
Advanced Echocardiographic Analysis in Medium-Term Follow-Up of Children with Previous Multisystem Inflammatory Syndrome

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic and Biochemical Data of the Population
3.2. Advanced Echocardiographic Evaluation in the Overall Population
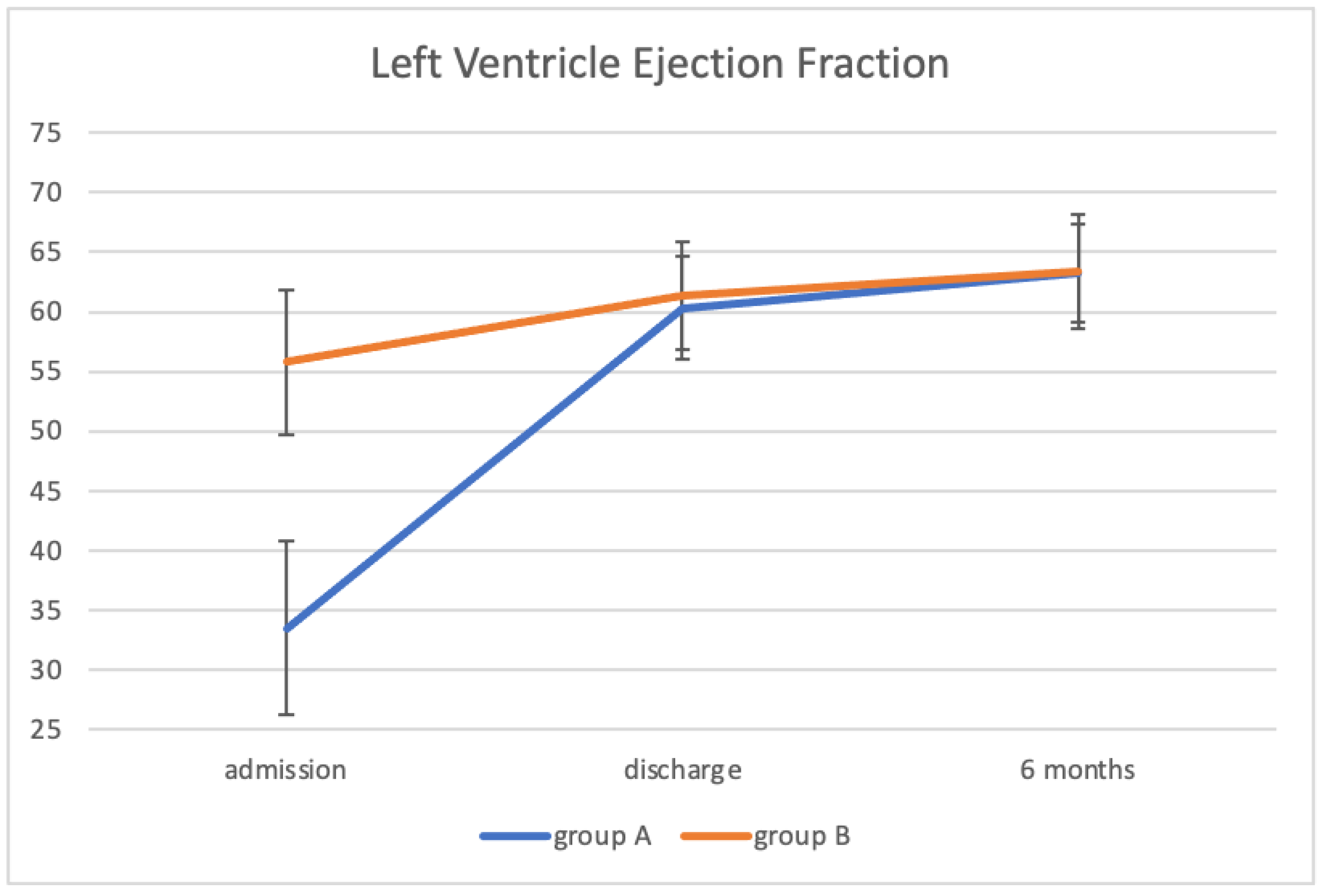
3.3. Advanced Echocardiographic Evaluation: Group A vs. Group B
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feldstein, L.R.; Rose, E.B.; Horwitz, S.M.; Collins, J.P.; Newhams, M.M.; Son, M.B.F.; Newburger, J.W.; Kleinman, L.C.; Heidemann, S.M.; Martin, A.A.; et al. Multisystem inflammatory syndrome in U.S. children and adolescents. N. Engl. J. Med. 2020, 383, 334–346. [Google Scholar] [CrossRef] [PubMed]
- Abrams, J.Y.; Godfred-Cato, S.E.; Oster, M.E.; Chow, E.J.; Koumans, E.H.; Bryant, B.; Leung, J.W.; Belay, E.D. Multisystem inflammatory syndrome in children associated with severe acute respiratory syndrome coronavirus 2: A systematic review. J. Pediatr. 2020, 226, 45–54.e1. [Google Scholar] [CrossRef] [PubMed]
- Graciano-Machuca, O.; Villegas-Rivera, G.; López-Pérez, I.; Macías-Barragán, J.; Sifuentes-Franco, S. Multisystem inflammatory syndrome in children (MIS-C) following SARS-CoV-2 infection: Role of oxidative stress. Front. Immunol. 2021, 12, 4167. [Google Scholar] [CrossRef]
- Schulert, G.S.; Blum, S.A.; Cron, R.Q. Host genetics of pediatric SARS-CoV-2 COVID-19 and multisystem inflammatory syndrome in children. Curr. Opin. Pediatr. 2021, 33, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Henderson, L.A.; Canna, S.W.; Friedman, K.G.; Gorelik, M.; Lapidus, S.K.; Bassiri, H.; Behrens, E.M.; Ferris, A.; Kernan, K.F.; Schulert, G.S.; et al. American college of rheumatology clinical guidance for pediatric patients with multisystem inflammatory syndrome in children (MIS-C) associated with SARS-CoV-2 and hyperinflammation in COVID-19. Version 1. Arthritis Rheumatol. 2020, 72, 1791–1805. [Google Scholar] [CrossRef] [PubMed]
- Living Guidance for Clinical Management of COVID-19: Living Guidance, 23 November 2021—World Health Organization (WHO). 2021. Available online: https://apps.who.int/iris/bitstream/handle/10665/349321/WHO-2019-nCoV-clinical-2021.2-eng.pdf (accessed on 6 April 2022).
- Belhadjer, Z.; Méot, M.; Bajolle, F.; Khraiche, D.; Legendre, A.; Abakka, S.; Auriau, J.; Grimaud, M.; Oualha, M.; Beghetti, M.; et al. Acute heart failure in multisystem inflammatory syndrome in children in the context of global SARS-CoV-2 pandemic. Circulation 2020, 142, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Nakra, N.A.; Blumberg, D.A.; Herrera-Guerra, A.; Lakshminrusimha, S. Multi-system inflammatory syndrome in children (Mis-c) following sars-cov-2 infection: Review of clinical presentation, hypothetical pathogenesis, and proposed management. Children 2020, 7, 69. [Google Scholar] [CrossRef]
