Raman-Guided Bronchoscopy: Feasibility and Detection Depth Studies Using Ex Vivo Lung Tissues and SERS Nanoparticle Tags

 , and
, and
Abstract
:1. Introduction
2. Methods and Materials
2.1. Materials
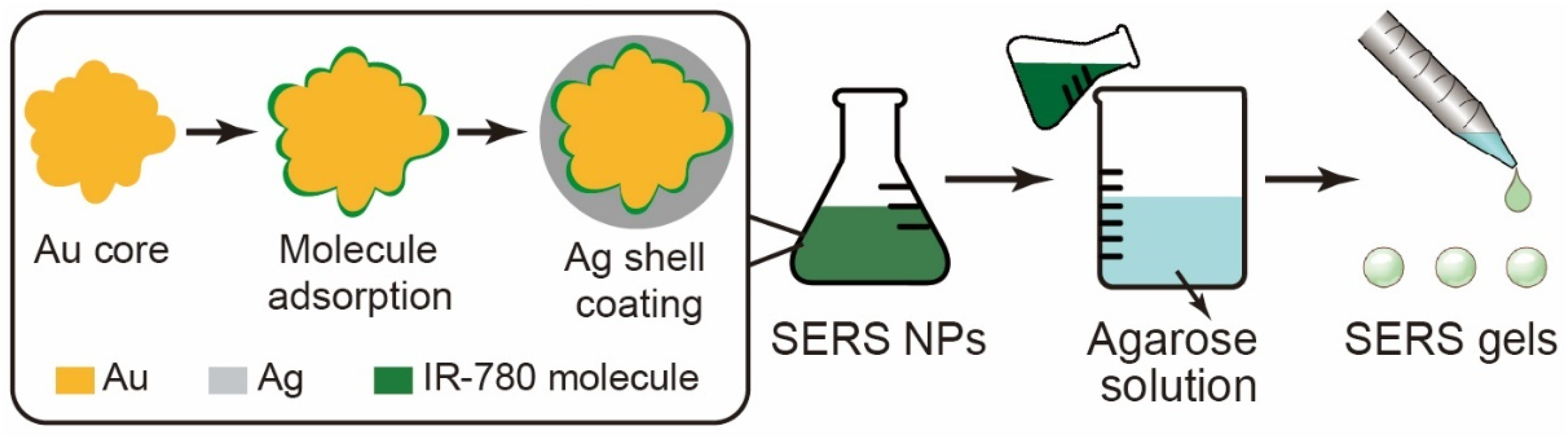
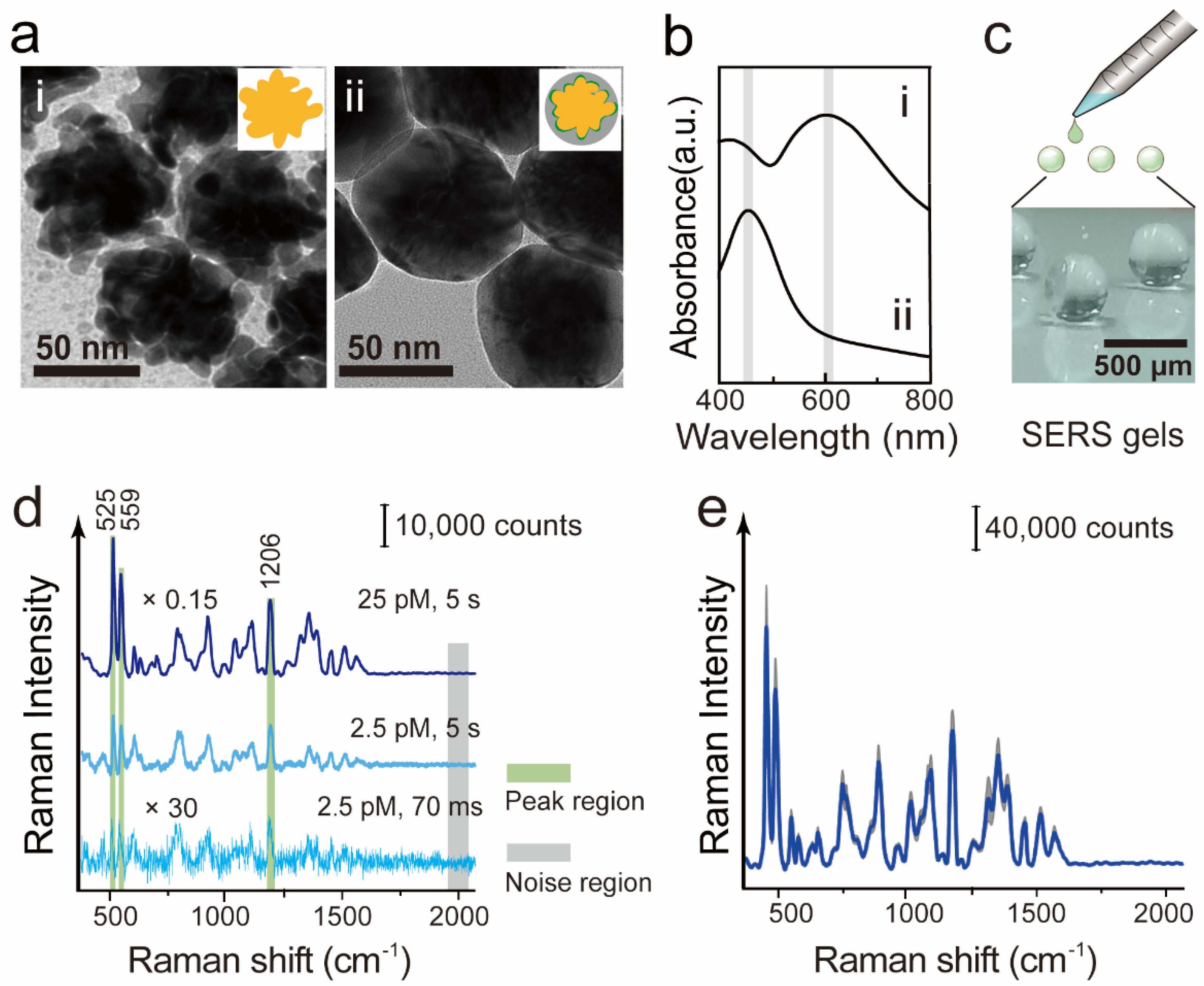
2.2. Preparation of SERS NPs and SERS Gels
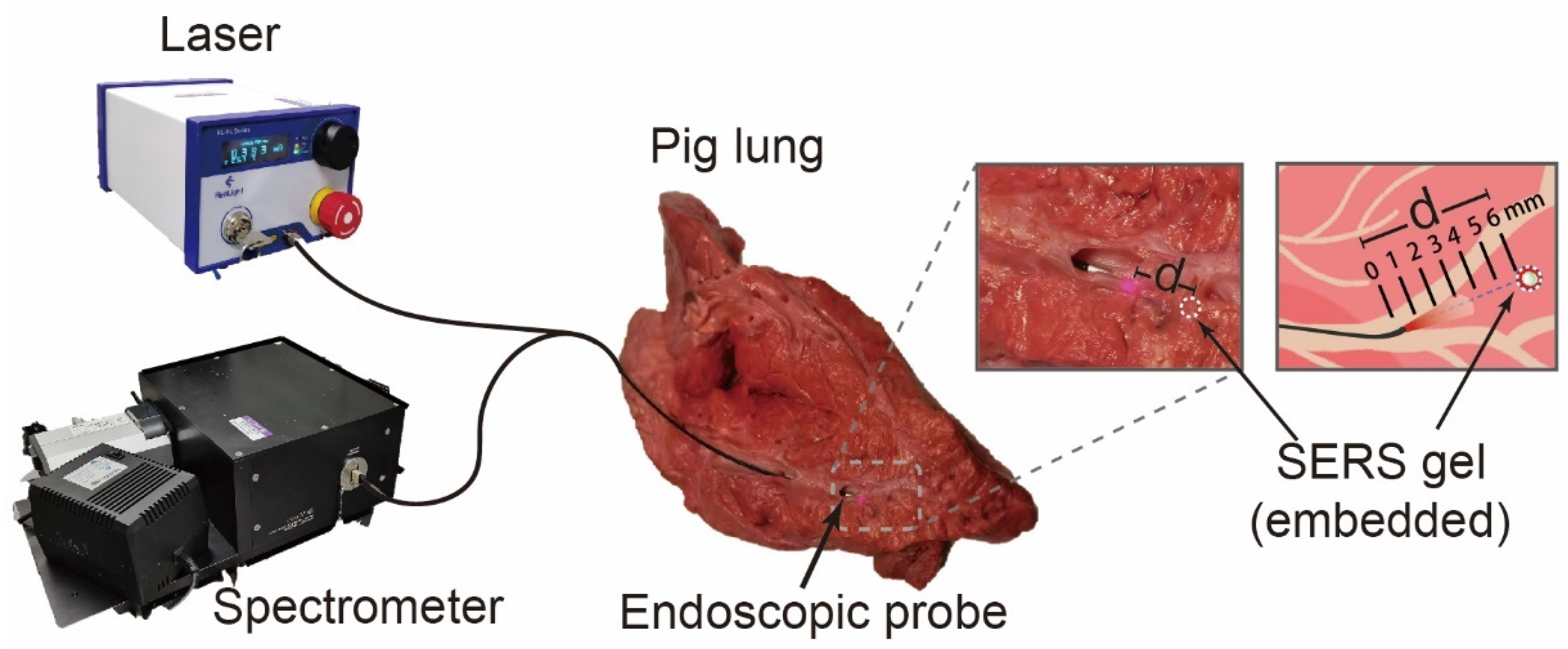
2.3. SERS Measurements on Ex Vivo Tissues and Spectral Analysis
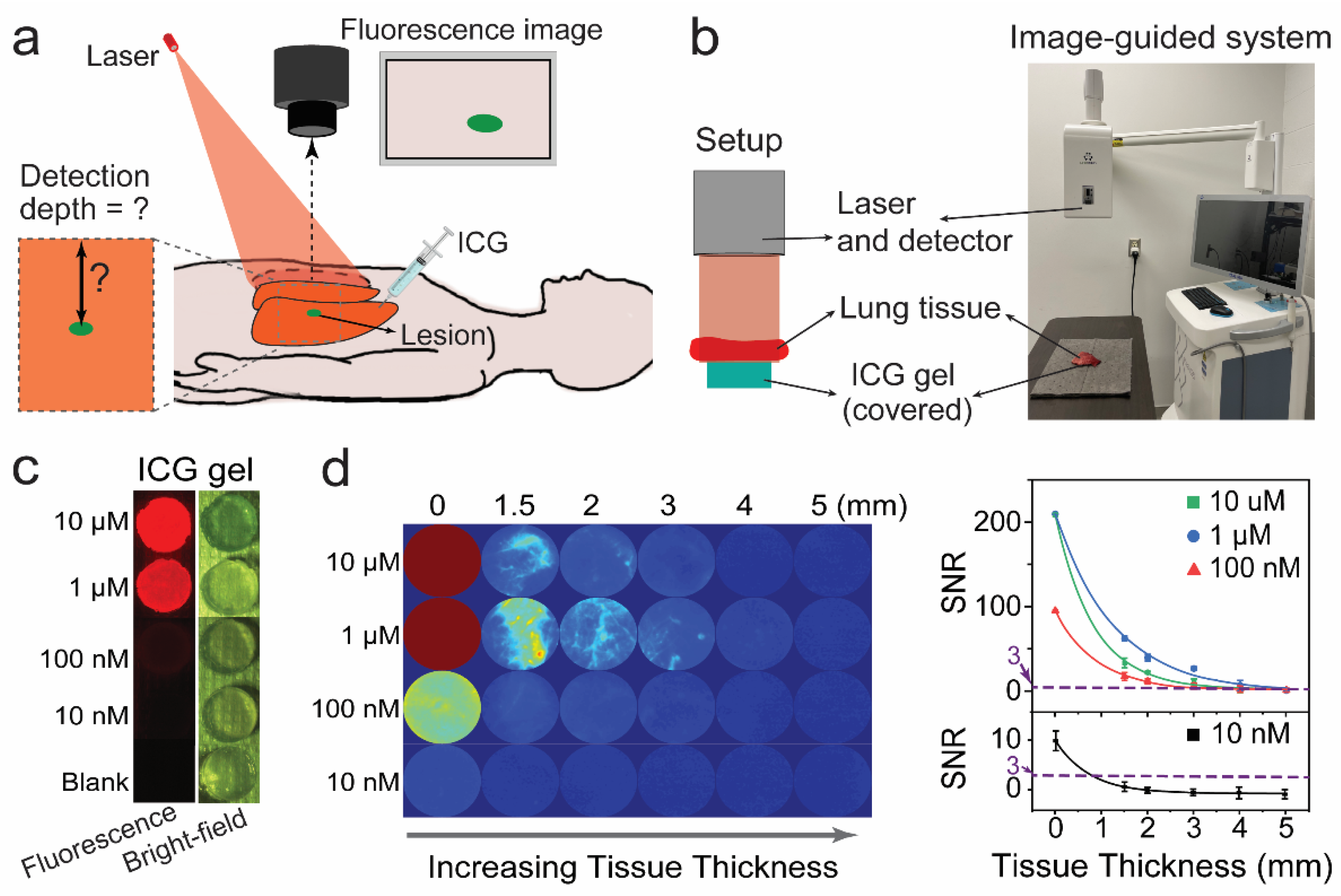
2.4. Fluorescence Detection Depth Measurement and Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abbas, A.; Kadakia, S.; Ambur, V.; Muro, K.; Kaiser, L. Intraoperative electromagnetic navigational bronchoscopic localization of small, deep, or subsolid pulmonary nodules. J. Thorac. Cardiovasc. Surg. 2017, 153, 1581–1590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rojas-Solano, J.R.; Ugalde-Gamboa, L.; Machuzak, M. Robotic Bronchoscopy for Diagnosis of Suspected Lung Cancer: A Feasibility Study. J. Bronchol. Interv. Pulmonol. 2018, 25, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Chaddha, U.; Kovacs, S.P.; Manley, C.; Hogarth, D.K.; Cumbo-Nacheli, G.; Bhavani, S.V.; Kumar, R.; Shende, M.; Egan, J.P.; Murgu, S. Robot-assisted bronchoscopy for pulmonary lesion diagnosis: Results from the initial multicenter experience. BMC Pulm. Med. 2019, 19, 243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemp, S.V. Navigation Bronchoscopy. Respiration 2020, 99, 277–286. [Google Scholar] [CrossRef]
- Anantham, D.; Feller-Kopman, D.; Shanmugham, L.N.; Berman, S.M.; DeCamp, M.M.; Gangadharan, S.P.; Eberhardt, R.; Herth, F.; Ernst, A. Electromagnetic navigation bronchoscopy-guided fiducial placement for robotic stereotactic radiosurgery of lung tumors: A feasibility study. Chest 2007, 132, 930–935. [Google Scholar] [CrossRef]
