1. Introduction
Occupational exposure remains a global health hazard as a result of population growth and industrialization. Workers all around the world are being exposed to hazardous substances as a result of their line of work, resulting in a worldwide health crisis [
1]. Despite improvements in workplace technology, practices, and exposures over the past few decades, occupational hazards remain a significant source of morbidity and mortality in several countries and worldwide [
2]. The International Labour Organization estimates that 5–7% of global fatalities are caused by occupational diseases and injuries [
3]. They are a major source of disability and absence from work among the working population [
4]. Interstitial lung disease and respiratory malignancies accounted for one-third of the cases of occupational disease [
5]. Workers in low- and middle-income countries (LMICs) are at a higher risk of occupational diseases; in 2016, workers in LMICs accounted for more than 92% of unintentional occupational injury deaths [
6]. The fact that factory workers, particularly in LMICs, do not receive adequate medical attention exacerbates the situation; it is estimated that less than 15% of the global workforce is covered by occupational health services [
7].
The last few decades have seen a rise in the widespread use of chemical cleaning products. Cleaning agents can be liquids, sprays, powders, or granules. Examples include oven cleaners (containing sodium hydroxide), toilet cleaners, hygiene and deodorant products (containing hydrochloric, phosphoric, or formic acids), metal cleaners (containing fatty alcohol or alkyl phenol polyglycol ethers, ethylene oxide, and ammonia), and glass cleaners (containing thiourea, ethanol or isopropanol, hydrochloric or sulfuric acid, and possibly small amounts of ammonia) [
8,
9,
10].
According to the International Labour Organization fact sheet outlining the risks and preventative measures associated with this occupation, the risks these workers face include accidental exposure to toxic substances as well as dust from detergent and raw material manufacturing (phosphates, sulfates, and other substances), which can irritate the skin and eyes and affect the respiratory system. In addition, exposure to dust containing enzymes during detergent production may induce skin irritation and allergic reactions of the respiratory system; exposure to excessive levels of this dust can cause asthma [
11]. A cross-sectional study of detergent workers in the Netherlands found that they are exposed to proteases, a-amylase, lipase, and cellulase, with the maximum exposures occurring in the mixing area. Liquid spills with concentrated enzyme preparations and leakage of enzymes during weighing, transportation, and filling were causing workplace contaminations and subsequently leading to both dermal and inhalation exposure for workers [
12].
Cleaning is primarily intended to safeguard health; however, the hazardous chemicals or substances contained in these products expose workers in chemical industries to these chemicals, putting them at risk for health problems, especially over the long term. The presence of respiratory sensitizers in cleaning products, such as enzymes and powder, has been related to occupational asthma in employees. Exposure to cleaning sprays, chlorine bleach, and other disinfectants may be especially important, resulting in both specific sensitization and irritant-related features [
13]. In addition to being irritants, they can induce short- or long-term respiratory diseases, including chronic bronchitis [
14]. In a meta-analysis and systematic review of cleaning agents and respiratory health outcomes in occupational cleaners, Archangelidi O et al. reported that cleaners had a 50% higher relative risk of asthma and a 43% higher risk of chronic obstructive pulmonary disease [
10,
15]. This includes both new-onset and work-aggravated asthma, which may be induced by cleaning exposure [
13].
Pulmonary function tests (PFTs) are parameters to assess lung function and changes in lung function over time are an important indicator of lungs health. Spirometry is a physiological test that measures the maximum amount of air a person can inhale and exhale with the greatest effort [
16]. It assesses and monitors general respiratory health as well as the mechanical features of the respiratory system by measuring expiratory volumes and flow rates. Parameters are recorded as forced vital capacity (FVC), peak expiratory flow (PEF), forced expiratory volume in the first second (FEV1), FEV1/FVC ratio, and forced expiratory flow between 25–75% of FVC (FEF25–75%) [
17]. Another important spirometry-derived parameter is estimated lung age, which was introduced in 1985 to make spirometry data easier to understand and as a physiological tool to monitor lung function decline [
18].
