
National Cross-Sectional Study of Mental Health Screening Practices for Primary Caregivers of NICU Infants

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Sample, and Recruitment
2.2. Survey Instrument
2.3. Data Analysis
3. Results
3.1. Participants
3.2. Psychosocial Staffing
3.3. Caregiver Education
3.4. Caregiver PMAD Screening
3.5. Referral and Treatment
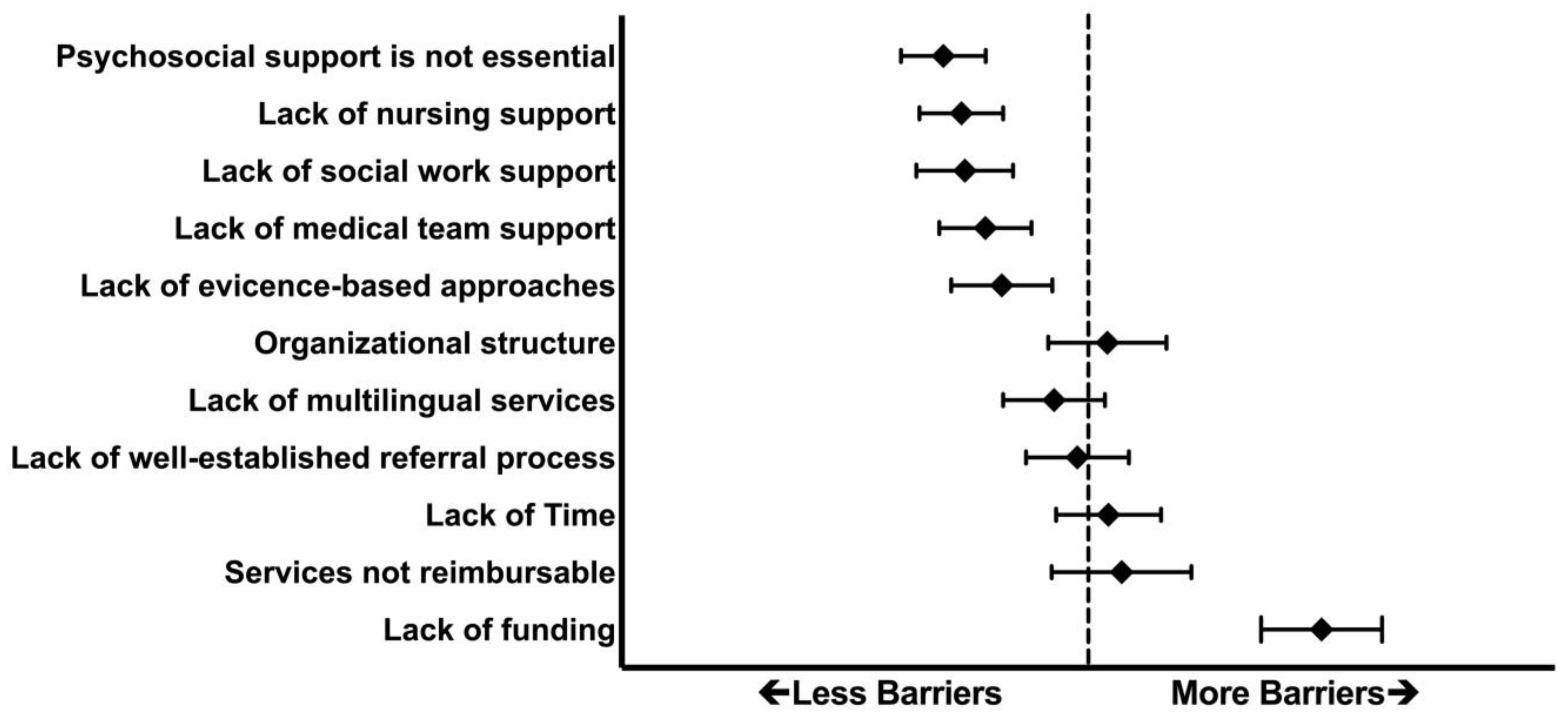
3.6. Challenges in Implementing NICU Caregiver Mental Health Services
4. Discussion
4.1. Staff
4.2. Education
4.3. Screening Timing and Instruments
4.4. Referral and Treatment
4.5. Challenges and Barriers
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Kleine, I. Interventions to Prevent Perinatal Depression: US Preventive Services Task Force Recommendation Statement. Arch. Dis. Child.-Educ. Amp Pract. Ed. 2020, 105, 242. [Google Scholar] [CrossRef] [PubMed]
- Rao, W.-W.; Zhu, X.-M.; Zong, Q.-Q.; Zhang, Q.; Hall, B.J.; Ungvari, G.S.; Xiang, Y.-T. Prevalence of Prenatal and Postpartum Depression in Fathers: A Comprehensive Meta-Analysis of Observational Surveys. J. Affect. Disord. 2020, 263, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Tahirkheli, N.N.; Cherry, A.S.; Tackett, A.P.; McCaffree, M.A.; Gillaspy, S.R. Postpartum Depression on the Neonatal Intensive Care Unit: Current Perspectives. Int. J. Womens Health 2014, 6, 975–987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldoni, F.; Giannotti, M. Perinatal Distress in Fathers: Toward a Gender-Based Screening of Paternal Perinatal Depressive and Affective Disorders. Front. Psychol. 2020, 11, 1892. [Google Scholar] [CrossRef] [PubMed]
- Cox, E.Q.; Sowa, N.A.; Meltzer-Brody, S.E.; Gaynes, B.N. The Perinatal Depression Treatment Cascade: Baby Steps Toward Improving Outcomes. J. Clin. Psychiatry 2016, 77, 1189–1200. [Google Scholar] [CrossRef]
- McKee, K.; Admon, L.K.; Winkelman, T.N.A.; Muzik, M.; Hall, S.; Dalton, V.K.; Zivin, K. Perinatal Mood and Anxiety Disorders, Serious Mental Illness, and Delivery-Related Health Outcomes, United States, 2006–2015. BMC Womens Health 2020, 20, 150. [Google Scholar] [CrossRef]
- Slomian, J.; Honvo, G.; Emonts, P.; Reginster, J.-Y.; Bruyère, O. Consequences of Maternal Postpartum Depression: A Systematic Review of Maternal and Infant Outcomes. Womens Health 2019, 15, 1745506519844044. [Google Scholar] [CrossRef] [Green Version]
