
Understanding the Mechanisms through Which Family Risk Affects Adolescent Mental Health: A Model of Multisystemic Resilience in Context

 , , and
, , and
Abstract
:1. Introduction
1.1. Family Risk, Parenting, and Adolescent Conduct Difficulties
1.2. Peer Support and Adolescent Resilience to Conduct Difficulties
1.3. Appreciation for Community Traditions and Adolescent Resilience to Conduct Difficulties
1.4. Family Risk and Adolescent Resilience to Conduct Difficulties
1.4.1. The Canadian Context
1.4.2. The South African Context
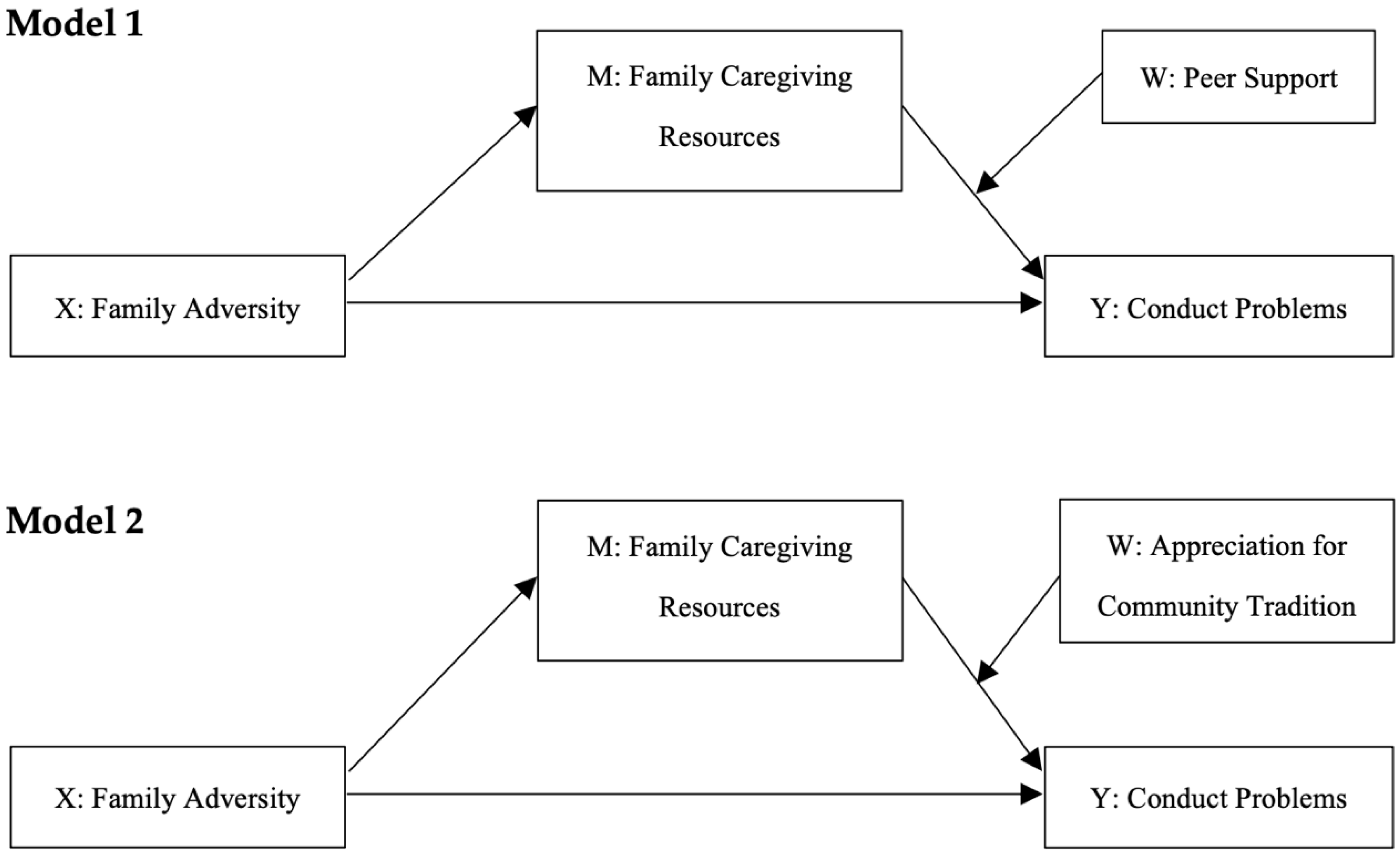
1.5. The Present Study
2. Materials and Methods
2.1. Procedure
2.2. Participants
2.2.1. Canada
2.2.2. South Africa
2.3. Measures
2.3.1. Family Adversity
2.3.2. Family Caregiving
2.3.3. Peer Support
2.3.4. Appreciation for Community Traditions
2.3.5. Conduct Problems
2.3.6. Sociodemographic Characteristics
2.4. Statistical Analysis
2.4.1. Model Estimation
2.4.2. Model Inference
3. Results
3.1. Descriptive Analysis CA and SA Samples
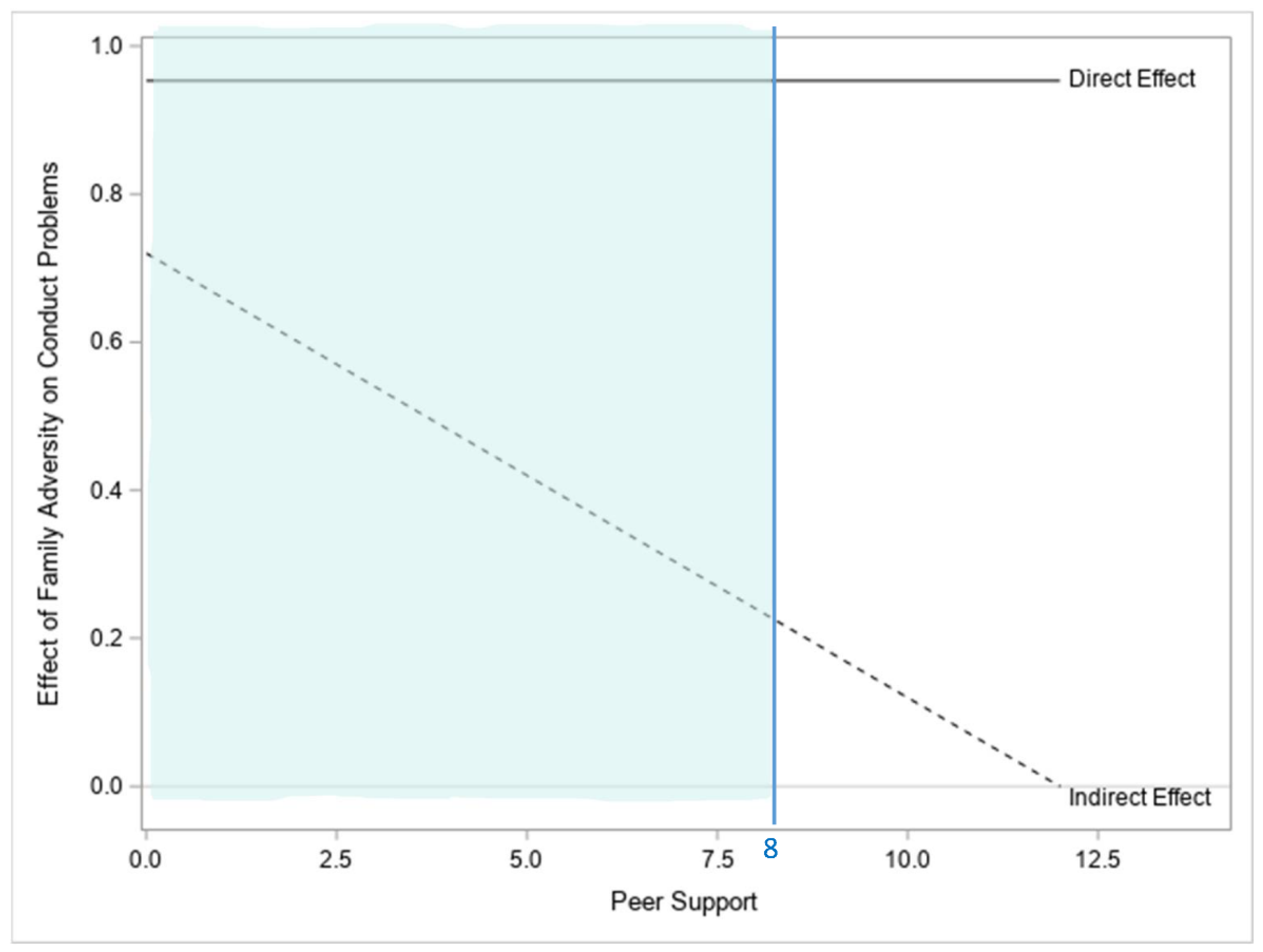
3.2. Model 1
3.2.1. Canada
3.2.2. South Africa
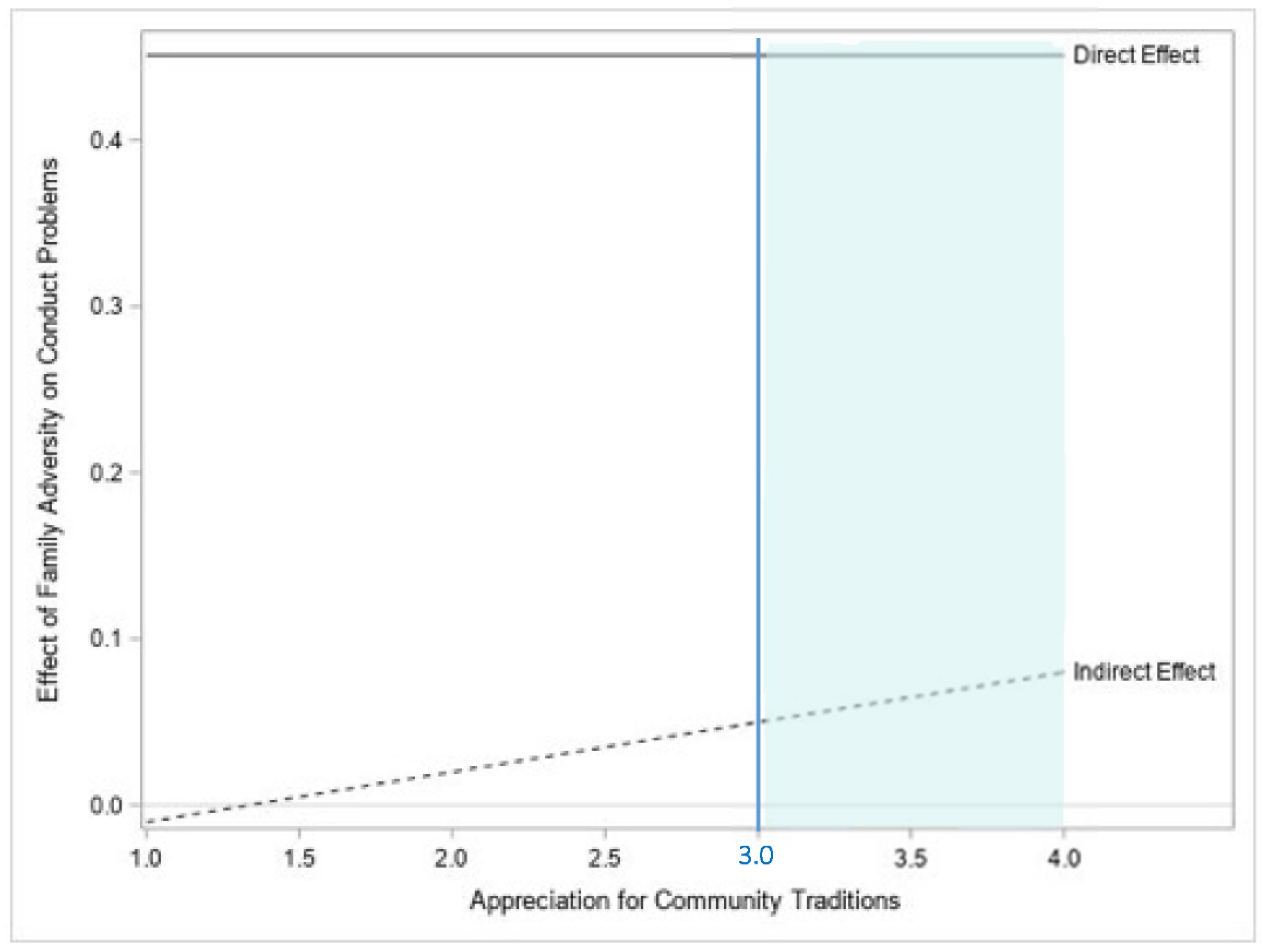
3.3. Model 2
3.3.1. Canada
3.3.2. South Africa
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Danielson, M.L.; Bitsko, R.H.; Holbrook, J.R.; Charania, S.N.; Claussen, A.H.; McKeown, R.E.; Cuffe, S.P.; Owens, J.S.; Evans, S.W.; Kubicek, L.; et al. Community-based prevalence of externalizing and internalizing disorders among school-aged children and adolescents in four geographically dispersed school districts in the United States. Child Psychiatry Hum. Dev. 2021, 52, 500–514. [Google Scholar] [CrossRef] [PubMed]
- Polanczyk, G.V.; Salum, G.A.; Sugaya, L.S.; Caye, A.; Rohde, L.A. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J. Child Psychol. Psychiatry 2015, 56, 345–365. [Google Scholar] [CrossRef] [PubMed]
