
Use of Self-Figure Drawing as an Assessment Tool for Child Abuse: Differentiating between Sexual, Physical, and Emotional Abuse


Abstract
:1. Introduction
1.1. Childhood Sexual Abuse (CSA)
1.2. Child Physical Abuse (CPA)
1.3. Child Emotional Abuse (CEA)
1.4. Multi-Type Abuse
1.5. Child Abuse and Brain
1.6. Disclosure of Child Abuse
1.7. Self-Figure Drawing as an Assessment Tool
1.8. Thai Culture
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.2.1. Demographic Questionnaire
2.2.2. Childhood Trauma Questionnaire (CTQ)
2.2.3. The Medical Somatic Dissociation Questionnaire (MSDQ)
2.2.4. The Disclosure of Trauma Questionnaire (DTQ)
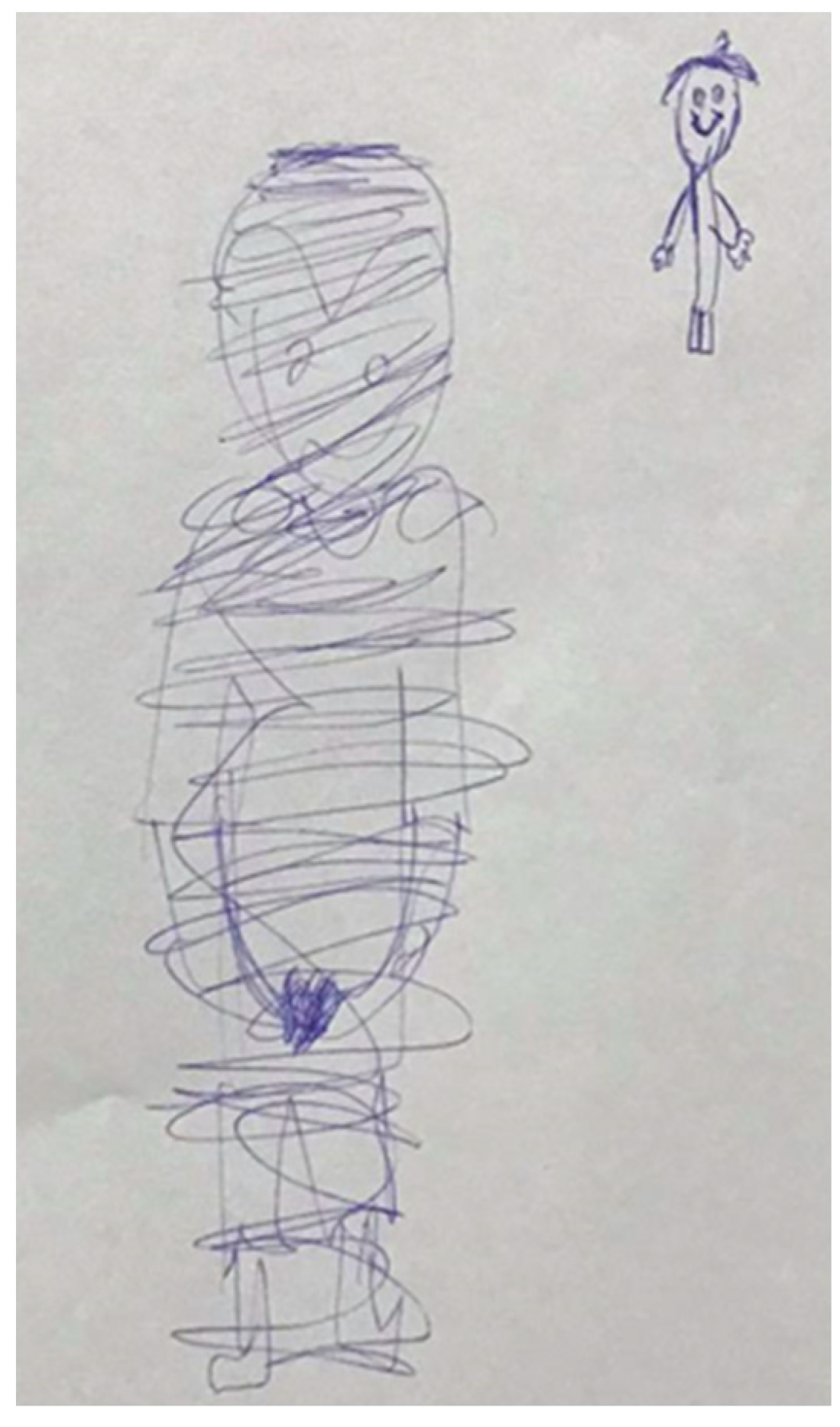
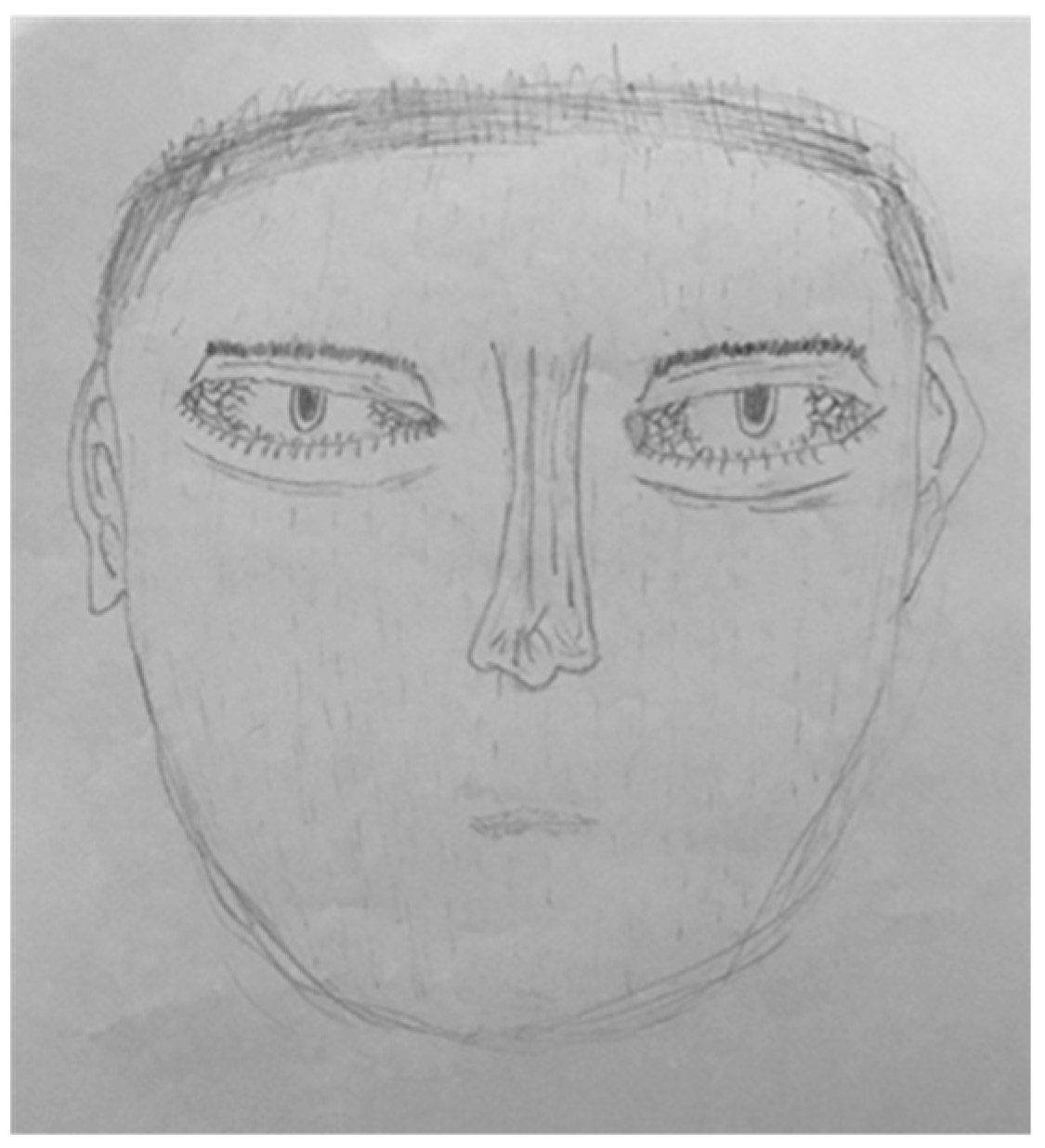
2.2.5. The Draw Yourself Test
2.3. Data Analysis
3. Results
3.1. Characterizing Drawing Indicators and Demographical Differences by Groups of Abuse
3.2. Correlation of Drawing Indicators and CTQ, MSDQ, and DTQ Scales for All the Sample
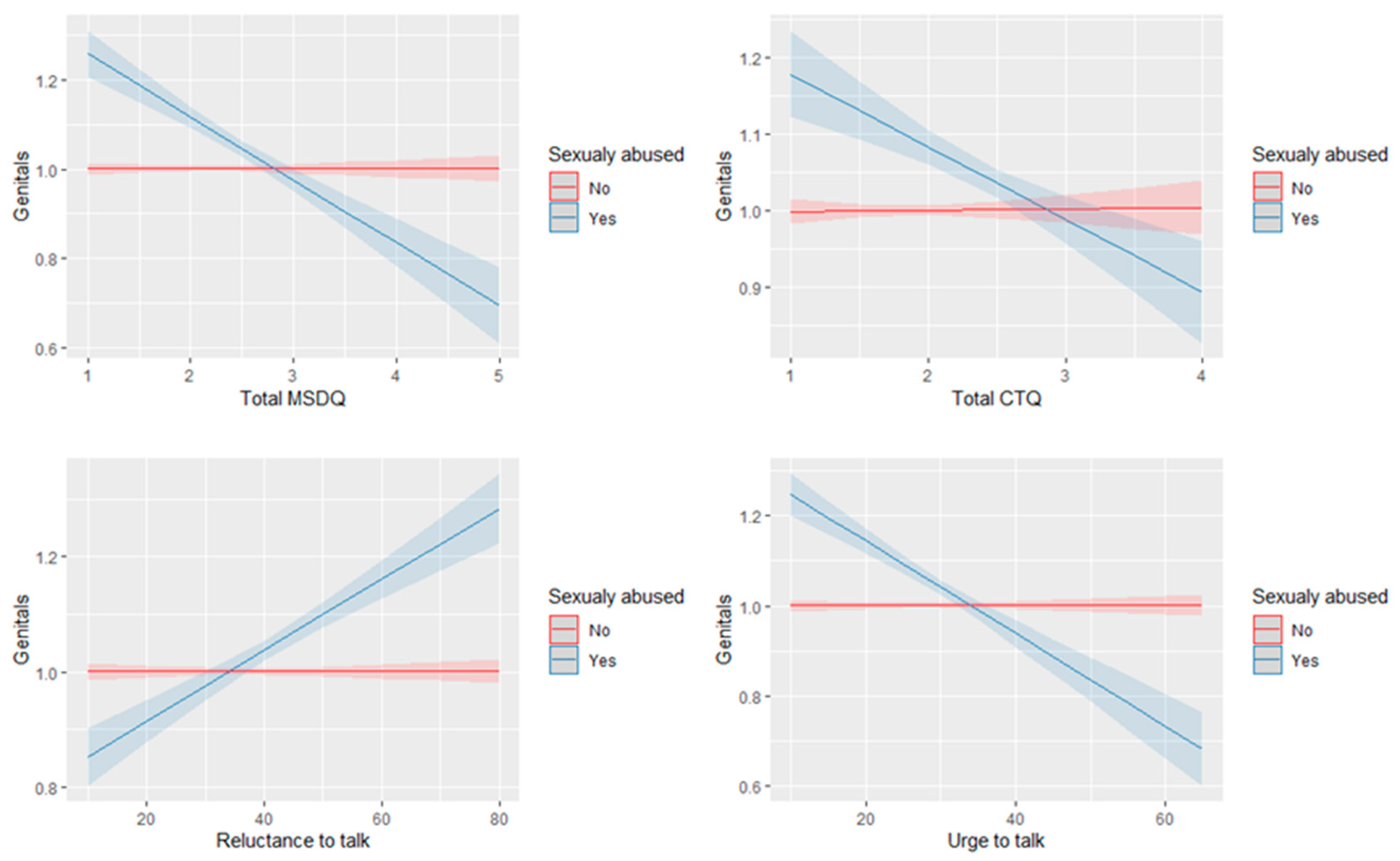
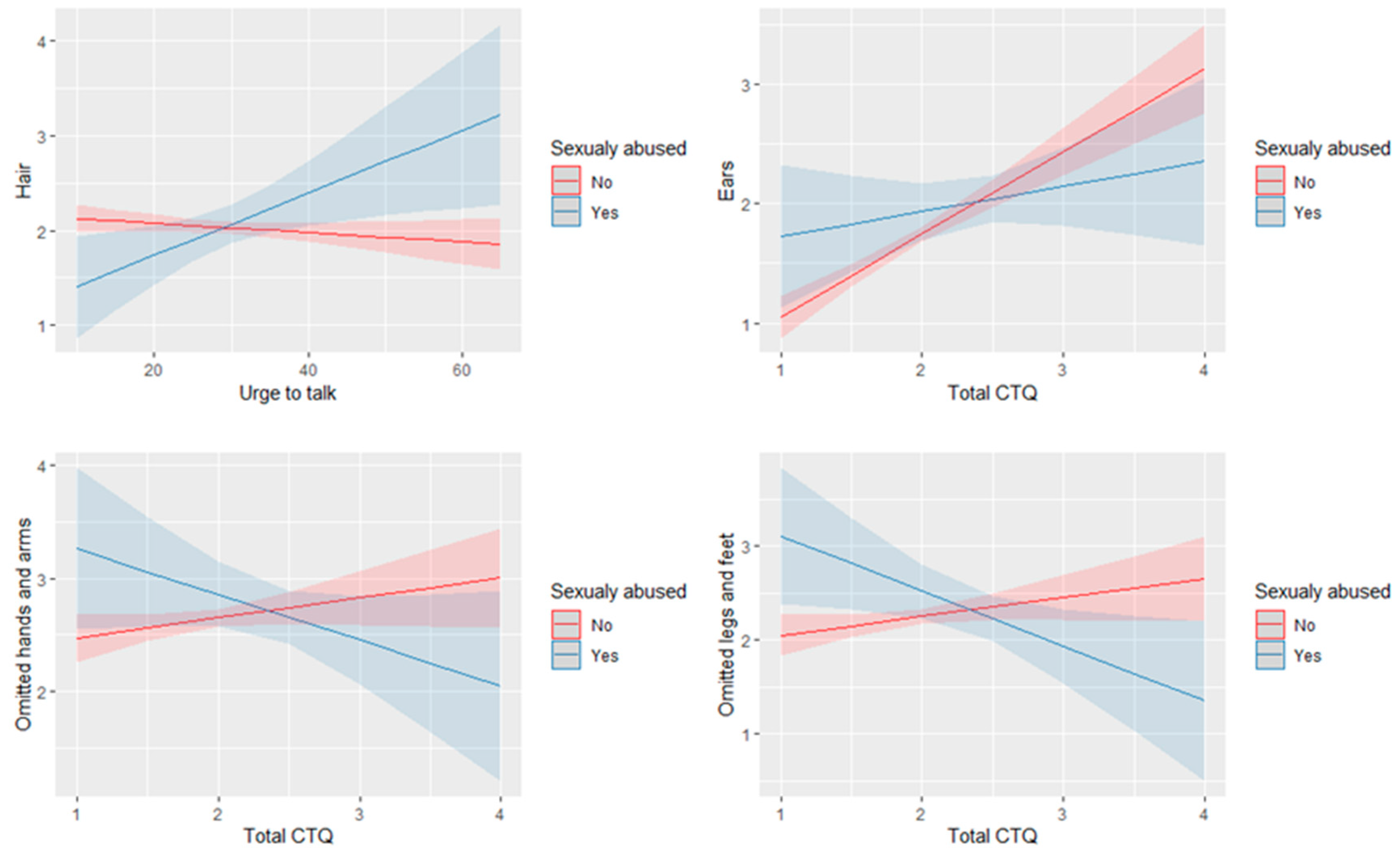