- Earls, M.F.; Yogman, M.W.; Mattson, G.; Rafferty, J.; Committee on Psychosocial Aspects of Child and Family Health; Baum, R.; Gambon, T.; Lavin, A.; Wissow, L. Incorporating Recognition and Management of Perinatal Depression Into Pediatric Practice. Pediatrics 2019, 143, e20183259. [Google Scholar] [CrossRef] [Green Version]
- Kendig, S.; Keats, J.P.; Hoffman, M.C.; Kay, L.B.; Miller, E.S.; Moore Simas, T.A.; Frieder, A.; Hackley, B.; Indman, P.; Raines, C.; et al. Consensus Bundle on Maternal Mental Health: Perinatal Depression and Anxiety. Obstet. Gynecol. 2017, 129, 422–430. [Google Scholar] [CrossRef] [Green Version]
- Siu, A.L.; the US Preventive Services Task Force (USPSTF). Screening for Depression in Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2016, 315, 380–387. [Google Scholar] [CrossRef]
- Braun, D.; Braun, E.; Chiu, V.; Burgos, A.E.; Gupta, M.; Volodarskiy, M.; Getahun, D. Trends in Neonatal Intensive Care Unit Utilization in a Large Integrated Health Care System. JAMA Netw. Open 2020, 3, e205239. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.K.; Driscoll, A.K. Births: Final Data for 2019. Natl. Vital. Stat. Rep. 2021, 70, 1–51. [Google Scholar] [PubMed]
- Harrison, W.N.; Wasserman, J.R.; Goodman, D.C. Regional Variation in Neonatal Intensive Care Admissions and the Relationship to Bed Supply. J. Pediatr. 2018, 192, 73–79.e4. [Google Scholar] [CrossRef] [PubMed]
- Rogers, C.E.; Kidokoro, H.; Wallendorf, M.; Inder, T.E. Identifying Mothers of Very Preterm Infants At-Risk for Postpartum Depression and Anxiety before Discharge. J. Perinatol. 2013, 33, 171–176. [Google Scholar] [CrossRef] [Green Version]
- Treyvaud, K.; Lee, K.J.; Doyle, L.W.; Anderson, P.J. Very Preterm Birth Influences Parental Mental Health and Family Outcomes Seven Years after Birth. J. Pediatr. 2014, 164, 515–521. [Google Scholar] [CrossRef] [Green Version]
- Roque, A.T.F.; Lasiuk, G.C.; Radünz, V.; Hegadoren, K. Scoping Review of the Mental Health of Parents of Infants in the NICU. J. Obstet. Gynecol. Neonatal Nurs. 2017, 46, 576–587. [Google Scholar] [CrossRef] [Green Version]
- Cole, J.C.M.; Olkkola, M.; Zarrin, H.E.; Berger, K.; Moldenhauer, J.S. Universal Postpartum Mental Health Screening for Parents of Newborns With Prenatally Diagnosed Birth Defects. J. Obstet. Gynecol. Neonatal Nurs. 2018, 47, 84–93. [Google Scholar] [CrossRef] [Green Version]
