
Digital Workflow for Edentulous Patients with Implant-Supported Fixed Prostheses: A Fully Digital Technique


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
Technical Description
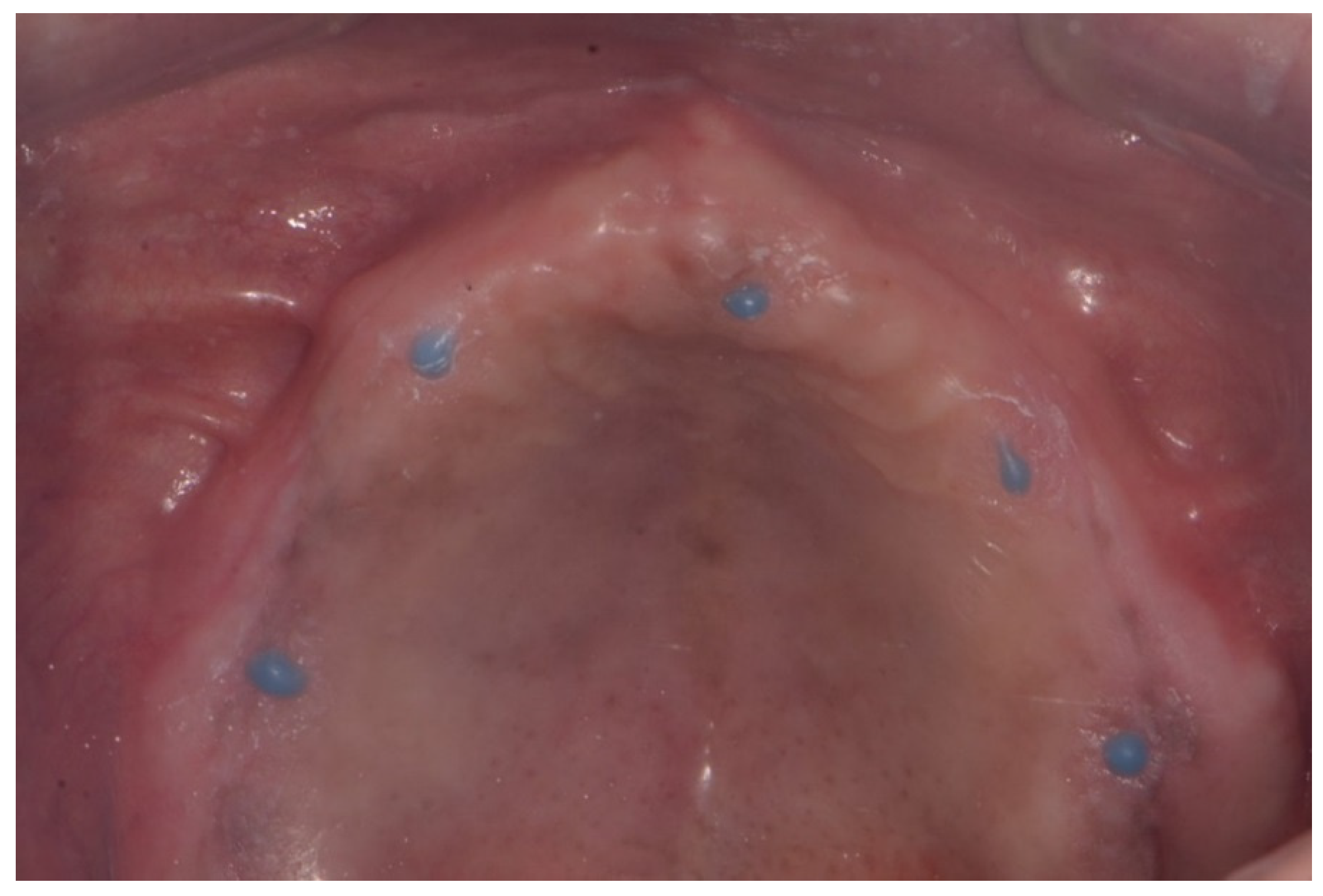
- Inject radiopaque flowable composite resins (Charmfil Flow; Dentkist Inc., Seoul, Korea) in hemispheres of 1–2 mm diameter in ≥3 sites of the attached gingiva (Figure 1). These pose as markers for superimposing intraoral scans and CBCT data. After photopolymerization of the injected resin, apply tissue adhesive (Histoacryl; B. Braun, Aesculap AG, Tuttlingen, Germany) around the resin marker to prevent the resin from falling off.
- Place vinyl polysiloxane with the light viscosity consistency of the material inside the patient’s existing denture and obtain an impression in occlusion similar to that using a custom tray. If the resin marker is attached intraorally, an impression of the resin marker is also obtained.
- Obtain CBCT images of the maxilla and mandible with the resin markers using a Point 3D Combi 500C (PointNix).
