
Correlation between BMI and Oral Health Status (DMFT, PI, mSBI, and Salivary 1,5-AG) among the Pediatric Population in Saudi Arabia: A Clinico-Biochemical Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Quantitative Estimation of Salivary 1,5-AG Using Enzyme-Linked Immunosorbent Assay (ELISA)
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Mallineni, S.K.; Nuvvula, S.; Bhumireddy, J.C.; Ismail, A.F.; Verma, P.; Sajja, R.; Alassaf, A.; Almulhim, B.; Alghamdi, S.; Saha, A.; et al. Knowledge and Perceptions Regarding Coronavirus (COVID-19) among Pediatric Dentists during Lockdown Period. Int. J. Environ. Res. Public Health 2022, 19, 209. [Google Scholar] [CrossRef] [PubMed]
- Luzzi, V.; Ierardo, G.; Bossù, M.; Polimeni, A. Pediatric Oral Health during and after the COVID-19 Pandemic. Int. J. Paediatr. Dent. 2021, 31, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Alhabdan, Y.A.; Albeshr, A.G.; Yenugadhati, N.; Jradi, H. Prevalence of dental caries and associated factors among primary school children: A population-based cross-sectional study in Riyadh, Saudi Arabia. Environ. Health Prev. Med. 2018, 23, 60. [Google Scholar] [CrossRef] [Green Version]
- Carounanidy, U.; Sathyanarayanan, R. Dental caries—A complete changeover (Part I). J. Conserv. Dent. 2009, 12, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Al-Hussaini, A.; Bashir, M.S.; Khormi, M.; AlTuraiki, M.; Alkhamis, W.; Alrajhi, M.; Halal, T. Overweight and obesity among Saudi children and adolescents: Where do we stand today? Saudi J. Gastroenterol. Off. J. Saudi Gastroenterol. Assoc. 2019, 25, 229. [Google Scholar] [CrossRef]
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar] [CrossRef]
- Martinez-Herrera, M.; Silvestre-Rangil, J.; Silvestre, F.J. Association between obesity and periodontal disease. A systematic review of epidemiological studies and controlled clinical trials. Med. Oral. Patol. Oral. Cir. Bucal. 2017, 22, e708–e715. [Google Scholar] [CrossRef]
- Nazir, M.; Al-Ansari, A.; Al-Khalifa, K.; Alhareky, M.; Gaffar, B.; Almas, K. Global Prevalence of Periodontal Disease and Lack of Its Surveillance. Sci. World J. 2020, 2020, 2146160. [Google Scholar] [CrossRef]
- Alghamdi, A.S.; Almarghlani, A.A.; AlYafi, R.A.; Kayal, R.A.; Al-Zahrani, M.S. Gingival health and oral hygiene practices among high school children in Saudi Arabia. Ann. Saudi Med. 2020, 40, 126–135. [Google Scholar] [CrossRef]
- Chapple, I.L.; Bouchard, P.; Cagetti, M.G.; Campus, G.; Carra, M.C.; Cocco, F.; Nibali, L.; Hujoel, P.; Laine, M.L.; Lingstrom, P.; et al. Interaction of lifestyle, behaviour or systemic diseases with dental caries and periodontal diseases: Consensus report of group 2 of the joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J. Clin. Periodontol. 2017, 44, S39–S51. [Google Scholar] [CrossRef] [Green Version]