- Schecter, R.; Pham, T.; Hua, A.; Spinazzola, R.; Sonnenklar, J.; Li, D.; Papaioannou, H.; Milanaik, R. Prevalence and Longevity of PTSD Symptoms Among Parents of NICU Infants Analyzed Across Gestational Age Categories. Clin. Pediatr. 2020, 59, 163–169. [Google Scholar] [CrossRef]
- Hynan, M.T.; Mounts, K.O.; Vanderbilt, D.L. Screening Parents of High-Risk Infants for Emotional Distress: Rationale and Recommendations. J. Perinatol. 2013, 33, 748–753. [Google Scholar] [CrossRef] [Green Version]
- Mendelson, T.; Cluxton-Keller, F.; Vullo, G.C.; Tandon, S.D.; Noazin, S. NICU-Based Interventions To Reduce Maternal Depressive and Anxiety Symptoms: A Meta-Analysis. Pediatrics 2017, 139, e20161870. [Google Scholar] [CrossRef] [Green Version]
- Hynan, M.T.; Steinberg, Z.; Baker, L.; Cicco, R.; Geller, P.A.; Lassen, S.; Milford, C.; Mounts, K.O.; Patterson, C.; Saxton, S.; et al. Recommendations for Mental Health Professionals in the NICU. J. Perinatol. Off. J. Calif. Perinat. Assoc. 2015, 35 (Suppl. S1), S14–S18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murthy, S.; Haeusslein, L.; Bent, S.; Fitelson, E.; Franck, L.S.; Mangurian, C. Feasibility of Universal Screening for Postpartum Mood and Anxiety Disorders among Caregivers of Infants Hospitalized in NICUs: A Systematic Review. J. Perinatol. 2021, 41, 1811–1824. [Google Scholar] [CrossRef]
- NICU Directory. Available online: https://neonatologysolutions.com/nicu-directory/ (accessed on 6 May 2021).
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- NICU Search. Available online: https://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/nicuverification/Pages/NICUSearch.aspx (accessed on 6 May 2021).
- Farr, S.L.; Denk, C.E.; Dahms, E.W.; Dietz, P.M. Evaluating Universal Education and Screening for Postpartum Depression Using Population-Based Data. J. Womens Health 2014, 23, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Moreyra, A.; Dowtin, L.L.; Ocampo, M.; Perez, E.; Borkovi, T.C.; Wharton, E.; Simon, S.; Armer, E.G.; Shaw, R.J. Implementing a Standardized Screening Protocol for Parental Depression, Anxiety, and PTSD Symptoms in the Neonatal Intensive Care Unit. Early Hum. Dev. 2021, 154, 105279. [Google Scholar] [CrossRef] [PubMed]
- California Children’s Services (CCS) Manual of Procedures Ch. 3.25 Standards for Neonatal Intensive Care Units (NICUs); Department of Health Care Services: Sacramento, CA, USA, 1999.
