
Audiological Risk Factors, Referral Rates and Dropouts: 9 Years of Universal Newborn Hearing Screening in North Sardinia

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Outcomes and Population
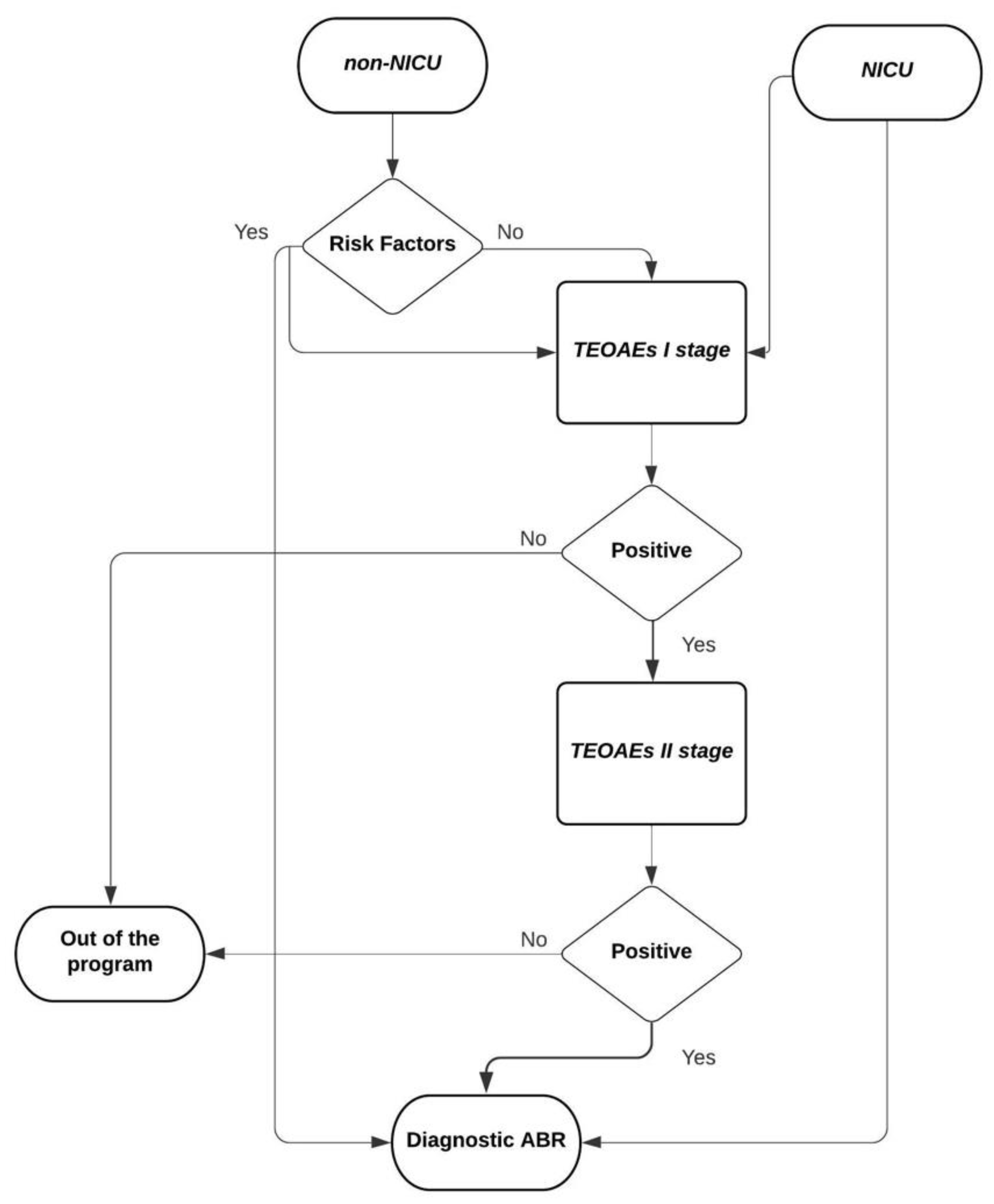
2.2. Our Screening Program
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Korver, A.M.H.; Smith, R.J.H.; Van Camp, G.; Schleiss, M.R.; Bitner-Glindzicz, M.A.K.; Lustig, L.R.; Usami, S.-I.; Boudewyns, A.N. Congenital Hearing Loss. Nat. Rev. Dis. Prim. 2017, 3, 16094. [Google Scholar] [CrossRef]
- Yoshinaga-Itano, C.; Sedey, A.L.; Wiggin, M.; Mason, C.A. Language Outcomes Improved Through Early Hearing Detection and Earlier Cochlear Implantation. Otol. Neurotol. 2018, 39, 1256–1263. [Google Scholar] [CrossRef]
- American Academy of Pediatrics; Joint Committee on Infant Hearing. Year 2007 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs. Pediatrics 2007, 120, 898–921. [Google Scholar] [CrossRef] [PubMed]
- Wroblewska-Seniuk, K.E.; Dabrowski, P.; Szyfter, W.; Mazela, J. Universal Newborn Hearing Screening: Methods and Results, Obstacles, and Benefits. Pediatr. Res. 2017, 81, 415–422. [Google Scholar] [CrossRef]
- Vohr, B.R.; Oh, W.; Stewart, E.J.; Bentkover, J.D.; Gabbard, S.; Lemons, J.; Papile, L.A.; Pye, R. Comparison of Costs and Referral Rates of 3 Universal Newborn Hearing Screening Protocols. J. Pediatr. 2001, 139, 238–244. [Google Scholar] [CrossRef] [PubMed]
- van Dyk, M.; Swanepoel, D.W.; Hall, J.W., 3rd. Outcomes with OAE and AABR Screening in the First 48 H--Implications for Newborn Hearing Screening in Developing Countries. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1034–1040. [Google Scholar] [CrossRef]
- Ricalde, R.R.; Chiong, C.M.; Labra, P.J.P. Current Assessment of Newborn Hearing Screening Protocols. Curr. Opin. Otolaryngol. Head Neck Surg. 2017, 25, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Ravi, R.; Gunjawate, D.R.; Yerraguntla, K.; Lewis, L.E.; Driscoll, C.; Rajashekhar, B. Follow-up in Newborn Hearing Screening—A Systematic Review. Int. J. Pediatr. Otorhinolaryngol. 