The effect of chemical materials and cleaning agents on the respiratory system has been studied in the literature, particularly using the spirometer, which showed a marked decrease in lung functions parameters. An Iranian study evaluated pulmonary function among detergent factory workers reported that the mean percentage of all spirometry indices significantly reduced including FVC, FEV1, FEV1/FVC ratio, PEF, and FEF (25–75) [
19]. A Nigerian study compared the pulmonary function of detergent factory workers exposed to alkyl benzene sulphonate to workers in the same factory who were not exposed. They concluded that exposed workers had significantly higher frequency of respiratory symptoms and lower FEV, FVC, and PEF than the unexposed workers [
20].
The state of Palestine is a developing country that is still under occupation, where the economic situation is challenging, and where occupational health and safety among workers is a concern. According to a study on a group of workers in the Gaza Strip, their occupational health and safety are constantly deteriorating, and none of them have ever received occupational health and safety training [
21]. Additionally, the yearly growth in the number of workplace accidents and diseases in the Palestinian manufacturing industry shows that there is a serious threat to occupational safety and health [
22]. The aim of this study is to assess the pulmonary function among detergents factory workers, and to compare their spirometry profiles to control workers. The study’s findings should improve our awareness of the health conditions of Palestinian chemical industrial workers and lead the way for health promotion activities and tighter policy monitoring. Healthcare workers in Palestine and the region can use these findings to better educate people about the risk of cleaning or chemical agents, as well as to encourage workers to follow safety measures and instructions.
2. Method
2.1. Study Design and Population
A comparative cross-sectional study was conducted to compare the lung function of detergent factory workers to that of a control group of workers from non-detergent factories. It involved 28 detergent factory workers in three West Bank factories located in the three main cities of the middle and north West Bank; Jenin, Nablus, and Ramallah. As well, it involved 66 non-detergent factory workers (comparison group) from the same surrounding areas of the three cities. The data collection and analysis of workers’ pulmonary functions for his study were conducted over a period of three months, from June to August of 2021. The main selection criterion in this study was continuous employment in detergent factory for at least a year, as this time should be enough for chronic inflammatory alterations to develop. In addition, there must be no history of similar occupations, such as chemical manufacturing, painting, or farming, that may have influenced the lungs by causing inflammatory alterations during or before the study period. We included all of the workers in each of the three factories who had direct contact with chemicals and were in charge of manufacturing detergents within the facility in a closed system. The manufacturing process consists of preparing and weighing the raw materials, mixing the chemicals, and constructing packaging. The comparison group included 66 healthy males who had never worked in a detergent or chemical factory or any other facility that could have an impact on lung function. They were selected from the same areas of the detergent factories and represented a variety of professions, including those in supermarkets, grocery stores, sweets shops, and taxi driving. People from either group (detergent factory workers and non-chemical workers) who exhibited the following attributes were excluded from the study: females, males under 18 years of age, those with any underlying medical condition that could alter spirometry results, such as asthma, hypersensitivity pneumonitis, cystic fibrosis, bronchiolitis, COPD, presence of comorbidities (neoplasia, cardiovascular disease), and chronic bronchitis treated with bronchodilators. The study was approved by the Institutional Review Board at An-Najah National University [Reference#: F. Med Sep. /2020/5]. All participants in the study were required to sign an informed consent form after being informed of the study’s objectives, potential risks, and the fact that participation was voluntary. The study subjects’ anonymity and confidentiality were carefully maintained both throughout and after the study period. All methods were carried out in accordance with relevant guidelines and regulations.
2.2. Sample Size
We determined the sample size using the software Epi Info [
23]. We calculated it using the following parameters: 95% confidence interval, 80% test power, expected FVC% 82.0 ± 12.0 for detergent factory workers group, and expected FVC% 89.0 ± 12.0 for comparison workers. On the basis of this information, the sample size was determined to be 35 detergent factory workers and 70 control workers in a ratio of 1:2. To reach the calculated sample size, we intended to include many detergent factory workers in the middle and north West Bank; however, three factories declined to participate in the study and enable us to examine their workers. For the control, a multi-stage sampling method was used. The central taxi park in Jenin’s city center connects to five important streets. Starting with the tenth door on the right side of each street, systemic sampling was used to select one building door every ten doors, beginning with the tenth door. Using simple random sampling, one house from each building was selected, and one person matching the inclusion criteria was selected from the house for spirometry. The same procedure was followed in the other two cities: Nablus and Ramallah.
