
Management of IgA Nephropathy in Pediatric Patients

Department of General Pediatrics, Adolescent Medicine and Neonatology, Faculty of Medicine, Medical Center, University of Freiburg, Mathildenstrasse 1, 79106 Freiburg, Germany
*
Author to whom correspondence should be addressed.
Children 2022, 9(5), 653; https://doi.org/10.3390/children9050653
Submission received: 10 March 2022
/
Revised: 25 April 2022
/
Accepted: 27 April 2022
/
Published: 2 May 2022
(This article belongs to the Special Issue Diagnosis and Treatment of IgA Nephropathy and IgA Vasculitis Nephritis in Children)
Abstract
:The onset of IgA nephritis in childhood and adolescence often develops into chronic glomerulonephritis with declining renal function. Although these long-term consequences are known, there is still a lack of evidence-based treatment recommendations in this age group. We report data from 22 pediatric patients who were biopsied to confirm the diagnosis of IgAN at our clinical center. 14 of them were treated with corticosteroids according to the recommendations for IgA nephritis vasculitis of the German Society of Pediatric Nephrology (GPN). Improvement was achieved in the majority of all cases, with a significant reduction in proteinuria five months after initiation of therapy. Our data suggest that treatment regimens for acute IgA nephritis and IgA vasculitis nephritis may be unified and are discussed in the context of current studies.
1. Introduction
IgA nephritis (IgAN) comprises a spectrum of heterogeneous courses, ranging from rapidly resolving glomerulonephritis to progressive loss of renal function [1]. Onset in childhood and adolescence often leads to transition to chronic nephritis and long-term impaired prognosis [2]. Most patients with IgAN who require renal replacement therapy are young adults [3,4] who possibly developed the disease in childhood.
While mild manifestations of IgAN allow watchful waiting combined with renoprotective therapy, the pediatric nephrologist faces a difficult decision in more aggressive cases, as no evidence-based guidelines have been formulated to date. The Kidney Disease Improving Global Outcomes (KDIGO) guidelines recommend the use of renin-angiotensin system blockade in children with proteinuria > 0.2 g/g creatinine. Despite widespread use of immunosuppressive therapy, especially glucocorticoids, there is no international consensus on their indication in more severe cases as strong trial-based evidence is still missing [5,6].
The aim of this small retrospective study and literature review is to highlight the challenges of pediatric IgAN in clinical practice and to discuss them in the context of current studies.
2. Materials and Methods
We retrospectively reviewed the charts of 22 children who were diagnosed with IgAN after renal biopsy in our pediatric nephrology center from 2001 to 2021.
Clinical findings such as hematuria and hypertension were assessed. Microhematuria was defined as microscopic evidence of more than 5 erythrocytes in a high-power field; macrohematuria meant a visible change of urine color. Hypertension was defined as a systolic and/or diastolic blood pressure above the 95th percentile according to age, height, and gender following the KiGGS-study [7]. Proteinuria was estimated using the urine protein to creatinine ratio (UPCR) in g protein/g creatinine. A ratio of >0.2 is considered as proteinuria and >3.5 as nephrotic range proteinuria. For glomerular filtration rate estimation (eGFR), the Schwartz formula using body length and plasma creatinine was used [8].
The biopsy specimens were analyzed by a pathologist according to the Oxford classification (MEST score). For 14 biopsies preceding the updated 2017 classification [9], the C-score was derived from the histopathological description. A minimum of 8 glomeruli per sample was needed for biopsy evaluation.
Follow-ups were carried out at four points in time: after 4 (2–6) weeks, 5 (3–7) months, one year (11–18 months), and two to three years (20–38 months). For patients with an observation period of more than 3.5 years, final follow-up data were also added (mean 5.8 years). Due to missing data points, the size of the patient collective varies as indicated. One patient with end-stage renal disease at initial presentation received kidney transplantation; all posttransplant clinical parameters were excluded from the study.
Treatment modalities included renoprotection with angiotensin converting-enzyme inhibitor (ACEI) or angiotensin II receptor blocker (ARB), immunosuppressive therapy (prednisone, cyclophosphamide, cyclosporine A, tacrolimus, or mycophenolate mofetil), plasmapheresis, or hemodialysis, as well as kidney transplantation. The treatment followed the recommendations of the German Society for Pediatric Nephrology (GPN) for IgAVN [10] and aimed for complete remission as documented by proteinuria < 0.2 g protein/g creatinine and normalized eGFR > 90 mL/min/1.73 m2. Glucocorticoid therapy was restricted to 8 weeks and then replaced by alternative immunosuppression where necessary to reduce steroid toxicity. The side effects of steroid therapy were monitored by regular determinations of blood pressure, weight, and glucosuria in urine dipstick.
Results were expressed as means with standard deviation and minimum–maximum values. Parameters such as proteinuria and eGFR over time were compared using the Wilcoxon signed-rank test, parameters of differently treated groups were compared by Mann–Whitney U test, and p-values < 0.05 were considered statistically significant. Analyses were performed using SciPy for Python [11]. The study was approved by the Ethics Committee of the University of Freiburg (22-1059).
