
Plasma Brain Natriuretic Peptide Levels in Children with Chronic Kidney Disease and Renal Transplant Recipients: A Single Center Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. CKD Definition and Staging Classification
2.4. Patient Evaluation
2.4.1. Anthropometric Measurements
2.4.2. Cardiac Evaluation
2.4.3. Laboratory Data
2.4.4. BNP Measurement
2.5. Statistical Analysis
3. Results
3.1. Population Description
3.2. BNP Levels in Patient Subgroups vs. Controls
3.3. Correlations between BNP Levels and Patient Subgroups
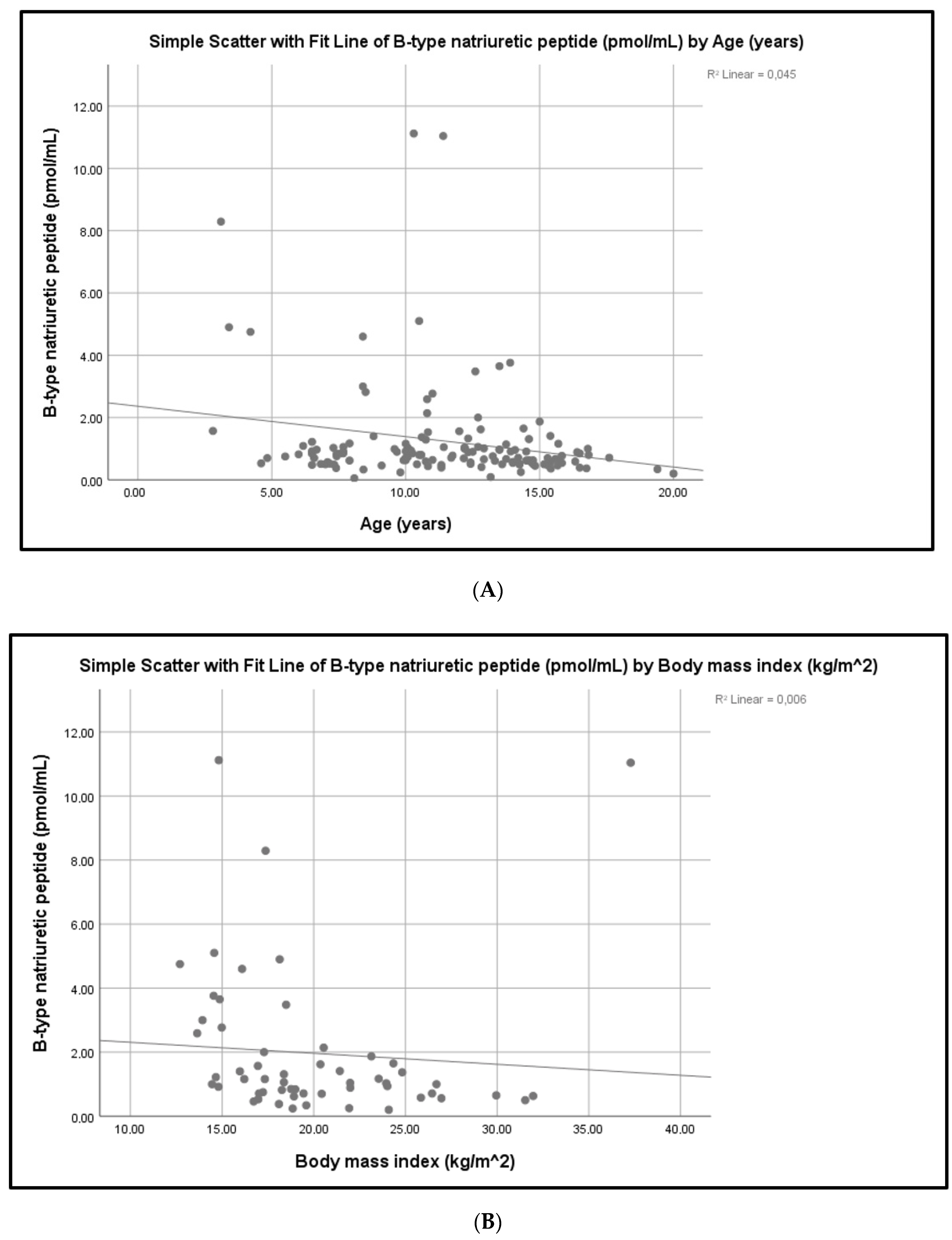
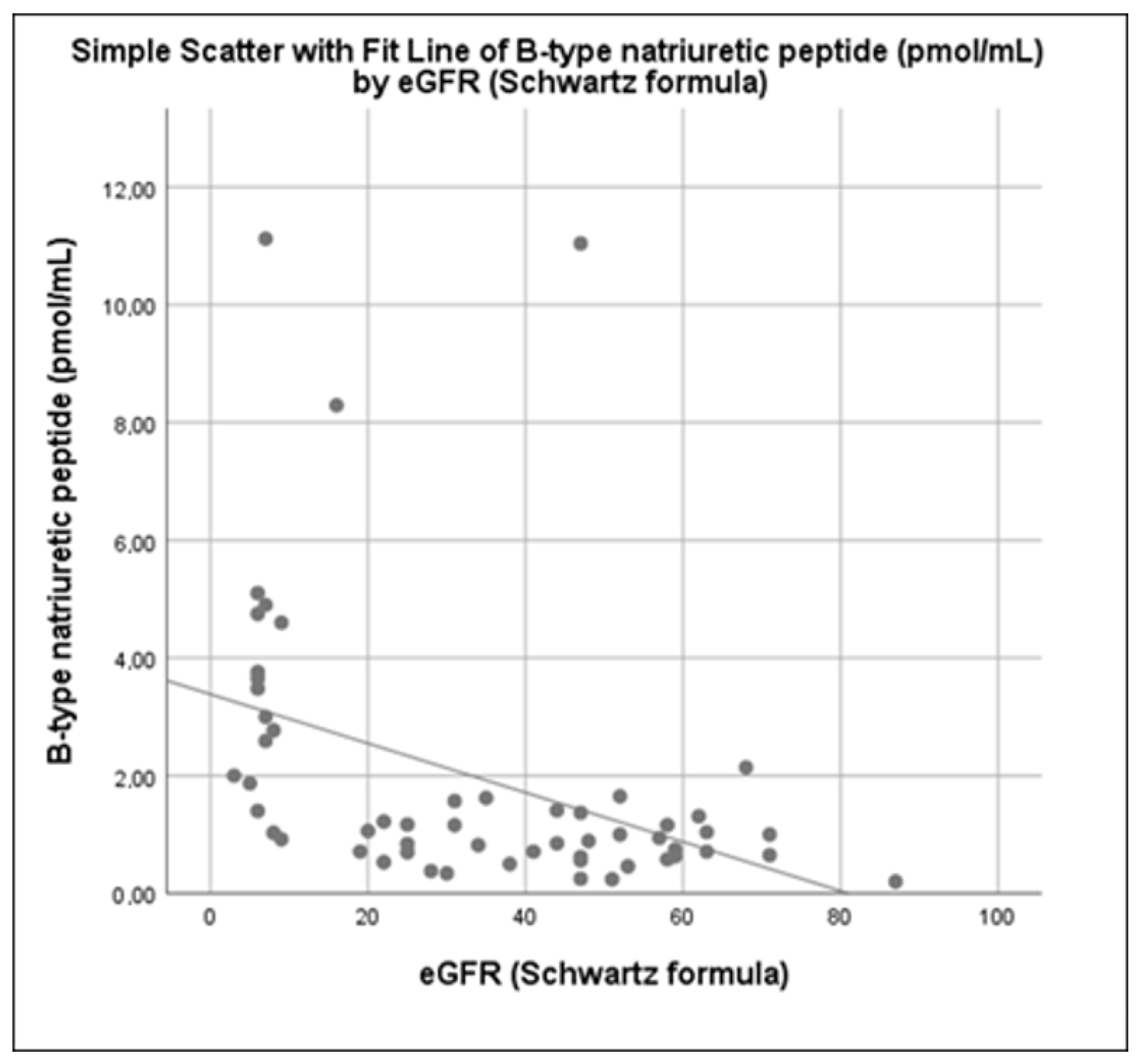
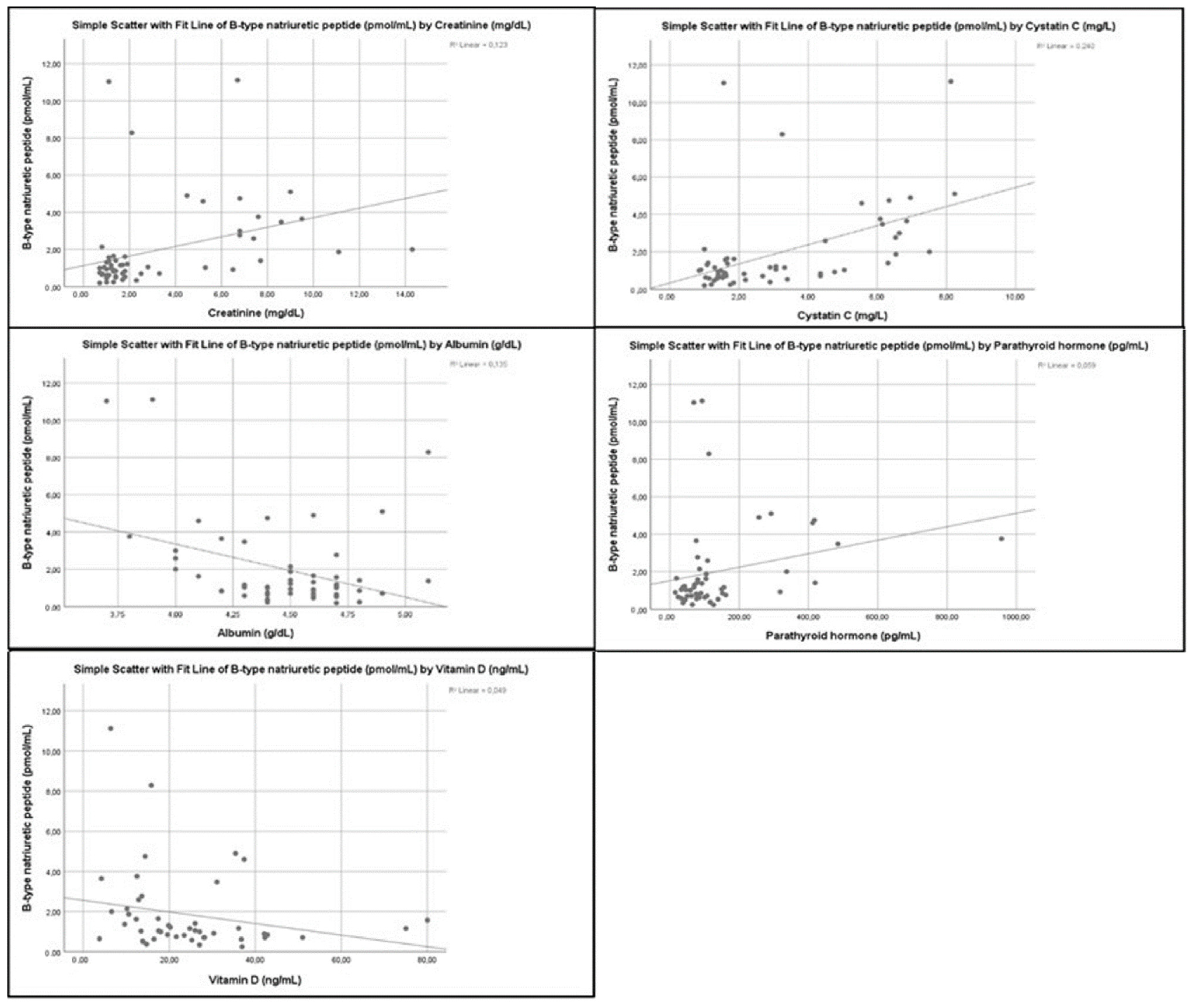
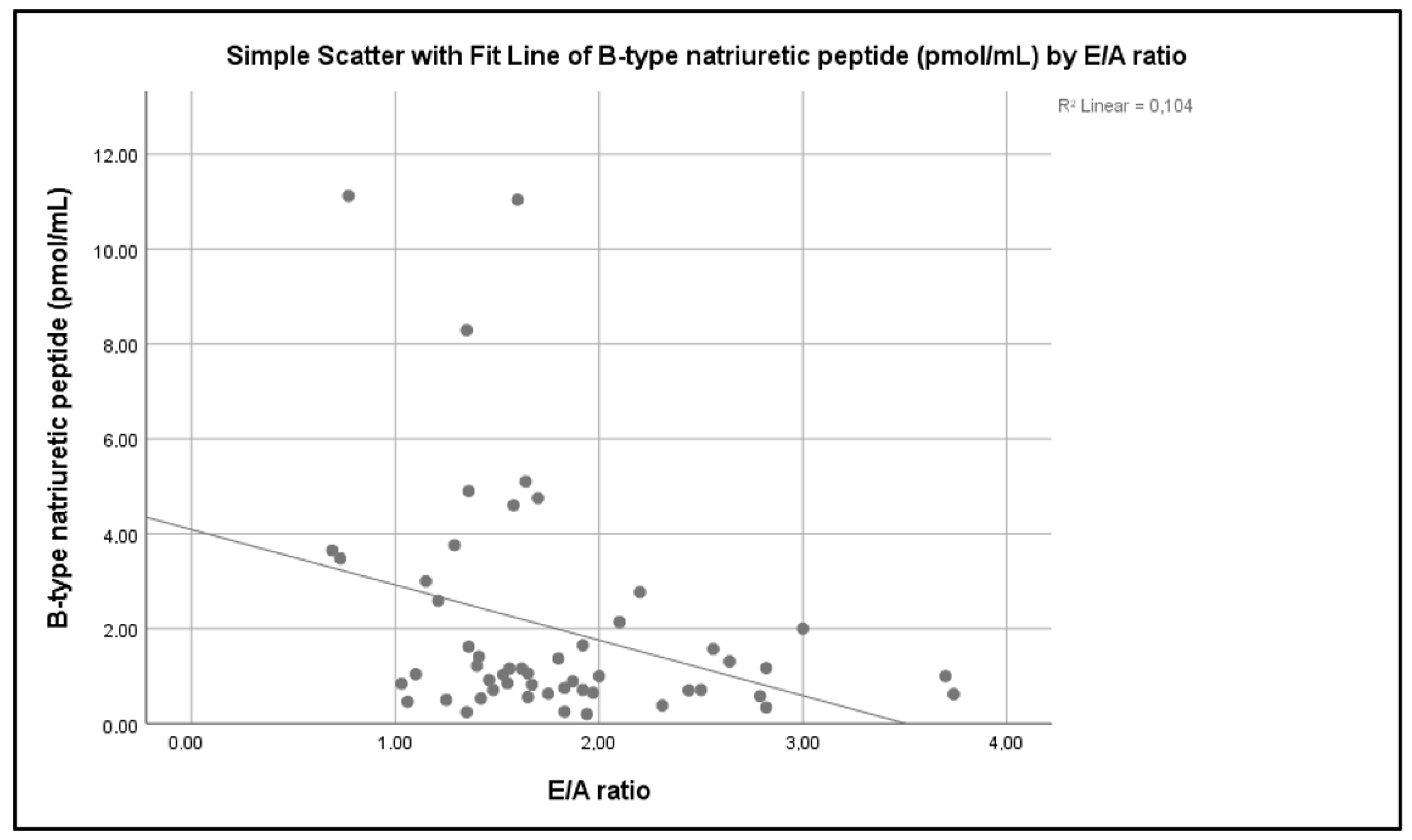
3.4. Correlations between BNP Levels and Demographic Parameters, Laboratory Markers, Medication Use and Cardiac Parameters
4. Discussion
5. Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, R. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harabat, J.; van Stralen, K.J.; Kim, J.J.; Tizard, J. Epidemiology of chronic kidney disease in children. Pediatr. Nephrol. 2012, 27, 363–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaspar, C.D.W.; Bholah, R.; Bunchman, T.E. A Review of Pediatric Chronic Kidney Disease. Blood Purif. 2016, 41, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Mitsnefes, M.M. Cardiovascular complications of pediatric chronic kidney disease. Pediatr. Nephrol. 2008, 23, 27–39. [Google Scholar] [CrossRef] [Green Version]
- Kavey, R.E.W.; Allada, V.; Daniels, S.R.; Hayman, L.L.; McCrindle, B.W.; Newburger, J.W.; Parekh, R.S.; Steinberger, J. Cardiovascular Risk Reduction in High-Risk Pediatric Patients A Scientific Statement From the American Heart Association Expert Panel on Population and Prevention Science; the Councils on Cardiovascular Disease in the Young, Epidemiology and Prevention, Nutrition, Physical Activity and Metabolism, High Blood Pressure Research, Cardiovascular Nursing, and the Kidney in Heart Disease; and the Interdisciplinary Working Group on Quality of Care and Outcomes Research Endorsed by the American Academy of Pediatrics. Circulation 2006, 114, 2710–2738. [Google Scholar]