- Fairchild, G.; Hawes, D.J.; Frick, P.J.; Copeland, W.E.; Odgers, C.L.; Franke, B.; Freitag, C.M.; De Brito, S.A. Conduct disorder. Nat. Rev. Dis. Primers 2019, 5, 1–25. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Frick, P.J. Current research on conduct disorder in children and adolescents: State of the science. S. Afr. J. Psychol. 2016, 46, 160–174. [Google Scholar] [CrossRef]
- Dodge, K.A.; Pettit, G.S. A biopsychosocial model of the development of chronic conduct problems in adolescence. Dev. Psychol. 2003, 39, 349. [Google Scholar] [CrossRef]
- Bevilacqua, L.; Kelly, Y.; Heilmann, A.; Priest, N.; Lacey, R.E. Adverse childhood experiences and trajectories of internalizing, externalizing, and prosocial behaviors from childhood to adolescence. Child Abus. Negl. 2021, 112, 104890. [Google Scholar] [CrossRef]
- Burkey, M.D.; Hosein, M.; Morton, I.; Purgato, M.; Adi, A.; Kurzrok, M.; Kohrt, B.A.; Tol, W.A. Psychosocial interventions for disruptive behaviour problems in children in low- and middle-income countries: A systematic review and meta-analysis. J. Child Psychol. Psychiatry 2018, 59, 982–993. [Google Scholar] [CrossRef]
- Evans, E.A.; Goffa, S.L.; Upchurchb, D.M.; Grellac, C.E. Childhood adversity and mental health comorbidity in men and women with opioid use disorder. Addict. Behave. 2020, 102, 106149. [Google Scholar] [CrossRef]
- Guarnaccia, C.; De Vita, E.; Sortino, L.; Giannone, F. Links between adverse childhood experiences, psychopathological symptoms and recidivism risk in juvenile delinquents. Eur. J. Criminol. 2020. [Google Scholar] [CrossRef]
- Samek, D.R.; Hicks, B.M. Externalizing disorders and environmental risk: Mechanisms of gene-environment interplay and strategies for intervention. Clin. Pract. 2014, 11, 537–547. [Google Scholar] [CrossRef] [Green Version]
- Levenson, J.S.; Socia, K.M. Adverse childhood experiences and arrest patterns in a sample of sex offenders. J. Interpers. Violence 2016, 31, 1883–1911. [Google Scholar] [CrossRef] [PubMed]
- Masten, A.S. Ordinary Magic: Resilience in Development; The Guilford Press: New York, NY, USA, 2014. [Google Scholar]