3. Results
3.1. Diagnosis
We studied 22 children and adolescents diagnosed with IgAN from 2001 to 2021 in the Department of Pediatrics, Adolescent Medicine and Neonatology, at the University Hospital of Freiburg, Germany. Table 1 outlines the clinical characteristics and the pathological findings at biopsy. Our study group was male-dominated (64%). The mean age at symptom onset was 10.2 ± 3.7 years. The average time to biopsy was 41 weeks (2 days–10 years). At the time of biopsy, the average age was 11.0 ± 3.5 years.
Half of the children and adolescents initially presented with hypertension; 32% showed microhematuria and 68% macrohematuria. The mean proteinuria at biopsy was 3.2 ± 3.7 g/g creatinine and average eGFR 81.3 ± 49.7 mL/min/1.73 m2; 32% showed severely impaired renal function with an eGFR < 60 mL/min/1.73 m2, and in 41% proteinuria extended into the nephrotic range. All children were followed for a median of 3.5 years (2 months-10 years).
The average number of glomeruli in the biopsy sample was 31.8 ± 24.1 (8–107) per biopsy. The Oxford classification [9] showed 68% of children with mesangial proliferation (M1), 55% with endocapillary proliferation (E1), 64% with segmental sclerosis/adhesion lesion (S1), 5% with moderate tubular atrophy/interstitial fibrosis (T1 25–50% of cortical area involved), none with severe tubular atrophy/interstitial fibrosis (T2 > 50% of cortical area involved), 59% with crescents (C1 < 25% of glomeruli), and none with more than 25% (C2).
3.2. Treatment
As described in Table 2, 95% of the 22 children received therapy with ACE inhibitors or AT receptor blockers and another 14 children (64%) underwent i.v. corticosteroid therapy. A total of 6 children (27%) received additional immunosuppressants (mycophenolate mofetil, cyclosporine A, cyclophosphamide, tacrolimus, budesonide). Hemodialysis was performed in 2 children (9%); one of them also required plasmapheresis. One patient (5%) with end-stage renal disease at initial presentation required renal transplantation.
Steroid therapy involved three intravenous administrations of methylprednisolone (or equivalent dose of i.v. prednisone) at a dose of 300 mg/m2 body surface area (max. 3 × 500 mg) every 48 h, followed by prednisone p.o. in descending doses (initially 4 weeks with 60 mg/m2 BSA/48 h, max. 80 mg, then 4 weeks 40 mg/m2 BSA/day, max. 60 mg). This is consistent with the treatment of IgA vasculitis nephritis (IgAVN) patients, as recommended by the German Society of Pediatric Nephrology (GPN) in 2013. In patients with deteriorating eGFR despite intensified immunosuppression (corticosteroid therapy and cyclophosphamide), plasmapheresis is used as rescue therapy [10].
Although treatment decisions were made on a case-by-case basis, the most important factors to initiate a steroid therapy were the evidence of crescents in the biopsy specimen (86% in the treated vs. 13% in non-treated group), nephrotic range proteinuria (57% vs. 13%), or severely impaired renal function (43% vs. 13% with an eGFR < 60 mL/min/1.73 m2).
3.3. Follow-Up and Outcome
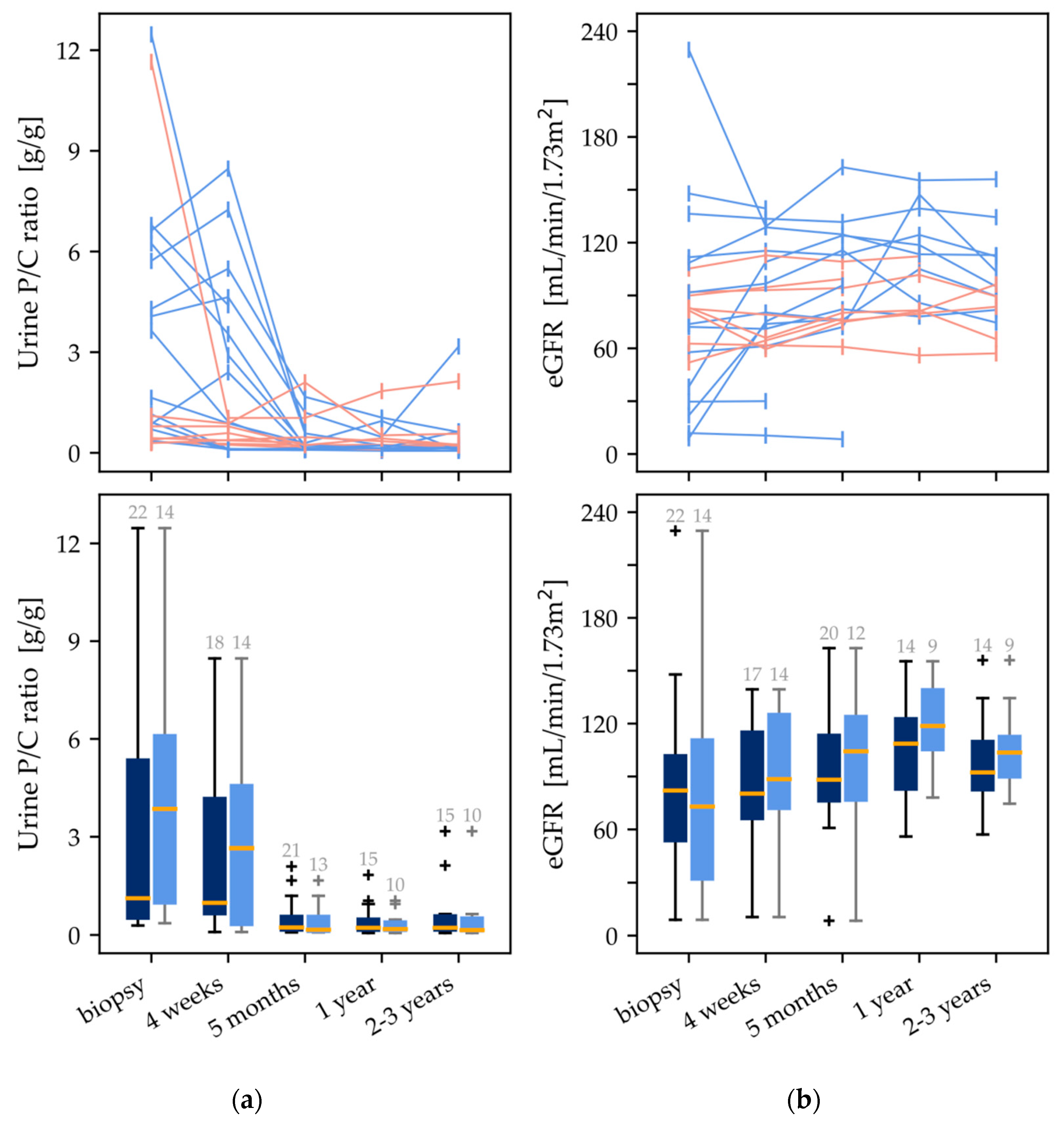
The collected data (proteinuria and eGFR) of five follow up visits are shown in Figure 1. Table 3 indicates the corresponding means, standard deviations, and ranges.