- Sirico, D.; Basso, A.; Reffo, E.; Cavaliere, A.; Castaldi, B.; Sabatino, J.; Meneghel, A.; Martini, G.; Da Dalt, L.; Zulian, F.; et al. Early echocardiographic and cardiac MRI findings in multisystem inflammatory syndrome in children. J. Clin. Med. 2021, 10, 3360. [Google Scholar] [CrossRef]
- Bermejo, I.A.; Bautista-Rodriguez, C.; Fraisse, A.; Voges, I.; Gatehouse, P.; Kang, H.; Piccinelli, E.; Rowlinson, G.; Lane, M.; Sample, T.; et al. Short-term sequelae of multisystem inflammatory syndrome in children asseszsed by CMR. JACC Cardiovasc. Imaging 2021, 14, 1666–1667. [Google Scholar] [CrossRef]
- Matsubara, D.; Kauffman, H.L.; Wang, Y.; Calderon-Anyosa, R.; Nadaraj, S.; Elias, M.D.; White, T.J.; Torowicz, D.L.; Yubbu, P.; Giglia, T.M.; et al. Echocardiographic findings in pediatric multisystem inflammatory syndrome associated with COVID-19 in the United States. J. Am. Coll. Cardiol. 2020, 76, 1947–1961. [Google Scholar] [CrossRef]
- Mannarino, S.; Raso, I.; Garbin, M.; Ghidoni, E.; Corti, C.; Goletto, S.; Nespoli, L.; Santacesaria, S.; Zoia, E.; Camporesi, A.; et al. Cardiac dysfunction in multisystem inflammatory syndrome in children. An Italian single-center study. Ital. J. Pediatr. 2022, 48, 25. [Google Scholar] [CrossRef] [PubMed]
- Verdoni, L.; Mazza, A.; Gervasoni, A.; Martelli, L.; Ruggeri, M.; Ciuffreda, M.; Bonanomi, E.; D’Antiga, L. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: An observational cohort study. Lancet 2020, 395, 1771–1778. [Google Scholar] [CrossRef]
- Valverde, I.; Singh, Y.; Sanchez-de-Toledo, J.; Theocharis, P.; Chikermane, A.; Di Filippo, S.; Kuciñska, B.; Mannarino, S.; Tamariz-Martel, A.; Gutierrez-Larraya, F.; et al. Acute cardiovascular manifestations in 286 children with multisystem inflammatory syndrome associated with COVID-19 infection in Europe. Circulation 2021, 143, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Haghighi Aski, B.; Manafi Anari, A.; Abolhasan Choobdar, F.; Zareh Mahmoudabadi, R.; Sakhaei, M. Cardiac abnormalities due to multisystem inflammatory syndrome temporally associated with Covid-19 among children: A systematic review and meta-analysis. Int. J. Cardiol. Heart Vasc. 2021, 33, 100764. [Google Scholar] [CrossRef] [PubMed]
- Khoo, N.S.; Smallhorn, J.F.; Atallah, J.; Kaneko, S.; Mackiing, A.S.; Paterson, I. Altered left ventricular tissue velocities, deformation and twist in children and young adults with acute myocarditis and normal ejection fraction. J. Am. Soc. Echocardiogr 2012, 25, 294–303. [Google Scholar] [CrossRef]