3.3. Experiencing CSA as Moderator of the Relation between CTQ, MSDQ, and DTQ Scales and Drawing Indicators
3.4. Experiencing CSA Compared with Experiencing CPA as Moderator of the Relation between CTQ, MSDQ, and DTQ Scales and Drawing Indicators
3.5. Cutoff Total Scores for Sexual Abuse, N = 1707
3.6. Cutoff Total Scores for Physical Abuse Compared with Emotional Abuse, N = 1544
4. Discussion
4.1. Drawing Indicators
4.2. The Association between CTQ and MSDQ
4.3. Disclosure of Abuse
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gilbert, R.; Widom, C.S.; Browne, K.; Fergusson, D.; Webb, E.; Janson, S. Burden and Consequences of Child Maltreatment in High-Income Countries. Lancet 2009, 373, 68–81. [Google Scholar] [CrossRef]
- Lev-Wiesel, R.; First, M. Willingness to Disclose Child Maltreatment: CSA Vs Other Forms of Child Abuse in Relation to Gender. Child Abuse Negl. 2018, 79, 183–191. [Google Scholar] [CrossRef]
- Somer, E.; Szwarcberg, S. Variables in Delayed Disclosure of Childhood Sexual Abuse. Am. J. Orthopsychiatry 2001, 71, 332–341. [Google Scholar] [CrossRef]