Five months after start of therapy, protein excretion decreased significantly (p < 0.001) from 3.2 ± 3.7 (0.29–12.5) to 0.5 ± 0.6 (0.08–2.1) g/g creatinine. However, the improvement in eGFR from 81.3 ± 49.7 (8.9–229.4) to 92.7 ± 32.4 (8.4–162.8) mL/min/1.73 m2 was not significant.
Considering only the patients who received i.v. steroid therapy after diagnosis, there was also a significant reduction in proteinuria (p < 0.001) from 4.0 ± 3.4 (0.29–12.5) to 0.4 ± 0.5 (0.08–1.7) g/g creatinine after 5 months of follow-up. This subgroup is shown as light blue boxplots in Figure 1.
As shown in Table 4, after 5 months, 25% (5/20) of patients were in complete remission (proteinuria < 0.2 g/g creatinine with normal renal function), 57% (12/21) showed proteinuria > 0.2 g/g creatinine, and 0% (0/21) showed nephrotic range proteinuria. Impaired renal function (eGFR < 90 mL/min/1.73 m2) was present in 50% (10/20). At later follow-up time points, patient numbers declined, but the percentages of proteinuria and impaired GFR did not change substantially.
4. Discussion
Treatment of newly diagnosed IgAN according to the GPN regimen for IgA vasculitis nephritis achieved an improvement in the majority of cases, with a significant reduction in proteinuria 5 months after initiation of therapy. Nonetheless, complete remission was only achieved in 25% of all cases, and additional immunosuppressants were used in six cases (27%). Interestingly, despite worse baseline conditions, eGFR tended to be better in the corticosteroid-treated patient group than in the untreated group during follow-up. After one year, mean eGFR was even significantly better in the treated group (118.6 vs. 86.5 mL/min/1.73 m2, p < 0.05 in Mann–Whitney U test). However, this study has limitations such as the small number of patients, the limited follow-up time, and the loss of some patients during this period. Therefore, it is primarily suitable for representing the short-term response to therapy.
In the clinical setting, it is difficult to use immunosuppressive therapy with known side effects and unclear efficacy if the long-term renal damage is not foreseeable, especially because guidelines are based on insufficient evidence. Therefore, based on the existing literature on IgAN in childhood, we would like to discuss why, whom, and how to treat.
4.1. Why Treat?
Spontaneous remissions of mild IgAN have been described [12] and led to the early assumption that IgAN in childhood is a benign disease. However, progression of IgAN in children to poor outcome (end points end-stage renal disease (ESRD) or decrease in GFR > 50% after more than 4 years of follow-up) was reached in 7.2% [13] and 12.4% [14] in China, 11% in Finland [15], 18.1% in Sweden [16], and 18.5% in Brazil [17]. The onset of the disease in childhood can therefore lead to a significant reduction in quality of life, as it may require renal replacement therapy at young age [18]. Some studies suggest that achieving remission of proteinuria correlates negatively with progression to chronic kidney disease [19] and that an earlier treatment might be beneficial [20,21]. In small randomized controlled pediatric IgAN studies, immunosuppression reduced proteinuria and the development of glomerulosclerosis [22,23]. In our retrospective analysis, immunosuppressive treatment was given in the more severe cases and led to an improvement and to a comparable outcome, as in the clinically and histologically less severe cases.