- Al-Ansari, A.; Nazir, M. Relationship between Obesity and Dental Caries in Saudi Male Adolescents. Int. J. Dent. 2020, 7, 8811974. [Google Scholar] [CrossRef]
- Li, L.-W.; Wong, H.M.; McGrath, C.P. Longitudinal association between obesity and periodontal diseases among secondary school students in Hong Kong: A prospective cohort study. BMC Oral Health 2018, 18, 189. [Google Scholar] [CrossRef]
- Modeer, T.; Blomberg, C.C.; Wondimu, B.; Julihn, A.; Marcus, C. Association between obesity, flow rate of whole saliva, and dental caries in adolescents. Obesity 2010, 18, 2367–2373. [Google Scholar] [CrossRef]
- Farronato, M.; Tadakamadla, S.K.; Ali Quadri, M.F.; Acharya, S.; Tadakamadla, J.; Love, R.M.; Jamal, M.; Mulder, R.; Maspero, C.; Farronato, D.; et al. A Call for Action to Safely Deliver Oral Health Care during and Post COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6704. [Google Scholar] [CrossRef]
- Anthonappa, R.P.; King, N.M.; Rabie, A.B. Evaluation of the long-term storage stability of saliva as a source of human DNA. Clin. Oral Investig. 2013, 17, 1719–1725. [Google Scholar] [CrossRef]
- Ying, L.; Jian, C.; Ma, X.; Ge, K.; Zhu, W.; Wang, Y.; Zhao, A.; Zhou, J.; Jia, W.; Bao, Y. Saliva 1,5-anhydroglucitol is associated with early-phase insulin secretion in Chinese patients with type 2 diabetes. BMJ Open Diabetes Res. Care 2021, 9, e002199. [Google Scholar] [CrossRef]
- Halama, A.; Kulinski, M.; Kader, S.A.; Satheesh, N.J.; Abou-Samra, A.B.; Suhre, K.; Mohammad, R.M. Measurement of 1,5-anhydroglucitol in blood and saliva: From non-targeted metabolomics to biochemical assay. J. Transl. Med. 2016, 14, 140. [Google Scholar] [CrossRef] [Green Version]
- Juraschek, S.P.; Miller, E.R., 3rd; Appel, L.J.; Christenson, R.H.; Sacks, F.M.; Selvin, E. Effects of dietary carbohydrate on 1, 5-anhydroglucitol in a population without diabetes: Results from the OmniCarb trial. Diabet. Med. 2017, 34, 1407–1413. [Google Scholar] [CrossRef] [Green Version]
- Syed, S.; Yassin, S.M.; Dawasaz, A.A.; Amanullah, M.; Alshahrani, I.; Togoo, R.A. Salivary 1,5-Anhydroglucitol and Vitamin Levels in Relation to Caries Risk in Children. BioMed Res. Int. 2019, 2019, 4503450. [Google Scholar] [CrossRef]
- Lohman, T.G.; Ring, K.; Pfeiffer, K.; Camhi, S.; Arredondo, E.; Pratt, C.; Pate, R.; Webber, L.S. Relationships among fitness, body composition, and physical activity. Med. Sci. Sports Exerc. 2008, 40, 1163–1170. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Summary Report of the Update of Systematic Reviews of the Evidence to Inform the WHO Guidelines on Physical Activity, Sedentary Behaviour and Sleep in Children under 5 Years of Age; World Health Organization: Geneva, Switzerland, 2018.