- Ungar, M. Designing resilience research: Using multiple methods to investigate risk exposure, promotive and protective processes, and contextually relevant outcomes for children and youth. Child Abus. Negl. 2019, 96, 104098. [Google Scholar] [CrossRef] [PubMed]
- Labella, M.H.; Masten, A.S. Family influences on the development of aggression and violence. Curr. Opin. Psyc. 2018, 19, 11–16. [Google Scholar] [CrossRef]
- Ungar, M.; Theron, L.; Murphy, K.; Jefferies, P. Researching multisystemic resilience: A sample methodology. Front. Psychol. 2021, 11, 607994. [Google Scholar] [CrossRef] [PubMed]
- Cox, R.S.; Irwin, P.; Scannell, L.; Ungar, M.; Bennett, T.D. Children and youth’s biopsychosocial wellbeing in the context of energy resource activities. Environ. Res. 2017, 158, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Höltge, J.; Theron, L.; Jefferies, P.; Ungar, M. Family resilience in a resource-cursed community dependent on the oil and gas industry. Fam. Process 2021, 60, 1453–1469. [Google Scholar] [CrossRef] [PubMed]
- Ungar, M.; Theron, L. Resilience and mental health: How multisystemic processes contribute to positive outcomes. Lancet Psychiatry 2020, 7, 441–448. [Google Scholar] [CrossRef]
- Masten, A.S.; Lucke, C.M.; Nelson, K.M.; Stallworthy, I.C. Resilience in development and psychopathology: Multisystem perspectives. Annu. Rev. Clin. Psychol. 2021, 17, 521–549. [Google Scholar] [CrossRef]
- Madrid Akpovo, S.; Nganga, L.; Acharya, D. Minority-world preservice teachers’ understanding of contextually appropriate practice while working in majority-world early childhood contexts. J. Res. Child Ed. 2018, 32, 202–218. [Google Scholar] [CrossRef]
- World Health Organization [WHO]. Access to Mental Health and Psychosocial Support Services Remains Unequal for Children and Adolescents in Africa, alert UNICEF & WHO. 2021. Available online: https://www.afro.who.int/news/access-mental-health-and-psychosocial-support-services-remains-unequal-children-and (accessed on 21 March 2022).
