
Parathyroid Hormone-Related Peptide (PTHrP): Evaluation of Pediatric, Covariate-Stratified Reference Intervals

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Sample Management
2.3. Analytical Determination
2.4. Statistical Analyzes
3. Results
4. Categorical Analysis
5. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Donovan, P.J.; Achong, N.; Griffin, K.; Galligan, J.; Pretorius, C.J.; McLeod, D.S. PTHrP-mediated hypercalcemia: Causes and survival in 138 patients. J. Clin. Endocrinol. Metab. 2015, 100, 2024–2029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goltzman, D. Nonparathyroid Hypercalcemia. Front. Horm. Res. 2019, 51, 77–90. [Google Scholar] [PubMed]
- Ngan, B.L.; Dorothy, M. Physiological roles of parathyroid hormone-related protein. Acta Biomed. 2019, 90, 510–516. [Google Scholar] [CrossRef]
- Martin, T.J. Parathyroid Hormone-Related Protein, Its Regulation of Cartilage and Bone Development, and Role in Treating Bone Diseases. Physiol. Rev. 2016, 96, 831–871. [Google Scholar] [CrossRef] [Green Version]
- John, J. Wysolmerski Parathyroid Hormone-Related Protein: An Update. J. Clin. Endocrinol. Metab. 2012, 97, 2947–2956. [Google Scholar]