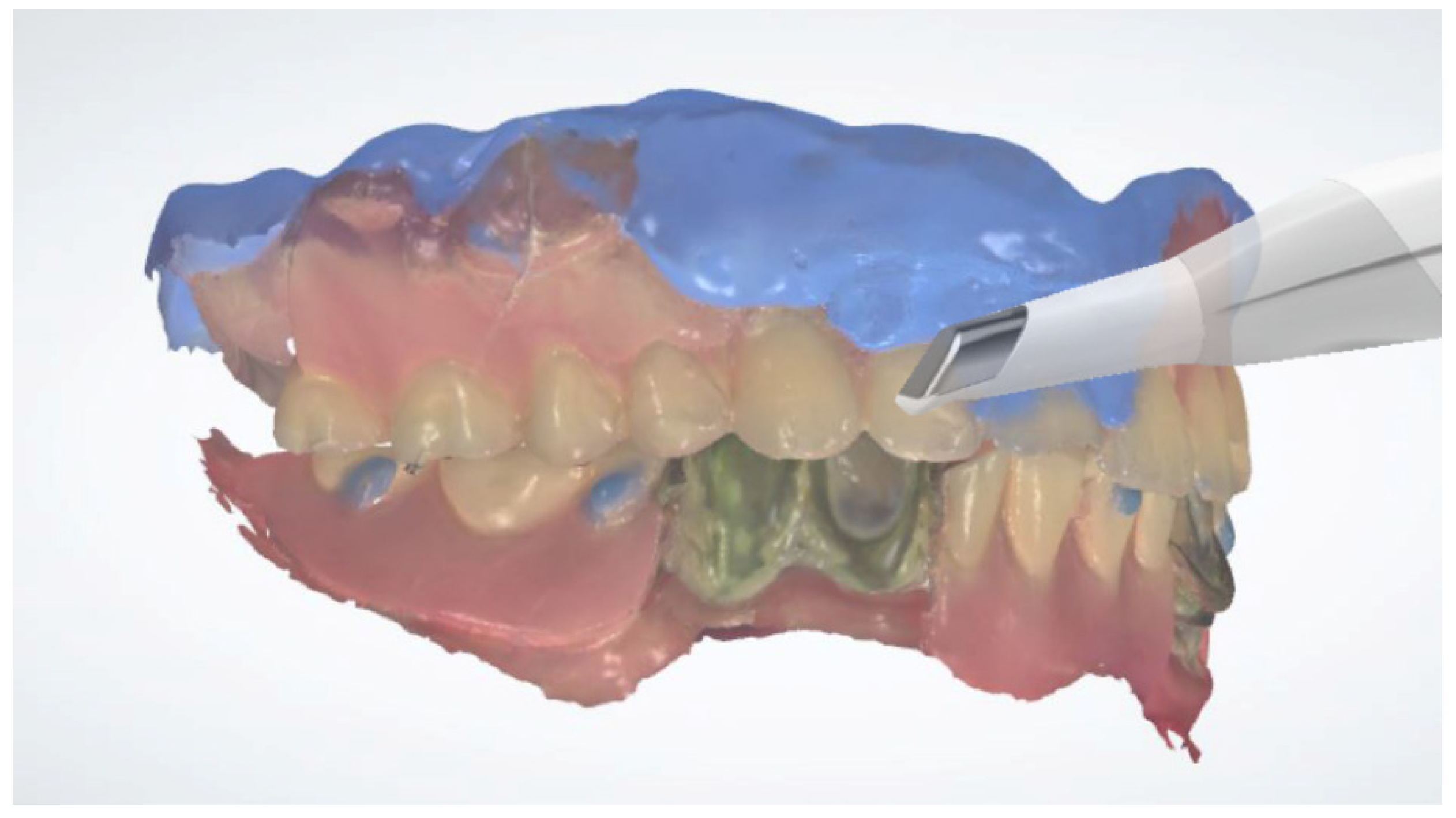
- Scan the impression surface of the denture, opposing teeth, and bite, registering the relationship of the jaw with the denture using an intraoral scanner (TRIOS 3; 3Shape A/S) (Figure 2).
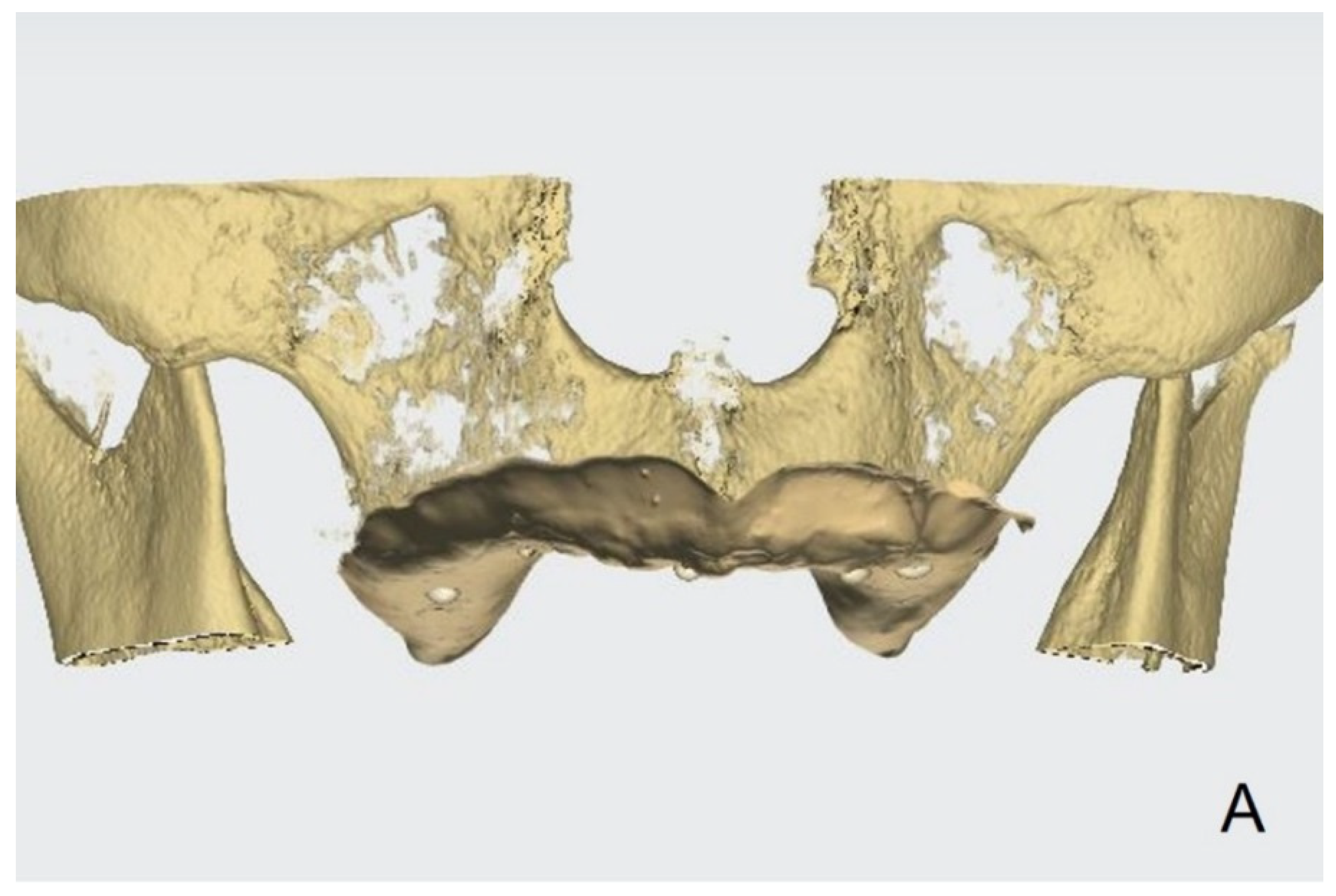
- Obtain the tissue surface details by scanning the impression surface of the denture with the intraoral scanner. Import the DICOM data of the inverted scan images and CBCT images into an implant-planning software (Implant Studio; 3Shape A/S, 2015). Virtually merge the inverted scan images and CBCT images by matching the hemisphere resin markers present in both (Figure 3A).
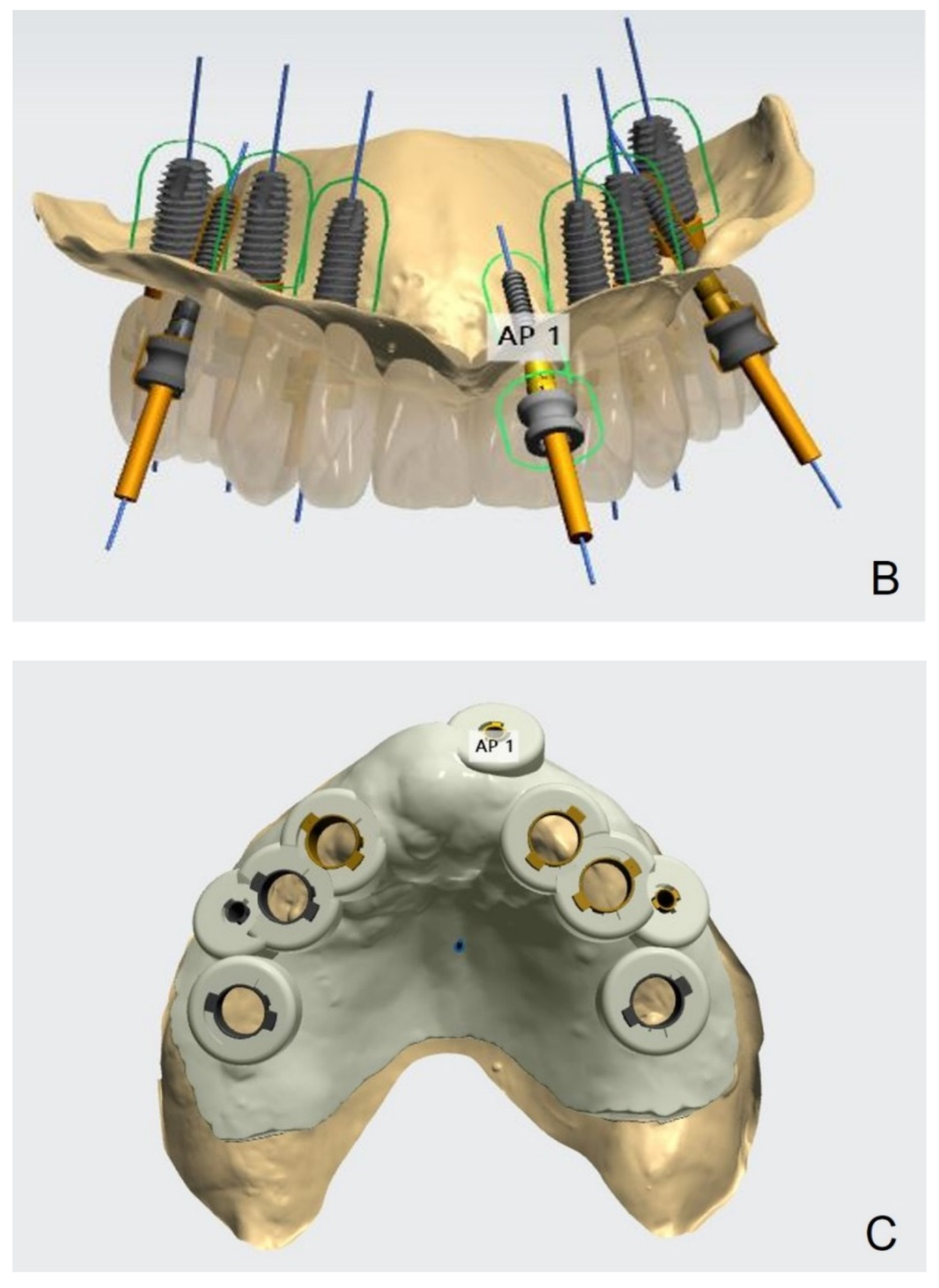