4.2. Whom to Treat?
In order to identify IgAN patients with poor prognosis already at initial diagnosis, many investigations have been conducted to evaluate corresponding risk factors. Early clinical or pathologic features that bear prognostic significance are summarized in Table 5. While several studies agree on a worse prognosis in older patients [20,24], high proteinuria [13,16,25,26,27] or impaired GFR at the time of diagnosis [16,20,26,27], the pathological results according to the Oxford classification are more controversial in their individual significance. The discordance of the studies can be explained by different inclusion criteria, by the timing of the biopsy (school screening programs in several Asian countries lead to earlier diagnosis and thus milder histopathological changes), by inconsistent outcome criteria, and finally by differences in statistical analysis [28].
Based on the International IgAN Prediction Tool at biopsy for adults, a version adapted to children and adolescents was developed in 2020 that promises to accurately predict the risk of a 30% decrease in GFR or ESRD [29]. The criteria considered were age, gender, race, height, weight, proteinuria, serum creatinine, blood pressure, and MEST score according to Oxford classification, as well as the use of RASB or immunosuppressants at or prior to biopsy. Such developments raise hope for a standardized assessment of pediatric patients and thus guideline-based therapy in the future.
4.3. How to Treat?
The question of how IgAN should be treated is the most controversial. Renoprotective therapy with ACEI or ARB is the basis of any treatment because of its positive effects, not only on hypertension but also on proteinuria and reduction of GFR decline [30]. Its benefits were demonstrated in a randomized placebo-controlled trial (RCT) in children and young people with IgAN (IgACE [31]). A recent review of previous studies [32] found that the use of ACEI and/or ARB in pediatric patients with IgAN appears to be safe and to reduce proteinuria. Nevertheless, it was pointed out that further RCTs with greater methodological rigor and longer follow-up are needed to confidently demonstrate the efficacy and safety of this therapy in a pediatric population.
However, the use of renin-angiotensin system blocking drugs alone does not always show sufficient response. A recent large study in China provides evidence of the benefit from additional immunosuppressive therapy for children with proteinuria ≥ 1 g/day and initial eGFR of >50 mL/min/1.73 m2 [13]. The European VALIGA cohort even suggests that corticosteroids reduce the risk of progression, regardless of initial eGFR and in direct proportion to the extent of proteinuria [33]. Steroids represent the most commonly used form of immunosuppression in IgAN, but the route of steroid administration, dose, and duration of use vary among studies, making comparisons difficult. Steroid pulse therapy, as recommended by the KDIGO guidelines, is discussed as a useful addition for the rapidly progressive glomerulonephritis form of IgAN to achieve faster and more potent efficacy. Furthermore, it may allow a steroid-sparing effect with less cumulative toxicity than sustained oral therapy. Still, the long-term efficacy is uncertain [21].
Other immunosuppressive regimens involve cyclophosphamide [34], azathioprine [22,23], mycophenolate mofetil [35], or tacrolimus [36], but the evidence of their use in children is even more scarce. Lastly, a double-blind, placebo-controlled study comparing vitamin E administration with placebo in children for 1–2 years demonstrated a significant reduction in proteinuria in the vitamin E group, although only mild cases of IgAN were included [37].
In summary, the available published experience suggests that early immunosuppressive therapy might have a beneficial effect on the long-term course of IgAN, at least in severe cases, but sufficiently large studies proving this assumption are outstanding. Our data showing improvement of proteinuria and stabilization of eGFR with an IgAVN treatment protocol and the very similar clinical and histological presentation of acute pediatric IgAN and IgAVN [38,39] may justify the use of the same treatment protocol for both disease entities until more evidence-based treatment protocols are established. Therefore, we suggest unifying treatment protocols for pediatric IgAN and IgAVN, which could also simplify patient recruitment for future prospective studies.
Author Contributions
S.S. and M.P. collected the data, S.S. analyzed the data, and S.S. and M.P. wrote and approved the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
We acknowledge support by the Open Access Publication Fund of the University of Freiburg.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the University of Freiburg (protocol code 22-1059, 15 February 2022).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study over more than 20 years, with the majority of the patients no longer being treated at our institution. In addition, data were collected and saved exclusively at the treating hospital.
Data Availability Statement
Not applicable.