2.3. Procedure and Data Collection
We evaluated the lung function by using a CareFusion Micro Lab ML3500 MK8 Spirometer which is fully compliant with the American Thoracic Society (ATS) and European Respiratory Society (ERS) 2005 Standard. Participants were initially given an overview of the spirometer’s principle, operation, and method, and were encouraged and guided during the entirety of the test performance by the investigators. A sitting position was employed throughout testing to reduce the risk of falling and harm in the event of a syncopal episode, although PFTS can be conducted in the standing position. Additionally, participants were encouraged to refrain from smoking for at least an hour before testing and from eating a large meal for at least two hours before testing as these may affect the results [
24]. Bronchodilators (if taken by any worker) were prohibited for at least 4 h before the test due to their effect on the PFTs, particularly by masking the obstructive respiratory pattern [
25]. The participant’s data were all documented in the Micro Lab ML3500 MK8 Spirometer. The following spirometry values were recorded: FEV1: the amount of air a person may forcefully expel in liters within the first second after maximal inhalation, FVC: the volume of air that can be exhaled in liters after taking the deepest possible inhalation., PEF: the maximum expiratory flow (L/min) obtained during a forced expiration beginning immediately after a deep inhalation based on total lung capacity, FEF (25−75): the average forced expiratory flow rate at 25–75% of the vital capacity, and the FEV1/FVC ratio and their percentages [
17]. Additionally, we estimated the participants’ lung age to be compared with their chronological age.
For the background and general health characteristics, we used a self-administered questionnaire that was designed by the researchers in the Arabic language. The questionnaire contained two main parts. The first part included questions about workers’ sociodemographic characteristics such as their age, smoking status, and physical activity status, which was defined as engage in 150 min of moderate-intensity aerobic activity per week, or at least 75 min of vigorous-intensity aerobic physical activity, or an equivalent combination of moderate- and vigorous exercise [
26]. The second part addressed the occupational condition of the participants, namely their employment in chemical detergent factories, duration of employment in these industries, and daily working hours. Additionally, we used a weighing scale and a meter to measure participants anthropometrics (weight in kilograms, height in centimeters) and computed their body mass index (BMI).
2.4. Statistical Analysis
All obtained data were entered and analyzed using the Statistical Packages for Social Sciences (SPSS) software version. The mean and standard deviation of spirometric data were computed, and the Mann–Whitney U Test and the chi-squared test were used to analyze the difference between the detergent factory workers and comparison groups. The level of significance was set at 0.05.
3. Results
The sample included 94 participants: 28 detergent factories workers and 66 comparison individuals. The participants’ ages ranged from 18 to 43 years, with a mean age of 31.1 ± 11.6. There were no females among the participants. A total of 59 (62.8%) of the participants were smokers (19 detergent factory workers and 40 from the comparison group) and 35 (37.2%) of them were non-smokers (9 detergent factory workers and 26 from the comparison group). There was no significant difference in age, BMI, and smoking status between the two groups (
p-value > 0.05) (
Table 1). The median number of working hours per day for detergent factory workers was 8 h, ranging from three to ten hours, while the median duration of employment in the factories was 7 years, ranging from one to twenty years.