- Labella, M.H.; Narayan, A.J.; McCormick, C.M.; Desjardins, C.D.; Masten, A.S. Risk and adversity, parenting quality, and children’s socio-emotional adjustment in families experiencing homelessness. Child Dev. 2019, 90, 227–244. [Google Scholar] [CrossRef] [Green Version]
- Scully, C.; McLaughlin, J.; Fitzgerald, A. The relationship between adverse childhood experiences, family functioning, and mental health problems among children and adolescents: A systematic review. J. Fam. Ther. 2020, 42, 291–316. [Google Scholar] [CrossRef]
- Appleyard, K.; Egeland, B.; van Dulmen, M.H.; Alan Sroufe, L. When more is not better: The role of cumulative risk in child behavior outcomes. J. Child Psychol. Psychiatry 2005, 46, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Baglivio, M.T.; Epps, N.; Swartz, K.; Huq, M.S.; Sheer, A.; Hardt, N.S. The prevalence of adverse childhood experiences (ACE) in the lives of juvenile offenders. J. Juv. Justice 2014, 3, 1–23. [Google Scholar]
- Conger, R.D.; Donnellan, M.B. An interactionist perspective on the socioeconomic context of human development. Annu. Rev. Psychol. 2007, 10, 175–199. [Google Scholar] [CrossRef] [Green Version]
- Shuey, E.A.; Leventhal, T. Neighborhoods and parenting. In Handbook of Parenting, 3rd ed.; Bornstein, M.H., Ed.; Routledge: London, UK, 2019; Volume 2, pp. 371–399. [Google Scholar]
- Simons, L.G.; Wickrama, K.A.S.; Lee, T.K.; Landers-Potts, M.; Cutrona, C.; Conger, R.D. Testing family stress and family investment explanations for conduct problems among African American adolescents. J. Marriage Fam. 2016, 78, 498–515. [Google Scholar] [CrossRef]
- Grogan-Kaylor, A.; Galano, M.M.; Stein, S.F.; Clark, H.M.; Graham-Bermann, S.A. Latent profiles of parenting among women exposed to intimate partner violence. Soc. Work. Res. 2020, 44, 33–46. [Google Scholar] [CrossRef]
- Miller-Graff, L.E.; Cater, Å.K.; Howell, K.H.; Graham-Bermann, S.A. Parent–child warmth as a potential mediator of childhood exposure to intimate partner violence and positive adulthood functioning. Anxiety Stress Coping 2016, 29, 259–273. [Google Scholar] [CrossRef]
