
Subjective Assessments and Serum Cortisol Levels as Risk Factors of Pain Persistence in the Late Postoperative Period in Old and Oldest-Old Patients

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments and Measures
2.3. Statistical Analysis
2.4. Ethics
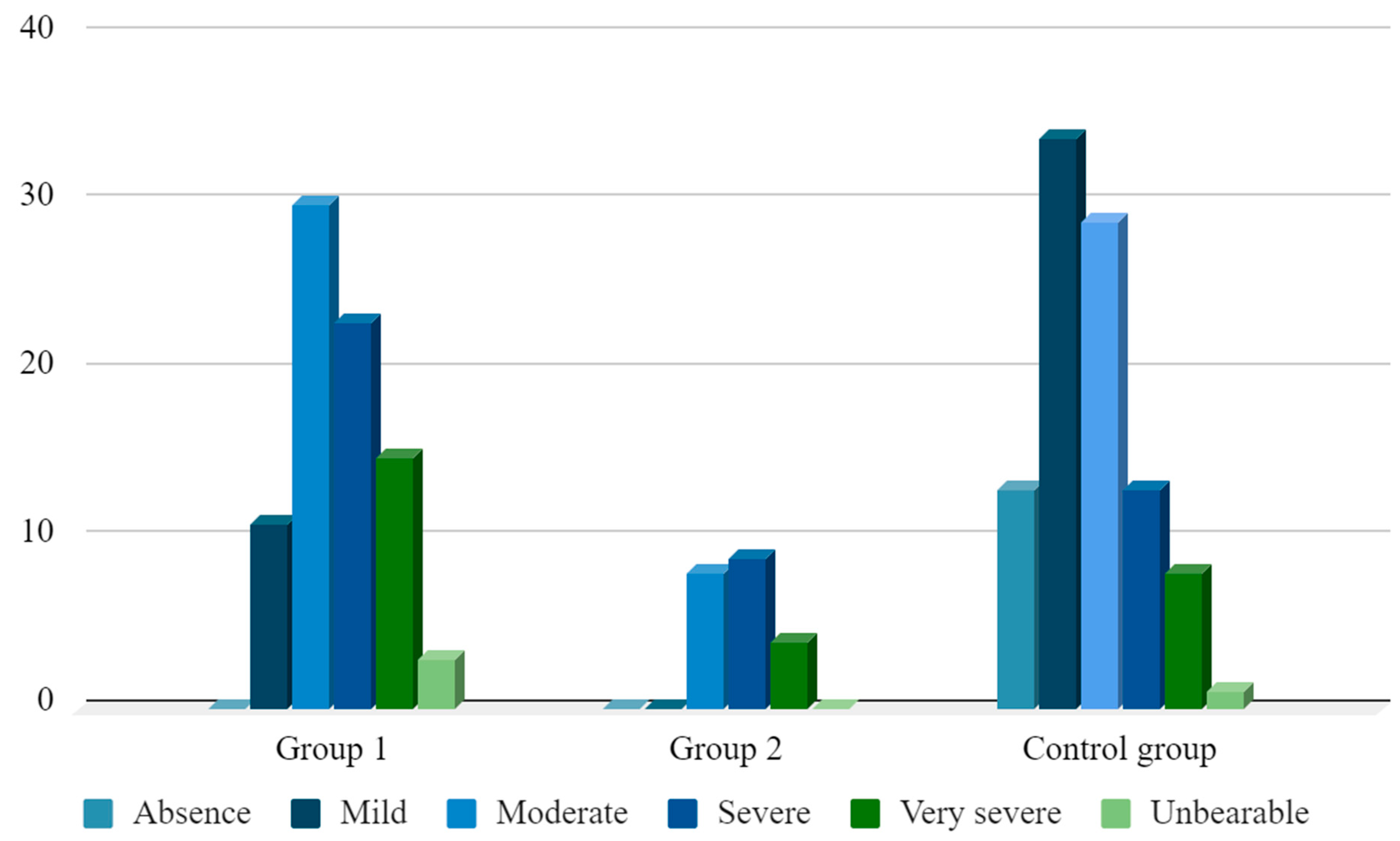
3. Results
- X1—age, years;
- X2—VAS scale on the seventh day, in points;
- X3—evaluation MPQ scale, in points;
- X4—concentration of cortisol in blood on the first day, in nmol/liter.