- Kobayashi, R.; Dionne, A.; Ferraro, A.; Harrild, D.; Newburger, J.; VanderPluym, C.; Gauvreau, K.; Son, M.B.; Lee, P.; Baker, A.; et al. Detailed assessment of left ventricular function in multisystem inflammatory syndrome in children, using strain analysis. CJC Open 2021, 3, 880–887. [Google Scholar] [CrossRef]
- Thacker, D. Multisystem inflammatory syndrome in children (MIS-C): An emerging immune mediated syndrome in children associated with COVID-19. Del. J. Public Health 2020, 6, 36–39. [Google Scholar] [CrossRef]
- Cattalini, M.; Taddio, A.; Bracaglia, C.; Cimaz, R.; Paolera, S.D.; Filocamo, G.; La Torre, F.; Lattanzi, B.; Marchesi, A.; Simonini, G.; et al. Childhood multisystem inflammatory syndrome associated with COVID-19 (MIS-C): A diagnostic and treatment guidance from the rheumatology study group of the Italian society of pediatrics. Ital. J. Pediatr. 2021, 47, 1–6. [Google Scholar] [CrossRef]
- Jonat, B.; Gorelik, M.; Boneparth, A.; Geneslaw, A.S.; Zachariah, P.; Shah, A.; Broglie, L.; Duran, J.; Morel, K.D.; Zorrilla, M.; et al. Multisystem inflammatory syndrome in children associated with coronavirus disease 2019 in a children’s hospital in New York City: Patient characteristics and an institutional protocol for evaluation, management, and follow-up. Pediatr. Crit. Care Med. 2021, 22, e178–e179. [Google Scholar] [CrossRef]
- Lopez, L.; Colan, S.D.; Frommelt, P.C.; Ensing, G.J.; Kendall, K.; Younoszai, A.K.; Lai, W.W.; Geval, T. Recommendations for quantification methods during the performance of a pediatric echocardiogram: A report from the pediatric measurements writing group of the American society of echocardiography pediatric and congenital heart disease council. J. Am. Soc. Echocardiogr. 2010, 23, 465–495. [Google Scholar] [CrossRef]
- Kampmann, C.; Wiethoff, C.M.; Wenzel, A.; Stolz, G.; Betancor, M.; Wippermann, C.F.; Huth, R.-G.; Habermehl, P.; Knuf, M.; Emschermann, T.; et al. Normal values of M mode echocardiographic measurements of more than 2000 healthy infants and children in central Europe. Heart 2000, 8, 667–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, B.J.; Mackie, A.S.; Mitsnefes, M.; Ali, H.; Mamber, S.; Colan, S.D. A novel method of expressing left ventricular mass relative to body size in children. Circulation 2008, 117, 2769–2775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuse, S.; Kobayashi, T.; Arakaki, Y.; Ogawa, S.; Katoh, H.; Sakamoto, N.; Hamaoka, K.; Saji, T. Standard method for ultrasound imaging of coronary artery in children. Pediatr. Int. 2010, 52, 876–882. [Google Scholar] [CrossRef] [PubMed]