- Higgins, D.; McCabe, M. Multi-type maltreatment and the long-term adjustment of adults. Child Abuse Rev. 2000, 9, 6–18. [Google Scholar] [CrossRef]
- Vizard, E.; Gray, J.; Bentovim, A. The impact of child maltreatment on the mental and physical health of child victims: A review of the evidence. Bjpsych Adv. 2021, 28, 60–70. [Google Scholar] [CrossRef]
- Kim, K.; Mennen, F.; Trickett, P. Patterns and correlates of co-occurrence among multiple types of child maltreatment. Child Fam. Soc. Work 2016, 22, 492–502. [Google Scholar] [CrossRef]
- Momtaz, V.; Mansor, M.; Talib, M.A.; Kahar, R.B.; Momtaz, T. Emotional Abuse Questionnaire (EAQ): A New Scale for Measuring Emotional Abuse and Psychological Maltreatment 1. Jpn. Psychol. Res. 2022, 64, 1–11. [Google Scholar] [CrossRef]
- Bottoms, B.L.; Peter-Hagene, L.C.; Epstein, M.A.; Wiley, T.R.; Reynolds, C.E.; Rudnicki, A.G. Abuse characteristics and individual differences related to disclosing childhood sexual, physical, and emotional abuse and witnessed domestic violence. J. Interpers. Violence 2014, 31, 1308–1339. [Google Scholar] [CrossRef]
