
Randomized Controlled Trial of Home Telemonitoring of Blood Pressure with an Adapted Tensiometer with SMS Capability


Abstract
:1. Introduction
2. Materials and Methods
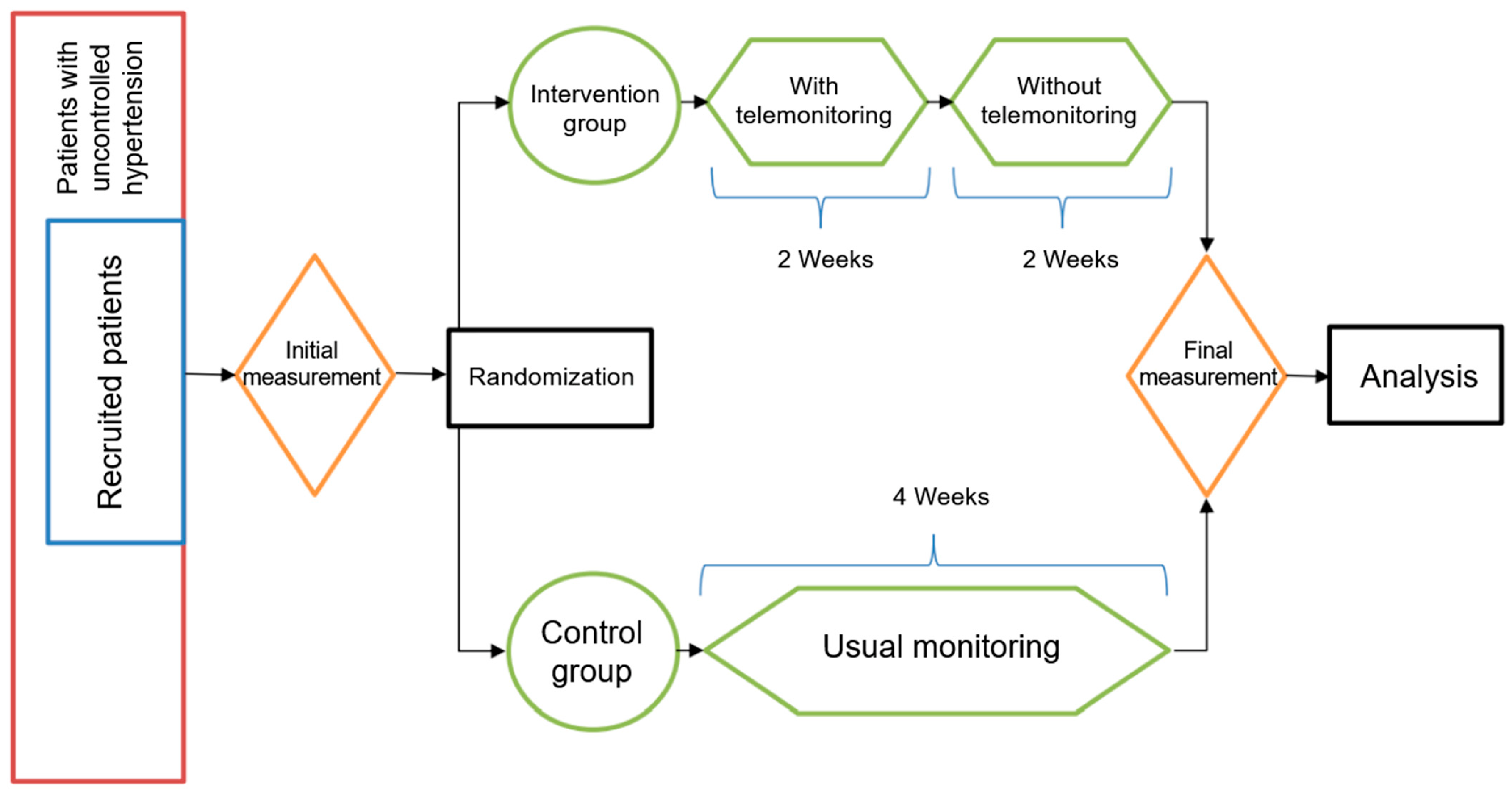
2.1. Study Design
2.2. Participants’ Enrollment
2.3. Randomized Grouping
2.4. Sample Size
2.5. Intervention