Acknowledgments
We thank C. Schell for his help with the biopsy classification.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lévy, M.; Gonzalez-Burchard, G.; Broyer, M.; Dommergues, J.P.; Foulard, M.; Sorez, J.P.; Habib, R. Berger’s Disease in Children. Natural History and Outcome. Medicine 1985, 64, 157–180. [Google Scholar] [CrossRef] [PubMed]
- Wyatt, R.J.; Kritchevsky, S.B.; Woodford, S.Y.; Miller, P.M.; Roy, S.; Holland, N.H.; Jackson, E.; Bishof, N.A. IgA Nephropathy: Long-Term Prognosis for Pediatric Patients. J. Pediatr. 1995, 127, 913–919. [Google Scholar] [CrossRef]
- Brunner, F.P.; Fassbinder, W.; Broyer, M.; Oulès, R.; Brynger, H.; Rizzoni, G.; Challah, S.; Selwood, N.H.; Dykes, S.R.; Wing, A.J. Survival on Renal Replacement Therapy: Data from the EDTA Registry. Nephrol. Dial. Transplant. 1988, 3, 109–122. [Google Scholar] [PubMed]
- Coppo, R. Treatment of IgA Nephropathy in Children: A Land without KDIGO Guidance. Pediatr. Nephrol. Berl. Ger. 2021, 36, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Rovin, B.H.; Adler, S.G.; Barratt, J.; Bridoux, F.; Burdge, K.A.; Chan, T.M.; Cook, H.T.; Fervenza, F.C.; Gibson, K.L.; Glassock, R.J.; et al. Executive Summary of the KDIGO 2021 Guideline for the Management of Glomerular Diseases. Kidney Int. 2021, 100, 753–779. [Google Scholar] [CrossRef] [PubMed]
- Rovin, B.H.; Adler, S.G.; Barratt, J.; Bridoux, F.; Burdge, K.A.; Chan, T.M.; Cook, H.T.; Fervenza, F.C.; Gibson, K.L.; Glassock, R.J.; et al. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int. 2021, 100, S1–S276. [Google Scholar] [CrossRef] [PubMed]
- Neuhauser, H.; Thamm, M. Blood pressure measurement in the German Health Interview and Examination Survey for Children and Adolescents (KiGGS). Methodology and initial results. Bundesgesundheitsblatt Gesundh. Gesundh. 2007, 50, 728–735. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, G.J.; Muñoz, A.; Schneider, M.F.; Mak, R.H.; Kaskel, F.; Warady, B.A.; Furth, S.L. New Equations to Estimate GFR in Children with CKD. J. Am. Soc. Nephrol. JASN 2009, 20, 629–637. [Google Scholar] [CrossRef] [Green Version]
- Trimarchi, H.; Barratt, J.; Cattran, D.C.; Cook, H.T.; Coppo, R.; Haas, M.; Liu, Z.-H.; Roberts, I.S.D.; Yuzawa, Y.; Zhang, H.; et al. Oxford Classification of IgA Nephropathy 2016: An Update from the IgA Nephropathy Classification Working Group. Kidney Int. 2017, 91, 1014–1021. [Google Scholar] [CrossRef] [Green Version]
- Gesellschaft Für Pädiatrische Nephrologie (GPN); Pohl, M.; Dittrich, K.; Ehrich, J.H.H.; Hoppe, B.; Kemper, M.J.; Klaus, G.; Schmitt, C.P.; Hoyer, P.F. Behandlung der Purpura-Schönlein-Henoch-Nephritis bei Kindern und Jugendlichen: Therapieempfehlungen der Gesellschaft für Pädiatrische Nephrologie (GPN). Monatsschr. Kinderheilkd. 2013, 161, 543–553. [Google Scholar] [CrossRef]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental Algorithms for Scientific Computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shima, Y.; Nakanishi, K.; Hama, T.; Mukaiyama, H.; Togawa, H.; Sako, M.; Kaito, H.; Nozu, K.; Tanaka, R.; Iijima, K.; et al. Spontaneous Remission in Children with IgA Nephropathy. Pediatr. Nephrol. Berl. Ger. 2013, 28, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Fang, X.; Xia, Z.; Gao, C.; Peng, Y.; Li, X.; Zhang, P.; Kuang, Q.; Wang, R.; Wang, M. Long-Term Renal Survival and Undetected Risk Factors of IgA Nephropathy in Chinese Children-a Retrospective 1243 Cases Analysis from Single Centre Experience. J. Nephrol. 2020, 33, 1263–1273. [Google Scholar] [CrossRef] [PubMed]
- Le, W.; Zeng, C.-H.; Liu, Z.; Liu, D.; Yang, Q.; Lin, R.-X.; Xia, Z.-K.; Fan, Z.-M.; Zhu, G.; Wu, Y.; et al. Validation of the Oxford Classification of IgA Nephropathy for Pediatric Patients from China. BMC Nephrol. 2012, 13, 158. [Google Scholar] [CrossRef] [Green Version]
- Ronkainen, J.; Ala-Houhala, M.; Autio-Harmainen, H.; Jahnukainen, T.; Koskimies, O.; Merenmies, J.; Mustonen, J.; Ormälä, T.; Turtinen, J.; Nuutinen, M. Long-Term Outcome 19 Years after Childhood IgA Nephritis: A Retrospective Cohort Study. Pediatr. Nephrol. Berl. Ger. 2006, 21, 1266–1273. [Google Scholar] [CrossRef]