- Sabri, Y.Y.; Kamel, K.M.; Hafez, M.A.F.; Nasef, S.M.S.S. Evaluation of the role of MSCT airway mapping in guiding trans-bronchial lung biopsy in cases of inaccessible lung lesions. Egypt. J. Radiol. Nucl. Med. 2017, 48, 947–952. [Google Scholar] [CrossRef]
- Lin, M.-W.; Chen, J.-S. Image-guided techniques for localizing pulmonary nodules in thoracoscopic surgery. J. Thorac. Dis. 2016, 8 (Suppl. 9), S749–S755. [Google Scholar] [CrossRef] [Green Version]
- Hong, G.; Antaris, A.L.; Dai, H. Near-infrared fluorophores for biomedical imaging. Nat. Biomed. Eng. 2017, 1, 0010. [Google Scholar] [CrossRef]
- Lane, L.A.; Xue, R.; Nie, S. Emergence of two near-infrared windows for in vivo and intraoperative SERS. Curr. Opin. Chem. Biol. 2018, 45, 95–103. [Google Scholar] [CrossRef]
- Lin, L.; Bi, X.; Gu, Y.; Wang, F.; Ye, J. Surface-enhanced Raman scattering nanotags for bioimaging. J. Appl. Phys. 2021, 129, 191101. [Google Scholar] [CrossRef]
- Khlebtsov, N.G.; Lin, L.; Khlebtsov, B.; Ye, J. Gap-enhanced Raman tags: Fabrication, optical properties, and theranostic applications. Theranostics 2020, 10, 2067–2094. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Gu, H.; Ye, J. Plasmonic multi-shell nanomatryoshka particles as highly tunable SERS tags with built-in reporters. Chem. Commun. 2015, 51, 17740–17743. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Tan, Z.; Lin, L.; He, J.; He, C.; Thackray, B.D.; Zhang, Y.; Ye, J. Surface-Enhanced Raman Nanoprobes with Embedded Standards for Quantitative Cholesterol Detection. Small Methods 2018, 2, 1800182. [Google Scholar] [CrossRef]
