. Prosthodont. Res. 2011, 55, 221–227. [Google Scholar] [CrossRef] [Green Version]
- Matsumura, H.; Aida, Y.; Ishikawa, Y.; Tanoue, N. Porcelain laminate veneer restorations bonded with a three-liquid silane bonding agent and a dual-activated luting composite. J. Oral Sci. 2006, 48, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Shafiei, F.; Memarpour, M.; Jowkar, Z. Marginal sealing of a porcelain laminate veneer luted with three different resin cements on fluorosed teeth. Int. J. Esthet. Dent. 2017, 12, 60–71. [Google Scholar]
- Stamatacos, C.; Simon, J.F. Cementation of indirect restorations: An overview of resin cements. Compend. Contin. Educ. Dent. 2013, 34, 42–44. [Google Scholar] [PubMed]
- Blatz, M.B.; Sadan, A.; Kern, M. Resin-ceramic bonding: A review of the literature. J. Prosthet. Dent. 2003, 89, 268–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yüksel, E.; Zaimoğlu, A. Influence of marginal fit and cement types on microleakage of all-ceramic crown systems. Braz. Oral Res. 2011, 25, 261–266. [Google Scholar] [CrossRef]
- D’Arcangelo, C.; De Angelis, F.; Vadini, M.; D’Amario, M. Clinical evaluation on porcelain laminate veneers bonded with light-cured composite: Results up to 7 years. Clin. Oral Investig. 2012, 16, 1071–1079. [Google Scholar] [CrossRef]
- Cenci, M.; Pereira-Cenci, T.; Donassollo, T.A.; Sommer, L.; Strapasson, A.; Demarco, F.F. Influence of thermal stress on marginal integrity of restorative materials. J. Appl. Oral Sci. 2008, 16, 106–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Versluis, A.; Tantbirojn, D.; Lee, M.S.; Tu, L.S.; DeLong, R. Can hygroscopic expansion compensate polymerization shrinkage? Part I. Deformation of restored teeth. Dent. Mater. 2011, 27, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Sadighpour, L.; Geramipanah, F.; Allahyari, S.; Fallahi Sichani, B.; Kharazi Fard, M.J. In vitro evaluation of the fracture resistance and microleakage of porcelain laminate veneers bonded to teeth with composite fillings after cyclic loading. J. Adv. Prosthodont. 2014, 6, 278–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loguercio, A.D.; Reis, A.; Ballester, R.Y. Polymerization shrinkage: Effects of constraint and filling technique in composite restorations. Dent. Mater. 2004, 20, 236–243. [Google Scholar] [CrossRef]
- Eden, E.; Topaloglu-Ak, A.; Topaloglu-Ak, V.; Cuijpers, V.; E Frencken, J. Micro-CT for measuring marginal leakage of Class II resin composite restorations in primary molars prepared in vivo. Am. J. Dent. 2008, 21, 393–397. [Google Scholar]
- Makarewicz, D.; Le Bell-Rönnlöf, A.-M.; Lassila, L.V.; Vallittu, P.K. Effect of Cementation Technique of Individually Formed Fiber-Reinforced Composite Post on Bond Strength and Microleakage. Open Dent. J. 2013, 7, 68–75. [Google Scholar] [CrossRef]
- Riccitiello, F.; Amato, M.; Leone, R.; Spagnuolo, G.; Sorrentino, R. In vitro Evaluation of the Marginal Fit and Internal Adaptation of Zirconia and Lithium Disilicate Single Crowns: Micro-CT Comparison Between Different Manufacturing Procedures. Open Dent. J. 2018, 12, 160–172. [Google Scholar] [CrossRef] [Green Version]
- Pelekanos, S.; Koumanou, M.; Koutayas, S.-O.; Zinelis, S.; Eliades, G. Micro-CT evaluation of the marginal fit of different In-Ceram alumina copings. Eur. J. Esthet. Dent. 2009, 4, 278–292. [Google Scholar]
- Nejatian, T.; Holliday, R.; Wassell, R. Material Choice. In Extra-Coronal Restorations; Springer: Berlin/Heidelberg, Germany, 2019; pp. 163–205. [Google Scholar]
- Raptis, N.V.; Michalakis, K.X.; Hirayama, H. Optical behavior of current ceramic systems. Int. J. Periodontics Restor. Dent. 2006, 26. [Google Scholar]
- Ma, L.; Guess, P.C.; Zhang, Y. Load-bearing properties of minimal-invasive monolithic lithium disilicate and zirconia occlusal onlays: Finite element and theoretical analyses. Dent. Mater. 2013, 29, 742–751. [Google Scholar] [CrossRef] [Green Version]
- Sannino, G.; Germano, F.; Arcuri, L.; Bigelli, E.; Arcuri, C.; Barlattani, A. CEREC CAD/CAM Chairside System. Oral Implant. 2014, 7, 57–70. [Google Scholar]