- -
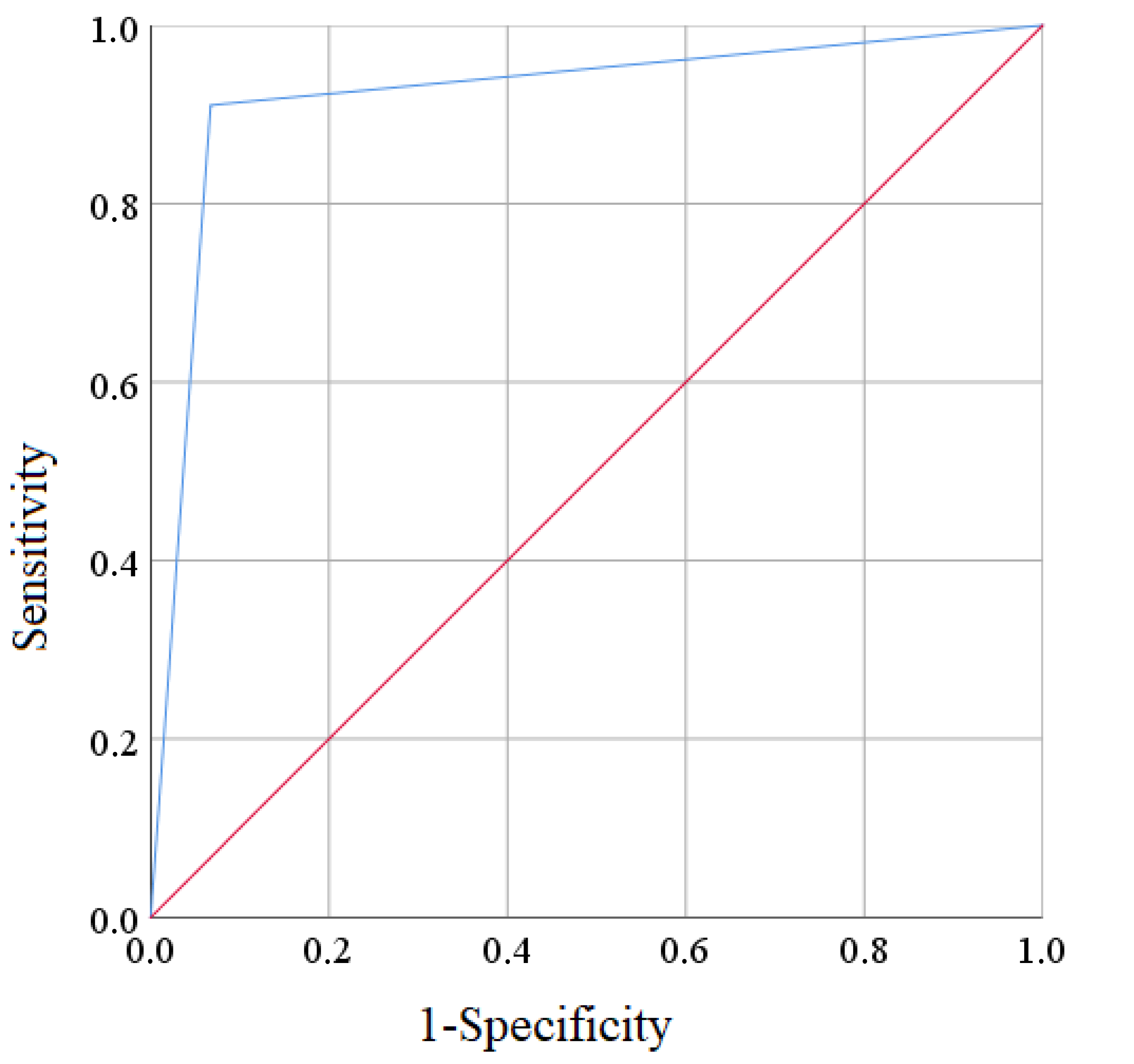
- the probability of a correctly predicted positive result (sensitivity) when using this model—87.1% (95% CI 82.9–91.3%);
- -
- the probability of a correctly predicted negative result (specificity)—95.4% (95% CI 93.7–97.1%);
- -
- the predictability of a positive test result—91.0% (95% CI 85.9–96.1%).