- Mitsnefes, M.M.; Kimbal, T.R.; Border, W.L.; Witt, S.A.; Glascock, B.J.; Khoury, P.R.; Daniels, S.R. Impaired left ventricular diastolic function in children with chronic renal failure. Kidney Int. 2004, 65, 1461–1466. [Google Scholar] [CrossRef] [Green Version]
- Ariceta, G.; Brooks, E.R.; Langman, C.B. Assessing cardiovascular risk in children with chronic kidney disease. B-type natriuretic peptide: A potential new marker. Pediatr. Nephrol. 2005, 20, 1701–1707. [Google Scholar] [CrossRef]
- Neves, A.L.; Henriques-Coelho, T.; Leite-Moreira, A.; Areias, J.C. The Utility of Brain Natriuretic Peptide in Pediatric Cardiology: A Review. Pediatr. Crit. Care Med. 2016, 17, e529–e538. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkien, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Han, X.; Zhang, S.; Chen, Z.; Adhikari, K.B.; Zhang, Y.; Zhang, J.; Sun, J.; Wang, Y. Cardiac biomarkers of heart failure in chronic kidney disease. Clin. Chim. Acta 2020, 510, 298–310. [Google Scholar] [CrossRef]
- Fernandes, B.A.; Maher, K.O.; Deshpande, S.R. Cardiac biomarkers in pediatric heart disease: A state of art review. World J. Cardiol. 2016, 8, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Rinat, C.; Becker-Cohen, R.; Nir, A.; Feinstein, S.; Algur, N.; Ben-Shalom, E.; Farber, B.; Frishberg, Y. B-type natriuretic peptides are reliable markers of cardiac strain in CKD pediatric patients. Pediatr. Nephrol. 2012, 27, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Zoair, A.M.; Abdel-Hafez, M.A.; Mawlana, W.; Sweylam, M.A.R. Serum Levels of N-terminal-pro B-type Natriuretic Peptide as a Diagnostic Marker for Left Ventricular Dysfunction in Children with End-stage Renal Disease on Hemodialysis. Saudi J. Kidney Dis. Transpl. 2016, 27, 1114–1122. [Google Scholar] [PubMed]
- Hogg, R.J.; Furth, S.; Lemley, K.V.; Portman, R.; Schwartz, G.J.; Coresh, J.; Balk, E.; Lau, J.; Levin, A.; Kausz, A.T.; et al. National Kidney Foundation’s Kidney Disease Outcomes Quality Initiative Clinical Practice Guidelines for Chronic Kidney Disease in Children and Adolescents: Evaluation, Classification, and Stratification. Pediatrics 2003, 111, 1416–1421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, G.J.; Haycock, G.B.; Edelmann, C.M., JR.; Spitzer, A. A simple estimate of glomerular filtration rate in children derived from body length and plasma creatinine. Pediatrics 1976, 58, 259–263. [Google Scholar] [CrossRef]
- Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents; National Heart, Lung, and Blood Institute. Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents: Summary Report. Pediatrics 2011, 128 (Suppl. 5), S213–S256. [Google Scholar] [CrossRef] [Green Version]
- Eidem, B.W.; Cetta, F.; O’leary, P.W. (Eds.) Chapter 3: Quantitative Methods in Echocardiography—Basic Techniques. In Echocardiography in Pediatric and Adult Congenital Heart Disease; Har/Psc Edition; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2022. [Google Scholar]
- Devereaux, R.B.; Alonso, D.R.; Lutas, E.M.; Gottlieb, G.J.; Campo, E.; Sachs, I.; Reichek, N. Echocardiographic assessment of left ventricular hypertrophy: Comparison to necropsy findings. Am. J. Cardiol. 1986, 57, 450–458. [Google Scholar] [CrossRef]
- De Simone, G.; Daniels, S.R.; Devereux, R.B.; Meyer, R.A.; Roman, M.J.; De Divitiis, O.; Alderman, M.H. Left Ventricular Mass and Body Size in Normotensive Children ~nd Adults: Assessment of Allometric Relations and Impact of Overweight. J. Am. Coll. Cardiol. 1992, 20, 1251–1260. [Google Scholar] [CrossRef] [Green Version]
- Khoury, P.R.; Mitsnefes, M.; Daniels, S.R.; Kimball, T. Age-specific reference intervals for indexed left ventricular mass in children. J. Am. Soc. Echocardiol. 2009, 22, 709–714. [Google Scholar] [CrossRef]
- Daniels, S.R.; Loggie, J.M.; Khoury, P.; Kimball, T.R. Left ventricular geometry and severe left ventricular hypertrophy in children and adolescents with essential hypertension. Circulation 1998, 97, 1907–1911. [Google Scholar] [CrossRef] [Green Version]
- Hedvig, J.; Podracká, L.; Potočeková, D. Elevated Brain Natriuretic Peptide Is Associated with Abnormal Heart Geometry in Children with Chronic Kidney Disease. Kidney Blood Press. Res. 2010, 33, 87–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nalcacioglu, H.; Ozkaya, O.; Kafali, H.C.; Tekcan, D.; Avci, B.; Baysal, K. Is N-terminal pro-brain natriuretic peptide a reliable marker for body fluid status in children with chronic kidney disease? Arch. Med. Sci. 2020, 16, 802–810. [Google Scholar] [CrossRef] [PubMed]