- Following image superimposition, plan the positions for the six implants based on the virtual tooth arrangement (Figure 3B). Subsequently, print the surgical guide for implant placement using a 3D printer (Probe; DIO Inc., Pusan, South Korea) (Figure 3C). Design an interim prosthesis for immediate loading after implant surgery using a virtual design program (Dental Designer; 3Shape A/S). The interim prosthesis consists of two parts—a fixed part similar to the definitive restoration and a denture flange part for repositioning the fixed part in the oral cavity (Figure 4). The flange part should be easily separable from the fixed part. After the design is complete, 3D-print the interim prosthesis using a commercial printable resin (DIOnavi Crown&Bridge; DIO Inc.).
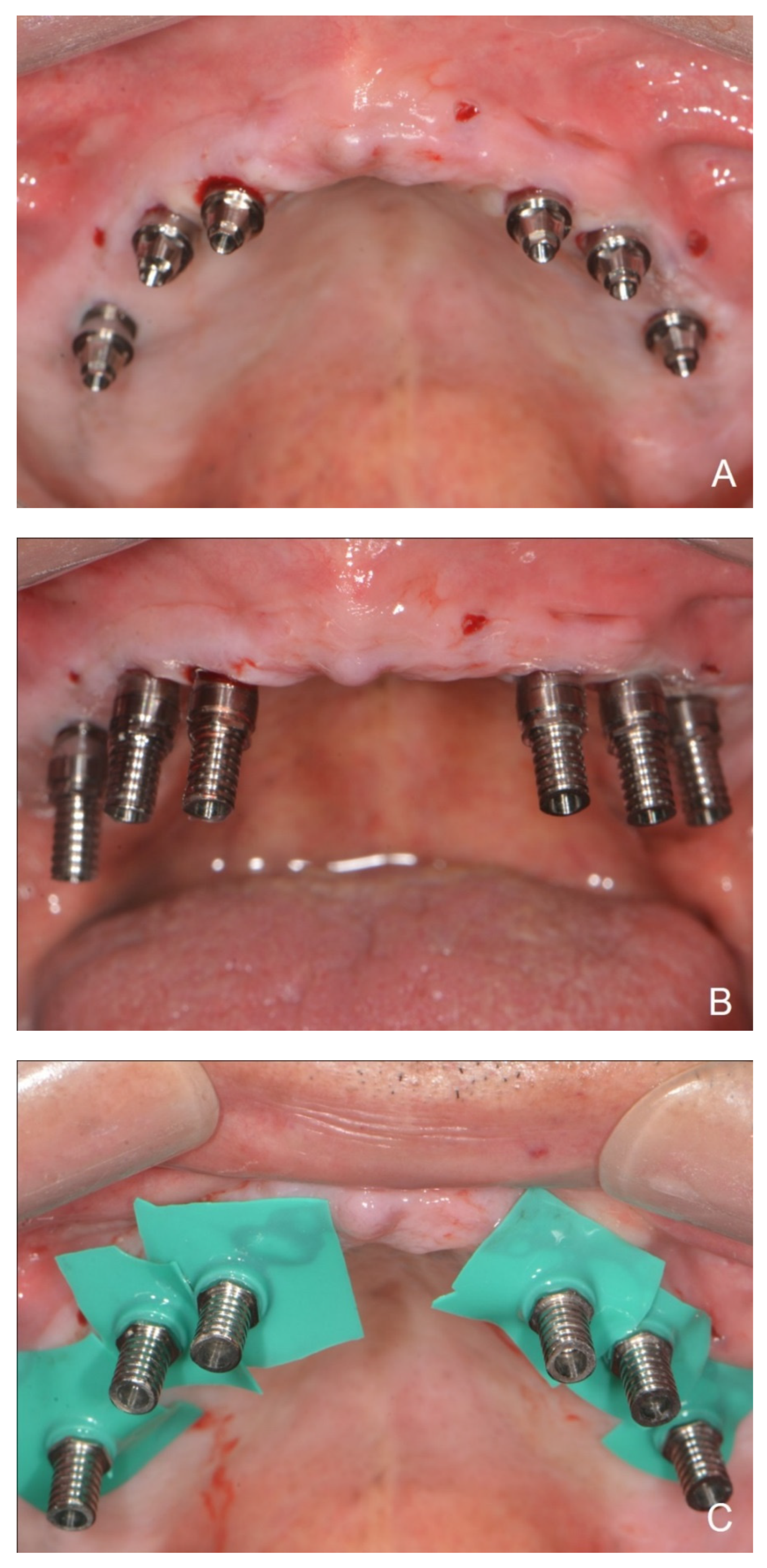
- After implant placement, remove the surgical guide and connect the abutment to the implant (Figure 5A). Then, connect the interim cylinder to the abutment (Figure 5B). Connect the interim prosthesis to the interim cylinder by adding acrylic resin (Duo-Link; Bisco Dental, Schaumburg, IL, USA) to the space between them using a syringe (Figure 5C,D). After allowing the resin to polymerize, remove the flange part of the interim prosthesis (Figure 6). Screw the attached part of the prosthesis to the abutment. Check for occlusal interferences and make occlusal adjustments if necessary.