- Ye, J.; Van Dorpe, P. Plasmonic behaviors of gold dimers perturbed by a single nanoparticle in the gap. Nanoscale 2012, 4, 7205–7211. [Google Scholar] [CrossRef]
- Nicolson, F.; Kircher, M.F.; Stone, N.; Matousek, P. Spatially offset Raman spectroscopy for biomedical applications. Chem. Soc. Rev. 2021, 50, 556–568. [Google Scholar] [CrossRef]
- Fenster, A.; Downey, D.B.; Cardinal, H.N. Three-dimensional ultrasound imaging. Phys. Med. Biol. 2001, 46, R67. [Google Scholar] [CrossRef]
- Blaivas, M. Lung ultrasound in evaluation of pneumonia. J. Ultrasound Med. 2012, 31, 823–826. [Google Scholar] [CrossRef] [Green Version]
- Grenier, P.A.; Beigelman-Aubry, C.; Fétita, C.; Prêteux, F.; Brauner, M.W.; Lenoir, S. New frontiers in CT imaging of airway disease. Eur. Radiol. 2002, 12, 1022–1044. [Google Scholar] [CrossRef]
- Ntziachristos, V. Going deeper than microscopy: The optical imaging frontier in biology. Nat. Methods 2010, 7, 603–614. [Google Scholar] [CrossRef]
- Ye, Z.; Lin, L.; Tan, Z.; Zeng, Y.-J.; Ruan, S.; Ye, J. Sub-100 nm multi-shell bimetallic gap-enhanced Raman tags. Appl. Surf. Sci. 2019, 487, 1058–1067. [Google Scholar] [CrossRef]
- Bi, X.; Gu, Y.; Ye, J. Ag-Coated Au Nanopetals: Dual-Type Single-Nanoparticle Detection of Gap-Enhanced Resonance Raman Tags. ACS Appl. Nano Mater. 2020, 3, 6987–6995. [Google Scholar] [CrossRef]
- Zhang, Y.; Gu, Y.; He, J.; Thackray, B.D.; Ye, J. Ultrabright gap-enhanced Raman tags for high-speed bioimaging. Nat. Commun. 2019, 10, 3905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khlebtsov, B.N.; Burov, A.M.; Bratashov, D.; Tumskiy, R.S.; Khlebtsov, N.G. Petal-like Gap-Enhanced Raman Tags with Controllable Structures for High-Speed Raman Imaging. Langmuir 2020, 36, 5546–5553. [Google Scholar] [CrossRef]