- Lev-Wiesel, R.; First, M.; Gottfried, R.; Eisikovits, Z. Reluctance versus urge to disclose child maltreatment: The impact of multi-type maltreatment. J. Interpers. Violence 2016, 34, 3888–3914. [Google Scholar] [CrossRef]
- Efrati, S.; Hadanny, A.; Daphna-Tekoah, S.; Bechor, Y.; Tiberg, K.; Pik, N.; Suzin, G.; Lev-Wiesel, R. Recovery of Repressed Memories in Fibromyalgia Patients Treated with Hyperbaric Oxygen—Case Series Presentation and Suggested Bio-Psycho-Social Mechanism. Front. Psychol. 2018, 9, 848. [Google Scholar] [CrossRef]
- Lev-Wiesel, R. The use of the Machover Draw-A-Person test in detecting adult survivors of sexual abuse: A pilot study. Am. J. Art Ther. 1999, 37, 106. [Google Scholar]
- Machover, K.A. Personality Projection in the Drawing of the Human Figure: A Method of Personality Investigation; Charles C. Thomas: Springfield, IL, USA, 1949. [Google Scholar]
- Krug, E.G.; Dahlberg, L.L.; Mercy, J.A.; Zwi, A.B.; Lozano, R. World Report on Violence and Health. Available online: https://apps.who.int/iris/bitstream/handle/10665/42495/9241545615_eng.pdf?sequence=1 (accessed on 12 April 2021).