- Cherry, A.S.; Blucker, R.T.; Thornberry, T.S.; Hetherington, C.; McCaffree, M.A.; Gillaspy, S.R. Postpartum Depression Screening in the Neonatal Intensive Care Unit: Program Development, Implementation, and Lessons Learned. J. Multidiscip. Healthc. 2016, 9, 59–67. [Google Scholar] [CrossRef]
- Scheans, P.; Mischel, R.; Munson, M.; Bulaevskaya, K. Postpartum Mood Disorders Screening in the NICU. Neonatal Netw. 2016, 35, 240–242. [Google Scholar] [CrossRef]
- Vaughn, A.T.; Hooper, G.L. Development and Implementation of a Postpartum Depression Screening Program in the NICU. Neonatal Netw. 2020, 39, 75–82. [Google Scholar] [CrossRef]
- Lambarth, C.; Green, B. Maternal Post-Partum Mood Disorder Screening Implementation in a Neonatal Intensive Care Unit: Lessons Learned through Multnomah Project LAUNCH; Portland State University: Portland, OR, USA, 2015. [Google Scholar]
- Mounts, K.O. Screening for Maternal Depression in the Neonatal ICU. Curr. Controv. Perinatol. 2009, 36, 137–152. [Google Scholar] [CrossRef]
- Teissèdre, F.; Chabrol, H. Detecting Women at Risk for Postnatal Depression Using the Edinburgh Postnatal Depression Scale at 2 to 3 Days Postpartum. Can. J. Psychiatry 2004, 49, 51–54. [Google Scholar] [CrossRef] [Green Version]
- El-Hachem, C.; Rohayem, J.; Bou Khalil, R.; Richa, S.; Kesrouani, A.; Gemayel, R.; Aouad, N.; Hatab, N.; Zaccak, E.; Yaghi, N.; et al. Early Identification of Women at Risk of Postpartum Depression Using the Edinburgh Postnatal Depression Scale (EPDS) in a Sample of Lebanese Women. BMC Psychiatry 2014, 14, 242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knights, J.E.; Salvatore, M.L.; Simpkins, G.; Hunter, K.; Khandelwal, M. In Search of Best Practice for Postpartum Depression Screening: Is Once Enough? Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 206, 99–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gavin, N.I.; Gaynes, B.N.; Lohr, K.N.; Meltzer-Brody, S.; Gartlehner, G.; Swinson, T. Perinatal Depression: A Systematic Review of Prevalence and Incidence. Obstet. Gynecol. 2005, 106, 1071–1083. [Google Scholar] [CrossRef] [PubMed]
- Matthey, S.; Barnett, B.; Kavanagh, D.J.; Howie, P. Validation of the Edinburgh Postnatal Depression Scale for Men, and Comparison of Item Endorsement with Their Partners. J. Affect. Disord. 2001, 64, 175–184. [Google Scholar] [CrossRef]
- Darwin, Z.; Domoney, J.; Iles, J.; Bristow, F.; Siew, J.; Sethna, V. Assessing the Mental Health of Fathers, Other Co-Parents, and Partners in the Perinatal Period: Mixed Methods Evidence Synthesis. Front. Psychiatry 2021, 11, 1260. [Google Scholar] [CrossRef]
- Myers, E.R.; Aubuchon-Endsley, N.; Bastian, L.A.; Gierisch, J.M.; Kemper, A.R.; Swamy, G.K.; Wald, M.F.; McBroom, A.J.; Lallinger, K.R.; Gray, R.N.; et al. Efficacy and Safety of Screening for Postpartum Depression; AHRQ Comparative Effectiveness Reviews; Agency for Healthcare Research and Quality (US): Rockville MD, USA, 2013. [Google Scholar]
