
Illness Characteristics of COVID-19 in Children Infected with the SARS-CoV-2 Delta Variant

 , , , ,
, , , ,  and add
Show full author list
and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study and Public Involvement
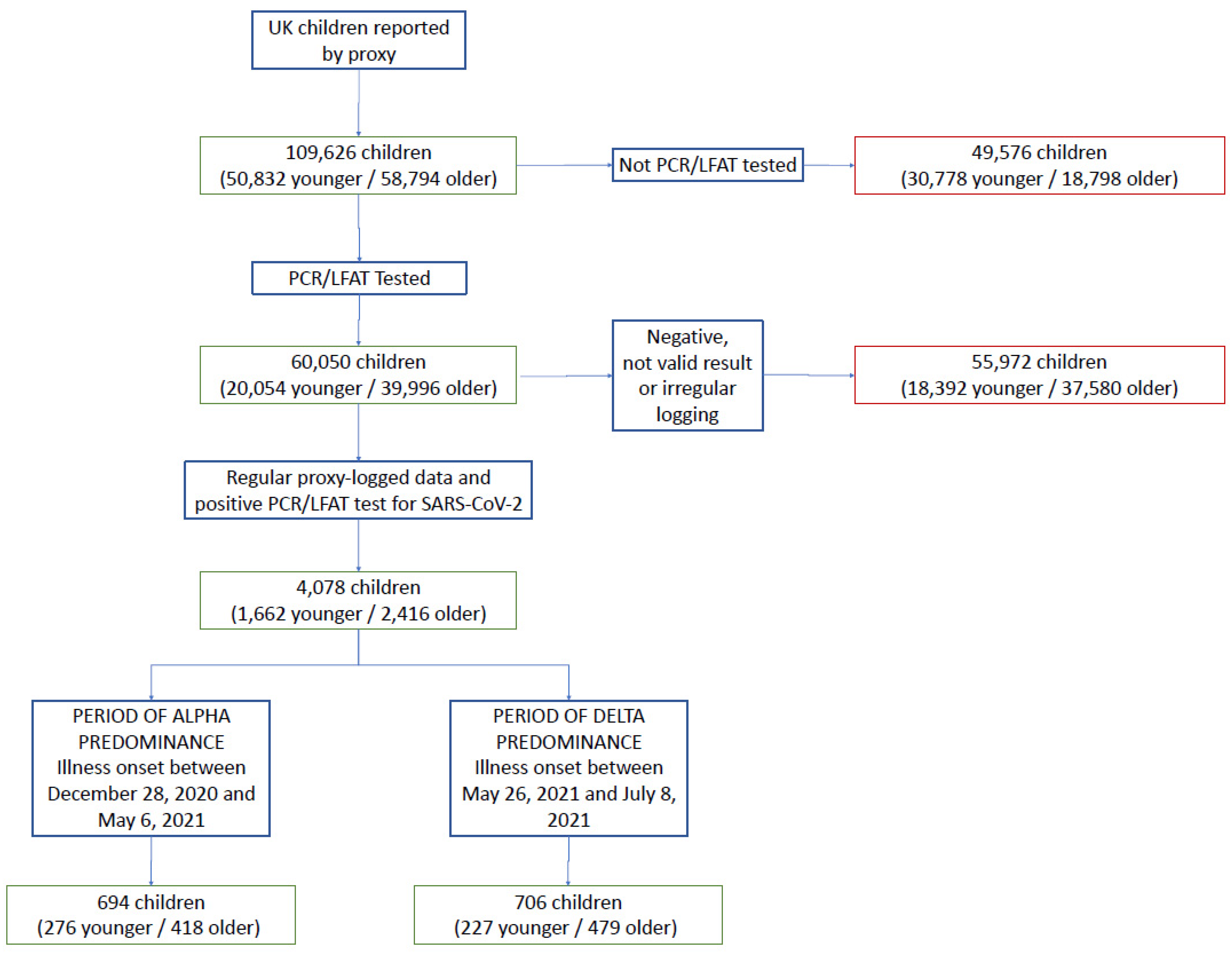
2.2. Participants
2.3. Data Analysis
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CI | Confidence interval |
| COVID-19 | Coronavirus disease 2019 |
| FDR | False discovery rate |
| IQR | Interquartile range |
| KCL | King’s College London |
| LFAT | Lateral flow antigen test |
| ONS | Office for National Statistics (UK) |
| PCR | Polymerase chain reaction |
| SARS-CoV-2 | Severe acute respiratory syndrome-related coronavirus 2 |
| UK | United Kingdom of Great Britain and Northern Ireland |
| USA | United States of America |
| WHO | World Health Organization |
References
- Forni, D.; Cagliani, R.; Pontremoli, C.; Clerici, M.; Sironi, M. The Substitution Spectra of Coronavirus Genomes. Brief. Bioinform. 2021, 23, bbab382. [Google Scholar] [CrossRef] [PubMed]
- Forni, D.; Cagliani, R.; Pontremoli, C.; Mozzi, A.; Pozzoli, U.; Clerici, M.; Sironi, M. Antigenic Variation of SARS-CoV-2 in Response to Immune Pressure. Mol. Ecol. 2021, 30, 3548–3559. [Google Scholar] [CrossRef]
- Anastassopoulou, C.; Gkizarioti, Z.; Patrinos, G.P.; Tsakris, A. Human Genetic Factors Associated with Susceptibility to SARS-CoV-2 Infection and COVID-19 Disease Severity. Hum. Genom. 2020, 14, 40. [Google Scholar] [CrossRef]
- Fan, W.; Mar, K.B.; Sari, L.; Gaszek, I.K.; Cheng, Q.; Evers, B.M.; Shelton, J.M.; Wight-Carter, M.; Siegwart, D.J.; Lin, M.M.; et al. TRIM7 Inhibits Enterovirus Replication and Promotes Emergence of a Viral Variant with Increased Pathogenicity. Cell 2021, 184, 3410–3425.e17. [Google Scholar] [CrossRef]
- Chen, H.L.; Lin, S.R.; Liu, H.F.; King, C.C.; Hsieh, S.C.; Wang, W.K. Evolution of Dengue Virus Type 2 during Two Consecutive Outbreaks with an Increase in Severity in Southern Taiwan in 2001–2002. Am. J. Trop. Med. Hyg. 2008, 79, 495–505. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, W.G. Impact of Virus Genetic Variability and Host Immunity for the Success of COVID-19 Vaccines. Biomed. Pharmacother. 2021, 136, 111272. [Google Scholar] [CrossRef] [PubMed]
- Planas, D.; Veyer, D.; Baidaliuk, A.; Staropoli, I.; Guivel-Benhassine, F.; Rajah, M.M.; Planchais, C.; Porrot, F.; Robillard, N.; Puech, J.; et al. Reduced Sensitivity of SARS-CoV-2 Variant Delta to Antibody Neutralization. Nature 2021, 596, 276–280. [Google Scholar] [CrossRef]