- Hailes, H.P.; Yu, R.; Danese, A.; Fazel, S. Long-Term Outcomes of Childhood Sexual Abuse: An Umbrella Review. Lancet Psychiatry 2019, 6, 830–839. [Google Scholar] [CrossRef]
- Cantón-Cortés, D.; Cortés, M.R.; Cantón, J. Pathways from Childhood Sexual Abuse to Trait Anxiety. Child Abus. Negl. 2019, 97, 104148. [Google Scholar] [CrossRef]
- Opydo-Szymaczek, J.; Jarząbek-Bielecka, G.; Kędzia, W.; Borysewicz-Lewicka, M. Child Sexual Abuse as an Etiological Factor of Overweight and Eating Disorders—Considerations for Primary Health Care Providers. Ginekol. Pol. 2018, 89, 48–54. [Google Scholar] [CrossRef]
- Hébert, M.; Amédée, L.M.; Blais, M.; Gauthier-Duchesne, A. Child Sexual Abuse among a Representative Sample of Quebec High School Students: Prevalence and Association with Mental Health Problems and Health-Risk Behaviors. Can. J. Psychiatry 2019, 64, 846–854. [Google Scholar] [CrossRef]
- Al-Shail, E.; Hassan, A.; Aldowaish, A.; Katt, H. The Cultural Reinforcers of Child Abuse. In Child Abuse and Neglect—A Multidimensional Approach; InTech: Vienna, Austria, 2012. [Google Scholar]
- Güngör, H.C. Hidden Behind Dental Trauma: Child Physical Abuse? Pesqui. Bras. Odontopediatria Clin. Integr. 2018, 18, e3869. [Google Scholar] [CrossRef]
- Ahmed Elsayed, S.M.; Hamed Frahat, N.; Khalil Ibrahim, W. Physical Abuse among Primary School Children. Egypt. J. Health Care 2020, 11, 191–204. [Google Scholar] [CrossRef]
- Dodaj, A.; Sesar, K. Consequences of Child Abuse and Neglect. Cent. Eur. J. Paediatr. 2020, 16, 168–181. [Google Scholar] [CrossRef]
- Glaser, D. How to Deal with Emotional Abuse and Neglect—Further Development of a Conceptual Framework (FRAMEA). Child Abus. Negl. 2011, 35, 866–875. [Google Scholar] [CrossRef]
- Newton, C.; Gavin, H. “My Reality Is Just Different from Yours, That Doesn’t Mean I’m Crazy.” Exploring the Impact of Childhood Emotional Abuse on Adult Emotional Adjustment. J. Aggress. Maltreat. Trauma 2018, 29, 2–21. [Google Scholar] [CrossRef]
- Li, E.T.; Carracher, E.; Bird, T. Linking Childhood Emotional Abuse and Adult Depressive Symptoms: The Role of Mentalizing Incapacity. Child Abus. Negl. 2020, 99, 104253. [Google Scholar] [CrossRef]
- Wielaard, I.; Hoyer, M.; Rhebergen, D.; Stek, M.L.; Comijs, H.C. Childhood Abuse and Late-Life Depression: Mediating Effects of Psychosocial Factors for Early- and Late-Onset Depression. Int. J. Geriatr. Psychiatry 2018, 33, 537–545. [Google Scholar] [CrossRef]
- You, D.S.; Meagher, M.W. Childhood Adversity and Pain Sensitization. Psychosom. Med. 2016, 78, 1084–1093. [Google Scholar] [CrossRef]
- Merrill, K.G.; Campbell, J.C.; Decker, M.R.; McGready, J.; Burke, V.M.; Mwansa, J.K.; Miti, S.; Frimpong, C.; Kennedy, C.E.; Denison, J.A. Prevalence of Physical and Sexual Violence and Psychological Abuse among Adolescents and Young Adults Living with HIV in Zambia. PLoS ONE 2020, 15, e0235203. [Google Scholar] [CrossRef]
- Witt, A.; Münzer, A.; Ganser, H.G.; Fegert, J.M.; Goldbeck, L.; Plener, P.L. Experience by Children and Adolescents of More than One Type of Maltreatment: Association of Different Classes of Maltreatment Profiles with Clinical Outcome Variables. Child Abus. Negl. 2016, 57, 1–11. [Google Scholar] [CrossRef]
- Mwakanyamale, A.A.; Wande, D.P.; Yizhen, Y. Multi-Type Child Maltreatment: Prevalence and Its Relationship with Self-Esteem among Secondary School Students in Tanzania. BMC Psychol. 2018, 6, 35. [Google Scholar] [CrossRef]
- Hazzard, V.M.; Bauer, K.W.; Mukherjee, B.; Miller, A.L.; Sonneville, K.R. Associations between Childhood Maltreatment Latent Classes and Eating Disorder Symptoms in a Nationally Representative Sample of Young Adults in the United States. Child Abus. Negl. 2019, 98, 104171. [Google Scholar] [CrossRef]
- Mahmood, K.S.; Hussien, H.A. Effects of Abuse and Neglect on Adolescents in Kirkuk City. Indian J. Public. Health. Res. Dev. 2020, 11, 2013–2016. [Google Scholar]
- Herrera Ortiz, A.F.; Rincón Cuenca, N.T.; Fernández Beaujon, L. Brain Changes in Magnetic Resonance Imaging Caused by Child Abuse: A Systematic Literature Review. SSRN Electron. J. 2021, 27, 27–33. [Google Scholar] [CrossRef]
- Wang, W.; Kang, L.; Zhang, N.; Guo, X.; Wang, P.; Zong, X.; Yao, L.; Bai, H.; Cheng, J.; Tu, N.; et al. The Interaction Effects of Suicidal Ideation and Childhood Abuse on Brain Structure and Function in Major Depressive Disorder Patients. J. Neural Transplant. Plast. 2021, 2021, 7088856. [Google Scholar] [CrossRef]
