
Creative Arts Therapy in the “Remote Therapeutic Response” Format in the Education System


Abstract
:1. Introduction
1.1. Remote Psychotherapy
1.2. Remote Creative Arts Therapy
1.3. Creative Arts Therapy in the “Remote Therapeutic Response” Format in the Education System
2. Materials and Methods
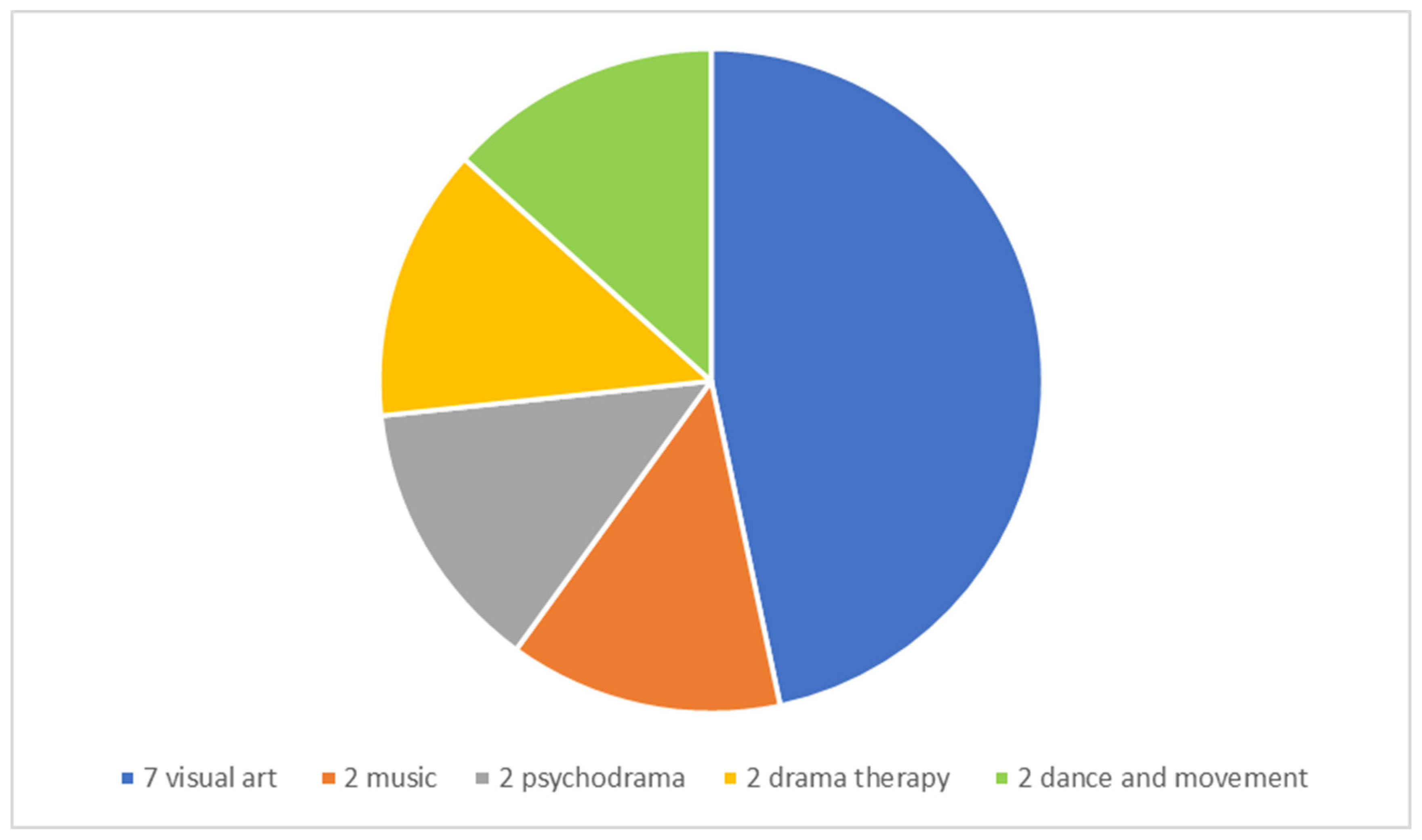
2.1. Participants
2.2. Procedure and Ethics
2.3. Data Processing
3. Results
3.1. The Emotional Experiences of Transitioning to a Remote Therapeutic Response
3.1.1. The Creative Arts Therapists’ Experiences at the Beginning of the Pandemic
3.1.2. The Adaptation Process
3.1.3. Continuing Instability
3.2. The Implementation of the Remote Therapeutic Response
3.2.1. Modes of Remote Therapeutic Response and Their Implementation
3.2.2. The Therapeutic Act
3.3. Benefits of Remote Creative Arts Therapy
3.3.1. Benefits for the Client
3.3.2. Benefits for the Creative Arts Therapist
3.4. Challenges in Remote Creative Arts Therapy
3.4.1. Technical and Logistical Challenges
3.4.2. Resistance during Remote Creative Arts Therapy
3.4.3. Lack of Close Contact and Body Language
3.4.4. Challenges in Maintaining Group Creative Arts Therapy
3.4.5. The Challenge of Being a Creative Arts Therapist during This Period
3.5. Remote Contact with Parents
3.5.1. Closer Connections than Usual
3.5.2. Parental Contributions to Managing the Remote Therapeutic Relationship
3.5.3. When Parents Are Not Available
3.6. Working in the Educational System
3.6.1. Contact with the Educational Staff
3.6.2. Contact with Officials in the Ministry of Education
3.7. Insights and Recommendations
3.7.1. Internal Strengths and Resources Contributing to the Work of Creative Arts Therapists during This Period
3.7.2. Feelings of Self-Worth and Professionalism
3.7.3. Recommendations
4. Discussion
Limitations and Suggestions for Further Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wittson, C.L.; Affleck, D.C.; Johnson, V. Two-way television in group therapy. Psychiatr. Serv. 1961, 12, 22–23. [Google Scholar] [CrossRef] [PubMed]
- Simpson, S. Psychotherapy via videoconferencing: A review. Br. J. Guid. Couns. 2009, 37, 271–286. [Google Scholar] [CrossRef]
- Nelson, E.-L.; Barnard, M.U.; Cain, S.T. Treating Childhood Depression over Videoconferencing. Telemed. E-Health 2003, 9, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Alessi, N.E. Telepsychiatric care for a depressed adolescent. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 894–895. [Google Scholar] [CrossRef] [PubMed]
- Sehon, C.M. Teleanalysis and teletherapy for children and adolescents? In Psychoanalysis Online 2: Impact of Technology on Development, Training, and Therapy; Savege-Scharff, J., Ed.; Routledge: Abingdon, UK, 2018; pp. 209–232. [Google Scholar]