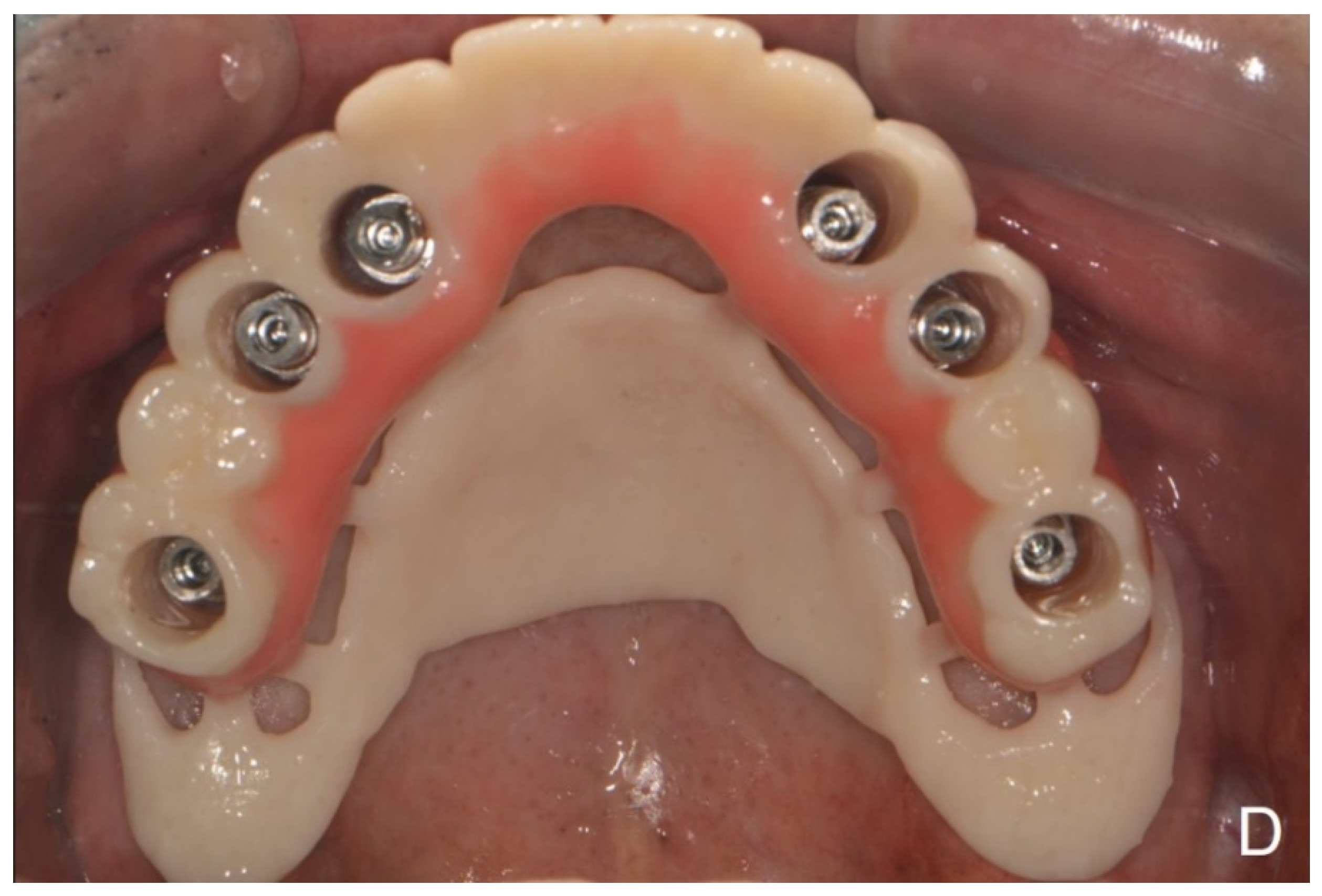
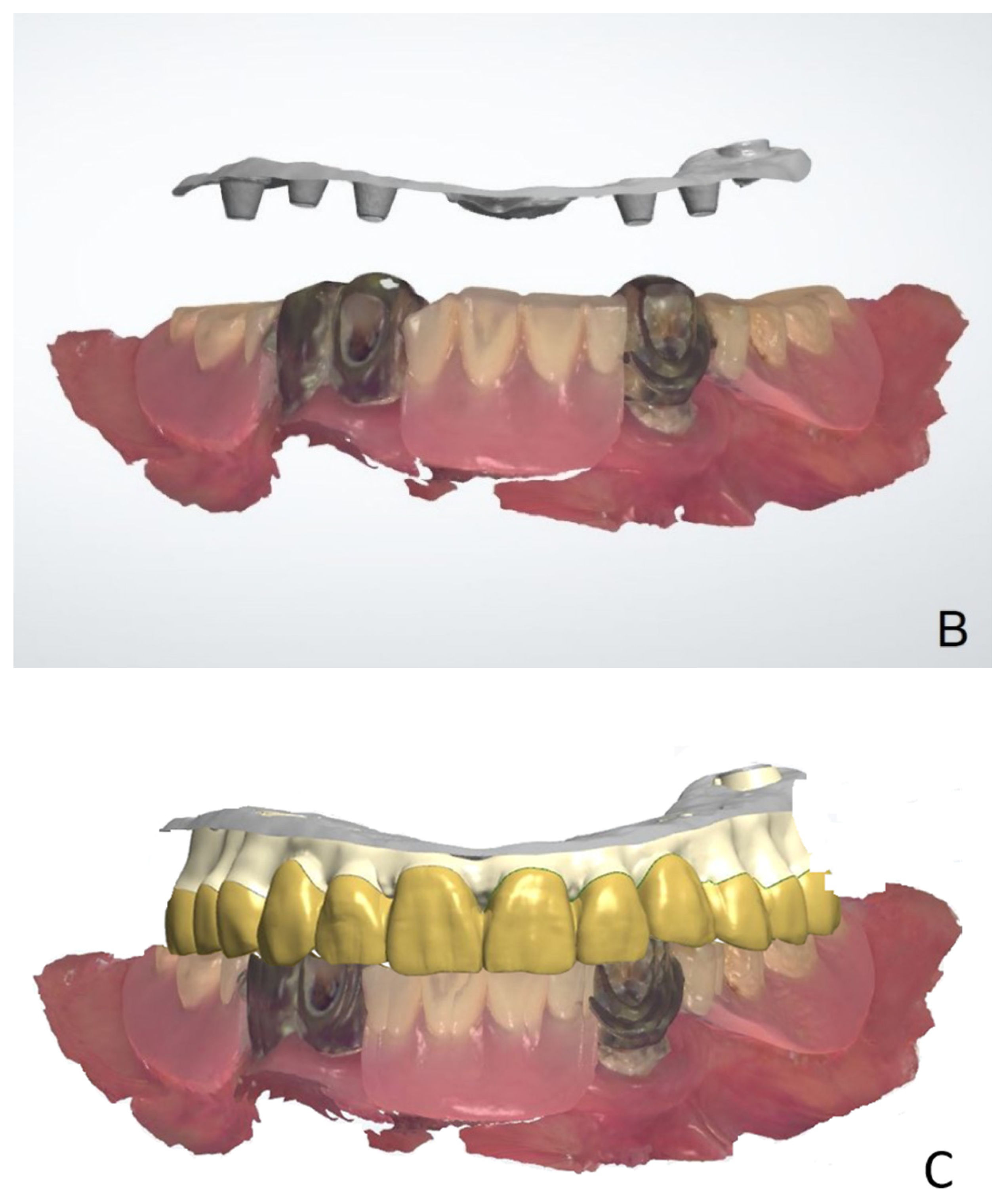
- Scan all sides of the interim prosthesis extraorally using the intraoral scanner to obtain scan data. With the interim prosthesis in the mouth, scan its labial surface, opposing teeth, and occlusal relationship using the intraoral scanner (Figure 7A).
- Reverse the interim prosthesis image using a CAD software (Shape Designer; 3Shape A/S) to obtain a positive image from the negatively recorded inside image of the cylinder (Figure 7B). Superimpose the markers on the cylinder cap and reversed cylinder images. Based on the previously registered occlusion, obtain a digital model of the cylinder cap and the interim prosthesis base associated with the opposing teeth.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Castellon, P.; Block, M.S.; Smith, M.B.; Finger, I.M. Immediate loading of the edentulous mandible: Delivery of the final restoration or a provisional restoration—Which method to use? J. Oral Maxillofac. Surg. 2004, 62, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Agliardi, E.; Panigatti, S.; Clerico, M.; Villa, C.; Malo, P. Immediate rehabilitation of the edentulous jaws with full fixed prostheses supported by four implants: Interim results of a single cohort prospective study. Clin. Oral Implant. Res. 2010, 21, 459–465. [Google Scholar] [CrossRef] [PubMed]
- De Bruyn, H.; Raes, S.; Ostman, P.O.; Cosyn, J. Immediate loading in partially and completely edentulous jaws: A review of the literature with clinical guidelines. Periodontol. 2000 2014, 66, 153–187. [Google Scholar] [CrossRef] [PubMed]
- De Bruyn, H.; Van de Velde, T.; Collaert, B. Immediate functional loading of TiOblast dental implants in full-arch edentulous mandibles: A 3-year prospective study. Clin. Oral Implant. Res. 2008, 19, 717–723. [Google Scholar] [CrossRef]
- Grunder, U. Immediate functional loading of immediate implants in edentulous arches: Two-year results. Int. J. Periodontics Restor. Dent. 2001, 21, 545–551. [Google Scholar]
- Horiuchi, K.; Uchida, H.; Yamamoto, K.; Sugimura, M. Immediate loading of Branemark system implants following placement in edentulous patients: A clinical report. Int. J. Oral Maxillofac. Implant. 2000, 15, 824–830. [Google Scholar]
- Misch, C.M. Immediate loading of definitive implants in the edentulous mandible using a fixed provisional prosthesis: The denture conversion technique. J. Oral Maxillofac. Surg. 2004, 62 (Suppl. S2), 106–115. [Google Scholar] [CrossRef]
- Santosa, R.E. Provisional restoration options in implant dentistry. Aust. Dent. J. 2007, 52, 234–242. [Google Scholar] [CrossRef]
- Branemark, P.I.; Engstrand, P.; Ohrnell, L.O.; Grondahl, K.; Nilsson, P.; Hagberg, K.; Darle, C.; Lekholm, U. Branemark Novum: A new treatment concept for rehabilitation of the edentulous mandible. Preliminary results from a prospective clinical follow-up study. Clin. Implant Dent. Relat. Res. 1999, 1, 2–16. [Google Scholar] [CrossRef]