- Levy, P.T.; Machefsky, A.; Sanchez, A.A.; Patel, M.D.; Rogal, S.; Fowler, S.; Yaeger, L.; Hardi, A.; Holland, M.R.; Hamvas, A.; et al. Reference ranges of left ventricular strain measures by two-dimensional speckle-tracking echocardiography in children: A systematic review and meta-analysis. J. Am. Soc. Echocardiogr. 2016, 29, 209–225.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugimoto, T.; Robinet, S.; Dulgheru, R.; Bernard, A.; Ilardi, F.; Contu, L.; Addetia, K.; Caballero, L.; Kacharava, G.; Athanassopoulos, G.D.; et al. Norre study. echocardiographic reference ranges for normal left atrial function parameters: Results from the EACVI NORRE study. Eur. Heart J.–Cardiovasc. Imaging 2018, 19, 630–638. [Google Scholar] [CrossRef] [Green Version]
- Hope, K.D.; Wang, Y.; Banerjee, M.M.; Montero, A.E.; Pandian, N.G.; Banerjee, A. Left atrial mechanics in children: Insights from new applications of strain imaging. Int. J. Cardiovasc. Imaging 2019, 35, 57–65. [Google Scholar] [CrossRef]
- Sabatino, J.; Di Salvo, G.; Prota, C.; Bucciarelli, V.; Josen, M.; Paredes, J.; Borrelli, N.; Sirico, D.; Prasad, S.; Indolfi, C.; et al. Left atrial strain to identify diastolic dysfunction in children with cardiomyopathies. J. Clin. Med. 2019, 8, 1243. [Google Scholar] [CrossRef] [Green Version]
- Krishna, M.R.; Sennaiyan, U.N. Peak left atrial longitudinal strain: A potential diagnostic entity in children with multi-inflammatory syndrome in children. Ann. Pediatr. Cardiol. 2021, 14, 393–396. [Google Scholar] [CrossRef]
- Levy, P.T.; Aura, A.; Sanchez, A.A.; Machefsky, A.; Fowler, S.; Holland, M.R.; Singh, G.K. Normal ranges of right ventricular systolic and diastolic strain measures in children: A systematic review and meta- analysis. J. Am. Soc. Echocardiogr. 2014, 27, 549–560. [Google Scholar] [CrossRef] [Green Version]
- Awasthi, P.; Kumar, V.; Naganur, S.; Nallasamy, K.; Angurana, S.K.; Bansal, A.; Jayashree, M. Multisystem inflammatory syndrome in children: Follow-up of a cohort from North India. Am. J. Trop. Med. Hyg. 2022, 106, 1108–1112. [Google Scholar] [CrossRef]
- Yamuna Sanil, Y.; Misra, A.; Safa, R.; Blake, J.M.; Eddine, A.C.; Balakrishnan, P.; Garcia, R.U.; Taylor, R.; Dentel, J.N.; Ang, J.; et al. Echocardiographic indicators associated with adverse clinical course and cardiac sequelae in multisystem inflammatory syndrome in children with coronavirus disease 2019. J. Am. Soc. Echocardiogr. 2021, 34, 862–876. [Google Scholar] [CrossRef] [PubMed]