- Hadanny, A.; Bechor, Y.; Catalogna, M.; Daphna–Tekoah, S.; Sigal, T.; Cohenpour, M.; Lev-Wiesel, R.; Efrati, S. Hyperbaric Oxygen Therapy Can Induce Neuroplasticity and Significant Clinical Improvement in Patients Suffering from Fibromyalgia with a History of Childhood Sexual Abuse—Randomized Controlled Trial. Front. Psychol. 2018, 9, 2495. [Google Scholar] [CrossRef] [PubMed]
- Lev-Wiesel, R.; Bechor, Y.; Daphna-Tekoah, S.; Hadanny, A.; Efrati, S. Brain and Mind Integration: Childhood Sexual Abuse Survivors Experiencing Hyperbaric Oxygen Treatment and Psychotherapy Concurrently. Front. Psychol. 2018, 9, 2535. [Google Scholar] [CrossRef] [PubMed]
- Kate, M.-A.; Jamieson, G.; Middleton, W. Childhood Sexual, Emotional, and Physical Abuse as Predictors of Dissociation in Adulthood. J. Child Sex. Abuse 2021, 30, 953–976. [Google Scholar] [CrossRef] [PubMed]
- Daphna-Tekoah, S.; Lev-Wiesel, R.; Israeli, D.; Balla, U. A Novel Screening Tool for Assessing Child Abuse: The Medical Somatic Dissociation Questionnaire–MSDQ. J. Child Sex. Abuse 2019, 28, 526–543. [Google Scholar] [CrossRef]
- Rosenblum, S. Handwriting Measures as Reflectors of Executive Functions among Adults with Developmental Coordination Disorders (DCD). Front. Psychol. 2013, 4, 357. [Google Scholar] [CrossRef]
- Fan, J.E.; Wammes, J.D.; Gunn, J.B.; Yamins, D.L.; Norman, K.A.; Turk-Browne, N.B. Relating Visual Production and Recognition of Objects in Human Visual Cortex. J. Neurosci. Res. 2019, 40, 1710–1721. [Google Scholar] [CrossRef]
- Chen, Q.; Beaty, R.E.; Qiu, J. Mapping the Artistic Brain: Common and Distinct Neural Activations Associated with Musical, Drawing, and Literary Creativity. Hum. Brain Mapp. 2020, 41, 3403–3419. [Google Scholar] [CrossRef]
- Schiferl, E.I. Both Sides Now: Visualizing and Drawing with the Right and Left Hemispheres of the Brain. Stud. Art Educ. 2008, 50, 67–82. [Google Scholar] [CrossRef]
- Refaie, E.E.L.; Payson, A.; Bliesemann de Guevara, B.; Gameiro, S. Pictorial and Spatial Metaphor in the Drawings of a Culturally Diverse Group of Women with Fertility Problems. Vis. Commun. 2018, 19, 257–280. [Google Scholar] [CrossRef]
- Ullman, S.E. Social Reactions to Child Sexual Abuse Disclosures: A Critical Review. J. Child Sex. Abus. 2002, 12, 89–121. [Google Scholar] [CrossRef]
- Lovett, B.B. Child Sexual Abuse Disclosure: Maternal Response and Other Variables Impacting the Victim. Child Adolesc. Soc. Work J. 2004, 21, 355–371. [Google Scholar] [CrossRef]
- Foynes, M.M.; Freyd, J.J.; DePrince, A.P. Child Abuse: Betrayal and Disclosure. Child Abus. Negl. 2009, 33, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Collin-Vézina, D.; Daigneault, I.; Hébert, M. Lessons Learned from Child Sexual Abuse Research: Prevalence, Outcomes, and Preventive Strategies. Child Adolesc. Psychiatry Ment. Health 2013, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Lahtinen, H.-M.; Laitila, A.; Korkman, J.; Ellonen, N.; Honkalampi, K. Children’s Disclosures of Physical Abuse in a Population-Based Sample. J. Interpers. Violence 2020, 37, 2011–2036. [Google Scholar] [CrossRef]
- McGuire, K.; London, K. A Retrospective Approach to Examining Child Abuse Disclosure. Child Abuse Negl. 2020, 99, 104263. [Google Scholar] [CrossRef]
- Zadeh, Z.F.; Malik, S.M. Expression of Aggressive Tendencies in the Drawings of Children and Youth Who Survived the Northern Pakistan Earthquake. Eur. J. Psychol. 2009, 5, 64–81. [Google Scholar] [CrossRef]
- Popa-Velea, O.; Lala, A.I.; Sturzu, L.M.; Bobîrnac, G.; Arsenie Spinu, D. The Usefulness of the Draw-a-Person (DAP) Test in Diagnosing Domestic Violence on Children. Rom. J. Leg. Med. 2017, 25, 217–220. [Google Scholar] [CrossRef]
- Potenza, S. Draw-a-Person for the Evaluation of Antisocial Personality Trait. Prev. Treat. 2016, 5, 9–15. [Google Scholar] [CrossRef]
- Lev-Wiesel, R. Abused Children of Holocaust Survivors: An Unspoken Issue. J. Fam. Soc. Work 1998, 3, 43–54. [Google Scholar] [CrossRef]
- McInnes, E. Young Children’s Drawings after Sexual Abuse: Disclosure and Recovery In Where to from Here?: Examining Conflict-Related and Relational Interaction Trauma; Brill: Boston, MA, USA, 2019; Volume 98, pp. 47–69. [Google Scholar]
- Osei, M. Illustration of Self-Concept through Drawings: The Perspective of the Child in an Orphanage. IJIRS 2013, 2, 761–779. [Google Scholar]