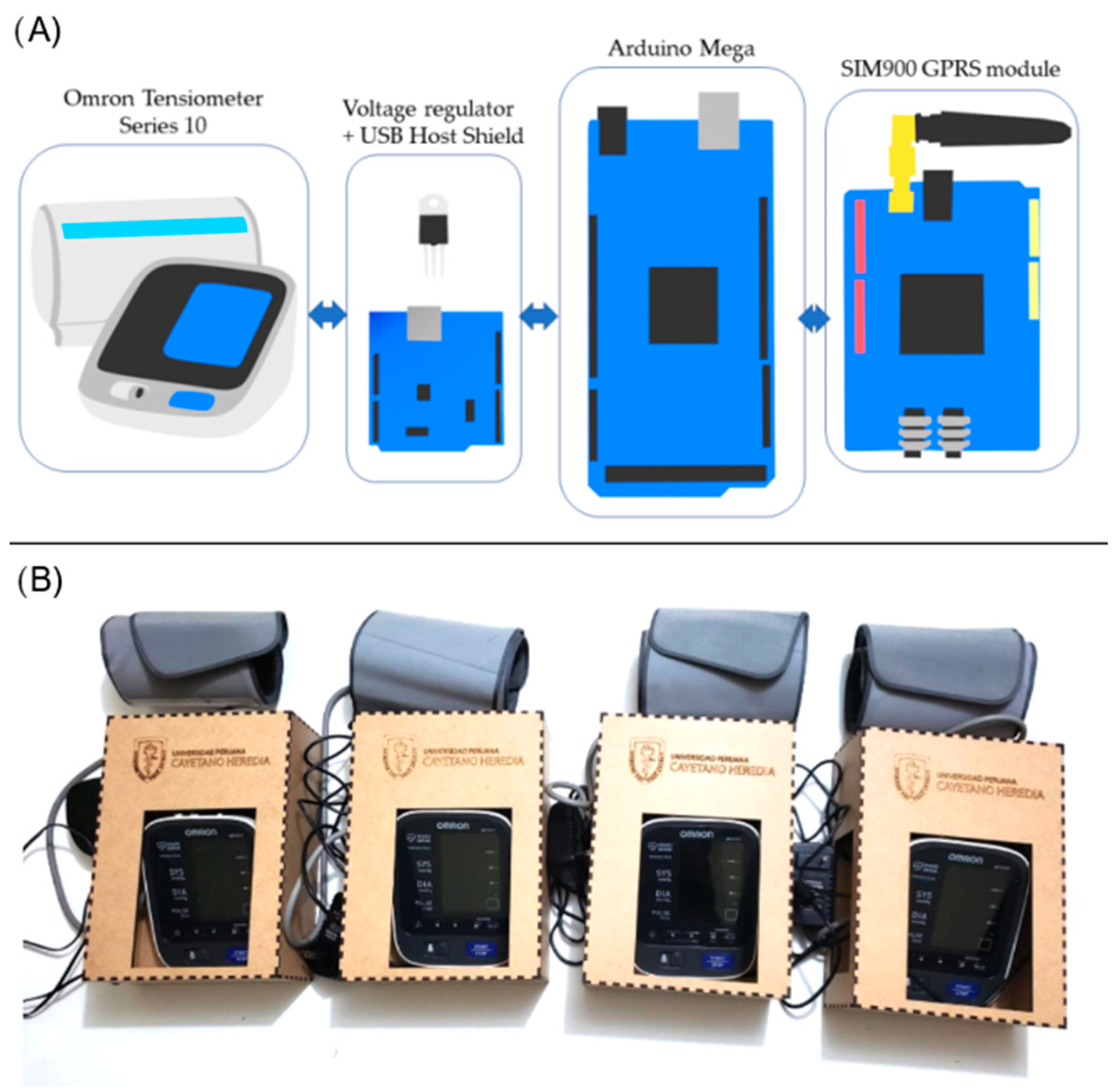
2.5.1. Development of the Telemonitoring System
2.5.2. Hardware Development
2.5.3. Software Development
2.5.4. Telemonitoring Protocol
2.5.5. Technical and Process Aspects
- Patient training: The patient is trained on how to properly use the blood pressure monitor and how to accurately record the readings.