- McCauley, L.K.; Martin, T.J. Twenty-five years of PTHrP progress: From cancer hormone to multifunctional cytokine. J. Bone Miner. Res. 2012, 27, 1231–1239. [Google Scholar] [CrossRef] [Green Version]
- Portal-Núñez, S.; Ardura, J.A.; Lozano, D.; De Toda, I.M.; De La Fuente, M.; Herrero-Beaumont, G.; Largo, R.; Esbrit, P. Parathyroid hormone-related protein exhibits antioxidant features in osteoblastic cells through its N-terminal and osteostatin domains. Bone Jt. Res. 2018, 7, 58–68. [Google Scholar] [CrossRef]
- Jans, D.A.; Thomas, R.J.; Gillespie, M.T. Parathyroid hormonerelated protein (PTHrP): A nucleocytoplasmic shuttling protein with distinct paracrine and intracrine roles. Vitam. Horm. 2003, 66, 345–384. [Google Scholar]
- Cafforio, P.; Savonarola, A.; Stucci, S.; De Matteo, M.; Tucci, M.; Brunetti, A.E.; Vecchio, V.M.; Silvestris, F. PTHrP Produced by Myeloma Plasma Cells Regulates Their Survival and Pro-Osteoclast Activity For Bone Disease Progression. J. Bone Miner. Res. 2013, 29, 55–66. [Google Scholar] [CrossRef]
- Edwards, C.M.; Johnson, R.W. From Good to Bad: The Opposing Effects of PTHrP on Tumor Growth, Dormancy, and Metastasis Throughout Cancer Progression. Front. Oncol. 2021, 11, 644303. [Google Scholar] [CrossRef]