- Hamama, L.; Alshech, M. Children with Epilepsy: Assessing State Anxiety through Drawings and a Self-Report Questionnaire. Arts Health 2018, 12, 139–153. [Google Scholar] [CrossRef] [PubMed]
- Auemaneekul, N. Parents’ Perceptions of Child Abuse and Child Discipline in Bangkok, Thailand. J. Med. Assoc. Thai 2013, 96, S181–S189. [Google Scholar]
- Rhucharoenpornpanich, O.; Chamratrithirong, A.; Fongkaew, W.; Rosati, M.J.; Miller, B.A.; Cupp, P.K. Parenting and Adolescent Problem Behaviors: A Comparative Study of Sons and Daughters in Thailand. J. Med. Assoc. Thai 2010, 93, 293–300. [Google Scholar] [PubMed]
- Binson, B.; Kinear, A. Creative Arts Therapy with Thailand’s Mobile Arts Therapy Group. JUCR 2014, 6, 26–35. [Google Scholar]
- Bernstein, D.P.; Stein, J.A.; Newcomb, M.D.; Walker, E.; Pogge, D.; Ahluvalia, T.; Stokes, J.; Handelsman, L.; Medrano, M.; Desmond, D.; et al. Development and Validation of a Brief Screening Version of the Childhood Trauma Questionnaire. Child Abus. Negl. 2003, 27, 169–190. [Google Scholar] [CrossRef]
- Mueller, J.; Moergeli, H.; Maercker, A. Disclosure and Social Acknowledgement as Predictors of Recovery from Posttraumatic Stress: A Longitudinal Study in Crime Victims. Can. J. Psychiatry 2008, 53, 160–168. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; The Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Youden, W.J. Index for Rating Diagnostic Tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Lev-Wiesel, R.; Ramot, O.; Niv, H.; Daniel, E.; Gosh, Y.; Dahan, A.; Weinger, S. Physical versus Sexual Abuse as Reflected in Adolescents’ Self-Figure Drawings: A Preliminary Study. J. Child Sex. Abus. 2021, 31, 33–50. [Google Scholar] [CrossRef] [PubMed]
- Lev-Wiesel, R.; Hershkovitz, D. Detecting Violent Aggressive Behavior among Male Prisoners through the Machover Draw-A-PERSON Test. Arts Psychother. 2000, 27, 171–177. [Google Scholar] [CrossRef]
- Lev-Wiesel, R.; Yosipov-Kaziav, J. Deafness as Reflected in Self-Figure Drawings of Deaf People. J. Dev. Phys. Disabil. 2005, 17, 203–212. [Google Scholar] [CrossRef]
- Girish, M.; Lev-Wiesel, R.; Bhattacharyya, A. Child Abuse as Reflected in Self-figure Drawings of Indian Street Children. J. Child Adolesc. Trauma. 2022, submitted.
- Farokhi, M.; Hashemi, M. The Analysis of Children’s Drawings: Social, Emotional, Physical, and Psychological Aspects. Procedia Soc. Behav. Sci. 2011, 30, 2219–2224. [Google Scholar] [CrossRef]
- Adjei, D.; Oppong, C.; Amponsah, L. Arts and Design Studies Children’s Drawings with Genitals: Art Works from Children Who Co-Sleep with Adults. IISTE 2016, 41, 5–11. [Google Scholar]
- Kissos, L.; Goldner, L.; Butman, M.; Eliyahu, N.; Lev-Wiesel, R. Can Artificial Intelligence Achieve Human-Level Performance? A Pilot Study of Childhood Sexual Abuse Detection in Self-Figure Drawings. Child Abus. Negl. 2020, 109, 104755. [Google Scholar] [CrossRef]
- Daugherty, J.C.; Verdejo-Román, J.; Pérez-García, M.; Hidalgo-Ruzzante, N. Structural Brain Alterations in Female Survivors of Intimate Partner Violence. J. Interpers. Violence 2020, 37, NP4684–NP4717. [Google Scholar] [CrossRef] [PubMed]
- Wiener, A.R. Traumatic Brain Injury (TBI): The Progressive Neurodegeneration and Mental Health Decline in United States Veterans. Master’s Thesis, Philadelphia College of Osteopathic Medicine, Philadelphia, PA, USA, 2021. [Google Scholar]
- Lev-Wiesel, R.; Massrawa, N.; Binson, B. Parents’ and Children’s Perceptions of Child Maltreatment. J. Soc. Work 2019, 20, 395–410. [Google Scholar] [CrossRef]
- Luk, J.W.; Bond, A.E.; Gabrielli, J.; LaCroix, J.M.; Perera, K.U.; Lee-Tauler, S.Y.; Goldston, D.B.; Soumoff, A.; Ghahramanlou-Holloway, M. A Latent Class Analysis of Physical, Emotional, and Sexual Abuse History among Suicidal Inpatients. J. Psychiatr. Res. 2021, 142, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Binson, B.; Federman, D.J.; Lev-Wiesel, R. Do Self-Figure Drawings Reveal the Drawer’s Cultural Values? Thais and Israelis Draw Themselves. J. Humanist. Psychol. 2019, 002216781983108. [Google Scholar] [CrossRef]
- Ionio, C.; Mascheroni, E. Psychological Well-Being and Graphic Representations of Self in Child Victims of Violence. Arts Psychother. 2021, 72, 101740. [Google Scholar] [CrossRef]
- Tsur, N.; Katz, C. “And Then Cinderella Was Lying in My Bed”: Dissociation Displays in Forensic Interviews with Children Following Intrafamilial Child Sexual Abuse. J. Interpers. Violence 2021, 088626052110163. [Google Scholar] [CrossRef]
- Mucci, C.; Scalabrini, A. Traumatic Effects beyond Diagnosis: The Impact of Dissociation on the Mind-Body-Brain System. Psychoanal. Psychol. 2021, 38, 279–289. [Google Scholar] [CrossRef]
- Engstrom, M.; Liu, G.; Santana-Gonzalez, C.; Teoh, J.Y.; Harms, M.; Koy, K.; Quevedo, K. The Impact of Child Abuse on the Neurobiology of Self-Processing in Depressed Adolescents. Neurobiol. Stress 2021, 14, 100310. [Google Scholar] [CrossRef] [PubMed]
- Yoon, M.; Cho, S.; Yoon, D. Child Maltreatment and Depressive Symptomatology among Adolescents in out-of-Home Care: The Mediating Role of Self-Esteem. Child. Youth Serv. Rev. 2019, 101, 255–260. [Google Scholar] [CrossRef]
- Gewehr, E.; Hensel, B.; Volbert, R. Predicting Disclosure Latency in Substantiated Cases of Child Sexual Abuse. Child Abus. Negl. 2021, 122, 105346. [Google Scholar] [CrossRef]
- McElvaney, R. Disclosure of Child Sexual Abuse: Delays, Non-Disclosure and Partial Disclosure. What the Research Tells Us and Implications for Practice. Child Abuse Rev. 2013, 24, 159–169. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CEA N = 984 | CPA N = 560 | CSA N = 163 | p Value | |
|---|---|---|---|---|
| Head (disproportionate size) | 2.10 (1.27) | 2.10 (1.29) | 2.07 (1.29) | 0.973 |
| Forehead (emphasized, shadowed) | 1.05 (0.36) | 1.06 (0.39) | 1.07 (0.42) | 0.826 |
| Hair (stand, emphasized) | 1.95 (1.26) | 2.17 (1.34) | 2.04 (1.34) | 0.005 |
| Face line (double, hollow, shaded) | 1.91 (1.23) | 2.30 (1.34) | 3.67 (0.52) | <0.001 |
| Ears (emphasized, shadowed, double) | 1.26 (0.77) | 2.47 (1.47) | 2.01 (1.38) | <0.001 |
| Eyebrows (emphasized) | 1.40 (0.95) | 1.50 (1.04) | 1.52 (1.10) | 0.082 |
| Eyes (dots, shaded, hollow, crossed) | 3.36 (1.22) | 3.38 (1.20) | 3.40 (1.20) | 0.923 |
| Eyes (omitted) | 1.11 (0.56) | 1.16 (0.66) | 1.17 (0.69) | 0.261 |
| Nose (emphasized, big, shadowed, nostrils) | 1.57 (1.04) | 1.61 (1.07) | 1.64 (1.13) | 0.581 |
| Teeth (presence) | 1.17 (0.68) | 1.17 (0.68) | 1.19 (0.72) | 0.919 |
| Moustache/beard (thick, shadowed) | 1.03 (0.29) | 1.05 (0.38) | 1.02 (0.23) | 0.346 |
| Shoulders (broad) | 1.72 (1.14) | 1.77 (1.19) | 1.80 (1.17) | 0.621 |
| Arm position (asymmetry, horizontal) | 1.52 (1.02) | 1.54 (1.04) | 1.53 (1.06) | 0.931 |
| Hands/arms (clinging, detached, shadowed) | 1.94 (1.35) | 2.12 (1.45) | 2.12 (1.38) | 0.029 |
| Hands/arms (omitted, cut off) | 2.67 (1.45) | 2.59 (1.45) | 2.71 (1.45) | 0.508 |
| Fingers (large, pointed, clawed) | 1.09 (0.47) | 1.10 (0.50) | 1.12 (0.57) | 0.627 |
| Genitals (shaded, blocked, disconnected) | 1.00 (0.00) | 1.00 (0.04) | 1.05 (0.37) | <0.001 |
| Legs/feet (distorted, disproportionate) | 1.46 (0.72) | 1.43 (0.70) | 1.48 (0.76) | 0.688 |
| Legs and/or feet (omitted, cut off) | 2.22 (1.47) | 2.28 (1.47) | 2.31 (1.48) | 0.646 |
| Posture (strong, stable) | 1.15 (0.55) | 1.16 (0.59) | 1.07 (0.39) | 0.145 |
| Reluctance to talk | 36.6 (11.8) | 40.0 (12.2) | 41.8 (11.6) | <0.001 |
| Urge to talk | 28.8 (9.18) | 29.5 (8.53) | 29.3 (7.72) | 0.339 |
| Emotional reactions | 25.1 (8.80) | 28.3 (10.3) | 30.5 (9.61) | <0.001 |
| DTQ total score | 90.4 (22.9) | 97.8 (25.2) | 102 (22.4) | <0.001 |
| MSDQ total score | 2.10 (0.51) | 2.41 (0.57) | 2.48 (0.53) | <0.001 |
| Somatization | 2.10 (0.65) | 2.45 (0.72) | 2.53 (0.72) | <0.001 |
| Depression | 2.66 (0.74) | 3.00 (0.76) | 3.09 (0.71) | <0.001 |
| Dissociation | 1.66 (0.45) | 1.93 (0.55) | 1.98 (0.54) | <0.001 |
| CTQ total score | 1.80 (0.26) | 2.17 (0.35) | 2.36 (0.45) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaroenkajornkij, N.; Lev-Wiesel, R.; Binson, B. Use of Self-Figure Drawing as an Assessment Tool for Child Abuse: Differentiating between Sexual, Physical, and Emotional Abuse. Children 2022, 9, 868. https://doi.org/10.3390/children9060868
Jaroenkajornkij N, Lev-Wiesel R, Binson B. Use of Self-Figure Drawing as an Assessment Tool for Child Abuse: Differentiating between Sexual, Physical, and Emotional Abuse. Children. 2022; 9(6):868. https://doi.org/10.3390/children9060868
Chicago/Turabian StyleJaroenkajornkij, Nisara, Rachel Lev-Wiesel, and Bussakorn Binson. 2022. "Use of Self-Figure Drawing as an Assessment Tool for Child Abuse: Differentiating between Sexual, Physical, and Emotional Abuse" Children 9, no. 6: 868. https://doi.org/10.3390/children9060868