2016, 90, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Gallus, R.; Rizzo, D.; De Luca, L.M.; Melis, A.; Kihlgren, C.; Parente, P.; Anzivino, R.; Frezza, S.; Priolo, F.; Bussu, F.; et al. Does the Involvement of First-Year Residents Have a Negative Impact on the Performance of a Newborn Hearing Screening Program? Int. J. Pediatr. Otorhinolaryngol. 2020, 138, 110270. [Google Scholar] [CrossRef]
- Vos, B.; Senterre, C.; Lagasse, R.; SurdiScreen Group; Levêque, A. Newborn Hearing Screening Programme in Belgium: A Consensus Recommendation on Risk Factors. BMC Pediatr. 2015, 15, 160. [Google Scholar] [CrossRef]
- Busonero, F.; Steri, M.; Orrù, V.; Sole, G.; Olla, S.; Marongiu, M.; Maschio, A.; Sidore, C.; Lai, S.; Mulas, A.; et al. A Sardinian Founder Mutation in Glycoprotein Ib Platelet Subunit Beta (GP1BB) That Impacts Thrombocytopenia. Br. J. Haematol. 2020, 191, e124–e128. [Google Scholar] [CrossRef] [PubMed]
- Frezza, S.; Catenazzi, P.; Gallus, R.; Gallini, F.; Fioretti, M.; Anzivino, R.; Corsello, M.; Cota, F.; Vento, G.; Conti, G. Hearing Loss in Very Preterm Infants: Should We Wait or Treat? Acta Otorhinolaryngol. Ital. 2019, 39, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Papacharalampous, G.X.; Nikolopoulos, T.P.; Davilis, D.I.; Xenellis, I.E.; Korres, S.G. Universal Newborn Hearing Screening, a Revolutionary Diagnosis of Deafness: Real Benefits and Limitations. Eur. Arch. Otorhinolaryngol. 2011, 268, 1399–1406. [Google Scholar] [CrossRef]
- Thornton, A.R.; Kimm, L.; Kennedy, C.R.; Cafarelli-Dees, D. External- and Middle-Ear Factors Affecting Evoked Otoacoustic Emissions in Neonates. Br. J. Audiol. 1993, 27, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Wroblewska-Seniuk, K.; Chojnacka, K.; Pucher, B.; Szczapa, J.; Gadzinowski, J.; Grzegorowski, M. The Results of Newborn Hearing Screening by Means of Transient Evoked Otoacoustic Emissions. Int. J. Pediatr. Otorhinolaryngol. 2005, 69, 1351–1357. [Google Scholar] [CrossRef]
- Year 2019 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs. Available online: https://www2.asha.org/articlesummary.aspx?id=8589983350 (accessed on 18 April 2021).