- Ouali, S.; Bougmiza, I.; Abroug, S.; Omezzine, A.; Salem, H.B.; Neffeti, E.; Remedi, F.; Bouslema, A.; Harabi, A.; Boughzela, E. Relationship of Brain Natriuretic Peptide Concentrations to Left Ventricular Function and Adverse Outcomes in Children with End-Stage Renal Disease Undergoing Hemodialysis. Pediatr. Cardiol. 2011, 32, 568–577. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, F.A.; Sad, I.A.E.S.; Elshamaa, M.F.; Badr, A.M.; Eldayem, S.A.; Ashmawy, I.; Elrahim, Y.A.E.M.A. Left ventricular dysfunction by conventional and tissue Doppler echocardiography in pediatric hemodialysis patients: Relation with plasma brain natriuretic peptide levels. Arch. Med. Sci. Atheroscler. Dis. 2018, 3, e18–e28. [Google Scholar] [CrossRef] [PubMed]
- Safley, D.M.; Awad, A.; Sullivan, R.A.; Sandberg, K.R.; Mourad, I.; Boulware, M.; Merhi, W.; McCullough, P.A. Changes in B-type Natriuretic Peptide levels in hemodialysis and the effect of depressed left ventricular function. Adv. Chronic Kidney Dis. 2005, 12, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Bargnoux, A.-S.; Klouche, K.; Fareh, J.; Barazer, I.; Villard-Saussine, S.; Dupuy, A.-M.; Leray-Moragues, H.; Giuliani, I.; Canaud, B.; Cristol, J.P. Prohormone brain natriuretic peptide (proBNP), BNP and N-terminal-proBNP circulating levels in chronic hemodialysis patients. Correlation with ventricular function, fluid removal and effect of hemodiafiltration. Clin. Chem. Lab. Med. 2008, 46, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Song, J.H.; Kim, G.A.; Lim, H.J.; Kim, M.-J. Plasma brain natriuretic peptide concentration on assessment of hydration status in hemodialysis patient. Am. J. Kidney Dis. 2003, 41, 1257–1266. [Google Scholar] [CrossRef]
- Laveborn, E.; Lindmark, K.; Skagerlind, M.; Stegmayr, B. NT-proBNP and troponin T levels differ after haemodialysis with a low versus high flux membrane. Int. J. Artif. Organs 2015, 38, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.-L.; Fahim, M.; Johnson, D.W. Pathophysiology and significance of natriuretic peptides in patients with end-stage kidney disease. Clin. Biochem. 2020, 83, 1–11. [Google Scholar] [CrossRef]