- Nwabuzor Ogbonnaya, I.; Keeney, A.J.; Villodas, M.T. The role of co-occurring intimate partner violence, alcohol use, drug use, and depressive symptoms on disciplinary practices of mothers involved with child welfare. Child Abus. Negl. 2019, 90, 76–87. [Google Scholar] [CrossRef]
- Rosser-Limiñana, A.; Suriá-Martínez, R.; Pérez, M.A.M. Children exposed to intimate partner violence: Association among battered mothers’ parenting competences and children’s behavior. Int. J. Environ. Res. Public Health 2020, 17, 1134. [Google Scholar] [CrossRef] [Green Version]
- Yockey, R.A.; King, K.A.; Vidourek, R.A. Family factors and parental correlates to adolescent conduct disorder. J. Fam. Stud. 2021, 27, 356–365. [Google Scholar] [CrossRef]
- Höltge, J.; Theron, L.; Cowden, R.G.; Govender, K.; Maximo, S.I.; Carranza, J.S.; Kapoor, B.; Tomar, A.; van Rensburg, A.; Lu, S.; et al. A cross-country network analysis of adolescent resilience. J. Adolesc. Health 2021, 68, 580–588. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, K.; Martinelli, A.; Bernhard, A.; Freitag, C.M.; Büttner, G.; Schwenck, C. Friendship quality in youth with and without disruptive behavior disorders: The role of empathy, aggression, and callousness. Child Psychiatry Hum. Dev. 2019, 50, 776–788. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, K.D.; Taylor, C.L.; Zubrick, S.R. Psychosocial resilience and vulnerability in Western Australian Aboriginal youth. Child Abus. Negl. 2017, 78, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Henggeler, S.W.; Sheidow, A.J. Conduct disorder and delinquency. J. Marital. Fam. Ther. 2003, 29, 505–522. [Google Scholar] [CrossRef] [PubMed]
- Fritz, J.; de Graaff, A.; Caisley, H.; van Harmelen, A.-L.; Wilkinson, P.O. A systematic review of amenable resilience factors that moderate and/or mediate the relationship between childhood adversity and mental health in young people. Front. Psychol. 2018, 9, 230. [Google Scholar] [CrossRef] [Green Version]