- Vos, B.; Lagasse, R.; Levêque, A. Main Outcomes of a Newborn Hearing Screening Program in Belgium over Six Years. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 1496–1502. [Google Scholar] [CrossRef]
- Nikolopoulos, T.P. Neonatal Hearing Screening: What We Have Achieved and What Needs to Be Improved. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 635–637. [Google Scholar] [CrossRef]
- Korres, S.; Nikolopoulos, T.P.; Peraki, E.E.; Tsiakou, M.; Karakitsou, M.; Apostolopoulos, N.; Economides, J.; Balatsouras, D.; Ferekidis, E. Outcomes and Efficacy of Newborn Hearing Screening: Strengths and Weaknesses (success or Failure?). Laryngoscope 2008, 118, 1253–1256. [Google Scholar] [CrossRef]
- Rehm, H.L. A Genetic Approach to the Child with Sensorineural Hearing Loss. Semin. Perinatol. 2005, 29, 173–181. [Google Scholar] [CrossRef]
- Butcher, E.; Dezateux, C.; Cortina-Borja, M.; Knowles, R.L. Prevalence of Permanent Childhood Hearing Loss Detected at the Universal Newborn Hearing Screen: Systematic Review and Meta-Analysis. PLoS ONE 2019, 14, e0219600. [Google Scholar] [CrossRef]
- Torre, P., 3rd; Zeldow, B.; Yao, T.J.; Hoffman, H.J.; Siberry, G.K.; Purswani, M.U.; Frederick, T.; Spector, S.A.; Williams, P.L. Newborn Hearing Screenings in Human Immunodeficiency Virus-Exposed Uninfected Infants. J. AIDS Immune Res. 2016, 1, 102. [Google Scholar]
- Bielecki, I.; Horbulewicz, A.; Wolan, T. Risk Factors Associated with Hearing Loss in Infants: An Analysis of 5282 Referred Neonates. Int. J. Pediatr. Otorhinolaryngol. 2011, 75, 925–930. [Google Scholar] [CrossRef]
- Fausti, S.A.; Henry, J.A.; Helt, W.J.; Phillips, D.S.; Frey, R.H.; Noffsinger, D.; Larson, V.D.; Fowler, C.G. An Individualized, Sensitive Frequency Range for Early Detection of Ototoxicity. Ear Hear. 1999, 20, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Noise: A Hazard for the Fetus and Newborn. American Academy of Pediatrics. Committee on Environmental Health. Pediatrics 1997, 100, 724–727.
- Choi, K.Y.; Lee, B.S.; Choi, H.G.; Park, S.-K. Analysis of the Risk Factors Associated with Hearing Loss of Infants Admitted to a Neonatal Intensive Care Unit: A 13-Year Experience in a University Hospital in Korea. Int. J. Environ. Res. Public Health 2020, 17, 8082. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Refer after I Stage | Refer after II Stage | |||
| Year | Non-NICU | NICU | Non-NICU | NICU |
| 2011 | 62/682 (9.09%) | 23/172 (13.37%) | 4/682 (0.58%) | 4/172 (2.32%) |
| 2012 | 63/1171 (5.38%) | 48/301 (15.95%) | 4/1171 (0.34%) | 1/301 (0.33%) |
| 2013 | 72/1133 (6.35%) | 32/295 (10.84%) | 7/1133 (0.61%) | 5/295 (1.69%) |
| 2014 | 199/1067 (9.37%) | 35/261 (13.41%) | 1/1067 (0.09%) | 9/261 (3.44%) |