- Khalifeh, N.; Haider, D.; Horl, W.H. Natriuretic Peptides in Chronic Kidney Disease and During Renal Replacement Therapy: An Update. J. Investig. Med. 2009, 57, 33–39. [Google Scholar] [CrossRef]
- Wahl, H.G.; Graf, S.; Renz, H.; Fassbinder, W. Elimination of the Cardiac Natriuretic Peptides B-Type Natriuretic Peptide (BNP) and N-Terminal proBNP by Hemodialysis. Clin. Chem. 2004, 50, 1071–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koch, A.; Singer, H. Normal values of B type natriuretic peptide in infants, children, and adolescents. Heart 2003, 89, 875–878. [Google Scholar] [CrossRef] [PubMed]
- Nir, A.; Bar-Oz, B.; Perles, Z.; Brooks, R.; Korach, A.; Rein, A.J.J.T. N-Terminal pro-B-type natriuretic peptide: Reference plasma levels from birth to adolescence; elevated levels at birth and in heart diseases. Acta Paediatr. 2004, 93, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Clerico, A.; Giannoni, A.; Vittorini, S.; Emdin, M. The paradox of low BNP levels in obesity. Heart Fail. Rev. 2012, 17, 81–96. [Google Scholar] [CrossRef]
- Hwang, H.-H.; Hong, S.-J.; Che, M.-Y.; Ko, C.-W. The Usefulness of NT-proBNP in Children with Chronic Kidney Disease. Korean J. Nephrol. 2009, 199–204. [Google Scholar]
- Skrzypczyk, P.; Okarska-Napierała, M.; Pietrzak, R.; Pawlik, K.; Wascinska, K.; Werner, B.; Panczyk-Tomaszewska, M. NT-proBNP as a Potential Marker of Cardiovascular Damage in Children with Chronic Kidney Disease. J. Clin. Med. 2021, 10, 4344. [Google Scholar] [CrossRef]
- Becker-Cohen, R.; Nir, A.; Rinat, C.; Feinstein, S.; Algur, N.; Farber, B.; Frishberg, Y. Risk Factors for Cardiovascular Disease in Children and Young Adults after Renal Transplantation. Clin. J. Am. Soc. Nephrol. 2006, 1, 1284–1292. [Google Scholar] [CrossRef] [Green Version]
- Kushimira, C.; Masutani, S.; Kuwata, S.; Iwamoto, Y.; Saiki, H.; Ishido, H.; Tamura, M.; Senzaki, H. Cystatin C and body surface area are major determinants of the ratio of N-terminal pro-brain natriuretic peptide to brain natriuretic peptide levels in children. J. Cardiol. 2015, 66, 175–180. [Google Scholar]