- World Health Organization. Oral Health Survey 1997: Basic Methods, 4th ed.; World Health Organization: Geneva, Swizerland, 1997.
- Greenstein, G. The role of bleeding upon probing in the diagnosis of periodontal disease. A literature review. J. Periodontol. 1984, 55, 684–688. [Google Scholar] [CrossRef] [PubMed]
- Newbrun, E. Indices to measure gingival bleeding. J. Periodontol. 1996, 67, 555–561. [Google Scholar] [CrossRef]
- American Academy of Pediatric Dentistry. Classification of Periodontal Diseases in Infants, Children, Adolescents, and Individuals with Special Health Care Needs. The Reference Manual of Pediatric Dentistry; American Academy of Pediatric Dentistry: Chicago, IL, USA, 2020; pp. 418–432. [Google Scholar]
- Wei, S.H.; Lang, K.P. Periodontal epidemiological indices for children and adolescents: I. Gingival and periodontal health assessments. Pediatr. Dent. 1981, 3, 353–360. [Google Scholar]
- Lee, J.M.; Garon, E.; Wong, D.T. Salivary diagnostics. Orthod. Craniofac. Res. 2009, 12, 206–211. [Google Scholar] [CrossRef]
- Hijji, T.M.; Saleheen, H.; AlBuhairan, F.S. Underweight, body image, and weight loss measures among adolescents in Saudi Arabia: Is it a fad or is there more going on? Int. J. Pediatr. Adolesc. Med. 2021, 8, 18–24. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef]
- Yoo, H.Y.; Kwak, B.O.; Son, J.S.; Kim, K.S.; Chung, S. Value of serum 1, 5-anhydroglucitol measurements in childhood obesity in the continuum of diabetes. Ann. Pediatr. Endocrinol. Metab. 2015, 20, 192–197. [Google Scholar] [CrossRef] [Green Version]
- Farooqi, F.A.; Khabeer, A.; Moheet, I.; Khan, S.Q.; Farooq, I.; Ar Rejaie, A.S. Prevalence of dental caries in primary and permanent teeth and its relation with tooth brushing habits among school children in Eastern Saudi Arabia. Saudi Med. J. 2015, 36, 737–742. [Google Scholar] [CrossRef]
- Al-Rafee, M.A.; AlShammery, A.R.; AlRumikan, A.S.; Pani, S.C. A Comparison of Dental Caries in Urban and Rural Children of the Riyadh Region of Saudi Arabia. Front. Public Health 2019, 7, 195. [Google Scholar] [CrossRef] [Green Version]
- Kotha, S.B.; Terkawi, S.A.; Mubaraki, S.A.; Saffan, A.D.A.; Kotha, S.L.; Mallineni, S.K. Association between Body Mass Index (BMI) and Dental Caries among 6–12-Year-Old School Children. Children 2022, 9, 608. [Google Scholar] [CrossRef] [PubMed]