- Kramann, R.; Schneider, R.K. Parathyroid hormone-related protein and regulation of cell survival in the kidney. Kidney Int. 2013, 83, 777–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKay, C.; Furman, W.L. Hypercalcemia complicating childhood malignancies. Cancer 1993, 72, 256–260. [Google Scholar] [CrossRef]
- Wood, A.J.; Bilezikian, J.P. Management of Acute Hypercalcemia. N. Engl. J. Med. 1992, 326, 1196–1203. [Google Scholar] [CrossRef] [PubMed]
- Kodous, N.; Filler, G.; Sharma, A.P.; Van Hooren, T.A. PTHrP-related Hypercalcaemia in Infancy and Congenital Anomalies of the Kidney and Urinary Tract (CAKUT). Can. J. Kidney Health Dis. 2015, 2, 21. [Google Scholar] [CrossRef] [Green Version]
- Lietman, S.A.; Germain-Lee, E.L.; Levine, M.A. Hypercalcemia in children and adolescents. Curr. Opin. Pediatr. 2010, 22, 508–515. [Google Scholar] [CrossRef] [Green Version]
- Hirschfeld, R.; Welch, J.J.; Harrison, D.J.; Kremsdorf, R.; Chawla, A. Two cases of humoral hypercalcemia of malignancy complicating infantile fibrosarcoma. Pediatr. Blood Cancer 2017, 64, e26511. [Google Scholar] [CrossRef]