- Smiseth, O.A.; Morris, D.A.; Cardim, N.; Cikes, M.; Delgado, V.; Donal, E.; Flachskampf, A.F.; Galderisi, M.; Gerber, B.L.; Gimelli, A.; et al. Reviewers: This document was reviewed by members of the 2018–2020 EACVI scientific documents committee. Multimodality imaging in patients with heart failure and preserved ejection fraction: An expert consensus document of the European association of cardiovascular imaging. Eur. Heart J. Cardiovasc. Imaging 2022, 23, e34–e61. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.A.; Belyavskiy, E.; Aravind-Kumar, R.; Kropf, M.; Frydas, A.; Braunauer, K.; Marquez, E.; Krisper, M.; Lindhorst, R.; Osmanoglou, E.; et al. Potential usefulness and clinical relevance of adding left atrial strain to left atrial volume index in the detection of left ventricular diastolic dysfunction. JACC Cardiovasc. Imaging 2018, 11, 1405–1415. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Khan, F.H.; Remme, E.W.; Ohte, N.; García-Izquierdo, E.; Chetrit, M.; Moñivas-Palomero, V.; Mingo-Santos, S.; Andersen, S.; Gude, E.; et al. Determinants of left atrial reservoir and pump strain and use of atrial strain for evaluation of left ventricular filling pressure. Eur. Heart J. Cardiovasc. Imaging 2021, 23, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Riollano-Cruz, M.; Akkoyun, E.; Briceno-Brito, E.; Kowalsky, S.; Reed, J.; Posada, R.; Sordillo, E.M.; Tosi, M.; Trachtman, R.; Paniz-Mondolfi, A. Multisystem inflammatory syndrome in children related to COVID-19: A New York City experience. J. Med. Virol. 2021, 93, 424–433. [Google Scholar] [CrossRef] [PubMed]
- Capone, C.A.; Subramony, A.; Sweberg, T.; Schneider, J.; Shah, S.; Rubin, L.; Schleien, C.; Epstein, S.; Johnson, J.C.; Kessel, A.; et al. Characteristics, cardiac involvement, and outcomes of multisystem inflammatory syndrome of childhood associated with severe acute respiratory syndrome coronavirus 2 Infection. J. Pediatr. 2020, 224, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, A.; Gupta, S.; Sood, M.; Sharma, S.; Verma, S. A Systematic review of multisystem inflammatory syndrome in children associated with SARS-CoV-2 infection. Pediatr. Infect. Dis. J. 2020, 39, e340–e346. [Google Scholar] [CrossRef]
- Ganguly, M.; Nandi, A.; Banerjee, P.; Gupta, P.; Sarkar, S.D.; Basu, S.; Pal, P. A comparative study of IL-6, CRP and NT-proBNP levels in post-COVID multisystem inflammatory syndrome in children (MISC) and Kawasaki disease patients. Int. J. Rheum Dis 2021, 25, 27–31. [Google Scholar] [CrossRef]
- Patel, T.; Kelleman, M.; West, Z.; Peter, A.; Dove, M.; Butto, A.; Oster, M.E. Comparison of MIS-C related myocarditis, classic viral myocarditis, and COVID-19 vaccine related myocarditis in children. Available online: https://www.medrxiv.org/content/10.1101/2021.10.05.21264581v1 (accessed on 16 June 2022).