As shown in
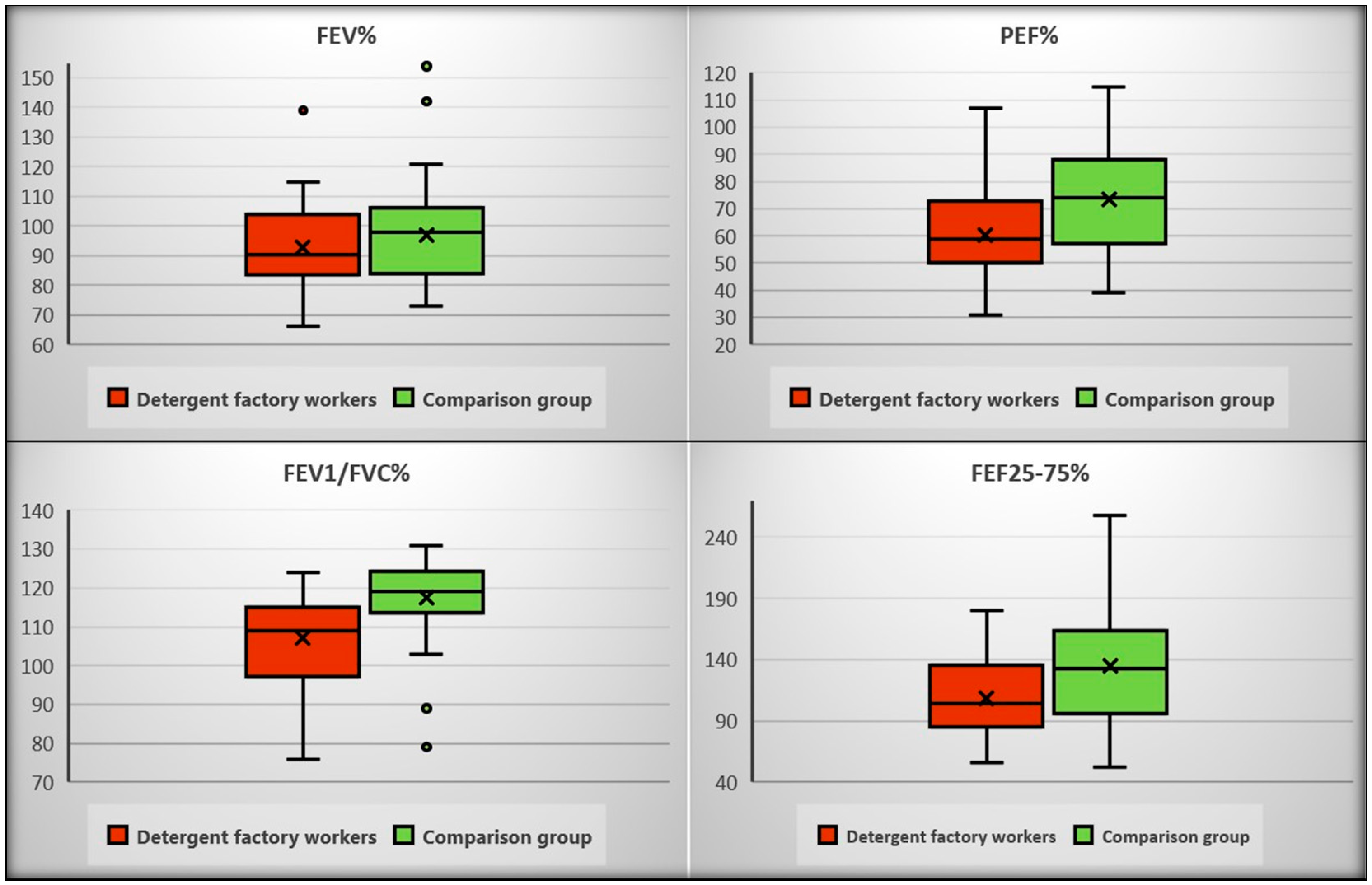
Table 2, there were significant differences in spirometry parameters between the two groups (
p < 0.05), except for forced vital capacity (FVC). Participants from the comparison group obtained better outcomes in peak expiratory flow (PEF), forced expiratory volume at 1 s (FEV1), FEV1/FVC%, and forced expiratory flow FEF 25–75.
Detergent factory workers had a higher lung age than the comparison group (44.2 ± 16.9 versus 36.0 ± 14.8) this can make breathing slightly more difficult. The difference was statistically significant (p < 0.05).
Figure 1 presents the difference in spirometry parameters (FEV%, PEF%, FEV1/FVC, and Forced expiratory flow FEF 25–75%) between the detergent factory workers and the comparison group.
4. Discussion
The International Labor Organization has long recognized that safeguarding employees from hazardous substances is critical to ensuring healthy populations and long-term environmental sustainability. Despite this, workers continue to be subjected to disproportionate levels of chemical exposure in almost every occupational field [
1]. Occupational lung diseases are the most frequent work-related conditions that contribute to worldwide health concerns. They are related to long-term occupational exposure to irritants such as lung irritants, which are known to aggravate chronic respiratory disorders. The literature on the effects of working in detergent factories is limited, particularly in developing countries. Notwithstanding the small sample size and other limitations, we hope that the findings of this study, which is the first in Palestine to examine the impact of working in detergent factories on the pulmonary function test, will expand the literature on the subjects and shed light on this problem.