- Lin, T.-M.; Liu, P.-R.; Ramp, L.C.; Essig, M.E.; Givan, D.A.; Pan, Y.-H. Fracture resistance and marginal discrepancy of porcelain laminate veneers influenced by preparation design and restorative material in vitro. J. Dent. 2012, 40, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Hekimoǧlu, C.; Anil, N.; Yalçin, E. A microleakage study of ceramic laminate veneers by autoradiography: Effect of incisal edge preparation. J. Oral Rehabil. 2004, 31, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Soares-Rusu, I.; Villavicencio-Espinoza, C.; de Oliveira, N.; Wang, L.; Honório, H.; Rubo, J.; Francisconi, P.; Borges, A. Clinical evaluation of lithium disilicate veneers manufactured by CAD/CAM compared with heat-pressed methods: Randomized controlled clinical trial. Oper. Dent. 2021, 46, 4–14. [Google Scholar] [CrossRef]
- Basheer, R.; Elsayed, S.; Bahgat, S. Assessment of Accuracy of Different Cad/Cam Fabricated Porcelain Laminate Veneers. Egypt. Dent. J. 2017, 63, 3767–3782. [Google Scholar] [CrossRef]
- El-Damanhoury, H.; Haj-Ali, R.; Platt, J. Fracture Resistance and Microleakage of Endocrowns Utilizing Three CAD-CAM Blocks. Oper. Dent. 2015, 40, 201–210. [Google Scholar] [CrossRef] [Green Version]
- Haralur, S.B. Microleakage of porcelain laminate veneers cemented with different bonding techniques. J. Clin. Exp. Dent. 2018, 10, e166–e171. [Google Scholar] [CrossRef]
- Stacey, G.D. A shear stress analysis of the bonding of porcelain veneers to enamel. J. Prosthet. Dent. 1993, 70, 395–402. [Google Scholar] [CrossRef]
- Davidson, C.; De Gee, A.; Feilzer, A. The Competition between the Composite-Dentin Bond Strength and the Polymerization Contraction Stress. J. Esthet. Restor. Dent. 2000, 12, 51. [Google Scholar] [CrossRef]
- Pozzi, A.; Tallarico, M.; Barlattani, A. Monolithic Lithium Disilicate Full-Contour Crowns Bonded on CAD/CAM Zirconia Complete-Arch Implant Bridges With 3 to 5 Years of Follow-Up. J. Oral Implant. 2015, 41, 450–458. [Google Scholar] [CrossRef]
- Fabianelli, A.; Pollington, S.; Davidson, C.L.; Cagidiaco, M.C.; Goracci, C. The relevance of microleakage studies. Int. Dent. SA 2007, 9, 64–74. [Google Scholar]
- Zarone, F.; Epifania, E.; Leone, G.; Sorrentino, R.; Ferrari, M. Dynamometric assessment of the mechanical resistance of porcelain veneers related to tooth preparation: A comparison between two techniques. J. Prosthet. Dent. 2006, 95, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Jankar, A.S.; Kale, Y.; Kangane, S.; Ambekar, A.; Sinha, M.; Chaware, S. Comparative evaluation of fracture re-sistance of Ceramic Veneer with three different incisal design preparations-An In-vitro Study. J. Int. Oral Health JIOH 2014, 6, 48–54. [Google Scholar] [PubMed]
- Sorrentino, R.; Ruggiero, G.; Borelli, B.; Barlattani, A.; Zarone, F. Dentin Exposure after Tooth Preparation for Laminate Veneers: A Microscopical Analysis to Evaluate the Influence of Operators’ Expertise. Materials 2022, 15, 1763. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Mean Marginal Gap (μm) | n | Std. Deviation (μm) | Minimum (μm) | Maximum (μm) |
|---|---|---|---|---|---|
| CEREC CAD/CAM | 91.594 | 16 | 1.626 | 88.143 | 93.807 |
| IPS e.max CAD | 106.489 | 16 | 2.507 | 101.210 | 109.807 |
| Levene’s Test for Equality of Variances | t-Test for Equality of Means | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| F | Sig. | t | df | Sig. (2-Tailed) | Mean Difference | Std. Error Difference | 95% Confidence Interval | |||
| Lower | Upper | |||||||||
| Marginal fit | Equal variances assumed | 2.055 | 0.162 | −19.939 | 30.000 | 0.000 | −14.894 | 0.746 | −16.419 | −13.368 |
| Equal variances not assumed | −19.939 | 25.725 | 0.000 | −14.894 | 0.746 | −16.430 | −13.358 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanoon, Z.A.; Abdullah, H.A.; Al-Ibraheemi, Z.A.; Alamoush, R.A.; Sami, S.M.; Haider, J. Marginal Fit of Porcelain Laminate Veneer Materials under Thermocycling Condition: An In-Vitro Study. Dent. J. 2023, 11, 12. https://doi.org/10.3390/dj11010012
Hanoon ZA, Abdullah HA, Al-Ibraheemi ZA, Alamoush RA, Sami SM, Haider J. Marginal Fit of Porcelain Laminate Veneer Materials under Thermocycling Condition: An In-Vitro Study. Dentistry Journal. 2023; 11(1):12. https://doi.org/10.3390/dj11010012
Chicago/Turabian StyleHanoon, Zanbaq Azeez, Huda Abbas Abdullah, Zahraa Abdulaali Al-Ibraheemi, Rasha A. Alamoush, Suha Mohammad Sami, and Julfikar Haider. 2023. "Marginal Fit of Porcelain Laminate Veneer Materials under Thermocycling Condition: An In-Vitro Study" Dentistry Journal 11, no. 1: 12. https://doi.org/10.3390/dj11010012