- -
- the predictability of a negative test result—93.3% (95% CI 86.9–99.7%).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zheng, Z.-H.; Yeh, T.-T.; Yeh, C.-C.; Lin, P.-A.; Wong, C.-S.; Lee, P.-Y.; Lu, C.-H. Multimodal Analgesia with Extended-Release Dinalbuphine Sebacate for Perioperative Pain Management in Upper Extremity Trauma Surgery: A Retrospective Comparative Study. Pain Ther. 2022, 11, 643–653. [Google Scholar] [CrossRef]
- Waelkens, P.; Alsabbagh, E.; Sauter, A.; Joshi, G.P.; Beloeil, H. Pain management after complex spine surgery. Eur. J. Anaesthesiol. 2021, 38, 985–994. [Google Scholar] [CrossRef]
- Telegan, V.O.; Shkurupiy, D.A. Clinical characteristics of postoperative analgesia in elderly and old patients. Actual Probl. Mod. Med. Bull. Ukr. Med. Stomatol. Acad 2019, 19, 78–82. [Google Scholar] [CrossRef]
- Starchenko, I.I.; Grinko, R.M.; Shkodina, A.D.; Filenko, B.M.; Vynnyk, N.I.; Roiko, N.V.; Proskurnya, S.A.; Sovhyria, S.M.; Cherniak, V.V.; Babenko, V.I. The Degree of Pineal Gland Calcification in the Aged People is Associated with Changes in the Internal Structure. J. Int. Dent. Med. Res. 2021, 14, 841–844. [Google Scholar]
- Shkodina, A.D.; Grinko, R.M.; Starchenko, I.I.; Vynnyk, N.I.; Sovhyria, S.M.; Kyslyi, V.F. Changes of structural organization of human olfactory bulbs under conditions of severe forms of pneumonia and cerebrovascular pathology. Medicni Perspekt. 2021, 26, 97–104. [Google Scholar] [CrossRef]
- Boiko, D.I.; Kachur, R.V.; Ajala, O.M.; Bodnar, L.A.; Zhyvotovska, L.V. Characteristics of anxiety and depressive manifestations in patients with acute myocardial infarction taking into account their personal accentuations. Azerbaijan Med. J. 2021, 61, 25–31. [Google Scholar]
- Chekalina, N.; Shut, S.V.; A Trybrat, T.; Burmak, Y.H.; Petrov, Y.Y.; I Manusha, Y.; Kazakov, Y. Effect of quercetin on parameters of central hemodynamics and myocardial ischemia in patients with stable coronary heart disease. Wiad. Lek. 2017, 70, 707–711. [Google Scholar]
- Boiko, D.I.; Zhyvotovska, L.V.; Sonnik, G.T.; Skrypnikov, A.M. Clinical and psychopathological characteristics of the autoagressive behavior in patients with the first psychotic episode with considering circadian rhythms. Wiad. Lek. 2017, 70, 553–557. [Google Scholar] [PubMed]
- Schnabel, A.; Yahiaoui-Doktor, M.; Meissner, W.; Zahn, P.K.; Pogatzki-Zahn, E.M. Predicting poor postoperative acute pain outcome in adults: An international, multicentre database analysis of risk factors in 50,005 patients. PAIN Rep. 2020, 5, e831. [Google Scholar] [CrossRef]
- Yang, M.M.H.; Hartley, R.L.; Leung, A.; E Ronksley, P.; Jetté, N.; Casha, S.; Riva-Cambrin, J. Preoperative predictors of poor acute postoperative pain control: A systematic review and meta-analysis. BMJ Open 2019, 9, e025091. [Google Scholar] [CrossRef]
- Consortium of Authors. Control of perioperative pain (Adapted clinical guidance, based on evidence). PMJUA 2018, 2, 6–53. Available online: https://painmedicine.org.ua/index.php/pnmdcn/article/view/70 (accessed on 17 January 2023).