- Inukai, T.; Hirose, K.; Inaba, T.; Kurosawa, H.; Hama, A.; Inada, H.; Chin, M.; Nagatoshi, Y.; Ohtsuka, Y.; Oda, M.; et al. Hypercalcemia in childhood acute lymphoblastic leucemia: Frequent implication of parathyroid hormone-related peptide and E2A-HLF from translocation 17;19. Leukemia 2007, 21, 288–296. [Google Scholar] [CrossRef] [Green Version]
- Dagdelen, S.; Gurlek, A.; Kalan, I. Humoral Hypercalcemia of Benignancy Secondary to Parathyroid Hormone-Related Protein Secreting Uterine Leiomyoma. Am. J. Med Sci. 2008, 335, 407–408. [Google Scholar] [CrossRef]
- Herring, R.; Laji, K. Humoral hypercalcaemia of benignancy. A case report. QJM Int. J. Med. 2008, 101, 329–330. [Google Scholar] [CrossRef]
- Takeda, K.; Hara, N.; Kawaguchi, M.; Nishiyama, T.; Takahashi, K. Parathyroid hormone-related peptide-producing non-familial pheochromocytoma in a child. Int. J. Urol. 2010, 17, 673–676. [Google Scholar] [CrossRef]
- Stokes, V.J.; Nielsen, M.F.; Hannan, F.M.; Thakker, R.V. Hypercalcemic Disorders in Children. J. Bone Miner. Res. 2017, 32, 2157–2170. [Google Scholar] [CrossRef] [PubMed]