- Hernandez, N.D.; Francis, S.; Allen, M.; Bellamy, E.; Sims, O.T.; Oh, H.; Guillaume, D.; Parker, A.; Chandler, R. Prevalence and Predictors of Symptoms of Perinatal Mood and Anxiety Disorders among a Sample of Urban Black Women in the South. Matern. Child Health J. 2022, 26, 770–777. [Google Scholar] [CrossRef]
- Admon, L.K.; Winkelman, T.N.A.; Zivin, K.; Terplan, M.; Mhyre, J.M.; Dalton, V.K. Racial and Ethnic Disparities in the Incidence of Severe Maternal Morbidity in the United States, 2012–2015. Obstet. Gynecol. 2018, 132, 1158–1166. [Google Scholar] [CrossRef]
- The American College of Obstetricians and Gynecologists. Committee Opinion No. 630: Screening for Perinatal Depression. Obstet. Gynecol. 2015, 125, 1268–1271. [Google Scholar] [CrossRef]
- Mangurian, C.; Packman, W.; Riano, N.S.; Kearney, J. The Need to Support Caregivers during Pediatric Bone Marrow Transplantation (BMT): A Case Report. Palliat. Support. Care 2018, 16, 367–370. [Google Scholar] [CrossRef]
- De Figueiredo, F.P.; Parada, A.P.; Cardoso, V.C.; Batista, R.F.L.; da Silva, A.A.M.; Barbieri, M.A.; de Cavalli, R.C.; Bettiol, H.; Del-Ben, C.M. Postpartum Depression Screening by Telephone: A Good Alternative for Public Health and Research. Arch. Womens Ment. Health 2015, 18, 547–553. [Google Scholar] [CrossRef]
- Chow, R.; Huang, E.; Li, A.; Li, S.; Fu, S.Y.; Son, J.S.; Foster, W.G. Appraisal of Systematic Reviews on Interventions for Postpartum Depression: Systematic Review. BMC Pregnancy Childbirth 2021, 21, 18. [Google Scholar] [CrossRef] [PubMed]
- Hanach, N.; de Vries, N.; Radwan, H.; Bissani, N. The Effectiveness of Telemedicine Interventions, Delivered Exclusively during the Postnatal Period, on Postpartum Depression in Mothers without History or Existing Mental Disorders: A Systematic Review and Meta-Analysis. Midwifery 2021, 94, 102906. [Google Scholar] [CrossRef] [PubMed]
- Eisman, A.B.; Kilbourne, A.M.; Dopp, A.R.; Saldana, L.; Eisenberg, D. Economic Evaluation in Implementation Science: Making the Business Case for Implementation Strategies. VSIImplementation Sci. 2020, 283, 112433. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, L.; Long, M.; Theodorou, P.; Barclay Hoffman, S.; Soghier, L.; Beers, L. Perinatal Mental Health Task Force: Integrating Care Across a Pediatric Hospital Setting. Pediatrics 2021, 148, e2021050300. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Geographic Distribution (US Census Regions) a | n (%) |
|---|---|
| Midwest | 15 (20%) |
| West | 18 (24%) |
| South | 18 (24%) |
| Northeast | 24 (32%) |
| Type of NICU Setting b | |
| Independent Children’s Hospital vs. Not | |
| Children’s hospital | 28 (37%) |
| Non-children’s hospital | 47 (63%) |
| Academic vs. Community Hospital | |
| Academic medical center | 25 (33%) |
| Community center | 32 (42%) |
| NICU Level | |
| I | 1 (1%) |
| II | 7 (9%) |
| III | 45 (60%) |
| IV | 22 (29%) |
| Patient Volume (per month) | |
| 0–50 | 38 (50%) |
| 51–100 | 24 (32%) |
| 101–150 | 6 (8%) |
| 150–200 | 2 (3%) |
| 200+ | 5 (7%) |
| Geographic Distribution (US Census Regions) | Study Sample n (%) | National Sample n (%) a | p-Value |
|---|---|---|---|
| Midwest | 15 (20%) | 303 (21.8%) | 0.78 |
| West | 18 (24%) | 323 (23.3%) | 0.89 |