| 2015 | 38/1020 (3.73%) | 30/324 (9.26%) | 1/1020 (0.09%) | 22/324 (9.02%) |
| 2016 | 36/886 (4.06%) | 11/352 (3.12%) | 6/886 (0.67%) | 3/352 (0.85%) |
| 2017 | 34/927 (3.67%) | 15/301 (4.98%) | 8/927 (0.86%) | 7/301 (2.32%) |
| 2018 | 32/949 (3.37%) | 10/292 (3.42%) | 14/949 (1.47%) | 5/292 (1.71%) |
| 2019 | 112/1116 (10.04%) | 26/439 (5.92%) | 10/1116 (0.89%) | 10/439 (2.27%) |
| All yrs | 648/8951 (7.23%) | 230/2737 (8.40%) | 55/8951 (0.61%) | 66/2737 (2.41%) |
| Dropout II Stage | Dropout ABR | |||
| Year | Non-NICU | NICU | Non-NICU | NICU |
| 2011 | 19/62 (30.64%) | 8/23 (34.78%) | 5/13 (38.46%) | 62/172 (36.04%) |
| 2012 | 16/63 (25.39%) | 11/48 (22.91%) | 1/54 (1.85%) | 95/301 (31.56%) |
| 2013 | 13/72 (18.05%) | 4/31 (12.90%) | 7/40 (17.5%) | 101/295 (34.23%) |
| 2014 | 71/100 (71%) | 7/35 (20%) | 11/44 (25%) | 94/261 (36.01%) |
| 2015 | 22/38 (57.89%) | 3/30 (10%) | 9/43 (20.93%) | 81/324 (25%) |
| 2016 | 11/36 (30.55%) | 6/11 (54.54%) | 11/40 (27.5%) | 109/352 (30.96%) |
| 2017 | 15/34 (44.11%) | 3/15 (20%) | 16/40 (40%) | 73/301 (24.25%) |
| 2018 | 15/32 (46.87%) | 1/10 (10%) | 6/45 (13.33%) | 74/292 (25.34%) |
| 2019 | 13/112 (11.60%) | 1/26 (3.84%) | 10/49 (20.4%) | 175/439 (39.86%) |
| All yrs | 195/549 (35.51%) | 44/229 (19.21%) | 76/368 (20.65%) | 864/2737 (31.56%) |
| Clinical Features | |||
|---|---|---|---|
| Non-NICU | NICU | p-Value (Log Odds Ratio—95% IC) | |
| Sex | F 4379; (48.92%) | F 1256; (45.88%) | 0.005 * |
| (−0.122; −0.208 −0.036) | |||
| Family history of hearing loss | Yes 299, (3.34%) | Yes 14; (0.51%) | <0.001 * |
| (−1.905; −2.443 −1.368) | |||
| TORCH | Yes 12; (0.13%) | Yes 100; (3.65%) | <0.001 * |
| (3.341; 2.741 3.941) | |||
| Low birth weight | Yes 4; (0.04%) | Yes 1503; (54.91%) | <0.001 * |
| (<1500 g) | (7.910; 6.927 8.893) | ||
| Hyperbilirubinemia | Yes 6; (0.06%) | Yes 475; (17.35%) | <0.001 * |
| (5.746; 4.940 6.553) | |||
| Encephalopathy and meningitis | Yes 0; (0%) | Yes 12; (0.43%) | <0.001 * |
| (4.408; 1.581 7.235) | |||
| Ototoxic medications | Yes 3; (0.03%) | Yes 75; (2.74%) | <0.001 * |
| (4.431; 3.276 5.586) | |||
| Opioids | Yes 0; (0.00%) | Yes 13; (0.47%) | <0.001 * |
| (4.485; 1.662 7.308) | |||
| Connexin 26 | Yes 1; (0.01%) | Yes 0; (0%) | 0.58 |
| (0.086; −3.115 3.287) | |||
| Apgar 0–4/0–6 | Yes 0; (0%) | Yes 255; (9.31%) | <0.001 * |
| (7.519; 4.744 10.294) | |||
| Syndromes | Yes 14; (0.15%) | Yes 68; (2.48%) | <0.001 * |
| (2.789; 2.212 3.366) | |||
| Prematurity | Yes 2; (0.02%) | Yes 666; (24.33%) | <0.001 * |
| (7.272; 5.883 8.660) | |||
| Mechanical ventilation for at least 5 days | Yes 1; (0.01%) | Yes 661; (24.15%) | <0.001 * |
| (7.955; 5.993 9.917) | |||
| Diabetes | Yes 3; (0.03%) | Yes 74; (2.70%) | <0.001 * |
| (4.417; 3.262 5.573) | |||