- Halling, S.E.; Soderberg, M.P.; Berg, U.B. Predictors of Outcome in Paediatric IgA Nephropathy with Regard to Clinical and Histopathological Variables (Oxford Classification). Nephrol. Dial. Transplant. 2012, 27, 715–722. [Google Scholar] [CrossRef] [Green Version]
- Fabiano, R.C.G.; Araújo, S.A.; Bambirra, E.A.; Oliveira, E.A.; e Silva, A.C.S.; Pinheiro, S.V.B. The Oxford Classification Predictors of Chronic Kidney Disease in Pediatric Patients with IgA Nephropathy. J. Pediatr. 2017, 93, 389–397. [Google Scholar] [CrossRef]
- Fassbinder, W.; Brunner, F.P.; Brynger, H.; Ehrich, J.H.; Geerlings, W.; Raine, A.E.; Rizzoni, G.; Selwood, N.H.; Tufveson, G.; Wing, A.J. Combined Report on Regular Dialysis and Transplantation in Europe, XX, 1989. Nephrol. Dial. Transplant. 1991, 6 (Suppl. S1), 5–35. [Google Scholar]
- Matsushita, S.; Ishikura, K.; Okamoto, S.; Okuda, Y.; Nagaoka, Y.; Harada, R.; Hamada, R.; Sakai, T.; Hamasaki, Y.; Hataya, H.; et al. Long-Term Morbidity of IgA Nephropathy in Children Evaluated with Newly Proposed Remission Criteria in Japan. Clin. Exp. Nephrol. 2015, 19, 1149–1156. [Google Scholar] [CrossRef]
- Suh, J.-S.; Jang, K.M.; Hyun, H.; Cho, M.H.; Lee, J.H.; Park, Y.S.; Oh, J.H.; Kim, J.H.; Yoo, K.H.; Chung, W.Y.; et al. Remission of Proteinuria May Protect against Progression to Chronic Kidney Disease in Pediatric-Onset IgA Nephropathy. J. Clin. Med. 2020, 9, 2058. [Google Scholar] [CrossRef]
- Cambier, A.; Boyer, O.; Deschenes, G.; Gleeson, J.; Couderc, A.; Hogan, J.; Robert, T. Steroid Therapy in Children with IgA Nephropathy. Pediatr. Nephrol. Berl. Ger. 2020, 35, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, N.; Honda, M.; Iijima, K.; Awazu, M.; Hattori, S.; Nakanishi, K.; Ito, H. Steroid Treatment for Severe Childhood IgA Nephropathy: A Randomized, Controlled Trial. Clin. J. Am. Soc. Nephrol. 2006, 1, 511–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshikawa, N.; Ito, H.; Sakai, T.; Takekoshi, Y.; Honda, M.; Awazu, M.; Ito, K.; Iitaka, K.; Koitabashi, Y.; Yamaoka, K.; et al. A Controlled Trial of Combined Therapy for Newly Diagnosed Severe Childhood IgA Nephropathy. J. Am. Soc. Nephrol. 1999, 10, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Coppo, R.; Lofaro, D.; Camilla, R.R.; Bellur, S.; Cattran, D.; Cook, H.T.; Roberts, I.S.D.; Peruzzi, L.; Amore, A.; Emma, F.; et al. Risk Factors for Progression in Children and Young Adults with IgA Nephropathy: An Analysis of 261 Cases from the VALIGA European Cohort. Pediatr. Nephrol. Berl. Ger. 2017, 32, 139–150. [Google Scholar] [CrossRef]
- Yoshikawa, N.; Ito, H.; Nakamura, H. Prognostic Indicators in Childhood IgA Nephropathy. Nephron 1992, 60, 60–67. [Google Scholar] [CrossRef]
- Mizerska-Wasiak, M.; Małdyk, J.; Turczyn, A.; Cichoń-Kawa, K.; Rybi-Szumińska, A.; Wasilewska, A.; Bieniaś, B.; Zajączkowska, M.; Miklaszewska, M.; Pietrzyk, J.; et al. Predictors of Progression in IgA Nephropathy in Childhood. Adv. Exp. Med. Biol. 2017, 955, 65–73. [Google Scholar] [CrossRef]
- Coppo, R. Clinical and Histological Risk Factors for Progression of IgA Nephropathy: An Update in Children, Young and Adult Patients. J. Nephrol. 2017, 30, 339–346. [Google Scholar] [CrossRef]
- Fabiano, R.C.G.; Pinheiro, S.V.B.; de Almeida Araújo, S.; e Silva, A.C.S. Immunoglobulin a Nephropathy: Pathological Markers of Renal Survival in Paediatric Patients. Nephrology 2016, 21, 995–1002. [Google Scholar] [CrossRef] [Green Version]
- Barbour, S.J.; Coppo, R.; Er, L.; Russo, M.L.; Liu, Z.-H.; Ding, J.; Katafuchi, R.; Yoshikawa, N.; Xu, H.; Kagami, S.; et al. Updating the International IgA Nephropathy Prediction Tool for Use in Children. Kidney Int. 2021, 99, 1439–1450. [Google Scholar] [CrossRef]
- The GISEN Group (Gruppo Italiano Di Studi Epidemiologici in Nefrologia). Randomised Placebo-Controlled Trial of Effect of Ramipril on Decline in Glomerular Filtration Rate and Risk of Terminal Renal Failure in Proteinuric, Non-Diabetic Nephropathy. Lancet 1997, 349, 1857–1863. [Google Scholar] [CrossRef]
- Coppo, R.; Peruzzi, L.; Amore, A.; Piccoli, A.; Cochat, P.; Stone, R.; Kirschstein, M.; Linné, T. IgACE: A Placebo-Controlled, Randomized Trial of Angiotensin-Converting Enzyme Inhibitors in Children and Young People with IgA Nephropathy and Moderate Proteinuria. J. Am. Soc. Nephrol. JASN 2007, 18, 1880–1888. [Google Scholar] [CrossRef] [PubMed]