- Zhang, Y.; Lin, L.; He, J.; Ye, J. Optical penetration of surface-enhanced micro-scale spatial offset Raman spectroscopy in turbid gel and biological tissue. J. Innov. Opt. Health Sci. 2021, 14, 2141001. [Google Scholar] [CrossRef]
- Ramos, P.M.; Ruisánchez, I. Noise and background removal in Raman spectra of ancient pigments using wavelet transform. J. Raman Spectrosc. 2005, 36, 848–856. [Google Scholar] [CrossRef]
- Watanabe, M.; Williams, D.B.; Tomokiyo, Y. Comparison of detectability limits for elemental mapping by EF-TEM and STEM-XEDS. Micron 2003, 34, 173–183. [Google Scholar] [CrossRef]
- Hu, F.; Shi, L.; Min, W. Biological imaging of chemical bonds by stimulated Raman scattering microscopy. Nat. Methods 2019, 16, 830–842. [Google Scholar] [CrossRef]
- Varghese, H.T.; Panicker, C.Y.; Philip, D.; Mannekutla, J.R.; Inamdar, S.R. IR, Raman and SERS studies of methyl salicylate. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2007, 66, 959–963. [Google Scholar] [CrossRef]
- Ouyang, B.; Poon, W.; Zhang, Y.-N.; Lin, Z.P.; Kingston, B.R.; Tavares, A.J.; Zhang, Y.; Chen, J.; Valic, M.S.; Syed, A.M.; et al. The dose threshold for nanoparticle tumour delivery. Nat. Mater. 2020, 19, 1362–1371. [Google Scholar] [CrossRef]
- Rastinehad, A.R.; Anastos, H.; Wajswol, E.; Winoker, J.S.; Sfakianos, J.P.; Doppalapudi, S.K.; Carrick, M.R.; Knauer, C.J.; Taouli, B.; Lewis, S.C.; et al. Gold nanoshell-localized photothermal ablation of prostate tumors in a clinical pilot device study. Proc. Natl. Acad. Sci. USA 2019, 116, 18590–18596. [Google Scholar] [CrossRef] [Green Version]