- Blondiaux, E.; Parisot, P.; Redheuil, A.; Tzaroukian, L.; Levy, Y.; Sileo, C.; Schnuriger, A.; Lorrot, M.; Guedj, R.; Le Pointe, H.D. Cardiac MRI in children with multisystem inflammatory syndrome associated with COVID-19. Radiology 2020, 297, E283–E288. [Google Scholar] [CrossRef]
- Theocharis, P.; Wong, J.; Pushparajah, K.; Mathur, S.K.; Simpson, J.M.; Pascall, E.; Cleary, A.; Stewart, K.; Adhvaryu, K.; Savis, A.; et al. Multimodality cardiac evaluation in children and young adults with multisystem inflammation associated with COVID-19. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 896–903. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Baseline Characteristics | Total |
|---|---|
| Patient numbers (n) | 32 |
| Age (years), median (IQR) | 10 (7–13) |
| Gender | |
| Male, n (%) | 24 (75) |
| Female, n (%) | 8 (25) |
| Overweight, n (%) | 4 (12.4%) |
| RT-PCR positive, n (%) | 2 (6.3) |
| Serology-positive, n (%) | 32 (100) |
| Fever, n (%) | 32 (100) |
| Fever duration (days) | 6 |
| Gastrointestinal, n (%) | 30 (94) |
| Shock, n (%) | 8 (25) |
| Neurological, n (%) | 5 (16) |
| Hospital stay (days) | 13 |
| Pediatric Intensive Care Unit admission, n (%) | 22 (69) |
| Pediatric Intensive Care Unit stay (days) | 2 |
| Noninvasive ventilation, n (%) | 12 (37.5) |
| Ventilation (days) | 2.5 |
| Inotropic support, n (%) | 11 (34.4) |
| Echocardiographic Variables | Discharge (n = 32) | At 6 Months (n = 32) | p-Value |
|---|---|---|---|
| RV systolic function | |||
| TAPSE (mm) | 20.1 (±2.1) | 20.7 (±1.9) | ns |
| s wave (m/s) | 0.13 (±0.02) | 0.14 (±0.02) | 0.049 |
| RVFWLS (%) | −27.8 (±3.9) | −28.1 (±3.9) | ns |
| LV systolic function | |||
| EF (%) | 61.0 (±4.4) | 63.3 (±4.5) | 0.002 |
| LV GLS (%) | −22.1 (±1.8) | −22.1 (±1.9) | ns |
| LV diastolic function | |||
| E/A | 1.5 (±0.3) | 1.7 (±0.4) | 0.015 |
| E/e’ | 5.7 (±1.3) | 5.8 (±0.9) | ns |
| LAS (%) | 46.5 (±7.9) | 45.0 (±6.8) | ns |
| LV measurements | |||
| EDD (mm) | 41.2 (±6.0) | 40.1 (±6.0) | ns |
| EDD Z-score median (IQR) | 0.41 (−0.04–1.13) | 0.39 (−0.01–0.86) | ns |
| IVSd (mm) | 6.7 (±1.1) | 6.7 (±1.1) | ns |
| IVSd Z-score median (IQR) | 0.56 (−0.04–1.13) | 0.19 (0.06–0.43) | ns |
| PWd (mm) | 6.7 (±1.3) | 6.6 (±1.1) | ns |
| PWd Z-score median (IQR) | 0.27 (0.04–0.59) | 0.27 (0.04–0.47) | ns |
| EDV (mL) | 65.3 (±26.7) | 63.2 (±23.9) | ns |
| EDVi (mL/m2) | 54.1 (±9.4) | 50.8 (±6.9) | 0.017 |
| LV mass (g) | 83.0 (±34.4) | 77.7 (±33.6) | 0.0024 |
| LV mass indexed for BSA (g/m2) | 68.4 (±13.8) | 63.5 (±11.3) | 0.0012 |
| LV mass indexed for heigh (g/m) | 34.2 (±4.4) | 30.9 (±3.1) | <0.001 |
| Coronary arteries dilation (Z-score > 2) (n) | 0 | 0 | - |
| Echocardiographic Variables | Group A, LVEF < 45% (n = 10) | Group B, LVEF ≥ 45% (n = 22) | p-Value | |||
|---|---|---|---|---|---|---|
| Discharge | At 6 Months | Discharge | At 6 Months | Discharge | At 6 Months | |