- Rinat, S.; Feldman, A. Zoom-Out: About Art Therapy in the Time of COVID-19 Pandemic. Available online: https://www.betipulnet.co.il/particles/zoom_out_art_therapy (accessed on 27 November 2020).
- Engelhard, E.S.; Furlager, A.Y. Remaining held: Dance/movement therapy with children during lockdown. Body Mov. Dance Psychother. 2020, 16, 73–86. [Google Scholar] [CrossRef]
- Datlen, G.W.; Pandolfi, C. Developing an online art therapy group for learning disabled young adults using WhatsApp. Int. J. Art Ther. 2020, 25, 192–201. [Google Scholar] [CrossRef]
- Shaw, L. ‘Don’t look!’ An online art therapy group for adolescents with Anorexia Nervosa. Int. J. Art Ther. 2020, 25, 211–217. [Google Scholar] [CrossRef]
- Baker, F.; Krout, R. Songwriting via Skype. Br. J. Music Ther. 2009, 23, 3–14. [Google Scholar] [CrossRef]
- Hudgins, K. Action across the distance with telemedicine: The therapeutic spiral model to treat trauma online. In Combining the Creative Therapies with Technology: Using Social Media and Online Counseling to Treat Clients; Brooke, S.L., Ed.; Charles C. Thomas: Springfield, IL, USA, 2017; pp. 137–168. [Google Scholar]
- Mesika, S.L.; Wengrower, H.; Maoz, H. Waking up the bear: Dance/movement therapy group model with depressed adult patients during COVID-19 2020. Body Mov. Dance Psychother. 2021, 16, 32–46. [Google Scholar] [CrossRef]
- Glassman, E.L.; Prasad, S. Art therapy in schools: Its variety and benefits. In Using Art Therapy with Diverse Populations: Crossing Cultures and Abilities; Howie, P., Prasad, S., Kristel, J., Eds.; Jessica Kingsley Publisher: London, UK, 2013; pp. 126–133. [Google Scholar]
- Deboys, R.; Holttum, S.; Wright, K. Processes of change in school-based art therapy with children: A systematic qualitative study. Int. J. Art Ther. 2016, 22, 118–131. [Google Scholar] [CrossRef]
- Harpazi, S.; Regev, D.; Snir, S.; Raubach-Kaspy, R. Perceptions of Art Therapy in Adolescent Clients Treated within the School System. Front. Psychol. 2020, 11, 518304. [Google Scholar] [CrossRef] [PubMed]
- Snir, S.; Regev, D.; Keinan, V.; El Kader-Shahada, H.A.; Salamey, A.; Mekel, D.; Melzak, D.; Daoud, H.; Green-Orlovich, A.; Belity, I.; et al. Art therapy in the Israeli education system—A qualitative meta-analysis. Int. J. Art Ther. 2017, 23, 169–179. [Google Scholar] [CrossRef]
- Hill, C.E.; Thompson, B.J.; Williams, E.N. A Guide to Conducting Consensual Qualitative Research. Couns. Psychol. 1997, 25, 517–572. [Google Scholar] [CrossRef] [Green Version]
- Hill, C.E.; Knox, S.; Thompson, B.J.; Williams, E.N.; Hess, S.A.; Ladany, N. Consensual qualitative research: An update. J. Couns. Psychol. 2005, 52, 196–205. [Google Scholar] [CrossRef] [Green Version]
- Zubala, A.; Hackett, S. Online art therapy practice and client safety: A UK-wide survey in times of COVID-19. Int. J. Art Ther. 2020, 25, 161–171. [Google Scholar] [CrossRef]