- Thomas, G.; Nguyen, T.-Q.; Pence, I.; Caldwell, B.; O’Connor, M.E.; Giltnane, J.; Sanders, M.E.; Grau, A.; Meszoely, I.; Hooks, M.; et al. Evaluating feasibility of an automated 3-dimensional scanner using Raman spectroscopy for intraoperative breast margin assessment. Sci. Rep. 2017, 7, 13548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, S.; Bowden, A.K. Bowden, Review of methods and applications of attenuation coefficient measurements with optical coherence tomography. J. Biomed. Opt. 2019, 24, 090901. [Google Scholar] [CrossRef] [PubMed]
- Anayama, T.; Qiu, J.; Chan, H.; Nakajima, T.; Weersink, R.; Daly, M.; McConnell, J.; Waddell, T.; Keshavjee, S.; Jaffray, D.; et al. Localization of pulmonary nodules using navigation bronchoscope and a near-infrared fluorescence thoracoscope. Ann. Thorac. Surg. 2015, 99, 224–230. [Google Scholar] [CrossRef]
- Descovich, M.; Dionisio, S.A.; Dasgupta, T.; Yom, S.S. A new method to characterize target location in lung cancer patients treated with stereotactic body radiation therapy. J. Radiat. Oncol. 2012, 1, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Murgu, S.D. Robotic assisted-bronchoscopy: Technical tips and lessons learned from the initial experience with sampling peripheral lung lesions. BMC Pulm. Med. 2019, 19, 89. [Google Scholar] [CrossRef] [Green Version]
- Theriault, M.-M.; Eddy, K.; Borgaonkar, J.N.; Babar, J.L.; Manos, D. Diseases Involving the Central Bronchi: Multidetector CT for Detection, Characterization, and Differential Diagnosis. Radiographics 2018, 38, 58–59. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Qiu, Y.; Lin, L.; Gu, H.; Xiao, Z.; Ye, J. Ultraphotostable Mesoporous Silica-Coated Gap-Enhanced Raman Tags (GERTs) for High-Speed Bioimaging. ACS Appl. Mater. Interfaces 2017, 9, 3995–4005. [Google Scholar] [CrossRef]