This cross-sectional study compared the lung functions of detergent company workers, who served as the exposed group, to those of non-chemical workers, who served as the comparison group. We demonstrated that the main lung function parameters of detergent company employees decreased significantly compared to the non-chemical workers. In this study, age, weight, height, BMI, smoking, and physical activity were similar in both groups (detergent company workers and the comparison group) and were considered to have no effects on results.
Long-term exposure to chemical irritants such as dust, exhausts, fuels, and detergents has been linked to respiratory difficulties in numerous studies [
19,
20,
27]. Our study showed that most spirometric parameters (FEV1, PEF, PEF%, FEV1/FVC, FEV1/FVC%, FEF25–75, and FEF25–75%) were lower in the detergent company workers when compared to the non-chemical workers, except for FVC. Additionally, the detergent company workers have higher lung age. The mean parameter differences between the detergent company workers and comparison group were statistically significant (
p-value < 0.05). These findings are in line with the results of the limited number of studies that we were able to find. In Nigeria, a 2008 study by Babashani et al. found that lung function parameters, particularly FEV1, FVC, and PEFR, were significantly lower among detergent workers [
20]. Moreover, Malek et al. revealed that workers in detergent powder factories had a significant loss in lung function, FEV1, FEV1/FVC, and FEF25–75 [
19]. According to Ibraheem TM et al., the significantly reduced values of multiple respiratory function parameters (FVC, FVC%, and FEV1) among detergent industry production workers is attributed to exposure to some of the compounds utilized in the sector [
28]. In accordance with our findings, a cross-sectional study of detergent product workers found both restrictive (52%) and obstructive (2.4%) lesions, with over 65% radioallergosorbent testing (RAST) grade III. Moreover, RAST grade III workers showed decreased lung function, as measured using FVC and FEV1 [
28].
Interestingly, our results find that there is a larger reduction in the mid-flow rate (FEF25–75%). FEF is effort independent and highly sensitive for early airway and lung diseases. Both restriction and obstruction diseases were seen in detergent workers [
19]. Although the results, despite being statistically significant, remain within the normal clinical range, they should be taken seriously because pulmonary function changes increase over time. Cullinan et al. revealed that the longest length of protease (one of four types of enzymes used in detergents) exposure resulted in lower respiratory tract illnesses, but the lowest period of exposure increased the risk of upper respiratory tract disorders [
5]. These findings highlight the necessity of enforcing policies and implementing interventions pertaining to occupational and work-related illnesses and injuries. These interventions can be both clinical, such as health examinations and regular checkups, and nonclinical, such as workplace risk assessment, and they can be both preventive and treatments. Typically, preventive interventions are offered to people who are not seeking help and who do not have symptoms [
29]. The World Health Organization calls for greater access to essential interventions and basic occupational health services, particularly in agriculture, small- and medium-sized businesses, the informal economy, and migrant workers [
30]. In addition to improving workplace conditions, enhancing workers’ awareness of occupational safety and providing them with safety training can lower the risks associated with their working conditions. Furthermore, a study on occupational health and safety knowledge, attitudes, and practice among students in Palestine recommended that clinical training departments and universities continue to offer occupational health and safety courses and training for health science students [
31]. The use of respiratory protective equipment, such as masks, can reduce the likelihood of developing occupational lung diseases. Grammer et al. concluded that occupational asthma induced by hexahydrophthalic anhydride was decreased by 80%, owing primarily to respiratory protection [
32].
Strengths and Limitations
To the best of our knowledge, this is the first study in Palestine to evaluate the spirometry features of the detergent factories’ workers. We believe that this study provides light on an essential health issue as well as a highly important component of community, workers. As a result, we think it will help to raise awareness among workers and the local population in general, whether in Palestine or the surrounding region. However, certain limitations should be considered when interpreting the results of this study. First, we only looked at the effects of detergents on lung function using a spirometry test, and we did not consider clinical symptoms such as cough and exertional dyspnea that this occupational population would experience. Second, a lack of information on both groups’ occupational histories, such as duration of work, past exposures, and home characteristics, could have influenced the results. Third, we were unable to acquire the anticipated sample size since not all factories agreed to participate in the study; as a result, the small sample size we ended up with may have limited the study’s power and representativeness. Lastly, the healthy workers effect cannot be ignored in this study, since it is likely that the workers present in the workplaces at the time of the study are the healthiest. This would indicate that the results of the study underestimate the magnitude of the problem that our workers face.


 ,
, 


{kind=link}