- Equipment: A blood pressure monitor with telemonitoring capability, such as an adapted tensiometer with SMS capability, is provided to the patient.
- Monitoring frequency: The frequency of monitoring was determined and agreed upon between the patient and healthcare provider in two measurements in the morning and two measurements at night spaced out by 5 min each daily, after 1 min of rest.
- Data transmission: The patient takes their blood pressure readings, and the telemonitoring capability of the blood pressure monitor transmits the data to their healthcare provider using via SMS.
- Review by a healthcare provider: The healthcare provider receives the transmitted data and reviews the readings to monitor the patient’s blood pressure and identify any potential issues.
- Follow-up: The healthcare provider may schedule a follow-up appointment with the patient, if necessary, based on the review of the transmitted data.
2.6. Study Setting
2.7. Statistical Analysis
3. Results
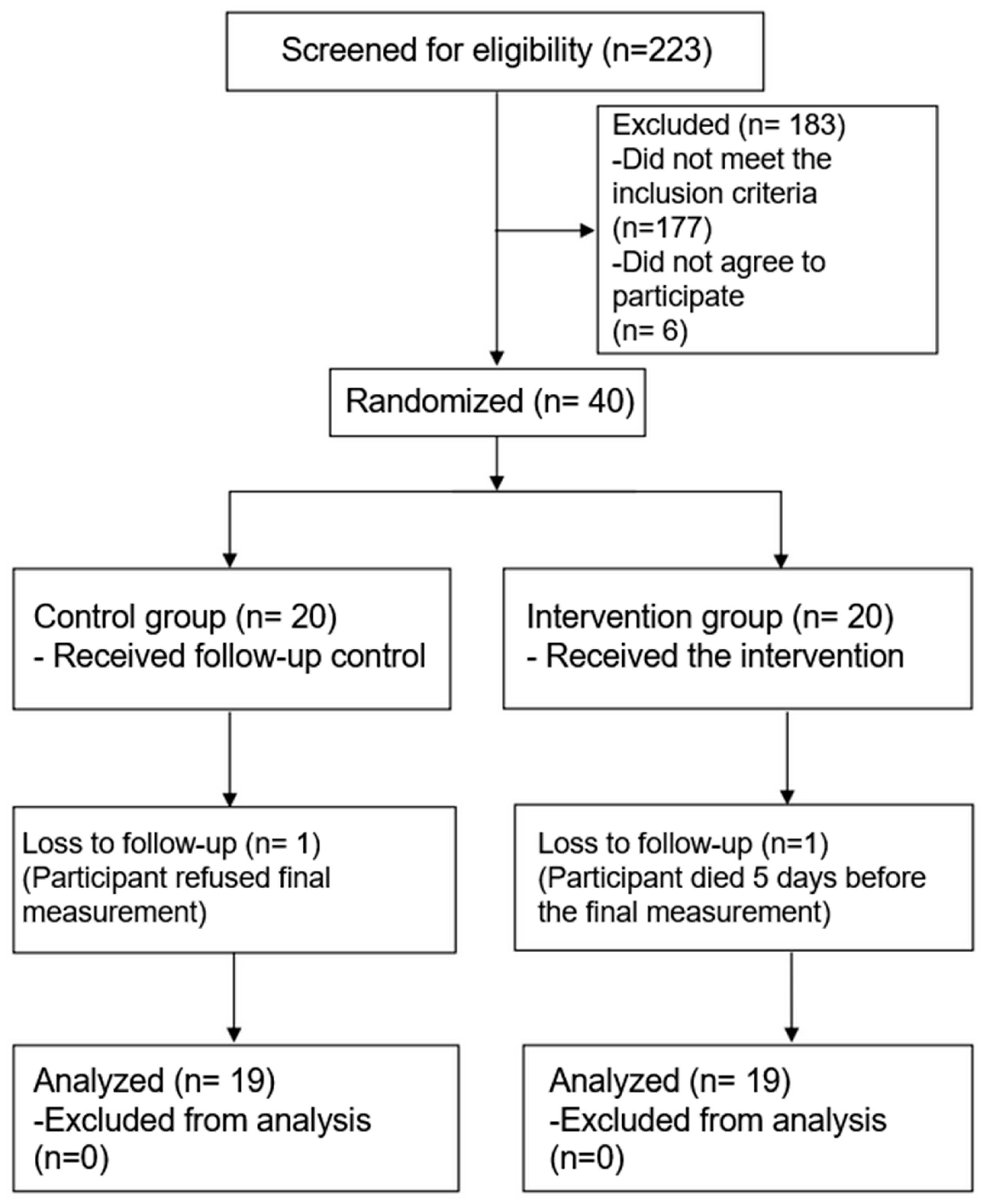
3.1. Recruitment of Participants
3.2. Baseline Characteristics
3.2.1. Demographics Data
3.2.2. Clinical Data
3.3. Primary Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Beaney, T.; Schutte, A.E.; Tomaszewski, M.; Ariti, C.; Burrell, L.M.; Castillo, R.R.; Charchar, F.J.; Damasceno, A.; Kruger, R.; Lackland, D.T.; et al. May Measurement Month 2017: An analysis of blood pressure screening results worldwide. Lancet Glob. Health 2018, 6, e736–e743. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Jaramillo, P.; Lopez-Lopez, J.; Cohen, D.; Alarcon-Ariza, N.; Mogollon-Zehr, M. Epidemiology of Hypertension and Diabetes Mellitus in Latin America. Curr. Hypertens. Rev. 2021, 17, 112–120. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Regional Health-Americas. Latin America and Caribbean’s path to improve hypertension control: Time for bolder, tougher actions. Lancet Reg. Health Am. 2022, 9, 100278. [Google Scholar] [CrossRef]
- Villarreal-Zegarra, D.; Carrillo-Larco, R.M.; Bernabe-Ortiz, A. Short-term trends in the prevalence, awareness, treatment, and control of arterial hypertension in Peru. J. Hum. Hypertens. 2021, 35, 462–471. [Google Scholar] [CrossRef] [PubMed]
- Elnaem, M.H.; Mosaad, M.; Abdelaziz, D.H.; Mansour, N.O.; Usman, A.; Elrggal, M.E.; Cheema, E. Disparities in Prevalence and Barriers to Hypertension Control: A Systematic Review. Int. J. Environ. Res. Public. Health 2022, 19, 14571. [Google Scholar] [CrossRef] [PubMed]