- Briccoli, L.; Barone, R.; Clauser, C. A technique for fabricating a definitive immediate implant-supported prosthesis for the edentulous mandible. J. Prosthet. Dent. 2012, 108, 196–199. [Google Scholar] [CrossRef]
- Henry, P.J.; van Steenberghe, D.; Blomback, U.; Polizzi, G.; Rosenberg, R.; Urgell, J.P.; Wendelhag, I. Prospective multicenter study on immediate rehabilitation of edentulous lower jaws according to the Branemark Novum protocol. Clin. Implant Dent. Relat. Res. 2003, 5, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Kupeyan, H.K.; Shaffner, M.; Armstrong, J. Definitive CAD/CAM-guided prosthesis for immediate loading of bone-grafted maxilla: A case report. Clin. Implant Dent. Relat. Res. 2006, 8, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Marchack, C.B. An immediately loaded CAD/CAM-guided definitive prosthesis: A clinical report. J. Prosthet. Dent. 2005, 93, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Menini, M.; Bagnasco, F.; Pera, P.; Tealdo, T.; Pesce, P. Branemark novum immediate loading rehabilitation of edentulous mandibles: Case series with a 16-year follow-up. Int. J. Periodontics Restor. Dent. 2019, 39, 729–735. [Google Scholar] [CrossRef]
- Oh, J.H.; An, X.; Jeong, S.M.; Choi, B.H. A digital technique for fabricating an interim implant-supported fixed prosthesis immediately after implant placement in patients with complete edentulism. J. Prosthet. Dent. 2019, 121, 26–31. [Google Scholar] [CrossRef]
- Esposito, M.; Grufferty, B.; Papavasiliou, G.; Dominiak, M.; Trullenque-Eriksson, A.; Heinemann, F. Immediate loading of occluding definitive partial fixed prostheses vs non-occluding provisional restorations—3-year post-loading results from a pragmatic multicentre randomised controlled trial. Eur. J. Oral Implantol. 2018, 11, 309–320. [Google Scholar]
- Heinemann, F.; Grufferty, B.; Papavasiliou, G.; Dominiak, M.; Garcia, J.J.; Trullenque-Eriksson, A.; Esposito, M. Immediate occluding definitive partial fixed prosthesis versus non-occluding provisional restorations—4-month post-loading results from a pragmatic multicenter randomised controlled trial. Int. J. Oral Implantol. 2016, 9, 47–56. [Google Scholar]
- An, X.; Fang, J.H.; Jeong, S.M.; Choi, B.H. A CAD-CAM technique for conversion of interim-to-definitive restoration in patients with complete edentulism. J. Prosthet. Dent. 2018, 120, 190–193. [Google Scholar] [CrossRef]
- Amin, S.; Weber, H.P.; Finkelman, M.; El Rafie, K.; Kudara, Y.; Papaspyridakos, P. Digital vs. conventional full-arch implant impressions: A comparative study. Clin. Oral Implant. Res. 2017, 28, 1360–1367. [Google Scholar] [CrossRef]