- Thong, I.S.K.; Jensen, M.P.; Miró, J.; Tan, G. The validity of pain intensity measures: What do the NRS, VAS, VRS, and FPS-R measure? Scand. J. Pain 2018, 18, 99–107. [Google Scholar] [CrossRef]
- Fortin, J.D.; Schwartz-Barcott, D.; Rossi, S. The Postoperative Pain Experience. Clin. Nurs. Res. 1992, 1, 292–304. [Google Scholar] [CrossRef] [PubMed]
- Aceto, P.; Incalzi, R.A.; Bettelli, G.; Carron, M.; Chiumiento, F.; Corcione, A.; Crucitti, A.; Maggi, S.; Montorsi, M.; Pace, M.C.; et al. Perioperative Management of Elderly patients (PriME): Recommendations from an Italian intersociety consensus. Aging Clin. Exp. Res. 2020, 32, 1647–1673. [Google Scholar] [CrossRef]
- Zheng, H.; Schnabel, A.; Yahiaoui-Doktor, M.; Meissner, W.; Van Aken, H.; Zahn, P.; Pogatzki-Zahn, E. Age and preoperative pain are major confounders for sex differences in postoperative pain outcome: A prospective database analysis. PLoS ONE 2017, 12, e0178659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ip, H.Y.V.; Abrishami, A.; Peng, P.W.H.; Wong, J.; Chung, F. Predictors of Postoperative Pain and Analgesic Consumption. Anesthesiology 2009, 111, 657–677. [Google Scholar] [CrossRef] [Green Version]
- van Dijk, J.F.M.; Zaslansky, R.; van Boekel, R.L.M.; Cheuk-Alam, J.M.; Baart, S.J.; Huygen, F.J.P.M.; Rijsdijk, M. Postoperative Pain and Age: A Retrospective Cohort Association Study. Anesthesiology 2021, 135, 1104–1119. [Google Scholar] [CrossRef] [PubMed]
- Kanaan, S.F.; Melton, B.L.; Waitman, L.R.; Simpson, M.H.; Sharma, N.K. The effect of age and gender on acute postoperative pain and function following lumbar spine surgeries. Physiother. Res. Int. 2021, 26, e1888. [Google Scholar] [CrossRef]
- Cohn, D.E.; Castellon-Larios, K.; Huffman, L.; Salani, R.; Fowler, J.M.; Copeland, L.J.; O’Malley, D.M.; Backes, F.; Eisenhauer, E.L.; Abdel-Rasoul, M.; et al. A Prospective, Comparative Study for the Evaluation of Postoperative Pain and Quality of Recovery in Patients Undergoing Robotic Versus Open Hysterectomy for Staging of Endometrial Cancer. J. Minim. Invasive Gynecol. 2016, 23, 429–434. [Google Scholar] [CrossRef]
- Betcher, R.E.; Chaney, J.P.; Lacy, P.R.; Otey, S.K.; Wood, D.J. Analysis of postoperative pain in robotic versus traditional laparoscopic hysterectomy. J. Robot. Surg. 2014, 8, 35–41. [Google Scholar] [CrossRef]
- Mangalath, A.S.; Kumar, L.; Sawant, A.B.; Kesavan, R.; Ravindran, G.; Sunil, R. Comparison of analgesic requirements in robot-assisted versus conventional laparoscopic abdominal surgeries. J. Anaesthesiol. Clin. Pharmacol. 2021, 37, 79–84. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| MPQ Indicator | Group | p-Value | ||