- Pekmezaris, R.; Tortez, L.; Williams, M.; Patel, V.; Makaryus, A.; Zeltser, R.; Sinvani, L.; Wolf-Klein, G.; Lester, J.; Sison, C.; et al. Home Telemonitoring In Heart Failure: A Systematic Review And Meta-Analysis. Health Aff. (Millwood) 2018, 37, 1983–1989. [Google Scholar] [CrossRef]
- Omboni, S.; McManus, R.J.; Bosworth, H.B.; Chappell, L.C.; Green, B.B.; Kario, K.; Logan, A.G.; Magid, D.J.; Mckinstry, B.; Margolis, K.L.; et al. Evidence and Recommendations on the Use of Telemedicine for the Management of Arterial Hypertension. Hypertension 2020, 76, 1368–1383. [Google Scholar] [CrossRef] [PubMed]
- Nerenberg, K.A.; Zarnke, K.B.; Leung, A.A.; Dasgupta, K.; Butalia, S.; McBrien, K.; Harris, K.C.; Nakhla, M.; Cloutier, L.; Gelfer, M.; et al. Hypertension Canada’s 2018 Guidelines for Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension in Adults and Children. Can. J. Cardiol. 2018, 34, 506–525. [Google Scholar] [CrossRef]
- Batista, E.; Moncusi, M.A.; López-Aguilar, P.; Martínez-Ballesté, A.; Solanas, A. Sensors for Context-Aware Smart Healthcare: A Security Perspective. Sensors 2021, 21, 6886. [Google Scholar] [CrossRef]
- Ceballos, F.; Hernandez, M.A.; Olivet, F.; Paz, C. Assessing the use of cell phones to monitor health and nutrition interventions: Evidence from rural Guatemala. PLoS ONE 2020, 15, e0240526. [Google Scholar] [CrossRef]
- Khoong, E.C.; Commodore-Mensah, Y.; Lyles, C.R.; Fontil, V. Use of Self-Measured Blood Pressure Monitoring to Improve Hypertension Equity. Curr. Hypertens. Rep. 2022, 24, 599–613. [Google Scholar] [CrossRef] [PubMed]
- Allen, M.E.; Irizarry, T.; Einhorn, J.; Kamarck, T.W.; Suffoletto, B.P.; Burke, L.E.; Rollman, B.L.; Muldoon, M.F. SMS-Facilitated Home Blood Pressure Monitoring: A Qualitative Analysis of Resultant Health Behavior Change. Patient Educ. Couns. 2019, 102, 2246–2253. [Google Scholar] [CrossRef] [PubMed]
- Gopalakrishnan, S.; Savitha, A.K.; Rama, R. Evaluation of inter-arm difference in blood pressure as predictor of vascular diseases among urban adults in Kancheepuram District of Tamil Nadu. J. Fam. Med. Prim. Care 2018, 7, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Pletcher, M.J.; Fontil, V.; Carton, T.; Shaw, K.M.; Smith, M.; Choi, S.; Todd, J.; Chamberlain, A.M.; O’Brien, E.C.; Faulkner, M.; et al. The PCORnet Blood Pressure Control Laboratory. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e006115. [Google Scholar] [CrossRef] [PubMed]
- Arduino—Home. Available online: https://www.arduino.cc/ (accessed on 5 September 2022).
- Duan, Y.; Xie, Z.; Dong, F.; Wu, Z.; Lin, Z.; Sun, N.; Xu, J. Effectiveness of home blood pressure telemonitoring: A systematic review and meta-analysis of randomised controlled studies. J. Hum. Hypertens. 2017, 31, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Hu, J.; Yao, Y.; Zuo, C.; Wang, Z.; Li, X.; Lv, Q. Evaluation of pharmacist-led telemedicine medication management for hypertension established patients during COVID-19 pandemic: A pilot study. Front. Public Health 2022, 10. [Google Scholar] [CrossRef]
- Park, S.-H.; Shin, J.-H.; Park, J.; Choi, W.-S. An Updated Meta-Analysis of Remote Blood Pressure Monitoring in Urban-Dwelling Patients with Hypertension. Int. J. Environ. Res. Public. Health 2021, 18, 10583. [Google Scholar] [CrossRef]
- Hanley, J.; Pinnock, H.; Paterson, M.; McKinstry, B. Implementing telemonitoring in primary care: Learning from a large qualitative dataset gathered during a series of studies. BMC Fam. Pract. 2018, 19, 118. [Google Scholar] [CrossRef]
- Baratta, J.; Brown-Johnson, C.; Safaeinili, N.; Rosas, L.G.; Palaniappan, L.; Winget, M.; Mahoney, M. Patient and Health Professional Perceptions of Telemonitoring for Hypertension Management: Qualitative Study. JMIR Form. Res. 2022, 6, e32874. [Google Scholar] [CrossRef]
- Pekmezaris, R.; Williams, M.S.; Pascarelli, B.; Finuf, K.D.; Harris, Y.T.; Myers, A.K.; Taylor, T.; Kline, M.; Patel, V.H.; Murray, L.M.; et al. Adapting a home telemonitoring intervention for underserved Hispanic/Latino patients with type 2 diabetes: An acceptability and feasibility study. BMC Med. Inform. Decis. Mak. 2020, 20, 324. [Google Scholar] [CrossRef]
- Hammersley, V.; Parker, R.; Paterson, M.; Hanley, J.; Pinnock, H.; Padfield, P.; Stoddart, A.; Park, H.G.; Sheikh, A.; McKinstry, B. Telemonitoring at scale for hypertension in primary care: An implementation study. PLoS Med. 2020, 17, e1003124. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Control | Intervention | Total | p | |
|---|---|---|---|---|
| Female Sex | 16 (84.2%) | 10 (52.6%) | 26 (68.4%) | 0.079 |
| Age (years) | 68.7 ± 11.5 | 67.5 ± 10.3 | 68.1 ± 10.8 | 0.744 |
| BMI (kg/m2) | 29.4 ± 3.4 | 29.5 ± 4.6 | 29.5 ± 4.0 | 0.988 |
| Born in Lima | 5 (26.3%) | 9 (47.4%) | 14 (36.8%) | 0.313 |
| Marital status | ||||
| Single | 3 (15.8%) | 2 (10.5%) | 5 (13.2%) | 0.026 |
| Married/Cohabiting | 7 (36.8%) | 15 (79.0%) | 22 (57.9%) | |
| Divorced | 1 (5.3%) | 0 | 1 (2.6%) | |
| Widow/widower | 8 (42.1%) | 2 (10.5%) | 10 (26.3%) | |
| Education level | ||||