- De Castro, P.A.S.V.; Bitencourt, L.; Pereira, B.W.S.; Lima, A.Q.R.; Hermida, H.S.; Moreira Neto, C.R.; Mestriner, M.D.; e Silva, A.C.S. Efficacy and Safety of Angiotensin-Converting Enzyme Inhibitors or Angiotensin Receptor Blockers for IgA Nephropathy in Children. Pediatr. Nephrol. Berl. Ger. 2021, 37, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Tesar, V.; Troyanov, S.; Bellur, S.; Verhave, J.C.; Cook, H.T.; Feehally, J.; Roberts, I.S.D.; Cattran, D.; Coppo, R.; VALIGA study of the ERA-EDTA Immunonephrology Working Group. Corticosteroids in IgA Nephropathy: A Retrospective Analysis from the VALIGA Study. J. Am. Soc. Nephrol. JASN 2015, 26, 2248–2258. [Google Scholar] [CrossRef] [Green Version]
- Jiang, X.-Y.; Mo, Y.; Sun, L.-Z.; Yue, Z.-H.; Chen, S.-M.; Wu, W. Efficacy of Methylprednisolone, Cyclophosphamide in Pediatric IgA Nephropathy Assessed by Renal Biopsy. Clin. Nephrol. 2009, 71, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Hogg, R.J.; Bay, R.C.; Jennette, J.C.; Sibley, R.; Kumar, S.; Fervenza, F.C.; Appel, G.; Cattran, D.; Fischer, D.; Hurley, R.M.; et al. Randomized Controlled Trial of Mycophenolate Mofetil in Children, Adolescents, and Adults with IgA Nephropathy. Am. J. Kidney Dis. 2015, 66, 783–791. [Google Scholar] [CrossRef]
- Zhang, J.-J.; Wang, Q.; Dou, W.-J.; Jia, L.-M.; Zhang, L.; Cheng, Y.-B.; Tan, W.-X.; Zhao, F. Clinical effect of tacrolimus combined with glucocorticoid in the treatment of IgA nephropathy in children. Zhongguo Dang Dai Er Ke Za Zhi Chin. J. Contemp. Pediatr. 2019, 21, 265–270. [Google Scholar]
- Chan, J.C.M.; Mahan, J.D.; Trachtman, H.; Scheinman, J.; Flynn, J.T.; Alon, U.S.; Lande, M.B.; Weiss, R.A.; Norkus, E.P. Vitamin E Therapy in IgA Nephropathy: A Double-Blind, Placebo-Controlled Study. Pediatr. Nephrol. 2003, 18, 1015–1019. [Google Scholar] [CrossRef] [PubMed]
- Davin, J.C.; Ten Berge, I.J.; Weening, J.J. What Is the Difference between IgA Nephropathy and Henoch-Schönlein Purpura Nephritis? Kidney Int. 2001, 59, 823–834. [Google Scholar] [CrossRef] [Green Version]
- Oh, H.J.; Ahn, S.V.; Yoo, D.E.; Kim, S.J.; Shin, D.H.; Lee, M.J.; Kim, H.R.; Park, J.T.; Yoo, T.-H.; Kang, S.-W.; et al. Clinical Outcomes, When Matched at Presentation, Do Not Vary between Adult-Onset Henöch-Schönlein Purpura Nephritis and IgA Nephropathy. Kidney Int. 2012, 82, 1304–1312. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Follow-up data for five points in time: (a) urine protein to creatinine ratio (P/C) in g/g; (b) eGFR (mL/min/1.73 m2). The blue lines represent patients who received i.v. corticosteroid therapy, and the orange lines represent those without. The boxplots below show the data for all patients (dark blue) and for the proportion of patients who received i.v. corticosteroids (light blue). The box-plot outliers are represented by the symbol “+”.
Figure 1.
Follow-up data for five points in time: (a) urine protein to creatinine ratio (P/C) in g/g; (b) eGFR (mL/min/1.73 m2). The blue lines represent patients who received i.v. corticosteroid therapy, and the orange lines represent those without. The boxplots below show the data for all patients (dark blue) and for the proportion of patients who received i.v. corticosteroids (light blue). The box-plot outliers are represented by the symbol “+”.


{kind=link}
Table 1.
Symptom onset and renal biopsy.
| Patients | n = 22 |
|---|---|
| Gender | 14 (64%) males, 8 (36%) females |
| Age at first symptoms | 10.2 ± 3.7 (3.5–15.5) |
| Age at biopsy | 11.0 ± 3.5 (3.5–15.5) |
| Time to biopsy | 41 weeks ± 115 weeks (2 days–10 years) |
| Clinical findings | |
| Hematuria | 7 (32%) micro-, 15 (68%) macrohematuria |
| Hypertension | 11 (50%) |
| Laboratory findings | (at biopsy) |
| Creatinine (mg/dL) | 1.5 ± 1.8 (0.18–7.8) |
| eGFR (mL/min/1.73 m2) | 81.3 ± 49.7 (8.9–229.4) |
| eGFR < 60 mL/min/1.73 m2 | 7/22 (32%) |
| IgA (mg/dL) | 234.5 ± 126.2 (98–649) |
| Urine protein to creatinine ratio | 3.2 ± 3.7 g/g (0.29–12.5) |
| UPCR > 3.5 g/g creatinine | 9/22 (41%) |
| Kidney biopsy | |
| M1 | 15 (68%) |
| E1 | 12 (55%) |
| S1 | 14 (64%) |
| T1 | 1 (5%) |
| Crescents (C1) | 13 (59%) |
Table 2.