- Criss, M.M.; Pettit, G.S.; Bates, J.E.; Dodge, K.A.; Lapp, A.L. Family adversity, positive peer relationships, and children’s externalizing behavior: A longitudinal perspective on risk and resilience. Child Dev. 2002, 73, 1220–1237. [Google Scholar] [CrossRef]
- Cameranesi, M.; Ripat, J.; Piotrowski, C.C. “I wouldn’t be here without them”: Resilience in youth exposed to intimate partner violence. Adv. Res. Sci. 2021, 2, 19–35. [Google Scholar] [CrossRef]
- Flores, E.; Cicchetti, D.; Rogosch, F.A. Predictors of resilience in maltreated and nonmaltreated Latino children. Dev. Psychopatol. 2005, 41, 338–351. [Google Scholar] [CrossRef]
- Bottrell, D. Dealing with disadvantage resilience and the social capital of young people’s networks. Youth Soc. 2009, 40, 476–501. [Google Scholar] [CrossRef]
- Sanders, J.; Munford, R.; Boden, J. Culture and context: The differential impact of culture, risks and resources on resilience among vulnerable adolescents. Child Youth Serv. Rev. 2017, 79, 517–526. [Google Scholar] [CrossRef]
- Sanders, J.; Munford, R.; Liebenberg, L.; Ungar, M. Peer paradox: The tensions that peer relationships raise for vulnerable youth. Child Fam. Soc. Work 2017, 22, 3–14. [Google Scholar] [CrossRef]
- Wikström, P.-O.H.; Treiber, K. Social disadvantage and crime: A criminological puzzle. Am. Behav. Sci. 2016, 60, 1232–1259. [Google Scholar] [CrossRef] [PubMed]
- Rankin, B.H.; Quane, J.M. Social contexts and urban adolescent outcomes: The interrelated effects of neighborhoods, families, and peers on African-American youth. Soc. Probl. 2002, 49, 79–100. [Google Scholar] [CrossRef] [Green Version]
- Sellström, E.; Bremberg, S. The significance of neighbourhood context to child and adolescent health and well-being: A systematic review of multilevel studies. Scand. J. Public Health 2006, 34, 544–554. [Google Scholar] [CrossRef]
- Ungar, M.; Liebenberg, L. Assessing resilience across cultures using mixed methods: Construction of the child and youth resilience measure. J. Mix. Method. