
Early Physiotherapy Intervention Program for Preterm Infants and Parents: A Randomized, Single-Blind Clinical Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
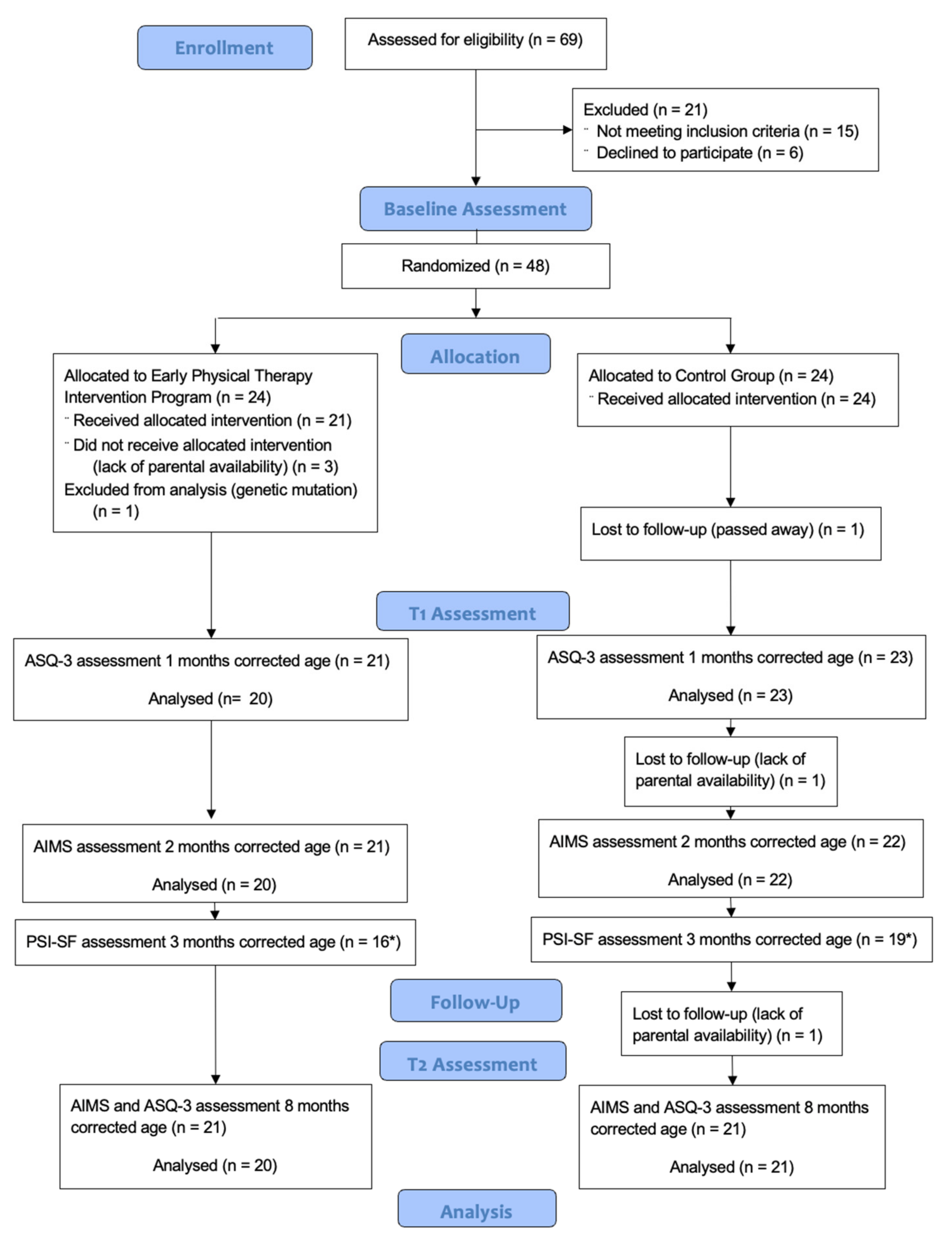
2.1. Study Design
2.2. Participants
2.3. Sample Size
2.4. Randomization and Masking
2.5. Intervention
2.6. Measures
2.7. Statistical Analysis
3. Results
3.1. Primary Outcome Measure (AIMS)
3.2. Secondary Outcome Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mottahedin, A.; Ardalan, M.; Chumak, T.; Riebe, I.; Ek, J.; Mallard, C. Effect of Neuroinflammation on Synaptic Organization and Function in the Developing Brain: Implications for Neurodevelopmental and Neurodegenerative Disorders. Front. Cell. Neurosci. 2017, 11, 190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadders-Algra, M. Early Human Brain Development: Starring the Subplate. Neurosci. Biobehav. Rev. 2018, 92, 276–290. [Google Scholar] [CrossRef] [PubMed]
- Valentini, N.C.; Pereira, K.R.G.; Chiquetti, E.M.D.S.; Formiga, C.K.M.R.; Linhares, M.B.M. Motor Trajectories of Preterm and Full-Term Infants in the First Year of Life. Pediatr. Int. 2019, 61, 967–977. [Google Scholar] [CrossRef] [PubMed]
- Albuquerque, P.L.D.; Lemos, A.; Guerra, M.Q.D.F.; Eickmann, S.H. Accuracy of the Alberta Infant Motor Scale (AIMS) to Detect Developmental Delay of Gross Motor Skills in Preterm Infants: A Systematic Review. Dev. Neurorehabilit. 2015, 18, 15–21. [Google Scholar] [CrossRef] [PubMed]
- van Haastert, I.C.; de Vries, L.S.; Helders, P.J.M.; Jongmans, M.J. Early Gross Motor Development of Preterm Infants According to the Alberta Infant Motor Scale. J. Pediatr. 2006, 149, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Dusing, S.C.; Kyvelidou, A.; Mercer, V.S.; Stergiou, N. Infants Born Preterm Exhibit Different Patterns of Center-of-Pressure Movement Than Infants Born at Full Term. Phys. Ther. 2009, 89, 1354–1362. [Google Scholar] [CrossRef] [Green Version]
- Baumann, N.; Bartmann, P.; Wolke, D. Health-Related Quality of Life into Adulthood after Very Preterm Birth. Pediatrics 2016, 137, e20153148. [Google Scholar] [CrossRef] [Green Version]
- Lobo, M.A.; Harbourne, R.T.; Dusing, S.C.; McCoy, S.W. Grounding Early Intervention: Physical Therapy Cannot Just Be About Motor Skills Anymore. Phys. Ther. 2013, 93, 94–103. [Google Scholar] [CrossRef]
- Dusing, S.C.; Tripathi, T.; Marcinowski, E.C.; Thacker, L.R.; Brown, L.F.; Hendricks-muñoz, K.D. Supporting Play Exploration and Early Developmental Intervention versus Usual Care to Enhance Development Outcomes during the Transition from the Neonatal Intensive Care Unit to Home: A Pilot Randomized Controlled Trial. BMC Pediatr. 2018, 18, 46. [Google Scholar] [CrossRef]
- Puthussery, S.; Chutiyami, M.; Tseng, P.; Kilby, L.; Kapadia, J. Effectiveness of Early Intervention Programs for Parents of Preterm Infants: A Meta-Review of Systematic Reviews. BMC Pediatr. 2018, 18, 223. [Google Scholar] [CrossRef] [Green Version]
- Muller-Nix, C.; Forcada-Guex, M.; Pierrehumbert, B.; Jaunin, L.; Borghini, A.; Nasermet, F. Prematurity, Maternal Stress and Mother-Child Interactions. Early Hum. Dev. 2004, 79, 145–158. [Google Scholar] [CrossRef] [PubMed]
- Benzies, K.M.; Magill-Evans, J.E.; Hayden, K.A.; Ballantyne, M. Key Components of Early Intervention Programs for Preterm Infants and Their Parents: A Systematic Review and Meta-Analysis. BMC Pregnancy Childbirth 2013, 13, S10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Håkstad, R.B.; Obstfelder, A.; Øberg, G.K. Parents’ Perceptions of Primary Health Care Physiotherapy with Preterm Infants: Normalization, Clarity, and Trust. Qual. Health Res. 2016, 26, 1341–1350. [Google Scholar] [CrossRef] [PubMed]
- Al Maghaireh, D.F.; Abdullah, K.L.; Chan, C.M.; Piaw, C.Y.; Al Kawafha, M.M. Systematic Review of Qualitative Studies Exploring Parental Experiences in the Neonatal Intensive Care Unit. J. Clin. Nurs. 2016, 25, 2745–2756. [Google Scholar] [CrossRef] [PubMed]
- Øberg, G.K.; Ustad, T.; Jørgensen, L.; Kaaresen, P.I.; Labori, C.; Girolami, G.L. Parents’ Perceptions of Administering a Motor Intervention with Their Preterm Infant in the NICU. Eur. J. Physiother. 2018, 21, 134–141. [Google Scholar] [CrossRef]
- Ochandorena-Acha, M.; Noell-Boix, R.; Yildirim, M.; Iriondo-Sanz, M.; Troyano-Martos, M.J.; Casas-Baroy, J.C. Experiences and Coping Strategies of Preterm Infants’ Parents and Parental Competences after Early Physiotherapy Intervention: Qualitative Study. Physiother. Theory Pract. 2020, 1–14. [Google Scholar] [CrossRef]
- Spittle, A.; Treyvaud, K.; Hons, B. The Role of Early Developmental Intervention to Influence Neurobehavioral Outcomes of Children Born Preterm. Semin. Perinatol. 2016, 40, 542–548. [Google Scholar] [CrossRef]
- Khurana, S.; Kane, A.E.; Brown, S.E.; Tarver, T.; Dusing, S.C. Effect of Neonatal Therapy on the Motor, Cognitive, and Behavioral Development of Infants Born Preterm: A Systematic Review. Dev. Med. Child Neurol. 2020, 62, 684–692. [Google Scholar] [CrossRef]
- Schwarz, D.F.; O’Sullivan, A.L.; Guinn, J.; Mautone, J.A.; Carlson, E.C.; Zhao, H.; Zhang, X.; Esposito, T.L.; Askew, M.; Radcliffe, J. Promoting Early Intervention Referral Through a Randomized Controlled Home-Visiting Program. J. Early Interv. 2012, 34, 20–39. [Google Scholar] [CrossRef]
- Spittle, A.J.; Anderson, P.J.; Lee, K.J.; Ferretti, C.; Eeles, A.; Orton, J.; Boyd, R.N.; Inder, T.; Doyle, L.W. Preventive Care at Home for Very Preterm Infants Improves Infant and Caregiver Outcomes at 2 Years. Pediatrics 2010, 126, e171–e178. [Google Scholar] [CrossRef]
- Hughes, A.J.; Redsell, S.A.; Glazebrook, C. Motor Development Interventions for Preterm Infants: A Systematic Review and Meta-Analysis. Pediatrics 2016, 138, e20160147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spittle, A.; Orton, J.; Anderson, P.; Boyd, R.; Doyle, L.W. Early Developmental Intervention Programmes Post-Hospital Discharge to Prevent Motor and Cognitive Impairments in Preterm Infants. Cochrane Database Syst. Rev. 2015, 11, CD005495. [Google Scholar] [CrossRef] [PubMed]
- Guralnick, M.J. Preventive Interventions for Preterm Children: Effectiveness and Developmental Mechanisms. J. Dev. Behav. Pediatr. 2012, 33, 352–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Procianoy, R.S.; Mendes, E.W.; Silveira, R.C. Massage Therapy Improves Neurodevelopment Outcome at Two Years Corrected Age for Very Low Birth Weight Infants. Early Hum. Dev. 2010, 86, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Nordhov, S.M.; Ronning, J.A.; Dahl, L.B.; Ulvund, S.E.; Tunby, J.; Kaaresen, P.I. Early Intervention Improves Cognitive Outcomes for Preterm Infants: Randomized Controlled Trial. Pediatrics 2010, 126, e1088-94. [Google Scholar] [CrossRef] [PubMed]
- Kynø, N.M.; Ravn, I.H.; Lindemann, R.; Fagerland, M.W.; Smeby, N.A.; Torgersen, A.M. Effect of an Early Intervention Programme on Development of Moderate and Late Preterm Infants at 36 Months: A Randomized Controlled Study. Infant Behav. Dev. 2012, 35, 916–926. [Google Scholar] [CrossRef]
- Kanagasabai, P.S.; Mohan, D.; Lewis, L.E.; Kamath, A.; Rao, B.K. Effect of Multisensory Stimulation on Neuromotor Development in Preterm Infants. Indian J. Pediatr. 2013, 80, 460–464. [Google Scholar] [CrossRef]
- Fucile, S.; Gisel, E.G. Sensorimotor Interventions Improve Growth and Motor Function in Preterm Infants. Neonatal Netw. 2010, 29, 359–366. [Google Scholar] [CrossRef]
- Ustad, T.; Evensen, K.A.I.; Campbell, S.K.; Girolami, G.L.; Helbostad, J.; Jorgensen, L.; Kaaresen, P.I.; Oberg, G.K. Early Parent-Administered Physical Therapy for Preterm Infants: A Randomized Controlled Trial. Pediatrics 2016, 138, e20160271. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.-C.; Leng, C.-H.; Hsieh, W.-S.; Hsu, C.-H.; Chen, W.J.; Gau, S.S.-F.; Chiu, N.-C.; Yang, M.-C.; Fang, L.-J.; Hsu, H.-C.; et al. A Randomized Controlled Trial of Clinic-Based and Home-Based Interventinos in Comparison with Usual Care for Preterm Infants: Effects and Mediators. Res. Dev. Disabil. 2014, 35, 2384–2393. [Google Scholar] [CrossRef]
- Cameron, E.C.; Maehle, V.; Reid, J. The Effects of an Early Physical Therapy Intervention for Very Preterm, Very Low Birth Weight Infants: A Randomized Controlled Clinical Trial. Pediatr. Phys. Ther. 2005, 17, 107–119. [Google Scholar] [CrossRef] [PubMed]
- Lekskulchai, R.; Cole, J. Effect of a Developmental Program on Motor Performance in Infants Born Preterm. Aust. J. Physiother. 2001, 47, 169–176. [Google Scholar] [CrossRef] [Green Version]
- Jeong, J.; Pitchik, H.O.; Fink, G. Short-Term, Medium-Term and Long-Term Effects of Early Parenting Interventions in Low-and Middle-Income Countries: A Systematic Review. BMJ Glob. Health 2021, 6, e004067. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. BMJ 2010, 340, 698–702. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association (WMA). WMA Declaration Of Helsinki—Ethical Principles for Scientic Requirements and Research Protocols; World Medical Association: Ferney-Voltaire, France, 2013; pp. 29–32. [Google Scholar]
- Morales-Monforte, E.; Bagur-Calafat, C.; Suc-Lerin, N.; Fornaguera-Martí, M.; Cazorla-Sánchez, E.; Girabent-Farrés, M. The Spanish Version of the Alberta Infant Motor Scale: Validity and Reliability Analysis. Dev. Neurorehabilit. 2017, 20, 76–82. [Google Scholar] [CrossRef]
- Heathcock, J.C.; Lobo, M.; Galloway, J.C. Movement Training Advances the Emergence of Reaching in Infants Born at Less than 33 Weeks of Gestational Age: A Randomized Clinical Trial. Phys. Ther. 2008, 88, 310–322. [Google Scholar] [CrossRef] [Green Version]
- Marrugat, J.; Vila, J.; Pavesi, M.; Sanz, F. Estimation of the Sample Size in Clinical and Epidemiological Investigations. Med. Clin. 1998, 111, 267–276. [Google Scholar]
- Vanderveen, J.; Bassler, D.; Robertson, C.; Kirpalani, H. Early Interventions Involving Parents to Improve Neurodevelopmental Outcomes of Premature Infants: A Meta-Analysis. J. Perinatol. 2009, 29, 343–351. [Google Scholar] [CrossRef] [Green Version]
- de Albuquerque, P.L.; de Farias Guerra, M.Q.; de Carvalho Lima, M.; Eickmann, S.H. Concurrent Validity of the Alberta Infant Motor Scale to Detect Delayed Gross Motor Development in Preterm Infants: A Comparative Study with the Bayley III. Dev. Neurorehabilit. 2017, 21, 408–414. [Google Scholar] [CrossRef]
- Sarmiento Camposa, J.A.; Squires, J.; Ponte, J. Universal Developmental Screening: Preliminary Studies in Galicia, Spain. Early Child Dev. Care 2011, 181, 475–485. [Google Scholar] [CrossRef]
- van Heerden, A.; Hsiao, C.; Matafwali, B.; Louw, J.; Richter, L. Support for the Feasibility of the Ages and Stages Questionnaire as a Developmental Screening Tool: A Cross-Sectional Study of South African and Zambian Children Aged 2–60 Months. BMC Pediatr. 2017, 17, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, P.K.; Shi, L.; Daniel, L.M.; Yang, P.H.; Khoo, P.C.; Quek, B.H.; Zheng, Q.; Rajadurai, V.S. Prospective Evaluation of the Ages and Stages Questionnaire 3rd Edition in Very-Low-Birthweight Infants. Dev. Med. Child Neurol. 2017, 59, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Squires, J.; Bricker, D.; Potter, L.W. Revision of a Parent-Completed Developmental Screening Tool: Ages and Stages Questionnaires. J. Pediatr. Psychol. 1997, 22, 313–328. [Google Scholar] [CrossRef] [PubMed]
- Otalvaro, A.M.R.; Grañana, N.; Gaeto, N.; Torres, M.D.L.Á.; Zamblera, M.N.; Vasconez, M.A.; Squires, J. ASQ-3: Validation of the Ages and Stages Questionnaire for the Detection of Neurodevelopmental Disorders in Argentine Children. Arch. Argent. Pediatr. 2018, 116, 7–13. [Google Scholar] [CrossRef]
- Schonhaut, L.; Armijo, I.; Schonstedt, M.; Alvarez, J.; Cordero, M. Validity of the Ages and Stages Questionnaires in Term and Preterm Infants. Pediatrics 2013, 131, e1468–e1474. [Google Scholar] [CrossRef] [Green Version]
- Singh, A.; Yeh, C.J.; Boone Blanchard, S. Ages and Stages Questionnaire: A Global Screening Scale. Boletín Médico Hosp. Infant. México 2017, 74, 5–12. [Google Scholar] [CrossRef]
- Pérez-Padilla, J.; Menéndez, S.; Lozano, O. Validity of the Parenting Stress Index Short Form in a Sample of At-Risk Mothers. Eval. Rev. 2015, 39, 428–446. [Google Scholar] [CrossRef]
- Díaz-Herrero, Á.; López-Pina, J.A.; Pérez-López, J.; de la Nuez, A.G.B.; Martínez-Fuentes, M.T. Validity of the Parenting Stress Index-Short Form in a Sample of Spanish Fathers. Span. J. Psychol. 2011, 14, 990–997. [Google Scholar] [CrossRef]
- Díaz-Herrero, Á.; Brito de la Nuez, A.G.; López Pina, J.A.; Pérez-López, J.; Martínez-Fuentes, M.T. Estructura Factorial y Consistencia Interna de La Versión Española Del Parenting Stress Index-Short Form. Psicothema 2010, 22, 1033–1038. [Google Scholar]
- Barton, B.; Peat, J. Medical Statistics. A Guide to SPSS, Data Analysis and Critical Appraisal; John Wiley & Sons: Hoboken, NJ, USA, 2014. [Google Scholar]
- Cohen, J. The Earth Is Round! Am. Psychol. 1994, 49, 997–1003. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using SPSS, 2nd ed.; Sage Publications: London, UK, 2005; ISBN 0-7619-4452-4. [Google Scholar]
- Øberg, G.K.; Girolami, G.L.; Campbell, S.K.; Ustad, T.; Heuch, I.; Jacobsen, B.K.; Kaaresen, P.I.; Aulie, V.S.; Jørgensen, L. Effects of a Parent-Administered Exercise Program in the Neonatal Intensive Care Unit: Dose Does Matter—A Randomized Controlled Trial. Phys. Ther. 2020, 100, 860–869. [Google Scholar] [CrossRef] [PubMed]
- Spittle, A.J.; Treyvaud, K.; Lee, K.J.; Anderson, P.J.; Doyle, L.W. The Role of Social Risk in an Early Preventative Care Programme for Infants Born Very Preterm: A Randomized Controlled Trial. Dev. Med. Child Neurol. 2018, 60, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Ismail, F.Y.; Fatemi, A.; Johnston, M.V. Cerebral Plasticity: Windows of Opportunity in the Developing Brain. Eur. J. Paediatr. Neurol. 2017, 21, 23–48. [Google Scholar] [CrossRef] [PubMed]
- Belsky, J.; de Haan, M. Annual Research Review: Parenting and Children’s Brain Development: The End of the Beginning. J. Child Psychol. Psychiatry Allied Discip. 2011, 52, 409–428. [Google Scholar] [CrossRef] [PubMed]
- Orton, J.; Spittle, A.; Doyle, L.; Anderson, P.; Boyd, R. Do Early Intervention Programmes Improve Cognitive and Motor Outcomes for Preterm Infants after Discharge? A Systematic Review. Dev. Med. Child Neurol. 2009, 51, 851–859. [Google Scholar] [CrossRef] [PubMed]
- Medina-Mirapeix, F.; Lillo-Navarro, C.; Montilla-Herrador, J.; Gacto-Sánchez, M.; Franco-Sierra, M.A.; Escolar-Reina, P. Predictors of Parents’ Adherence to Home Exercise Programs for Children with Developmental Disabilities, Regarding Both Exercise Frequency and Duration: A Survey Design. Eur. J. Phys. Rehabil. Med. 2017, 53, 545–555. [Google Scholar] [CrossRef]
- Santer, M.; Ring, N.; Yardley, L.; Geraghty, A.W.A.; Wyke, S. Treatment Non-Adherence in Pediatric Long-Term Medical Conditions: Systematic Review and Synthesis of Qualitative Studies of Caregivers’ Views. BMC Pediatr. 2014, 14, 63. [Google Scholar] [CrossRef]
- McConnell, D.; Parakkal, M.; Savage, A.; Rempel, G. Parent-Mediated Intervention: Adherence and Adverse Effects. Disabil. Rehabil. 2015, 37, 864–872. [Google Scholar] [CrossRef]
- Lillo-Navarro, C.; Medina-Mirapeix, F.; Escolar-Reina, P.; Montilla-Herrador, J.; Gomez-Arnaldos, F.; Oliveira-Sousa, S.L. Parents of Children with Physical Disabilities Perceive That Characteristics of Home Exercise Programs and Physiotherapists’ Teaching Styles Influence Adherence: A Qualitative Study. J. Physiother. 2015, 61, 81–86. [Google Scholar] [CrossRef] [Green Version]
- Mobbs, C.; Spittle, A.; Johnston, L. PreEMPT (Preterm Infant Early Intervention for Movement and Participation Trial): Feasibility Outcomes of a Randomised Controlled Trial. Early Hum. Dev. 2022, 166, 105551. [Google Scholar] [CrossRef]
- Roué, J.M.; Kuhn, P.; Maestro, M.L.; Maastrup, R.A.; Mitanchez, D.; Westrup, B.; Sizun, J. Eight Principles for Patient-Centred and Family-Centred Care for Newborns in the Neonatal Intensive Care Unit. Arch. Dis. Child. -Fetal Neonatal Ed. 2017, 102, F364–F368. [Google Scholar] [CrossRef] [PubMed]
- Landsem, I.P.; Handegård, B.H.; Tunby, J.; Ulvund, S.E.; Rønning, J.A. Early Intervention Program Reduces Stress in Parents of Preterms during Childhood, a Randomized Controlled Trial. Trials 2014, 15, 387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaaresen, P.I.; Ronning, J.A.; Ulvund, S.E.; Dahl, L.B.; Rønning, J.A.; Ulvund, S.E.; Dahl, L.B. A Randomized, Controlled Trial of the Effectiveness of an Early-Intervention Program in Reducing Parenting Stress After Preterm Birth. Pediatrics 2006, 118, e9–e19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newnham, C.A.; Milgrom, J.; Skouteris, H. Effectiveness of a Modified Mother-Infant Transaction Program on Outcomes for Preterm Infants from 3 to 24 Months of Age. Infant Behav. Dev. 2009, 32, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Johnston, M.V. Plasticity in the Developing Brain: Implications for Rehabilitation. Dev. Disabil. Res. Rev. 2009, 15, 94–101. [Google Scholar] [CrossRef]
- Chen, R.; Cohen, L.G.; Hallett, M. Nervous System Reorganization Following Injury. Neuroscience 2002, 111, 761–773. [Google Scholar] [CrossRef]
- Duncan, A.F.; Matthews, M.A. Neurodevelopmental Outcomes in Early Childhood. Clin. Perinatol. 2018, 45, 377–392. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Children Characteristics | IG (n = 24) | CG (n = 24) | p-Value |
|---|---|---|---|
| Gestational age at birth, M (SD) (weeks) | 31.84 (1.82) | 32.05 (1.59) | 0.675 a |
| Prematurity classification, n (%) | |||
| Moderate premature 32 < 34 | 13 (48.1) | 14 (51.9) | 0.771 c |
| Very premature 28 < 32 | 11 (52.4) | 10 (47.6) | |
| Intrauterine growth restriction, n (%) | 4 (16.7) | 6 (25.0) | 0.724 b |
| Birth weight, M (DE) (g) | 1462.46 (437.27) | 1590.79 (331.21) | 0.258 a |
| Cranial circumference at birth, M (SD) (cm) | 27.75 (2.61) | 28.48 (1.51) | 0.247 a |
| Gender, n (%) | |||
| Girls | 12 (50.0) | 8 (33.3) | 0.242 c |
| Boys | 12 (50.0) | 16 (66.7) | |
| Twins, n (%) | 8 (33.3) | 8 (33.3) | 1.000 c |
| Cesarean birth, n (%) | 14 (58.3) | 12 (50.0) | 0.562 c |
| Assisted reproduction, n (%) | 9 (37.5) | 5 (20.8) | 0.204 c |
| Antibiotic therapy, n (%) | |||
| Yes | 10 (41.7) | 8 (33.3) | 0.551 c |
| No | 14 (58.3) | 16 (66.7) | |
| Oxygen therapy, n (%) | |||
| Yes | 4 (16.7) | 4 (16.7) | 1.000 b |
| No | 20 (83.3) | 20 (83.3) | |
| Jaundice with phototherapy, n (%) | |||
| Yes | 17 (70.8) | 17 (70.8) | 1.000 c |
| No | 7 (29.2) | 7 (29.2) | |
| Caffeine, n (%) | |||
| Yes | 13 (54.2) | 14 (58.3) | 0.771 c |
| No | 11 (45.8) | 10 (41.7) | |
| Hospital admission days, M (SD) | 37.00 (19.12) | 32.25 (17.04) | 0.368 a |
| Weight at hospital discharge, M (SD) (g) | 2086.67 (283.05) | 2096.46 (236.83) | 0.897 a |
| Cranial circumference at discharge, M (SD) (cm) | 32.42 (3.91) | 31.38 (1.24) | 0.224 a |
| Mother Characteristics | IG (n = 20) | CG (n = 20) | p-Value |
|---|---|---|---|
| Age, M (DE) (years) | 33.80 (5.95) | 32.20 (6.26) | 0.413 a |
| Education level, n (%) | |||
| Primary | 1 (5.0) | 2 (10.0) | 0.160 b |
| High school | 2 (10.0) | 7 (35.0) | |
| Medium | 11 (55.0) | 6 (30.0) | |
| Undergraduate | 6 (30.0) | 5 (25.0) | |
| Father characteristics | IG (n = 20) | CG (n = 19) | pvalue |
| Age, M (DE) (years) | 33.40 (4.83) | 33.74 (7.24) | 0.866 a |
| Education level, n (%) | |||
| Primary | 0 (0.0) | 1 (5.3) | 0.259 b |
| High school | 3 (15.0) | 3 (15.8) | |
| Medium | 11 (55.0) | 12 (63.2) | |
| Undergraduate | 6 (30.0) | 3 (15.8) |
| AIMS | 2 Months Corrected Age | 8 Months Corrected Age | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| IG (n = 20) | CG (n = 22) | p-Value a | Z Mann Whitney | Effect Size b | IG (n = 20) | CG (n = 21) | p-Value a | Z Mann Whitney | Effect Size b | |
| Prone, M (SD) | 2.30 (1.13) | 2.73 (0.99) | 0.121 | −1.550 | −0.239 | 12.30 (4.04) | 12.33 (3.53) | 0.875 | −0.157 | −0.025 |
| Supine, M (SD) | 3.15 (0.37) | 3.36 (0.58) | 0.190 | −1.310 | −0.202 | 7.30 (1.42) | 7.29 (1.42) | 0.989 | −0.013 | −0.002 |
| Sitting, M (SD) | 1.05 (0.22) | 1.05 (0.38) | 0.980 | −0.025 | −0.004 | 7.55 (2.95) | 8.76 (2.05) | 0.230 | −1.201 | −0.188 |
| Standing positions, M (SD) | 1.25 (0.64) | 1.55 (0.60) | 0.118 | −1.563 | −0.241 | 3.10 (0.97) | 3.67 (1.02) | 0.063 | −2.921 | −0.456 |
| Total score, M (SD) | 7.80 (1.20) | 8.55 (1.50) | 0.073 | −1.793 | −0.277 | 30.25 (7.15) | 32.10 (6.83) | 0.396 | −1.045 | −0.163 |
| ASQ-3 | 1 Month Corrected Age | 8 Months Corrected Age | ||||||||
| IG (n = 20) | CG (n = 23) | pValue a | Z Mann Whitney | Effect Size b | IG (n = 20) | CG (n = 23) | pValue a | Z Mann Whitney | Effect Size b | |
| Gross Motor, M (SD) | 50.00 (5.85) | 49.13 (7.18) | 0.830 | −0.215 | −0.033 | 38.25 (14.63) | 41.09 (13.73) | 0.532 | −0.625 | −0.095 |