- Luo, C.H.; Morris, C.P.; Sachithanandham, J.; Amadi, A.; Gaston, D.; Li, M.; Swanson, N.J.; Schwartz, M.; Klein, E.Y.; Pekosz, A.; et al. Infection with the SARS-CoV-2 Delta Variant Is Associated with Higher Infectious Virus Loads Compared to the Alpha Variant in Both Unvaccinated and Vaccinated Individuals. medRxiv, 2021; Preprint. [Google Scholar]
- Twohig, K.A.; Nyberg, T.; Zaidi, A.; Thelwall, S.; Sinnathamby, M.A.; Aliabadi, S.; Seaman, S.R.; Harris, R.J.; Hope, R.; Lopez-Bernal, J.; et al. Hospital Admission and Emergency Care Attendance Risk for SARS-CoV-2 Delta (B.1.617.2) Compared with Alpha (B.1.1.7) Variants of Concern: A Cohort Study. Lancet Infect. Dis. 2021, 22, 35–42. [Google Scholar] [CrossRef]
- Ong, S.W.X.; Chiew, C.J.; Ang, L.W.; Mak, T.-M.; Cui, L.; Toh, M.P.H.S.; Lim, Y.D.; Lee, P.H.; Lee, T.H.; Chia, P.Y.; et al. Clinical and Virological Features of SARS-CoV-2 Variants of Concern: A Retrospective Cohort Study Comparing B.1.1.7 (Alpha), B.1.315 (Beta), and B.1.617.2 (Delta). Clin. Infect. Dis. 2021; Online ahead of print. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of Covid-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef]
- Antonelli, M.; Penfold, R.S.; Merino, J.; Sudre, C.H.; Molteni, E.; Berry, S.; Canas, L.S.; Graham, M.S.; Klaser, K.; Modat, M.; et al. Risk Factors and Disease Profile of Post-Vaccination SARS-CoV-2 Infection in UK Users of the COVID Symptom Study App: A Prospective, Community-Based, Nested, Case-Control Study. Lancet Infect. Dis. 2021, 22, 43–55. [Google Scholar] [CrossRef]
- Molteni, E.; Sudre, C.H.; Canas, L.S.; Bhopal, S.S.; Hughes, R.C.; Antonelli, M.; Murray, B.; Kläser, K.; Kerfoot, E.; Chen, L.; et al. Illness Duration and Symptom Profile in Symptomatic UK School-Aged Children Tested for SARS-CoV-2. Lancet Child Adolesc. Health 2021, 5, 708–718. [Google Scholar] [CrossRef]
- Struyf, T.; Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Leeflang, M.M.G.; Spijker, R.; Hooft, L.; Emperador, D.; Domen, J.; et al. Signs and Symptoms to Determine If a Patient Presenting in Primary Care or Hospital Outpatient Settings Has COVID-19. Cochrane Database Syst. Rev. 2021, 2021, CD013665. [Google Scholar]
- Sudre, C.; Murray, B.; Varsavsky, T.; Graham, M.; Penfold, R.; Bowyer, R.; Pujol, J.; Klaser, K.; Antonelli, M.; Canas, L.; et al. Attributes and Predictors of Long COVID. Nat. Med. 2021, 10, 626–631. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Galván Casas, C.; Català, A.; Carretero Hernández, G.; Rodríguez-Jiménez, P.; Fernández-Nieto, D.; Rodríguez-Villa Lario, A.; Navarro Fernández, I.; Ruiz-Villaverde, R.; Falkenhain-López, D.; Llamas Velasco, M.; et al. Classification of the Cutaneous Manifestations of COVID-19: A Rapid Prospective Nationwide Consensus Study in Spain with 375 Cases. Br. J. Dermatol. 