| Craniofacial anomalies | Yes 15; (0.16%) | Yes 27; (0.98%) | <0.001 * |
| (1.781; 1.148 2.414) | |||
| Cytomegalovirus | Yes 7; (0.07%) | Yes 25; (0.91%) | <0.001 * |
| (2.466; 1.627 3.305) | |||
| Toxoplasma | Yes 2; (0.02%) | Yes 17; (0.62%) | <0.001 * |
| (3.331; 1.865 4.797) | |||
| Rubella | Yes 1; (0.01%) | Yes 5; (0.18%) | <0.001 * |
| (2.796; 0.694 4.944) | |||
| HIV | Yes 2; (0.02%) | Yes 3; (0.11%) | 0.053 |
| (1.591; −0.198 3.381) | |||
| HBV | Yes 0; (0.00%) | Yes 2; (0.07%) | 0.011 * |
| (2.795; −0.242 5.832) | |||
| HCV | Yes 0; (0.00%) | Yes 4; (0.14%) | <0.001 * |
| (3.383; 0.461 0.306) | |||
| HZV | Yes 0; (0.00%) | Yes 1; (0.03%) | 0.071 |
| (2.284; −0.917 5.485) | |||
| Total concomitant known audiological risk factors | 0:8615; (96.24%) | 0:0; (0%) | <0.001 *(-) |
| 1:331; (3.69%) | 1:702; (25.64%) | ||
| 2:5; (0.05%) | 2:915; (33.43%) | ||
| 3:0; (0%) | 3:636; (23.23%) | ||
| 4:0; (0%) | 4:318; (11.61%) | ||
| 5:0; (0%) | 5:144; (5.26%) | ||
| 6:0; (0%) | 6:20; (0.73%) | ||
| 7:0;(0%) | 7:2; (0.07%) | ||
| Audiological features | |||
| non-NICU | NICU | p-value (Log odds ratio—95% IC) | |
| Hearing loss | Yes 35; (0.39%) | Yes 98; (3.58%) | <0.001 * |
| (2.247; 1.859 2.635) | |||
| Profound bilateral hearing loss | Yes 2; (0.02%) | Yes 2; (0.07%) | 0.566 |
| (0.492; −1.206 2.190) | |||
| Degree of hearing loss (worst ear) | 0:15; (0.16%) | 0:64; (2.33%) | 0.055(-) |
| 1:9; (0.10%) | 1:22; (0.80%) | ||
| 2:5; (0.05%) | 2:8; (0.29%) | ||
| 3:1; (0.01%) | 3:1; (0.03%) | ||
| 4:5; (0.05%) | 4:3; (0.11%) | ||
| Unilateral/bilateral hearing loss | Bil 27/35; (77.14%) | Bil 57/98; (58.16%) | 0.046 * |
| (0.887; 0.002 1.772) | |||
| Side in unilateral cases (right–left) | R 6/8; (75%) | R 9/41; (21.95%) | 0.002 * |
| (−2.398; −4.160 −0.636) | |||
| Hearing loss cases with (RF) and without risk factors | RF 14/35; (40%) | RF 98/98; (100%) | <0.001 * |
| (5.677; 2.820 8.535) | |||
| Risk Factor | All Newborns HL | All Newborns NHL | p-Value | Non-NICU HL | Non-NICU NHL | p-Value | NICU HL | NICU NHL | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| 133 | 11,555 | (Log Odds Ratio—95% IC) | 35 | 8916 | (Log Odds Ratio—95%) | 98 | 2639 | (Log Odds Ratio—95% IC) | |
| Sex | F 53; (0.94%) | F 5582; (99.05%) | 0.052 | F 13; (0.29%) | F 4366; (99.70%) | 0.162 | F 40; (3.18%) | F 1216; (96.81%) | 0.305 |
| (−0.344; −0.693 0.005) | (−0.485; −1.172 0.202) | (−0.214; −0.624 0.196) | |||||||
| Family history of hearing loss | Yes 13; (9.77%) | Yes 300; (2.59%) | <0.001 * | Yes 13; (37.14%) | Yes 286; (3.2%) | <0.001 * | Yes 0; (0%) | Yes 14; (0.53%) | - |
| (1.402; 0.819 1.986) | (2.881; 2.185 3.577) | ||||||||
| TORCH | Yes 3; (2.25%) | Yes 109; (0.94%) | - | Yes 0; (0%) | Yes 12; (0.13%) | - | Yes 3; (3.06%) | Yes 97; (3.67%) | - |