- Matias, P.J.; Ferreira, C.; Jorge, C.; Borges, M.; Aires, I.; Amaral, T.; Gil, C.; Cortez, J.; Ferreira, A. 25-Hydroxyvitamin D3, arterial calcifications and cardiovascular risk markers in haemodialysis patients. Nephrol. Dial. Transplant. 2009, 24, 611–618. [Google Scholar] [CrossRef] [Green Version]
- Obineche, E.N.; Saadi, H.; Benedict, S.; Pathan, J.Y.; Frampton, C.M.; Nicholls, M.G. Interrelationships between B-type Natriuretic peptides and vitamin D inpatients on maintenance peritoneal dialysis. Perit. Dial. Int. 2008, 28, 617–621. [Google Scholar] [CrossRef]
- Yi, S.; Chen, M. Decreased albumin is associated with elevated Nterminal pro-brain natriuretic peptide and poor long-term prognosis in patients with chronic heart failure. Medicine 2020, 99, 51. [Google Scholar] [CrossRef] [PubMed]
- Clothier, J.C.; Simpson, J.M.; Turner, C.; Dalton, R.N.; Rasmussen, P.; Rawlins, D.; Booth, C.J.; Peacock, J.L.; Sinha, M.D. Investigating the Role of Cardiovascular Biomarkers in Children with Pre-Dialysis Chronic Kidney Disease: A Substitute to Echocardiography to Detect Increased Left Ventricular Mass? Nephron Clin. Pract. 2013, 124, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.S.; Baek, J.S.; Yu, J.J.; Kim, Y.-H.; Ko, J.-K.; Lee, J.H. B-Type Natriuretic peptide levels and cardiac dysfunction in children on peritoneal dialysis. Perit. Dial. Int. 2019, 39, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Garoufi, A.; Drapanioti, S.; Marmarinos, A.; Askiti, V.; Mitsioni, A.J.; Mila, M.; Grigoriadou, G.; Georgakopoulos, D.; Stefanidis, C.J.; Gourgiotis, D. Plasma Urotensin II levels in children and adolescents with chronic kidney disease: A single-centre study. BMC Nephrol. 2017, 18, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Total (n = 56) | Pre-Dialysis Stage Group (n = 24) | HD Group (n = 14) | RTRs Group (n = 18) | p Value |
|---|---|---|---|---|---|
| Age (years) | 11.55 (8.4–14.5) | 11.45 (7.9–15.35) | 10.65 (8.4–12.7) | 12.2 (10.6–14.6) | 0.362 |
| Gender M/F (%) | 60.7/39.3 | 70.8/29.2 | 57.1/42.9 | 50/50 | 0.373 |
| Pre-pubertal/Pubertal stage (%) | 50/50 | 50/50 | 64.3/35.7 | 38.9/61.1 | 0.109 |
| CKD stages 2 and 3 (%) | 12.5/42.9 | 0/58.3 | 0/0 | 38.9/55.6 | |
| CKD stages 4 and 5 (%) | 16.1/28.6 | 33.3/8.3 | 0/100 | 5.6/0 | |