2020, 183, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Hospitalizations Associated with COVID-19 Among Children and Adolescents—COVID-NET, 14 States, March 1, 2020–August 14, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1255–1260. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, Risk of Hospital Admission, and Vaccine Effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Veneti, L.; Salamanca, B.V.; Seppälä, E.; Starrfelt, J.; Storm, M.L.; Bragstad, K.; Hungnes, O.; Bøås, H.; Kvåle, R.; Vold, L.; et al. No Difference in Risk of Hospitalisation between Reported Cases of the SARS-CoV-2 Delta Variant and Alpha Variant in Norway. Int. J. Infect. Dis. 2022, 115, 178–184. [Google Scholar] [CrossRef]
- Kim, T.Y.; Kim, E.C.; Agudelo, A.Z.; Friedman, L. COVID-19 Hospitalization Rate in Children across a Private Hospital Network in the United States: COVID-19 Hospitalization Rate in Children. Arch. Pediatr. 2021, 28, 530–532. [Google Scholar] [CrossRef] [PubMed]
- Canas, L.S.; Österdahl, M.F.; Deng, J.; Hu, C.; Selvachandran, S.; Polidori, L.; May, A.; Molteni, E.; Murray, B.; Chen, L.; et al. Disentangling Post-Vaccination Symptoms from Early COVID-19. EClinicalMedicine 2021, 42, 101212. [Google Scholar] [CrossRef]
- Molteni, E.; Sudre, C.H.; Canas, L.S.; Bhopal, S.S.; Hughes MPH MB ChB, R.C.; Chen, L.; Deng, J.; Murray, B.; Kerfoot, E.; Antonelli, M.; et al. Illness Characteristics of COVID-19 in Children Infected with the SARS-CoV-2 Delta Variant. medRxiv, 2021; Preprint. [Google Scholar] [CrossRef]
- Canas, L.S.; Sudre, C.H.; Capdevila Pujol, J.; Polidori, L.; Murray, B.; Molteni, E.; Graham, M.S.; Klaser, K.; Antonelli, M.; Berry, S.; et al. Early Detection of COVID-19 in the UK Using Self-Reported Symptoms: A Large-Scale, Prospective, Epidemiological Surveillance Study. Lancet Digit. Health 2021, 3, e587–e598. [Google Scholar] [CrossRef]
- Howard, L.M.; Garguilo, K.; Gillon, J.; LeBlanc, K.; Seegmiller, A.C.; Schmitz, J.E.; Byrne, D.W.; Domenico, H.J.; Moore, R.P.; Webber, S.A.; et al. The First 1000 Symptomatic Pediatric SARS-CoV-2 Infections in an Integrated Health Care System: A Prospective Cohort Study. BMC Pediatr. 2021, 21, 403. [Google Scholar] [CrossRef] [PubMed]
- Thelwall, S.; Aiano, F.; Harman, K.; Dabrera, G.; Ladhani, S.N. Risk of Hospitalisation and Death in Children with SARS-CoV-2 Delta (B.1.612.2) Infection. Lancet Child Adolesc. Health 2022, 6, e16–e17. [Google Scholar] [CrossRef]
- Varsavsky, T.; Graham, M.S.; Canas, L.S.; Ganesh, S.; Capdevila Pujol, J.; Sudre, C.H.; Murray, B.; Modat, M.; Jorge Cardoso, M.; Astley, C.M.; et al. Detecting COVID-19 Infection Hotspots in England Using Large-Scale Self-Reported Data from a Mobile Application: A Prospective, Observational Study. Lancet Public Health 2021, 6, e21–e29. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall Symptomatic Children with Positive SARS-CoV-2 Test | ||||||