- Desroches, J.; Lemoine, É.; Pinto, M.; Marple, E.; Urmey, K.; Diaz, R.; Guiot, M.-C.; Wilson, B.C.; Petrecca, K.; Leblond, F. Development and first in-human use of a Raman spectroscopy guidance system integrated with a brain biopsy needle. J. Biophotonics 2019, 12, e201800396. [Google Scholar] [CrossRef]
- Desroches, J.; Jermyn, M.; Pinto, M.; Picot, F.; Tremblay, M.-A.; Obaid, S.; Marple, E.; Urmey, K.; Trudel, D.; Soulez, G.; et al. A new method using Raman spectroscopy for in vivo targeted brain cancer tissue biopsy. Sci. Rep. 2018, 8, 1792. [Google Scholar] [CrossRef]
- Garai, E.; Sensarn, S.; Zavaleta, C.L.; Loewke, N.O.; Rogalla, S.; Mandella, M.J.; Flet, S.A.; Friedland, S.; Liu, J.T.C.; Contag, C.H.; et al. A real-time clinical endoscopic system for intraluminal, multiplexed imaging of surface-enhanced Raman scattering nanoparticles. PLoS ONE 2015, 10, e0123185. [Google Scholar] [CrossRef]
- Pinto, M.; Zorn, K.C.; Tremblay, J.P.; Desroches, J.; Dallaire, F.; Aubertin, K.; Maple, E.T.; Kent, C.; Leblond, F.; Trudel, D.; et al. Integration of a Raman spectroscopy system to a robotic-assisted surgical system for real-time tissue characterization during radical prostatectomy procedures. J. Biomed. Opt. 2019, 24, 025001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, B.; Li, W.; Chang, Y.; Yuan, B.; Wu, Y.; Zhang, M.; Xu, J.; Li, J.; Zhang, X. A Supramolecular Radical Dimer: High-Efficiency NIR-II Photothermal Conversion and Therapy. Angew. Chem. Int. Ed. 2019, 58, 15526–15531. [Google Scholar] [CrossRef] [PubMed]