- AlBlehed, A.K.; AlThumairy, A.F.; AlTurayri, W.S.; Alassaf, A.; Almulhim, B.; Alghamdi, S.; Almalki, A.; Mallineni, S.K. Assessment of Knowledge, Attitude and Practices Regarding Oral Hygiene among the Parents of Pre-School Children: A Cross-Sectional Study: A Cross-Sectional Study. Ann. Med. Health Sci. Res. 2021, 11, 82–86. [Google Scholar]
- Fagerberg, P.; Charmandari, E.; Diou, C.; Heimeier, R.; Karavidopoulou, Y.; Kassari, P.; Koukoula, E.; Lekka, I.; Maglaveras, N.; Maramis, C.; et al. Fast Eating Is Associated with Increased BMI among High-School Students. Nutrients 2021, 13, 880. [Google Scholar] [CrossRef] [PubMed]
- Farsi, D.J.; Elkhodary, H.M. The prevalence of overweight/obesity in high school adolescents in Jeddah and the association of obesity association with dental caries. Ann Saudi Med. 2017, 37, 114–121. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J.T.; Thomas, T.; Ahmed, M.; Kannan, S.K.; Abdullah, Z.; Alghamdi, S.A.; Joseph, B. Prevalence of Periodontal Disease among Obese Young Adult Population in Saudi Arabia—A Cross-Sectional Study. Medicina 2020, 56, 197. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, R.; Corrêa, M.G.; Magno, M.; Almeida, A.P.; Fagundes, N.C.; Rosing, C.; Maia, L.C.; Lima, R.R. Physical activity reduces the prevalence of periodontal disease: Systematic review and meta-analysis. Front. Physiol. 2019, 10, 234. [Google Scholar] [CrossRef]
- Khurshid, Z.; Zohaib, S.; Najeeb, S.; Zafar, M.S.; Slowey, P.D.; Almas, K. Human Saliva Collection Devices for Proteomics: An Update. Int. J. Mol. Sci. 2016, 17, 846. [Google Scholar] [CrossRef] [Green Version]
- Warsi, I.; Khurshid, Z.; Shazam, H.; Umer, M.F.; Imran, E.; Khan, M.O.; Slowey, P.D.; Goodson, J.M. Saliva Exhibits High Sensitivity and Specificity for the Detection of SARS-CoV-2. Diseases 2021, 9, 38. [Google Scholar] [CrossRef]
- Goodson, J.M. Disease reciprocity between gingivitis and obesity. J. Periodontol. 2020, 91 (Suppl. 1), S26–S34. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Mean ± S.D. |
|---|---|
| Age | 8.59 ± 2.06 |
| Height | 127.0 ± 16.20 |
| Weight | 30.75 ± 13.78 |
| Body mass index (BMI) | 18.86 ± 7.08 |
| Deciduous decayed tooth (d) | 5.67 ± 2.37 |
| Deciduous extracted tooth (e) | 1.50 ± 0.57 |
| Deciduous filled tooth (f) | 1.78 ± 0.97 |
| def score | 3.00 ± 3.35 |
| Permanent tooth decayed (D) | 2.53 ± 2.19 |
| Permanent missing tooth (M) | 0.93 ± 0.73 |
| Permanent filled tooth (F) | 1.68 ± 1.35 |
| DMF score | 2.90 ± 2.46 |
| Plaque index (PI) | 2.11 ± 1.21 |
| Modified sulcular bleeding index (mSBI) | 0.65 ± 0.65 |
| Salivary 1,5-AG level in μg/mL | 1.88 ± 1.56 |
| Characteristics of the Study Subjects | Frequency (n = 95) | Percentage (%) | |
|---|---|---|---|
| Eating speed | Very slow | 7 | 7.1 |
| Slow | 19 | 19.4 | |