|---|---|---|---|---|---|---|
| Alpha Variant Period | Delta Variant Period | |||||
| Younger Children (Aged 5–11 Years) | Older Children (Aged 12–17 Years) | Overall Cohort (Aged 5–17 Years) | Younger Children (Aged 5–11 Years) | Older Children (Aged 12–17 Years) | Overall Cohort (Aged 5–17 Years) | |
| Number | 276 | 418 | 694 | 227 | 479 | 706 |
| Males (n (%)) | 144 (52.2) | 213 (50.9) | 357 (51.4) | 102 (44.9) | 255 (53.2) | 357 (50.6) |
| Age, years (median (IQR)) | 9 (7–10) | 15 (13–16) | 12 (9–15) | 9 (8–11) | 15 (13–16) | 14 (13–16) |
| BMI (kg/m2) (median (IQR)) | 16.44 (14.79–18.90) | 19.53 (17.24–22.07) | 18.16 (15.97–21.16) | 16.68 (14.61–19.27) | 18.97 (16.88–21.31) | 18.21 (16.01–20.96) |
| Asthma (n (%)) | 32 (11.6) | 49 (11.7) | 81 (11.6) | 24 (10.6) | 56 (11.7) | 80 (11.3) |
| Heart disease (n (%)) | 0 (0.0) | 3 (0.9) | 3 (0.4) | 2 (0.7) | 1 (0.2) | 3 (0.4) |
| Diabetes (n (%)) | 1 (0.4) | 4 (1.0) | 5 (0.8) | 1 (0.4) | 1 (0.2) | 2 (0.3) |
| Renal disease (n (%)) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.2) | 4 (0.1) |
| Number of children presenting to hospital * (n (%)) | 6 (2.2) | 8 (1.9) | 14 (2.0) | 8 (3.5) | 8 (1.7) | 16 (2.2) |
| Illness duration (median (IQR)) | 4 (2–8) | 6 (3–10) | 5 (2–9.75) | 4 (2–7.5) | 6 (3–10) | 5 (2–9) |
| Number of symptoms in the first week (median (IQR)) | 3 (2–5) | 5 (3–7) | 4 (2–6) | 4 (2–6) | 6 (3–9) | 5 (3–8) |
| Number of children with illness duration ≥ 28 days (n (%)) | 2 (0.7) | 10 (2.4) | 14 (1.7) | 3 (1.3) | 12 (2.5) | 15 (2.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molteni, E.; Sudre, C.H.; Canas, L.D.S.; Bhopal, S.S.; Hughes, R.C.; Chen, L.; Deng, J.; Murray, B.; Kerfoot, E.; Antonelli, M.; et al. Illness Characteristics of COVID-19 in Children Infected with the SARS-CoV-2 Delta Variant. Children 2022, 9, 652. https://doi.org/10.3390/children9050652
Molteni E, Sudre CH, Canas LDS, Bhopal SS, Hughes RC, Chen L, Deng J, Murray B, Kerfoot E, Antonelli M, et al. Illness Characteristics of COVID-19 in Children Infected with the SARS-CoV-2 Delta Variant. Children. 2022; 9(5):652. https://doi.org/10.3390/children9050652
Chicago/Turabian StyleMolteni, Erika, Carole H. Sudre, Liane Dos Santos Canas, Sunil S. Bhopal, Robert C. Hughes, Liyuan Chen, Jie Deng, Benjamin Murray, Eric Kerfoot, Michela Antonelli, and et al. 2022. "Illness Characteristics of COVID-19 in Children Infected with the SARS-CoV-2 Delta Variant" Children 9, no. 5: 652. https://doi.org/10.3390/children9050652