| Low birth weight (<1500 g) | Yes 62; (46.61%) | Yes 1445; (12.50%) | <0.001 * | Yes 0; (0%) | Yes 4; (0.04%) | - | Yes 62; (63.26%) | Yes 1441; (54.60%) | 0.091 |
| (1.810; 1.465 2.155) | (0.359; −0.059 0.777) | ||||||||
| Hyperbilirubinemia | Yes 12; (9.02%) | Yes 469; (4.05%) | 0.004 * | Yes 0; (0%) | Yes 6; (0.6%) | - | Yes 12; (12.24%) | Yes 463; (17.54%) | 0.174 |
| (0.852; 0.252 1.452) | (−0.422; −1.034 0.190) | ||||||||
| Encephalopathy and meningitis | Yes 1; (0.75%) | Yes 11; (0.09%) | - | - | - | - | Yes 1; (1.02%) | Yes 11; (0.41%) | - |
| Ototoxic medications | Yes 1; (0.75%) | Yes 77; (0.66%) | - | Yes 0; (0%) | Yes 3; (0.03%) | - | Yes 1; (1.02%) | Yes 74; (2.80%) | - |
| Opioids | Yes 0; (0%) | Yes 13; (0.11%) | - | - | - | - | Yes 0; (0%) | Yes 13; (0.49%) | - |
| Connexin 26 | Yes 1; (0.75%) | Yes 0; (0%) | - | Yes 1; (2.85%) | Yes 0; (0%) | - | - | - | - |
| Apgar 0–4/0–6 | Yes 15; (11.27%) | Yes 240; (2.07%) | <0.001 * | - | - | - | Yes 15; (15.30%) | Yes 240; (9.09%) | 0.038 * |
| (1.791; 1.238 2.343) | (0.591; 0.026 1.157) | ||||||||
| Syndromes | Yes 10; (7.51%) | Yes 72; (0.62%) | <0.001 * | Yes 1; (2.85%) | Yes 13; (0.14%) | - | Yes 9; (9.18%) | Yes 59; (2.23%) | <0.001 * |
| (2.562; 1.877 3.247) | (1.487; 0.754 2.219) | ||||||||
| Prematurity | Yes 23;(17.29%) | Yes 645; (5.58%) | <0.001 * | Yes 0; (0%) | Yes 2; (0.02%) | - | Yes 23; (23.46%) | Yes 643; (24.36%) | 0.839 |
| (1.263; 0.807 1.720) | (−0.049; −0.525 0.426) | ||||||||
| NICU | Yes 98; (73.68%) | Yes 2639; (22.83%) | <0.001 * | - | - | - | - | - | - |
| (2.247; 1.859 2.666) | |||||||||
| Mechanical ventilation for at least 5 days | Yes 28; (21.05%) | Yes 634; (5.48%) | <0.001 * | Yes 0; (0%) | Yes 1; (0.01%) | - | Yes 28; (28.57%) | Yes 633; (23.98%) | 0.298 |
| (1.525; 1.100 1.949) | (0.237; −0.210 0.684) | ||||||||
| Diabetes | Yes 0; (0%) | Yes 77; (0.66%) | - | Yes 0; (0%) | Yes 3; (0.03%) | - | Yes 0; (0%) | Yes 74; (2.80%) | - |
| Craniofacial anomalies | Yes 9; (6.76%) | Yes 33; (0.28%) | <0.001 * | Yes 3; (8.57%) | Yes 12; (0.13%) | - | Yes 6; (6.12%) | Yes 21; (0.79%) | <0.001 * |
| (3.232; 2.474 3.990) | (2.096; 1.165 3.026) | ||||||||
| Cytomegalovirus | Yes 2; (1.50%) | Yes 30; (0.25%) | - | Yes 0; (0%) | Yes 7; (0.07%) | - | Yes 2; (2.04%) | Yes 23; (0.87%) | - |
| Toxoplasma | Yes 0; (0%) | Yes 19; (0.16%) | - | Yes 0; (0%) | Yes 2; (0.02%) | - | Yes 0; (0%) | Yes 17; (0.64%) | - |
| Rubella | Yes 0; (0%) | Yes 6; (0.05%) | - | Yes (0; 0%) | Yes 1; (0.01%) | - | Yes 0; (0%) | Yes 5; (0.18%) | - |
| HIV | Yes 1; (0.75%) | Yes 4; (0.03%) | - | Yes 0; (0) | Yes 2; (0.02%) | - | Yes 1; (1.02%) | Yes 2; (0.07%) | - |
| HBV | Yes 0; (0%) | Yes 2; (0.01%) | - | - | - | - | Yes 0; (0%) | Yes 2; (0.07%) | - |