| Ordinary | 49 | 50.0 | |
| Fast | 20 | 20.4 | |
| Very fast | 3 | 3.1 | |
| Family history of periodontal disease | Yes | 13 | 13.3 |
| No | 85 | 86.7 | |
| Family history of diabetes mellitus | Yes | 13 | 13.3 |
| No | 85 | 86.7 | |
| Use of brush in routine Daily oral hygiene | Yes | 94 | 95.1 |
| No | 4 | 4.9 | |
| Brushing frequency | No | 2 | 2.0 |
| Occasional | 1 | 1.0 | |
| Once | 79 | 80.6 | |
| Twice | 16 | 16.3 | |
| Frequency of dental visit | Never | 9 | 9.2 |
| Occasionally | 22 | 22.4 | |
| Once a year | 66 | 67.3 | |
| More than once a year | 1 | 1.0 | |
| Physical exercise in their daily routine | No activity | 9 | 9.2 |
| Sometimes | 87 | 88.8 | |
| Regular | 2 | 2.0 | |
| Variables | BMI | Mean | Std. Deviation | Std. Error | p-Value |
|---|---|---|---|---|---|
| Def | Underweight | 3.18 | 3.65 | 0.48 | 0.748 |
| Normal weight | 2.72 | 3.06 | 0.61 | ||
| Overweight | 1.50 | 1.97 | 0.80 | ||
| Obese | 3.55 | 2.87 | 0.95 | ||
| Total | 3.00 | 3.35 | 0.33 | ||
| DMF | Underweight | 2.84 | 2.53 | 0.33 | 0.066 |
| Normal weight | 3.64 | 2.41 | 0.48 | ||
| Overweight | 1.00 | 2.00 | 0.81 | ||
| Obese | 2.55 | 1.87 | 0.62 | ||
| Total | 2.90 | 2.46 | 0.24 | ||
| PI | Underweight | 1.74 | 1.03 | 0.13 | 0.003 * |
| Normal weight | 2.84 | 1.37 | 0.27 | ||
| Overweight | 2.33 | 1.03 | 0.42 | ||
| Obese | 2.33 | 1.11 | 0.37 | ||
| Total | 2.11 | 1.21 | 0.12 | ||
| mSBI | Underweight | 0.39 | 0.61 | 0.08 | 0.001 * |
| Normal weight | 0.96 | 0.61 | 0.12 | ||
| Overweight | 1.33 | 0.51 | 0.21 | ||
| Obese | 1.00 | 0.00 | 0.00 | ||
| Total | 0.65 | 0.65 | 0.06 | ||
| Salivary 1,5-AG levels (μg/mL) | Underweight | 1.41 | 1.23 | 0.16 | 0.001 * |
| Normal weight | 2.07 | 1.10 | 0.22 | ||
| Overweight | 1.70 | 1.40 | 0.57 | ||
| Obese | 4.52 | 2.14 | 0.71 | ||
| Total | 1.88 | 1.56 | 0.15 |
| Variables | Def | DMF | PI | mSBI | Salivary 1,5-AG | |
|---|---|---|---|---|---|---|
| BMI | Correlation coefficient | −0.089 | 0.122 | 0.222 | 0.441 | 0.402 |
| Sig. (2-tailed) | 0.383 | 0.232 | 0.028 * | 0.001 * | 0.001 * | |
| n | 98 | 98 | 98 | 98 | 98 | |
| def | Correlation coefficient | −0.468 | −0.075 | 0.107 | −0.048 | |
| Sig. (2-tailed) | 0.001 * | 0.460 | 0.295 | 0.637 | ||
| n | 98 | 98 | 98 | 98 | ||
| DMF | Correlation coefficient | 0.269 | 0.095 | −0.081 | ||
| Sig. (2-tailed) | 0.007 * | 0.350 | 0.426 | |||
| n | 98 | 98 | 98 | |||
| PI | Correlation coefficient | 0.548 | 0.159 | |||
| Sig. (2-tailed) | 0.001 * | 0.119 | ||||
| n | 98 | 98 | ||||
| mSBI | Correlation coefficient | 0.128 | ||||
| Sig. (2-tailed) | 0.209 | |||||
| n | 98 | |||||
| Socio Demographic Charters Tics | Options | BMI | Overall | p-Value | |