- Rivas-Arancibia, S.; Rodríguez-Martínez, E.; Badillo-Ramírez, I.; López-González, U.; Saniger, J.M. Structural Changes of Amyloid Beta in Hippocampus of Rats Exposed to Ozone: A Raman Spectroscopy Study. Front. Mol. Neurosci. 2017, 10, 137. [Google Scholar] [CrossRef] [PubMed]
- Widmaier, E.P.; Raff, H.; Strang, K.T. Vander’s Human Physiology; McGraw-Hill: New York, NY, USA, 2006. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site | Thickness of Bronchi Wall | Concentration of SERS NPs | Detection Depth in Lung Tissues | SNR at the Detection Depth |
|---|---|---|---|---|
| i | 0.85 mm | 25 pM | 5 mm | 4.6 ± 0.40 |
| ii | 1.06 mm | 25 pM | 4 mm | 9.5 ± 2.10 |
| iii | 1.29 mm | 25 pM | 3 mm | 28.4 ± 3.11 |
| iv | 0.76 mm | 2.5 pM | 2 mm | 11.0 ± 2.32 |
| v | 0.80 mm | 2.5 pM | 2 mm | 4.8 ± 0.22 |
| vi | 1.22 mm | 2.5 pM | <1 mm | / |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, Z.; Wang, Z.; Xie, H.; Wang, Y.; He, H.; Nie, S.; Ye, J.; Lin, L. Raman-Guided Bronchoscopy: Feasibility and Detection Depth Studies Using Ex Vivo Lung Tissues and SERS Nanoparticle Tags. Photonics 2022, 9, 429. https://doi.org/10.3390/photonics9060429
Wu Z, Wang Z, Xie H, Wang Y, He H, Nie S, Ye J, Lin L. Raman-Guided Bronchoscopy: Feasibility and Detection Depth Studies Using Ex Vivo Lung Tissues and SERS Nanoparticle Tags. Photonics. 2022; 9(6):429. https://doi.org/10.3390/photonics9060429
Chicago/Turabian StyleWu, Zongyu, Ziwen Wang, Haoqiang Xie, Yiming Wang, Haoqi He, Shuming Nie, Jian Ye, and Li Lin. 2022. "Raman-Guided Bronchoscopy: Feasibility and Detection Depth Studies Using Ex Vivo Lung Tissues and SERS Nanoparticle Tags" Photonics 9, no. 6: 429. https://doi.org/10.3390/photonics9060429