- Gherlone, E.; Cappare, P.; Vinci, R.; Ferrini, F.; Gastaldi, G.; Crespi, R. Conventional Versus Digital Impressions for “All-on-Four” Restorations. Int. J. Oral Maxillofac. Implant. 2016, 31, 324–330. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Gallucci, G.O.; Chen, C.J.; Hanssen, S.; Naert, I.; Vandenberghe, B. Digital versus conventional implant impressions for edentulous patients: Accuracy outcomes. Clin. Oral Implant. Res. 2016, 27, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Drago, C. frequency and type of prosthetic complications associated with interim, immediately loaded full-arch prostheses: A 2-year retrospective chart review. J. Prosthodont. 2016, 25, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Drago, C. cantilever lengths and anterior-posterior spreads of interim, acrylic resin, full-arch screw-retained prostheses and their relationship to prosthetic complications. J. Prosthodont. 2017, 26, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Francetti, L.; Corbella, S.; Taschieri, S.; Cavalli, N.; Del Fabbro, M. medium- and long-term complications in full-arch rehabilitations supported by upright and tilted implants. Clin. Implant. Dent. Relat. Res. 2015, 17, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Malo, P.; Rangert, B.; Nobre, M. “All-on-Four” immediate-function concept with Branemark System implants for completely edentulous mandibles: A retrospective clinical study. Clin. Implant. Dent. Relat. Res. 2003, 5 (Suppl. S1), 2–9. [Google Scholar] [CrossRef]
- Mozzati, M.; Arata, V.; Gallesio, G.; Mussano, F.; Carossa, S. Immediate postextractive dental implant placement with immediate loading on four implants for mandibular-full-arch rehabilitation: A retrospective analysis. Clin. Implant. Dent. Relat. Res. 2013, 15, 332–340. [Google Scholar] [CrossRef]
- Alt, V.; Hannig, M.; Wostmann, B.; Balkenhol, M. Fracture strength of temporary fixed partial dentures: CAD/CAM versus directly fabricated restorations. Dent. Mater. 2011, 27, 339–347. [Google Scholar] [CrossRef]
- Penarrocha-Oltra, D.; Covani, U.; Penarrocha, M.; Penarrocha-Diago, M. Immediate versus conventional loading with fixed full-arch prostheses in mandibles with failing dentition: A prospective controlled study. Int. J. Oral Maxillofac. Implant. 2015, 30, 427–434. [Google Scholar] [CrossRef]
- Penate, L.; Basilio, J.; Roig, M.; Mercade, M. Comparative study of interim materials for direct fixed dental prostheses and their fabrication with CAD/CAM technique. J. Prosthet. Dent. 2015, 114, 248–253. [Google Scholar] [CrossRef]
- Stawarczyk, B.; Liebermann, A.; Eichberger, M.; Guth, J.F. Evaluation of mechanical and optical behavior of current esthetic dental restorative CAD/CAM composites. J. Mech. Behav. Biomed. Mater. 2015, 55, 1–11. [Google Scholar] [CrossRef]
- Yilmaz, B.; Alp, G.; Seidt, J.; Johnston, W.M.; Vitter, R.; McGlumphy, E.A. Fracture analysis of CAD-CAM high-density polymers used for interim implant-supported fixed, cantilevered prostheses. J. Prosthet. Dent. 2018, 120, 79–84. [Google Scholar] [CrossRef] [PubMed]