|---|---|---|---|---|---|
| Not Obese | Obese | ||||
| Eating speed | Very slow | 7 (7.9) | 0 (0) | 7 (7.1) | 0.001 * |
| Slow | 18 (20.2) | 1 (11.1) | 19 (19.4) | ||
| Ordinary | 47 (52.8) | 2 (22.2) | 49 (50) | ||
| Fast | 17 (19.1) | 3 (33.3) | 20 (20.4) | ||
| Very fast | 0 (0) | 3 (33.3) | 3 (3.1) | ||
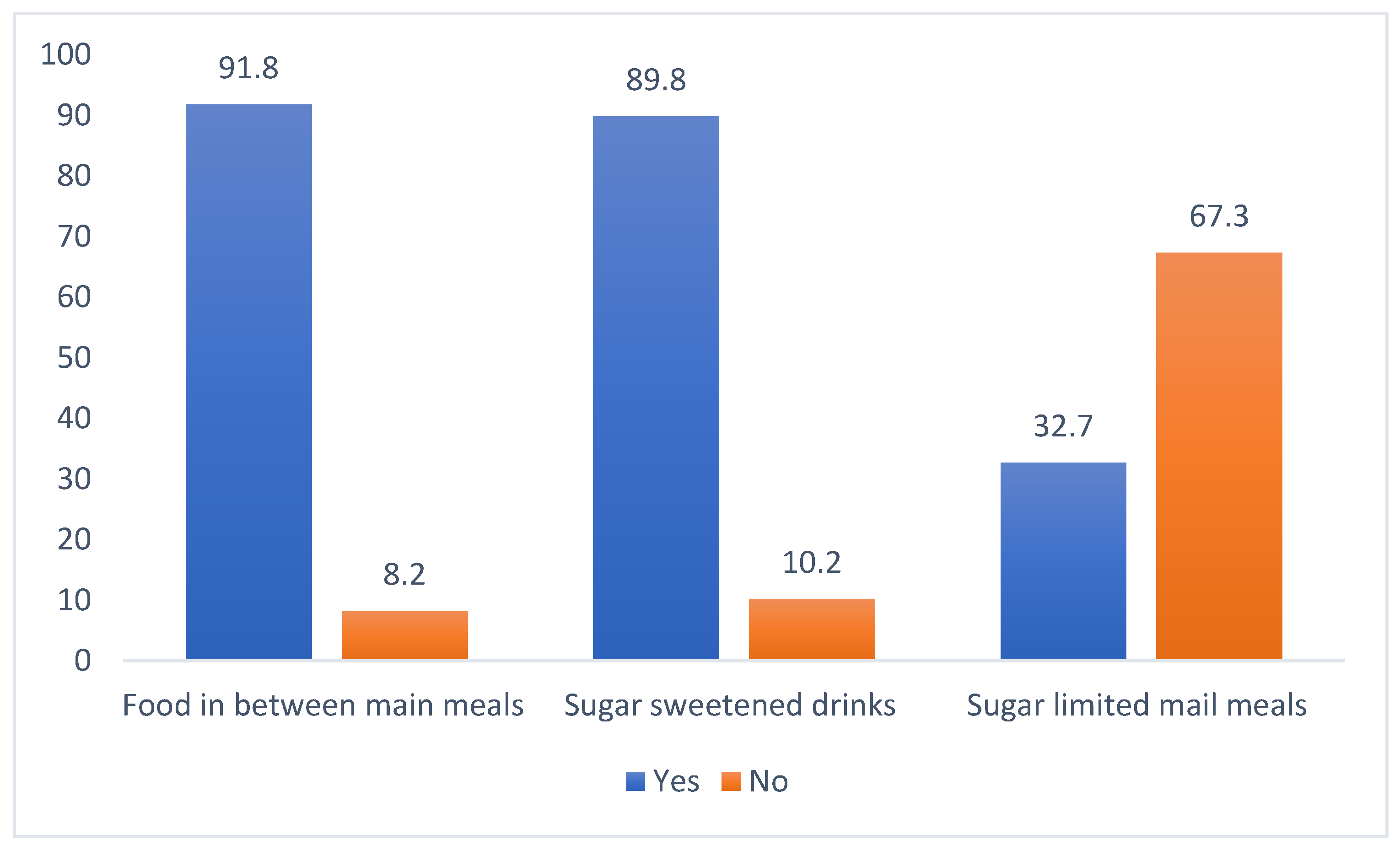
| Food intake between main meals | Yes | 81 (91) | 9 (100) | 90 (91.8) | 0.348 |
| No | 8 (9) | 0 (0) | 8 (8.2) | ||
| Intake of sweetened drinks between meals | Yes | 81 (91) | 7 (77.8) | 88 (89.8) | 0.211 |
| No | 8 (9) | 2 (22.2) | 10 (10.2) | ||
| Sugar intake limited to main meals | Yes | 32 (36) | 0 (0) | 32 (32.7) | 0.028 * |
| No | 57 (64) | 9 (100) | 66 (67.3) | ||
| Family history of periodontal disease | Yes | 12 (13.5) | 1 (11.1) | 13 (13.3) | 0.842 |
| No | 77 (86.5) | 8 (88.9) | 85 (86.7) | ||
| Family history of diabetes mellitus | Yes | 12 (13.5) | 1 (11.1) | 13 (13.3) | 0.84 |
| No | 77 (86.5) | 8 (88.9) | 85 (86.7) | ||
| Brush usage | No | 4 (4.5) | 0 (0) | 4 94.1) | 0.516 |
| Yes | 85 (95.5) | 9 (100) | 94 (95.9) | ||
| Brushing frequency | No | 2 (2.2) | 0 (0) | 2 (2) | 0.497 |
| Sometimes | 1 (1.1) | 0 (0) | 1(1) | ||
| Once | 70 (78.7) | 9 (100) | 79 (80.6) | ||
| Twice | 16 (18) | 0 (0) | 16 (16.3) | ||
| Previous dental visit | Rarely | 8 (9) | 1 (11.1) | 9 (9.2) | 0.384 |
| Less often | 18 (20.2) | 4 (44.4) | 22 (22.4) | ||
| Once a year | 62 (69.7) | 4 (44.4) | 66 (67.3) | ||
| More than once | 1 (1.1) | 0 (0) | 1 (1) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alghamdi, S.A.; Aljohar, A.; Almulhim, B.; Alassaf, A.; Bhardwaj, S.S.; Thomas, J.T.; Almalki, A.; Aljuaid, A.O.; Mallineni, S.K. Correlation between BMI and Oral Health Status (DMFT, PI, mSBI, and Salivary 1,5-AG) among the Pediatric Population in Saudi Arabia: A Clinico-Biochemical Study. Children 2022, 9, 1017. https://doi.org/10.3390/children9071017
Alghamdi SA, Aljohar A, Almulhim B, Alassaf A, Bhardwaj SS, Thomas JT, Almalki A, Aljuaid AO, Mallineni SK. Correlation between BMI and Oral Health Status (DMFT, PI, mSBI, and Salivary 1,5-AG) among the Pediatric Population in Saudi Arabia: A Clinico-Biochemical Study. Children. 2022; 9(7):1017. https://doi.org/10.3390/children9071017
Chicago/Turabian StyleAlghamdi, Sara Ayid, Aziza Aljohar, Basim Almulhim, Abdullah Alassaf, Smita Singh Bhardwaj, Julie Toby Thomas, Abdullah Almalki, Areej Owaid Aljuaid, and Sreekanth Kumar Mallineni. 2022. "Correlation between BMI and Oral Health Status (DMFT, PI, mSBI, and Salivary 1,5-AG) among the Pediatric Population in Saudi Arabia: A Clinico-Biochemical Study" Children 9, no. 7: 1017. https://doi.org/10.3390/children9071017