| HCV | Yes 0; (0%) | Yes 4; (0.03%) | - | - | - | - | Yes 0; (0%) | Yes 4; (0.15%) | - |
| HZV | Yes 0; (0%) | Yes 1; (0.008%) | - | - | - | - | Yes 0; (0%) | Yes 1; (0.03%) | - |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Males | 0.71 (0.50–1.01) | 0.05 * | - | - |
| Prematurity | 3.54 (2.24–5.58) | <0.001 * | 1.01 (0.31–3.32) | 1.38 |
| Family history of hearing loss | 4.06 (2.27–7.29) | <0.001 * | 17.55 (5.04–61.09) | <0.001 * |
| TORCH | 2.42 (0.76–7.73) | 0.14 | - | - |
| Low birth weight (<1500 g) | 6.11 (4.33–8.63) | <0.001 * | 3.19 (1.04–9.80) | 0.04 * |
| Hyperbilirubinemia | 2.34 (1.29–4.27) | 0.05 * | 0.83 (0.25–2.79) | 1.16 |
| Encephalopathy and meningitis | 7.95 (1.02–62.02) | 0.05 * | - | - |
| Ototoxic medications | 1.13 (0.16–8.18) | 1.3 | - | - |
| Mechanical ventilation for at least 5 days | 4.59 (3.00–7.02) | <0.001 * | 1.78 (0.56–5.66) | 0.33 |
| Apgar 0–4/0–6 | 5.99 (3.45–10.41) | <0.001 * | 2.51 (0.72–8.69) | 0.15 |
| NICU | 9.46 (6.42–13.95) | <0.001 * | 11.45 (3.29–39.89) | <0.001 * |
| Syndromes | 12.97 (6.54–25.72) | <0.001 * | 3.42 (0.77–15.21) | 0.11 |
| Total concomitant known audiological risk factors | 1.78 (1.62–1.95) | <0.001 * | 0.67 (0.23–1.92) | 0.45 |
| Cytomegalovirus | 5.87 (1.39–24.80) | 0.02 * | 4.05 (0.74–21.98) | 0.11 |
| Toxoplasma | - | - | - | - |
| Rubella | - | - | - | - |
| HIV | 21.88 (2.43–197.05) | 0.06 | 13.20 (1.22–143.10) | 0.03 * |
| HBV | - | - | - | - |
| HCV | - | - | - | - |
| HZV | - | - | - | - |
| Opioids | - | - | - | - |
| Diabetes | - | - | - | - |
| Craniofacial anomalies | 25.34 (11.88–54.08) | <0.001 * | 9.62 (2.97–31.13) | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Luca, L.M.; Malesci, R.; Gallus, R.; Melis, A.; Palmas, S.; Degni, E.; Crescio, C.; Piras, M.L.; Arca Sedda, M.F.; Canu, G.M.; et al. Audiological Risk Factors, Referral Rates and Dropouts: 9 Years of Universal Newborn Hearing Screening in North Sardinia. Children 2022, 9, 1362. https://doi.org/10.3390/children9091362
De Luca LM, Malesci R, Gallus R, Melis A, Palmas S, Degni E, Crescio C, Piras ML, Arca Sedda MF, Canu GM, et al. Audiological Risk Factors, Referral Rates and Dropouts: 9 Years of Universal Newborn Hearing Screening in North Sardinia. Children. 2022; 9(9):1362. https://doi.org/10.3390/children9091362
Chicago/Turabian StyleDe Luca, Laura Maria, Rita Malesci, Roberto Gallus, Andrea Melis, Sara Palmas, Emilia Degni, Claudia Crescio, Maria Lucia Piras, Maria Francesca Arca Sedda, Giovanna Maria Canu, and et al. 2022. "Audiological Risk Factors, Referral Rates and Dropouts: 9 Years of Universal Newborn Hearing Screening in North Sardinia" Children 9, no. 9: 1362. https://doi.org/10.3390/children9091362