| Fine Motor, M (SD) | 53.50 (5.16) | 42.17 (8.64) | 0.000 | −4.202 | −0.641 | 55.50 (6.05) | 54.78 (5.93) | 0.517 | −0.648 | −0.099 |
| Problem Solving, M (SD) | 49.25 (7.83) | 37.39 (14.91) | 0.006 | −2.725 | −0.416 | 52.50 (7.69) | 55.00 (5.22) | 0.351 | −0.932 | −0.142 |
| Personal-Social, M (SD) | 46.25 (5.10) | 41.96 (6.70) | 0.049 | −1.972 | −0.301 | 47.00 (11.17) | 50.87 (8.61) | 0.263 | −1.120 | −0.171 |
| Communication, M (SD) | 38.00 (12.61) | 26.52 (13.52) | 0.006 | −2.740 | −0.418 | 51.00 (9.40) | 51.30 (7.10) | 0.870 | −0.163 | 0.025 |
| ASQ-3 at 1 Month Corrected Age | IG (n = 20) | CG (n = 23) | p-Value a |
|---|---|---|---|
| Gross Motor, n (%) | 0.588 | ||
| High-risk | 2 (10.0) | 4 (17.4) | |
| Follow-up | 4 (20.0) | 4 (17.4) | |
| Correct | 14 (70.0) | 15 (65.2) | |
| Fine Motor, n (%) | 0.003 | ||
| High-risk | 0 (0) | 4 (17.4) | |
| Follow-up | 1 (5.0) | 7 (30.4) | |
| Correct | 19 (95.0) | 12 (52.2) | |
| Problem Solving, n (%) | 0.004 | ||
| High-risk | 0 (0) | 6 (26.1) | |
| Follow-up | 1 (5.0) | 4 (17.4) | |
| Correct | 19 (95.0) | 13 (56.5) | |
| Personal-Social, n (%) | 0.079 | ||
| High-risk | 0 (0) | 2 (8.7) | |
| Follow-up | 5 (25.0) | 9 (39.1) | |
| Correct | 15 (75.0) | 12 (52.2) | |
| Communication, n (%) | 0.003 | ||
| High-risk | 2 (10.0) | 9 (39.1) | |
| Follow-up | 6 (30.0) | 10 (43.5) | |
| Correct | 12 (60.0) | 4 (17.4) |
| Parenting Stress Index (PSI-SF) | IG (n = 16) | CG (n = 19) | p-Value a | Size Effect b |
|---|---|---|---|---|
| Parental Distress, M (SD) | 26.38 (10.51) | 27.05 (8.46) | 0.834 | 0.07 |
| Parent–Child Dysfunctional Interaction, M (SD) | 19.69 (5.63) | 18.84 (4.63) | 0.629 | 0.16 |
| Difficult Child, M (SD) | 21.75 (7.79) | 21.21 (5.35) | 0.810 | 0.08 |
| Total Stress, M (SD) | 68.31 (21.94) | 67.11 (16.24) | 0.853 | 0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ochandorena-Acha, M.; Terradas-Monllor, M.; López Sala, L.; Cazorla Sánchez, M.E.; Fornaguera Marti, M.; Muñoz Pérez, I.; Agut-Quijano, T.; Iriondo, M.; Casas-Baroy, J.C. Early Physiotherapy Intervention Program for Preterm Infants and Parents: A Randomized, Single-Blind Clinical Trial. Children 2022, 9, 895. https://doi.org/10.3390/children9060895
Ochandorena-Acha M, Terradas-Monllor M, López Sala L, Cazorla Sánchez ME, Fornaguera Marti M, Muñoz Pérez I, Agut-Quijano T, Iriondo M, Casas-Baroy JC. Early Physiotherapy Intervention Program for Preterm Infants and Parents: A Randomized, Single-Blind Clinical Trial. Children. 2022; 9(6):895. https://doi.org/10.3390/children9060895
Chicago/Turabian StyleOchandorena-Acha, Mirari, Marc Terradas-Monllor, Laura López Sala, Maria Engracia Cazorla Sánchez, Montserrat Fornaguera Marti, Isabel Muñoz Pérez, Thais Agut-Quijano, Martín Iriondo, and Joan Carles Casas-Baroy. 2022. "Early Physiotherapy Intervention Program for Preterm Infants and Parents: A Randomized, Single-Blind Clinical Trial" Children 9, no. 6: 895. https://doi.org/10.3390/children9060895