| RV systolic function | ||||||
| TAPSE (mm) | 19.7 (±2.8) | 20.7 (±2.1) | 20.3 (±1.7) | 20.6 (±1.9) | ns | ns |
| s wave (m/s) | 0.14 (±0.03) | 0.14 (±0.03) | 0.13 (±0.02) | 0.14 (±0.02) | ns | ns |
| RVFWLS (%) | −25.8 (±4.4) | −26.7 (±3.4) | −28.7 (±3.3) | −28.7 (±3.9) | ns (0.05) | ns |
| LV systolic function | ||||||
| EF (%) | 60.3 (±4.3) | 63.3 (±4.1) | 61.3 (±4.5) | 63.4 (±4.8) | ns | ns |
| LV GLS (%) | −21.1 (±1.6) | −22.3 (±2.0) | −22.6 (±1.7) | −22.1 (±1.9) | 0.02 | ns |
| LV diastolic function | ||||||
| E/A | 1.37 (±0.28) | 1.70 (±0.44) | 1.58 (±0.28) | 1.70 (±0.34) | ns | ns |
| E/e’ | 5.7 (±1.1) | 5.7 (±0.8) | 5.7 (±1.4) | 5.7 (±0.9) | ns | ns |
| LAS (%) | 45.4 (±10.8) | 44.5 (±7.9) | 47.0 (±6.5) | 45.3 (±6.4) | ns | ns |
| LV measurements | ||||||
| EDD (mm) | 41.9 (±7.6) | 41.8 (±8.2) | 40.9 (±5.2) | 40.4 (±4.9) | ns | ns |
| EDD Z-score median (IQR) | 0.3 (−0.93–1.57) | 0.37 (−0.47–1.39) | 0.54 (0.03–1.03) | 0.39 (0.15–0.74) | ns | ns |
| IVSd (mm) | 7.2 (±1.5) | 7.2 (±1.4) | 6.5 (±0.9) | 6.5 (±0.8) | ns | ns |
| IVSd Z-score median (IQR) | 0.73 (0.44–1.18) | 0.84 (0.67 –1.22) | 0.48 (0.27–0.89) | 0.50 (0.22–0.75) | ns | ns |
| PWd (mm) | 7.3 (±1.8) | 7.1 (±1.5) | 6.5 (±0.8) | 6.4 (±0.8) | ns | ns |
| PWd Z-score median (IQR) | 0.32 (0.13–0.71) | 0.31 (0.13–0.79) | 0.20 (−0.07–0.55) | 0.23 (−0.07–0.38) | ns | ns |
| EDV (mL) | 70.3 (±35.7) | 71.2 (±33.4) | 63.0 (±22.1) | 59.6 (±17.8) | ns | ns |
| EDVi (mL/m2) | 51.8 (±12.6) | 52.9 (±9.0) | 55.1 (±7.7) | 49.8 (±5.7) | ns | ns |
| LV mass (g) | 95.5 (±45.5) | 92.9 (±44.1) | 77.3 (±27.3) | 70.8 (±25.9) | ns | ns |
| LV mass indexed for BSA (g/m2) | 71.0 (±15.3) | 68.5 (±14.6) | 67.2 (±13.8) | 61.2 (±8.9) | ns | ns |
| LV mass indexed for heigh (g/m) | 34.4 (±3.6) | 32.1 (±3.0) | 34.1 (±4.7) | 30.3 (±3.0) | ns | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garbin, M.; Raso, I.; Piersanti, A.; Gianolio, L.; De Silvestri, A.; Calcaterra, V.; Corti, C.G.; Nespoli, L.F.; Santacesaria, S.; Fini, G.; et al. Advanced Echocardiographic Analysis in Medium-Term Follow-Up of Children with Previous Multisystem Inflammatory Syndrome. Children 2022, 9, 917. https://doi.org/10.3390/children9060917
Garbin M, Raso I, Piersanti A, Gianolio L, De Silvestri A, Calcaterra V, Corti CG, Nespoli LF, Santacesaria S, Fini G, et al. Advanced Echocardiographic Analysis in Medium-Term Follow-Up of Children with Previous Multisystem Inflammatory Syndrome. Children. 2022; 9(6):917. https://doi.org/10.3390/children9060917
Chicago/Turabian StyleGarbin, Massimo, Irene Raso, Alessandra Piersanti, Laura Gianolio, Annalisa De Silvestri, Valeria Calcaterra, Carla G. Corti, Luisa F. Nespoli, Sara Santacesaria, Giulia Fini, and et al. 2022. "Advanced Echocardiographic Analysis in Medium-Term Follow-Up of Children with Previous Multisystem Inflammatory Syndrome" Children 9, no. 6: 917. https://doi.org/10.3390/children9060917