- de Mello, G.P.S.; Mello, E.D.A.; Corazza, P.H. A new operative method for obtaining full-arch prostheses for immediate loading dental implants. J. Prosthodont. Res. 2017, 61, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Giordano, F.; Esposito, M. Immediate loading of fixed prostheses in fully edentulous jaws—1-year follow-up from a single-cohort retrospective study. Eur. J. Oral Implantol. 2017, 10, 339–348. [Google Scholar] [PubMed]
- Papaspyridakos, P.; Chen, C.J.; Chuang, S.K.; Weber, H.P. Implant loading protocols for edentulous patients with fixed prostheses: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Implant. 2014, 29, 256–270. [Google Scholar] [CrossRef]
- Pieri, F.; Aldini, N.N.; Fini, M.; Corinaldesi, G. Immediate occlusal loading of immediately placed implants supporting fixed restorations in completely edentulous arches: A 1-year prospective pilot study. J. Periodontol. 2009, 80, 411–421. [Google Scholar] [CrossRef]
- Schwarz, F.; Sanz-Martin, I.; Kern, J.S.; Taylor, T.; Schaer, A.; Wolfart, S.; Sanz, M. Loading protocols and implant supported restorations proposed for the rehabilitation of partially and fully edentulous jaws. Camlog Foundation Consensus Report. Clin. Oral Implant. Res. 2016, 27, 988–992. [Google Scholar] [CrossRef]
- Testori, T.; Del Fabbro, M.; Capelli, M.; Zuffetti, F.; Francetti, L.; Weinstein, R.L. Immediate occlusal loading and tilted implants for the rehabilitation of the atrophic edentulous maxilla: 1-year interim results of a multicenter prospective study. Clin. Oral Implant. Res. 2008, 19, 227–232. [Google Scholar] [CrossRef]
- Diehn, F.E.; Michalak, G.J.; DeLone, D.R.; Kotsenas, A.L.; Lindell, E.P.; Campeau, N.G.; Halaweish, A.F.; McCollough, C.H.; Fletcher, J.G. CT Dental artifact: Comparison of an iterative metal artifact reduction technique with weighted filtered back-projection. Acta Radiol. Open 2017, 6, 2058460117743279. [Google Scholar] [CrossRef]
- An, X.; Yang, H.W.; Choi, B.H. Digital Workflow for Computer-guided implant surgery in edentulous patients with an intraoral scanner and old complete denture. J. Prosthodont. 2019, 28, 715–718. [Google Scholar] [CrossRef]












Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, S.W.; Fan, Y.-Q.; Lee, C. Digital Workflow for Edentulous Patients with Implant-Supported Fixed Prostheses: A Fully Digital Technique. Dent. J. 2022, 10, 174. https://doi.org/10.3390/dj10090174
Jung SW, Fan Y-Q, Lee C. Digital Workflow for Edentulous Patients with Implant-Supported Fixed Prostheses: A Fully Digital Technique. Dentistry Journal. 2022; 10(9):174. https://doi.org/10.3390/dj10090174
Chicago/Turabian StyleJung, Seung Wook, Yi-Qin Fan, and Chunui Lee. 2022. "Digital Workflow for Edentulous Patients with Implant-Supported Fixed Prostheses: A Fully Digital Technique" Dentistry Journal 10, no. 9: 174. https://doi.org/10.3390/dj10090174