| BMI (kg/m2) | 18.58 (16.6–20.93) | 18.61 (16.74–20.8) | 15.97 (14.82–19.2) | 19.1 (17.98–21.98) | 0.004 |
| BMI z-score | −0.17 (−0.68–0.44) | −0.16 (−0.64–−0.41) | −0.84 (−1.14–0.01) | −0.03 (−0.32–0.71) | 0.004 |
| SBP (mmHg) | 109 (99–119) | 107 (96–120) | 111 (87–119) | 107 (100–118) | 0.084 |
| DBP (mmHg) | 67 (56–74) | 65 (52–73) | 68 (55–77) | 68 (61–73) | 0.004 |
| Pre-hypertension /Hypertension (%) | 25/12.5 | 16.7/4.2 | 35.7/28.6 | 27.8/11.1 | 0.615 |
| eGFR (ml/min/1.73 m2) | 33 (9–52) | 31 (22–47) | 6 (6–7) | 59 (47–63) | <0.001 |
| Creatinine (mg/dl) | 1.65 (1.1–5.25) | 1.7 (1.3–2.2) | 7.5 (6.8–9) | 1 (0.8–1.2) | <0.001 |
| Cystatin C (mg/L) | 2.01 (1.42–4.91) | 1.86 (1.55–3.16) | 6.54 (6.15–6.96) | 1.42 (1.04–1.67) | <0.001 |
| Albumin (g/dl) | 4.5 (4.3–4.7) | 4.6 (4.5–4.7) | 4.3 (4–4.6) | 4.45 (4.4–4.7) | 0.048 |
| Hemoglobulin (g/dl) | 11.85 (10.7–12.9) | 12.35 (10.85–13.6) | 10.9 (10.5–11.9) | 11.8 (11–12.7) | 0.131 |
| Hematocrit (%) | 35.75 (32.85–38.7) | 37.2 (34.05–39.95) | 33.75 (31.3–35.7) | 36 (32.4–39.6) | 0.043 |
| Anemia (%) | 51.8 | 37.5 | 71.4 | 55.6 | 0.121 |
| iPTH (pg/mL) | 85.35 (60.69–144) | 82.61 (50–116.3) | 257 (92.92–416.9) | 76.15 (57.65–92.24) | 0.066 |
| 25(OH)D (ng/mL) | 20.24 (13.6–31.06) | 28 (19.57–37.4) | 12.87 (6.57–14.37) | 19.82 (13.89–25.99) | 0.033 |
| Parameter | Total (n = 53) | Pre-Dialysis Stage Group (n = 24) | HD Group * (n = 12) | RTRs Group (n = 17) |
|---|---|---|---|---|
| LA (cm) | 2.57 (2.25–2.89) | 2.6 (2.15–2.82) | 2.29 (2.09–2.57) | 2.76 (2.43–3.1) |
| LVEDD (cm) | 3.81 (3.32–4.12) | 3.85 (3.4–4.33) | 3.18 (2.93–3.62) | 3.94 (3.58–4.12) |
| LVESD (cm) | 2.23 (1.83–2.42) | 2.26 (1.9–2.61) | 1.94 (1.73–2.11) | 2.33 (2.11–2.42) |
| IVSd (cm) | 0.66 (0.55–0.74) | 0.66 (0.52–0.75) | 0.64 (0.57–0.76) | 0.62 (0.55–0.73) |
| PWT (cm) | 0.6 (0.55–0.68) | 0.58 (0.5–0.66) | 0.6 (0.55–0.71) | 0.66 (0.57–0.75) |
| EF (%) | 70.4 (65–72.8) | 71 (66.25–75.4) | 65.15 (62.35–71.45) | 70.5 (66.4–72.2) |
| E (m/sec) | 0.85 (0.78–1.03) | 0.85 (0.79–1.1) | 0.84 (0.52–0.95) | 0.87 (0.83–1.03) |
| A (m/sec) | 0.51 (0.43–0.65) | 0.51 (0.38–0.6) | 0.51 (0.49–0.67) | 0.5 (0.4–0.68) |
| E/A ratio | 1.65 (1.36–2) | 1.65 (1.46–2.44) | 1.33 (0.96–1.67) | 1.78 (1.41–2) |