Treatment.
| Treatment | Number (%) |
|---|---|
| ACE inhibitors/ARB | 21 (95%) |
| Corticosteroid therapy (i.v. + oral) | 14 (64%) |
| Immunosuppressants | 6 (27%) |
| Plasmapheresis and/or hemodialysis | 2 (9%) |
| Transplantation | 1 (5%) |
| Treatment combinations | |
| ACEI/ARB alone | 6 (27%) |
| ACEI/ARB + CS | 9 (41%) |
| ACEI/ARB + CS + IS | 4 (18%) |
| ACEI/ARB + CS + IS + HD | 1 (5%) |
| ACEI/ARB + CS + IS + HD + PP + RT | 1 (5%) |
ACEI = angiotensin converter enzyme inhibitor, ARB = angiotensin receptor blocker, CS = corticosteroid therapy, IS = immunosuppressants, HD = hemodialysis, PP = plasmapheresis, RT = renal transplant.
Table 3.
Follow-up data.
| At Biopsy n = 22 | 4 Weeks after Treatment n = 18 | After 5 Months n = 20 | After 1 Year n = 14 | After 2–3 Years n = 14 | Last Follow-Up * n = 10 | |
|---|---|---|---|---|---|---|
| Creatinine | 1.5 ± 1.8 | 1.1 ± 1.4 | 1.0 ± 1.5 | 0.6 ± 0.2 | 0.7 ± 0.2 | 0.9 ± 0.2 |
| (mg/dL) | (0.18–7.8) | (0.32–6.13) | (0.26–7.51) | (0.29–1.04) | (0.3–1.1) | (0.49–1.2) |
| eGFR | 81.3 ± 49.7 | 87.8 ± 37.1 | 92.7 ± 32.4 | 107.1 ± 28.8 | 96.6 ± 26.4 | 86.4 ± 19.4 |
| (mL/min/1.73 m2) | (8.9–229.4) | (10.5–139.4) | (8.4–162.8) | (56.0–155.3) | (57.1–156.0) | (57.2–130.2) |
| Proteinuria | 3.2 ± 3.7 | 2.5 ± 2.6 | 0.5 ± 0.6 | 0.4 ± 0.5 | 0.6 ± 0.9 | 0.4 ± 0.41 |
| (g/g creatinine) | (0.29–12.5) | (0.09–8.47) | (0.08–2.1) | (0.06–1.84) | (0.06–3.17) | (0.08–1.13) |
* Patients who were followed for more than 3.5 years, mean value 5.8 years.
Table 4.
Outcome.
| No. of Patients with… | At Biopsy | After 4 Weeks | After 5 Months | After 1 Year | After 2–3 Years | Last Follow-Up * |
|---|---|---|---|---|---|---|
| Proteinuria > 0.2 g/g | 22/22 (100%) | 14/18 (78%) | 12/21 (57%) | 9/15 (60%) | 8/15 (53%) | 6/10 (60%) |
| Proteinuria > 3.5 g/g | 9/22 (41%) | 6/18 (33%) | 0/21 (0%) | 0/15 (0%) | 0/15 (0%) | 0/10 (0%) |
| eGFR < 90 mL/min/1.73 m2 | 13/22 (59%) | 9/18 (50%) | 10/20 (50%) | 5/14 (36%) | 7/14 (50%) | 5/10 (50%) |
* Patients who were followed for more than 3.5 years, mean value 5.8 years.
Table 5.
Prognostic factors in pediatric IgAN.
| Study | Factors Associated with Poor Prognosis |
|---|---|
| Yoshikawa et al. 1992 [25] (200 patients, Japan) |
|
| Halling et al. 2012 [16] (99 patients, Sweden) |
|
| Mizerska et al. 2017 [26] (55 patients, Poland) |
|
| Coppo et al. 2017 [24] (261 patients < 23 y, VALIGA European cohort) |
|
| Suh et al. 2020 [20] (1154 patients, Korea) |
|
| Wu et al. 2020 [13] (1243 patients, China) |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Schroda, S.; Pohl, M. Management of IgA Nephropathy in Pediatric Patients. Children 2022, 9, 653. https://doi.org/10.3390/children9050653
AMA Style
Schroda S, Pohl M. Management of IgA Nephropathy in Pediatric Patients. Children. 2022; 9(5):653. https://doi.org/10.3390/children9050653
Chicago/Turabian StyleSchroda, Sophie, and Martin Pohl. 2022. "Management of IgA Nephropathy in Pediatric Patients" Children 9, no. 5: 653. https://doi.org/10.3390/children9050653
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.