| Primary | 13 (68.4%) | 11 (57.9%) | 24 (63.2%) | 0.788 |
| High school | 5 (26.3%) | 6 (31.6%) | 11 (29.0%) | |
| Superior | 1 (3.3%) | 2 (10.5%) | 3 (7.9%) | |
| Occupation | ||||
| Housewife | 11 (57.9%) | 9 (47.4%) | 20 (52.6%) | 0.455 |
| Casual work | 2 (10.5%) | 5 (26.3%) | 7 (18.4%) | |
| Permanent job | 6 (31.6%) | 5 (26.3%) | 11 (29.0%) | |
| HTA diagnosis time (months) | 10 (5–12) | 10 (3–16) | 10 (5–15) | 0.918 |
| Treatment | ||||
| ACEI | 15 (79.0%) | 9 (47.4%) | 24 (63.2%) | 0.248 |
| ARA-II | 3 (15.8%) | 5 (26.3%) | 8 (21.1%) | |
| CCB | 0 | 1 (5.3%) | 1 (2.6%) | |
| ARA-II + CCB | 1 (5.3%) | 3 (15.8%) | 4 (10.5%) | |
| ACEI + CCB + ARA-II | 0 | 1 (5.3%) | 1 (2.6%) | |
| Family history of high blood pressure | 10 (52.6%) | 11 (57.9%) | 21 (55.3%) | 1 |
| Comorbidities | ||||
| Diabetes | 6 (31.6%) | 3 (15.8%) | 9 (23.7%) | 0.447 |
| Others | 14 (73.7%) | 12 (63.2%) | 26 (68.4%) | 0.728 |
| Control | Intervention | Total | p | P MW | |
|---|---|---|---|---|---|
| Baseline measurement (BM) | |||||
| SBP (mmHg) | 157.0 ± 15.2 | 156.3 ± 12.4 | 156.7 ± 13.7 | 0.880 | 0.9301 |
| DBP (mmHg) | 84.8 ± 9.1 | 88.3 ± 9.9 | 86.6 ± 9.6 | 0.276 | 0.3128 |
| Final measurement (FM) | |||||
| SPB (mmHg) | 149.8 ± 17.4 | 140.1 ± 12.6 | 144.9 ± 15.8 | 0.056 | 0.111 |
| DBP (mmHg) | 83.6 ± 10.9 | 81.1 ± 10.3 | 82.3 ± 10.3 | 0.460 | 0.6180 |
| FM–BM | |||||
| SBP (mmHg) | −7.2 ± 14.9 | −16.3 ± 16.7 | −11.7 ± 16.3 | 0.087 | 0.0470 |
| DBP (mmHg) | −1.2 ± 6.4 | −7.2 ± 9.8 | −4.2 ± 8.7 | 0.032 | 0.0452 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calderón-Anyosa, R.; Tincopa, J.P.; Raza, M.; Cárcamo, C.P. Randomized Controlled Trial of Home Telemonitoring of Blood Pressure with an Adapted Tensiometer with SMS Capability. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 440-449. https://doi.org/10.3390/ejihpe13020033
Calderón-Anyosa R, Tincopa JP, Raza M, Cárcamo CP. Randomized Controlled Trial of Home Telemonitoring of Blood Pressure with an Adapted Tensiometer with SMS Capability. European Journal of Investigation in Health, Psychology and Education. 2023; 13(2):440-449. https://doi.org/10.3390/ejihpe13020033
Chicago/Turabian StyleCalderón-Anyosa, Renzo, Jean Pierre Tincopa, Mabel Raza, and Cesar P. Cárcamo. 2023. "Randomized Controlled Trial of Home Telemonitoring of Blood Pressure with an Adapted Tensiometer with SMS Capability" European Journal of Investigation in Health, Psychology and Education 13, no. 2: 440-449. https://doi.org/10.3390/ejihpe13020033