| DT (m/sec) | 158.5 (140–178) | 164 (146–182) | 162 (140–180) | 152 (130–174) |
| RWT | 0.32 (0.29–0.37) | 0.31 (0.28–0.33) | 0.36 (0.34–0.43) | 0.33 (0.29–0.37) |
| HR (heats/sec) | 87 (75–96) | 93 (71–105) | 91 (80–96) | 85 (81–91) |
| Groups/Subgroups | BNP (pmol/mL) Median, IQR | p Value |
|---|---|---|
| Overall CKD Patients | 1.05 (0.71, 2.07) | p < 0.001 |
| Control group | 0.67 (0.51, 091) | |
| CKD in Pre-dialysis stage | 0.91 (0.59, 1.19) | p = 0.030 |
| Corresponding Controls | 0.65 (0.51, 0.90) | |
| HD: before dialysis | 3.24 (2.00, 4.75) | p < 0.001 |
| Corresponding Controls | 0.61 (0.44, 0.80) | |
| HD: after dialysis | 3.75 (2.78, 5.17) | p < 0.001 |
| Corresponding Controls | 0.61 (0.44, 0.80) | |
| RTRs | 0.83 (0.63, 1.31) | p = 0.273 |
| Corresponding Controls | 0.77 (0.51, 0.97) |
| Parameter | Coefficient | p Value |
|---|---|---|
| Cystatin C | 1.075 (0.651–1.500) | <0.001 |
| Creatinine | −0.555 (−0.885–−0.224) | 0.001 |
| Albumin | −1.988 (−3.286–−0.691) | 0.003 |
| Total 25(OH)D | −0.037(−0.0070–−0.004) | 0.028 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garoufi, A.; Koumparelou, A.; Askiti, V.; Lykoudis, P.; Mitsioni, A.; Drapanioti, S.; Servos, G.; Papadaki, M.; Gourgiotis, D.; Marmarinos, A. Plasma Brain Natriuretic Peptide Levels in Children with Chronic Kidney Disease and Renal Transplant Recipients: A Single Center Study. Children 2022, 9, 916. https://doi.org/10.3390/children9060916
Garoufi A, Koumparelou A, Askiti V, Lykoudis P, Mitsioni A, Drapanioti S, Servos G, Papadaki M, Gourgiotis D, Marmarinos A. Plasma Brain Natriuretic Peptide Levels in Children with Chronic Kidney Disease and Renal Transplant Recipients: A Single Center Study. Children. 2022; 9(6):916. https://doi.org/10.3390/children9060916
Chicago/Turabian StyleGaroufi, Anastasia, Aikaterini Koumparelou, Varvara Askiti, Panagis Lykoudis, Andromachi Mitsioni, Styliani Drapanioti, Georgios Servos, Maria Papadaki, Dimitrios Gourgiotis, and Antonios Marmarinos. 2022. "Plasma Brain Natriuretic Peptide Levels in Children with Chronic Kidney Disease and Renal Transplant Recipients: A Single Center Study" Children 9, no. 6: 916. https://doi.org/10.3390/children9060916