| South | 18 (24%) | 534 (38.5%) | 0.01 |
| Northeast | 24 (32%) | 229 (16.5%) | 0.001 |
| Type of NICU Setting b | |||
| Independent Children’s Hospital vs. Not | |||
| Children’s hospital | 28 (37%) | 212 (15.3%) | <0.001 |
| Non-children’s hospital | 47 (63%) | 1175 (84.7%) | <0.001 |
| Academic vs. Community Hospital | |||
| Academic medical center | 25 (33%) | 162 (12.6%) | <0.001 |
| Community center | 32 (42%) | 1128 (87.4%) | <0.001 |
| NICU Level | |||
| I | 1 (1%) | 0 (0%) | 0.05 |
| II | 7 (9%) | 552 (39.8%) | <0.001 |
| III | 45 (60%) | 708 (51.1%) | 0.15 |
| IV | 22 (29%) | 127 (9.2%) | <0.001 |
| Patient Volume (per month) c | |||
| 0–50 | 38 (50%) | 426 (41.4%) | 0.15 |
| 51–100 | 24 (32%) | 344 (33.5%) | 0.89 |
| 101–150 | 6 (8%) | 157 (15.3%) | 0.09 |
| 150–200 | 2 (3%) | 61 (5.9%) | 0.31 |
| 200+ | 5 (7%) | 40 (3.9%) | 0.23 |
| Education a n (%) | Screening b n (%) | Treatment n (%) | |
|---|---|---|---|
| Geographic Region | |||
| Midwest (n = 15) | 8 (53%) | 8 (83%) | 12 (80%) |
| West (n = 18) | 8 (44%) | 10 (56%) | 14 (78%) |
| South (n = 18) | 9 (50%) | 9 (50%) | 14 (78%) |
| Northeast (n = 24) | 10 (42%) | 6 (25%) | 20 (83%) |
| Hospital Type c | |||
| Independent Children’s Hospital vs. Not | |||
| Children’s hospital (n = 28) | 15 (54%) | 14 (50%) | 23 (82%) |
| Non-children’s hospital (n = 47) | 20 (43%) | 19 (40%) | 37 (79%) |
| Academic vs. Community Hospital | |||
| Academic (n = 39) | 21 (54%) | 20 (51%) | 32 (82%) |
| Community (n = 36) | 14 (39%) | 13 (36%) | 28 (78%) |
| NICU Level | |||
| I–III (n = 53) | 22 (42%) | 20 (38%) | 42 (79%) |
| IV (n = 22) | 13 (59%) | 13 (59%) | 18 (82%) |
| Patient Volume (per month) | |||
| 0–50 (n = 38) | 16 (42%) | 14 (37%) | 30 (79%) |
| 51+ (n = 37) | 19 (51%) | 19 (51%) | 30 (81%) |
| n (%) | |
|---|---|
| Referrals | |
| Referral to therapist in the community | 39 (65%) |
| Referral to therapist in hospital system | 34 (57%) |
| Referral to psychiatrist in hospital system | 29 (48%) |
| Referral to psychiatrist in the community | 27 (45%) |
| Services | |
| Support groups | 32 (53%) |
| Individual supportive psychotherapy | 19 (32%) |
| Couples/Marital counseling | 6 (10%) |
| Cognitive behavioral therapy | 4 (7%) |
| Family therapy | 3 (5%) |
| Problem solving skills training (PSST) | 2 (3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bloyd, C.; Murthy, S.; Song, C.; Franck, L.S.; Mangurian, C. National Cross-Sectional Study of Mental Health Screening Practices for Primary Caregivers of NICU Infants. Children 2022, 9, 793. https://doi.org/10.3390/children9060793
Bloyd C, Murthy S, Song C, Franck LS, Mangurian C. National Cross-Sectional Study of Mental Health Screening Practices for Primary Caregivers of NICU Infants. Children. 2022; 9(6):793. https://doi.org/10.3390/children9060793
Chicago/Turabian StyleBloyd, Cooper, Snehal Murthy, Clara Song, Linda S. Franck, and Christina Mangurian. 2022. "National Cross-Sectional Study of Mental Health Screening Practices for Primary Caregivers of NICU Infants" Children 9, no. 6: 793. https://doi.org/10.3390/children9060793