|---|---|---|---|---|
| Group 1 (n = 82) | Group 2 (n = 21) | Control Group (n = 98) | ||
| Evaluative scale | 2.62 ± 0.12 * | 2.81 ± 0.16 * | 1.71 ± 0.12 | <0.001 (1:3–<0.001; 2:3–<0.001; 1:2–0.772) |
| RPI on sensory scale | 9.27 ± 0.62 */** | 11.91 ± 1.09 * | 4.75 ± 0.28 | <0.001 (1:3–<0.001; 2:3–<0.001; 1:2–0.045) |
| INSD on sensory scale | 13.77 ± 1.06 */** | 30.86 ± 3.39 * | 6.05 ± 0.37 | <0.001 (1:3–<0.001; 2:3–<0.001; 1:2–<0.001) |
| RPI on affective scale | 5.32 ± 0.39 * | 4.91 ± 0.73 * | 1.99 ± 0.14 | <0.001 (1:3–<0.001; 2:3–<0.001; 1:2–0.968) |
| INSD on affective scale | 6.40 ± 0.44 ** | 11.52 ± 1.55 * | 6.23 ± 0.42 | <0.001 (1:3–0.892; 2:3–<0.001; 1:2–<0.001) |
| Parameter | Coefficient B ± m | Odds Ratio | 95% Confidence Index | p-Value |
|---|---|---|---|---|
| Constant | −10.01 ± 4.66 | - | - | 0.031 * |
| Age | 0.78 ± 0.03 | 1.08 | 1.02–1.15 | 0.009 * |
| VAS, day | 0.23 ± 0.06 | 1.26 | 1.13–1.41 | <0.001 * |
| Evaluative MPQ scale | 2.43 ± 1.05 | 11.37 | 1.45–88.96 | 0.021 * |
| Cortisol, the first day | 0.86 ± 0.08 | 2.36 | 1.07–4.99 | 0.013 * |
| Cases That Have Been Observed | Predicted Cases | Total | |
|---|---|---|---|
| Persistence of Pain Was Predicted | No Pain Persistence Was Predicted | ||
| Patients with persistent postoperative pain | 61 | 6 | 67 |
| Patients without persistent postoperative pain | 9 | 125 | 134 |
| Total | 70 | 131 | 201 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Telegan, V.O.; Tsagkaris, C.; Singh, S.K.; Tarasenko, K.V. Subjective Assessments and Serum Cortisol Levels as Risk Factors of Pain Persistence in the Late Postoperative Period in Old and Oldest-Old Patients. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 450-459. https://doi.org/10.3390/ejihpe13020034
Telegan VO, Tsagkaris C, Singh SK, Tarasenko KV. Subjective Assessments and Serum Cortisol Levels as Risk Factors of Pain Persistence in the Late Postoperative Period in Old and Oldest-Old Patients. European Journal of Investigation in Health, Psychology and Education. 2023; 13(2):450-459. https://doi.org/10.3390/ejihpe13020034
Chicago/Turabian StyleTelegan, Vladyslav O., Christos Tsagkaris, Sandeep Kumar Singh, and Kostiantyn V. Tarasenko. 2023. "Subjective Assessments and Serum Cortisol Levels as Risk Factors of Pain Persistence in the Late Postoperative Period in Old and Oldest-Old Patients" European Journal of Investigation in Health, Psychology and Education 13, no. 2: 450-459. https://doi.org/10.3390/ejihpe13020034