- Cole, L.P.; Henechowicz, T.L.; Kang, K.; Pranjić, M.; Richard, N.M.; Tian, G.L.J.; Hurt-Thaut, C. Neurologic Music Therapy via Telehealth: A Survey of Clinician Experiences, Trends, and Recommendations During the COVID-19 Pandemic. Front. Neurosci. 2021, 15, 648489. [Google Scholar] [CrossRef] [PubMed]
- Sperandeo, R.; Cioffi, V.; Mosca, L.L.; Longobardi, T.; Moretto, E.; Alfano, Y.M.; Scandurra, C.; Muzii, B.; Cantone, D.; Guerriera, C.; et al. Exploring the Question: “Does Empathy Work in the Same Way in Online and In-Person Therapeutic Settings?”. Front. Psychol. 2021, 12, 671790. [Google Scholar] [CrossRef] [PubMed]
- Regev, D.; Green-Orlovich, A.; Snir, S. Art therapy in schools—The therapist’s perspective. Arts Psychother. 2015, 45, 47–55. [Google Scholar] [CrossRef]
- Braus, M.; Morton, B. Art therapy in the time of COVID-19. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S267–S268. [Google Scholar] [CrossRef] [PubMed]
- Gabbard, G.O.; Kassaw, K.A.; Perez-Garcia, G. Professional Boundaries in the Era of the Internet. Acad. Psychiatry 2011, 35, 168–174. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Therapists’ Emotional Experiences | Implementation of Remote Therapeutic Response | Benefits of Remote Creative Arts Therapy | Challenges in Remote Creative Arts Therapy | Remote Contact with Parents | Working in the Educational System | Insights and Recommendations |
|---|---|---|---|---|---|---|
| Beginning of the pandemic The adaptation process Continuing instability | Modes of remote therapeutic response
| Benefits for the client Benefits for the creative arts therapist | Technical and logistical challenges Resistance Lack of close contact and less body language Maintaining group therapy Being a creative arts therapist during this period | Closer connections than usual Parental contribution to managing therapy When parents are not available | Contact with the educational staff Contact with officials in the Ministry of Education | Internal strengths and resources contributing to the therapists Self-worth and professionalism Recommendations |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korman-Hacohen, S.; Regev, D.; Roginsky, E. Creative Arts Therapy in the “Remote Therapeutic Response” Format in the Education System. Children 2022, 9, 467. https://doi.org/10.3390/children9040467
Korman-Hacohen S, Regev D, Roginsky E. Creative Arts Therapy in the “Remote Therapeutic Response” Format in the Education System. Children. 2022; 9(4):467. https://doi.org/10.3390/children9040467
Chicago/Turabian StyleKorman-Hacohen, Shir, Dafna Regev, and Efrat Roginsky. 2022. "Creative Arts Therapy in the “Remote Therapeutic Response” Format in the Education System" Children 9, no. 4: 467. https://doi.org/10.3390/children9040467