- Hoyoux, C.; Lombet, J.; Nicolescu, C.R. Malignancy-Induced Hypercalcemia—Diagnostic Challenges. Front. Pediatr. 2017, 5, 233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratcliffe, W.; Ratcliffe, J.; Hutchesson, A.; Bundred, N. Role of assays for parathyroid-hormone-related protein in investigation of hypercalcaemia. Lancet 1992, 339, 164–167. [Google Scholar] [CrossRef]
- CLSI. Defining, Establishing, and Verifying Reference Intervals in the Clinical Laboratory; Approved Guideline, 3rd ed.; CLSI Document C28-A3; CLSI: Wayne, PA, USA, 2008. [Google Scholar]
- Tukey, J.W. Exploratory Data Analysis; Addison-Wesley: Boston, MA, USA, 1977. [Google Scholar]
- Hubert, M.; Van der Veeken, S. Outlier detection for skewed data. J. Chemom. 2008, 22, 235–246. [Google Scholar] [CrossRef]
- Fritchie, K.; Zedek, D.; Grenache, D.G. The clinical utility of parathyroid hormone-related peptide in the assessment of hypercalcemia. Clin. Chim. Acta 2009, 402, 146–149. [Google Scholar] [CrossRef]
- Tate, J.R.; Yen, T.; Jones, G.R.D. Transference and Validation of Reference Intervals. Clin. Chem. 2015, 61, 1012–1015. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Sun, Y.; Zheng, H.; Li, L.; Yu, Q.; Yao, X. Parathyroid hormone-related protein overexpression protects goat mammary gland epithelial cells from calcium-sensing receptor activation-induced apoptosis. Mol. Biol. Rep. 2014, 42, 233–243. [Google Scholar] [CrossRef]
- Bond, H.; Dilworth, M.; Baker, B.; Cowley, E.; Jimenez, A.R.; Boyd, R.D.H.; Husain, S.M.; Ward, B.S.; Sibley, C.P.; Glazier, J.D. Increased maternofetal calcium flux in parathyroid hormone-related protein-null mice. J. Physiol. 2008, 586, 2015–2025. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
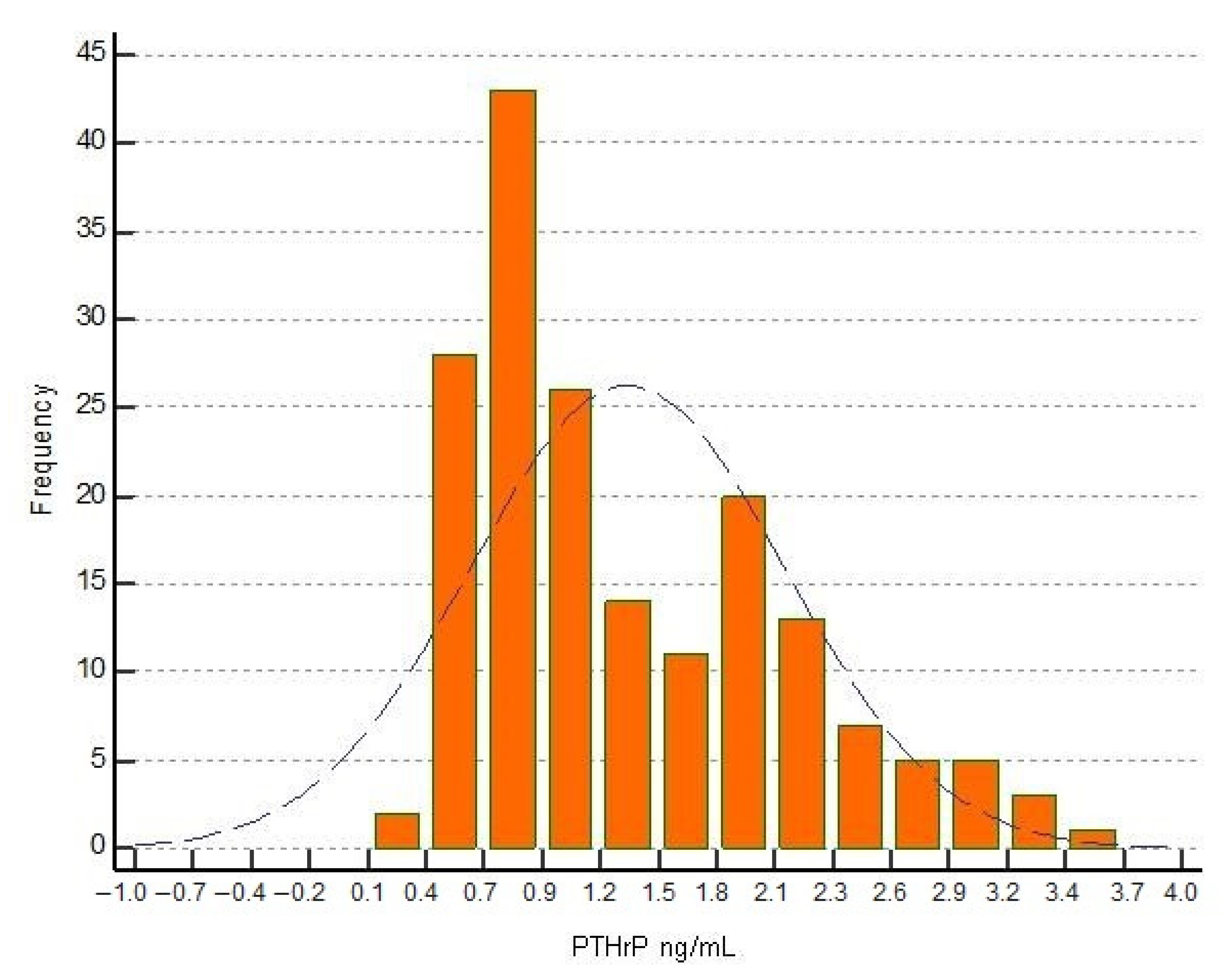
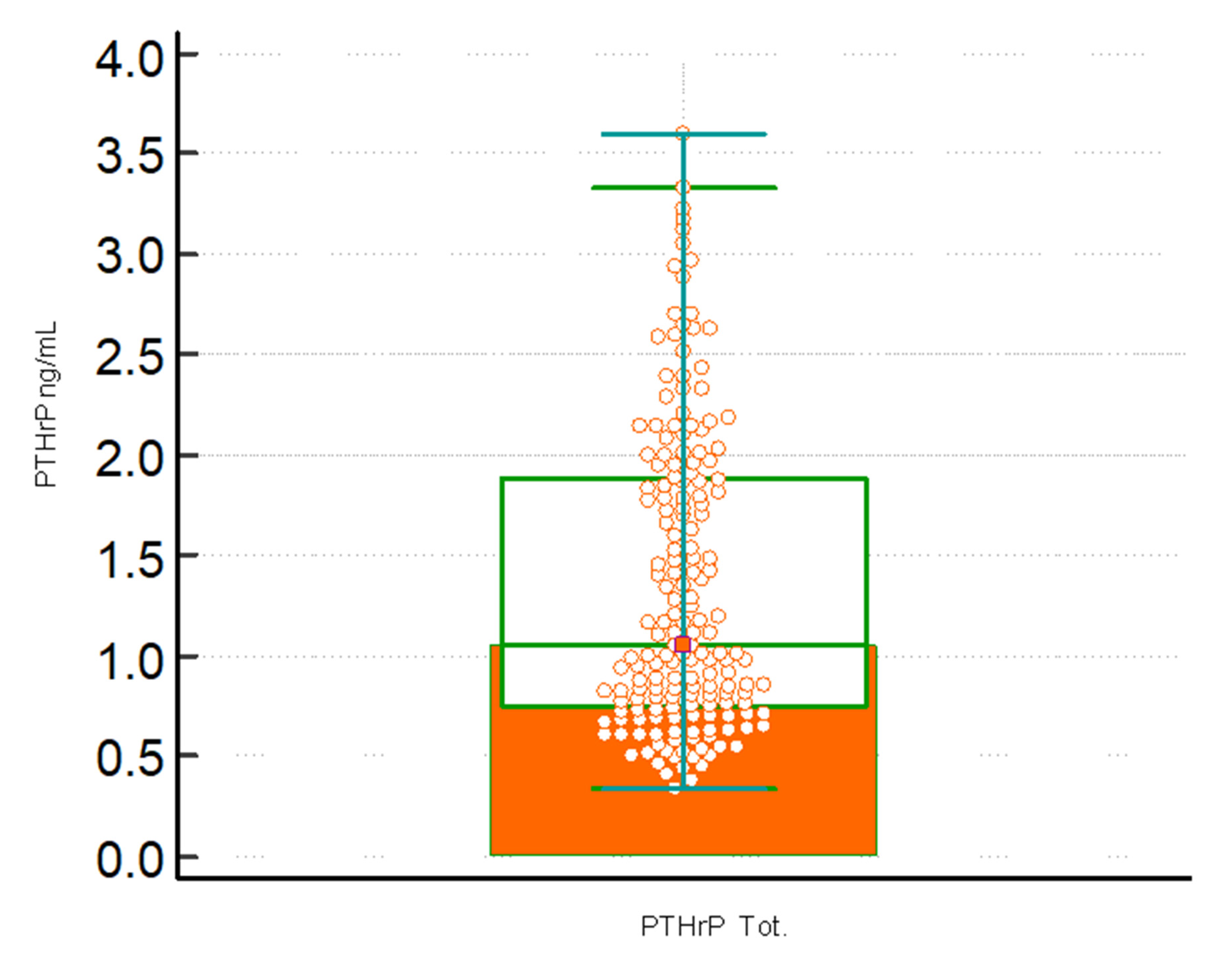
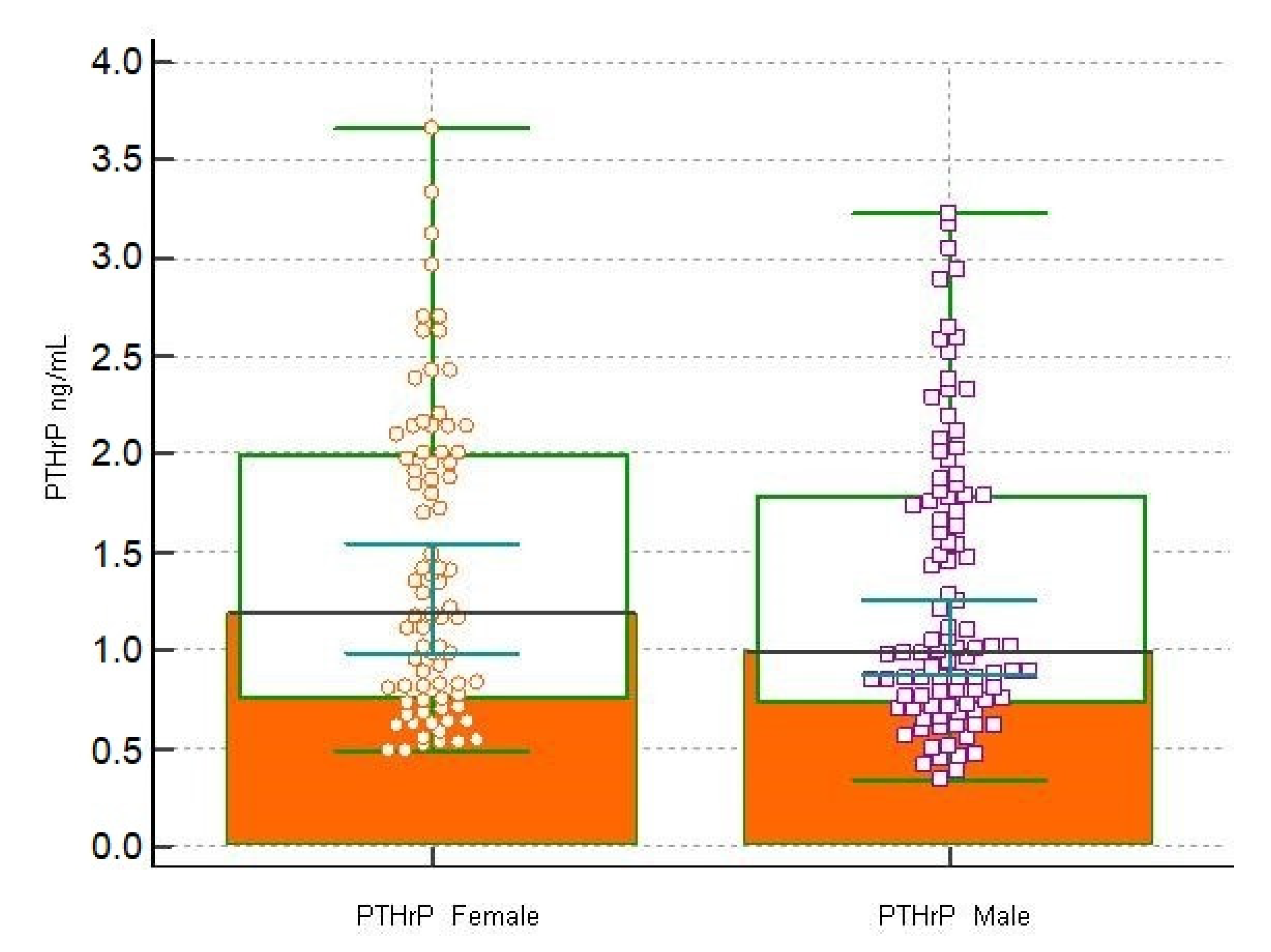
| Measurements | PTHrP (ng/mL) | PTHrP-M (ng/mL) | PTHrP-F (ng/mL) |
|---|---|---|---|
| Sample size (n) | 178 | 98 | 80 |
| Highest value | 3.66 | 3.23 | 3.66 |
| Mean | 1.35 | 1.29 | 1.43 |
| 95% CI | 1.24 to 1.46 | 1.14 to 1.43 | 1.26 to 1.60 |
| Geometric mean | 1.16 | 1.11 | 1.24 |
| Median | 1.08 | 1.00 | 1.20 |
| Standard deviation | 0.75 | 0.73 | 0.78 |
| 2.5–97.5 percentile | 0.45 to 3.12 | 0.41 to 3.06 | 0.50 to 3.22 |
| 5–95 percentile | 0.50 to 2.81 | 0.45 to 2.78 | 0.53 to 2.83 |
| Kolmogorov-Smirnov test for Normal distribution | p < 0.0001 | p < 0.0001 | p = 0.0016 |
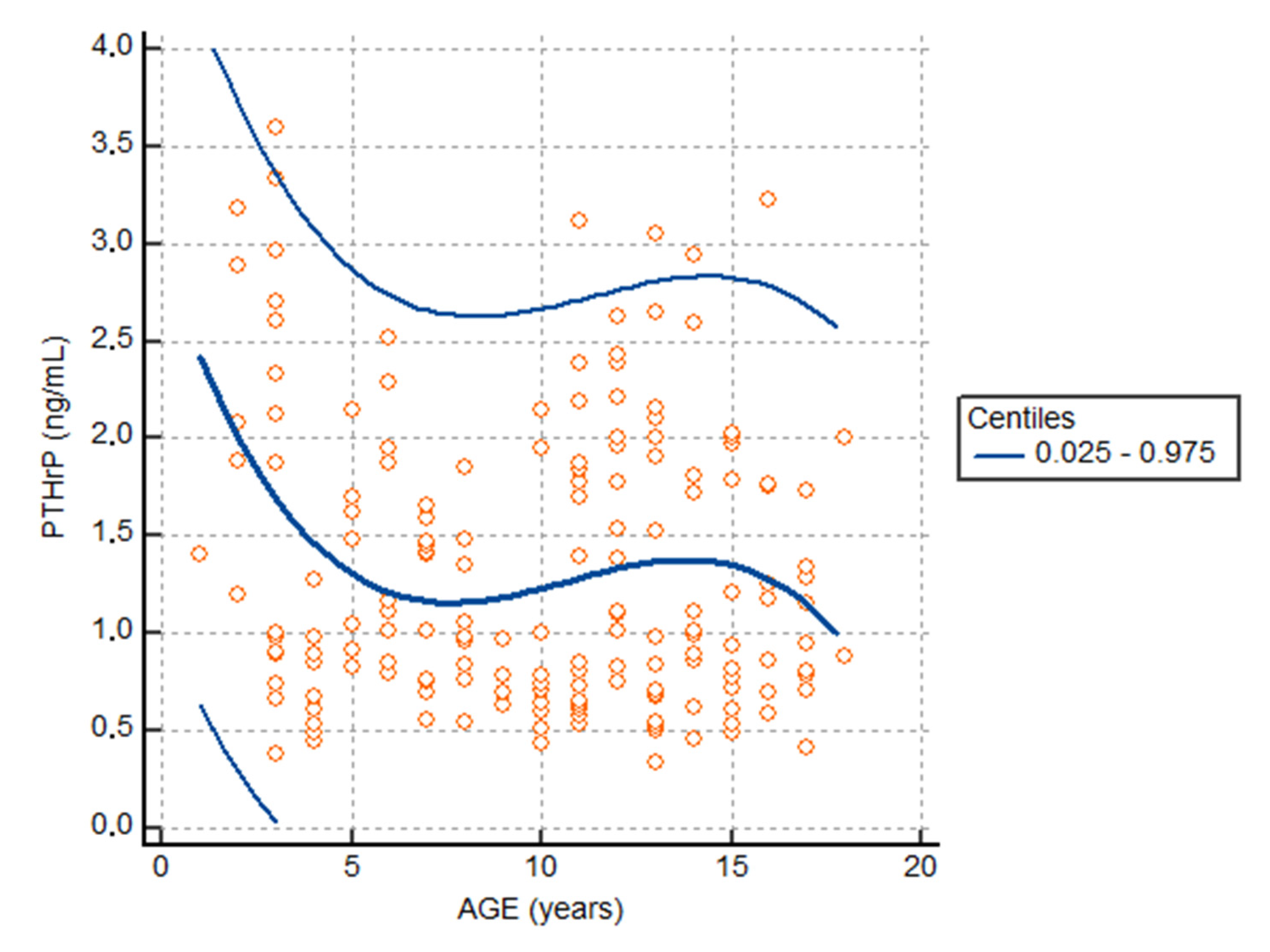
| Age Variable | Centiles of PTHrP ng/mL | |||
|---|---|---|---|---|
| (Years) | 0.025 | 0.05 | 0.95 | 0.975 |
| 2 | −1.14 | −0.69 | 3.98 | 4.43 |
| 4 | −0.21 | 0.04 | 2.67 | 2.92 |
| 6 | 0.20 | 0.37 | 2.23 | 2.41 |
| 8 | 0.15 | 0.34 | 2.24 | 2.41 |
| 10 | −0.11 | 0.11 | 2.44 | 2.66 |
| 12 | −0.38 | −0.11 | 2.65 | 2.92 |
| 14 | −0.46 | −0.19 | 2.72 | 3.00 |
| 16 | −0.17 | 0.06 | 2.47 | 2.70 |
| 18 | −0.47 | 0.44 | 1.97 | 2.64 |
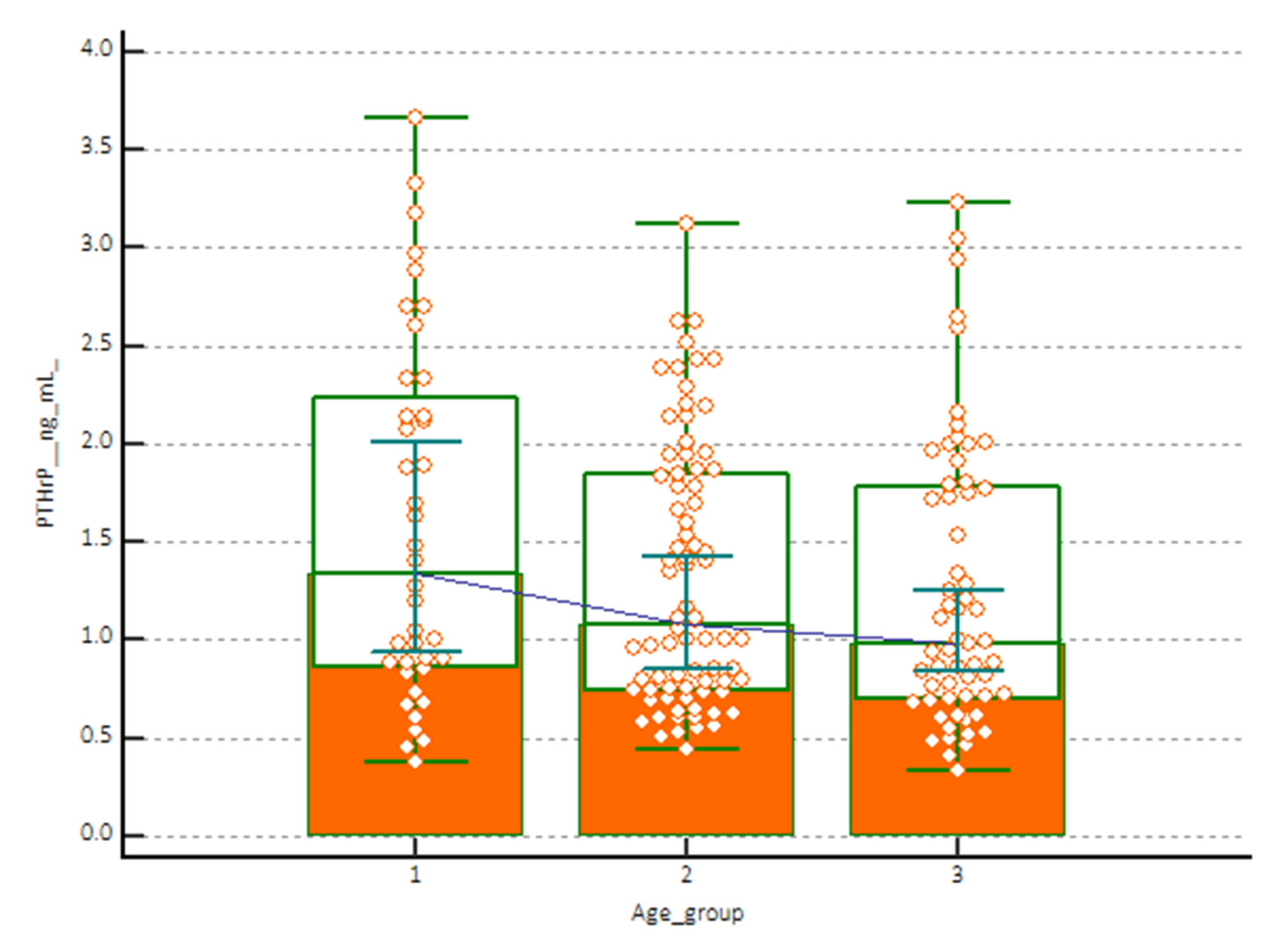
| Measurements | PTHrP (1–5 Years) ng/mL | PTHrP (6–12 Years) ng/mL | PTHrP (13–18 Years) ng/mL |
|---|---|---|---|
| Sample size | 40 | 78 | 60 |
| Lowest value | 0.38 | 0.44 | 0.34 |
| Highest value | 3.66 | 3.12 | 3.23 |
| Arithmetic mean | 1.59 | 1.31 | 1.25 |
| Median | 1.35 | 1.08 | 0.99 |
| Standard deviation | 0.91 | 0.66 | 0.72 |
| Kolmogorov-Smirnov test for normal distribution | reject Normality (p = 0.0044) | reject Normality (p < 0.0001) | reject Normality (p = 0.0003) |
| Mann-Whitney Test (Independent Samples) | |
|---|---|
| Variable | Two-Tailed Probability |
| PTHrP-M (ng/mL) vs PTHrP-F (ng/mL) | p = 0.2305 |
| PTHrP (1–5 years) ng/mL vs PTHrP (6–12 years) ng/mL | p = 0.1585 |
| PTHrP (1–5 years) ng/mL vs PTHrP (13–18 years) ng/mL | p = 0.0700 |
| PTHrP (6–12 years) ng/mL vs PTHrP (13–18 years) ng/mL | p = 0.4653 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brescia, V.; Fontana, A.; Lovero, R.; Capobianco, C.; Marsico, S.V.; De Chirico, T.; Pinto, C.; Mascolo, E.; Cazzolla, A.P.; Faienza, M.F.; et al. Parathyroid Hormone-Related Peptide (PTHrP): Evaluation of Pediatric, Covariate-Stratified Reference Intervals. Children 2022, 9, 896. https://doi.org/10.3390/children9060896
Brescia V, Fontana A, Lovero R, Capobianco C, Marsico SV, De Chirico T, Pinto C, Mascolo E, Cazzolla AP, Faienza MF, et al. Parathyroid Hormone-Related Peptide (PTHrP): Evaluation of Pediatric, Covariate-Stratified Reference Intervals. Children. 2022; 9(6):896. https://doi.org/10.3390/children9060896
Chicago/Turabian StyleBrescia, Vincenzo, Antonietta Fontana, Roberto Lovero, Carmela Capobianco, Stella Vita Marsico, Tiziana De Chirico, Carla Pinto, Elisa Mascolo, Angela Pia Cazzolla, Maria Felicia Faienza, and et al. 2022. "Parathyroid Hormone-Related Peptide (PTHrP): Evaluation of Pediatric, Covariate-Stratified Reference Intervals" Children 9, no. 6: 896. https://doi.org/10.3390/children9060896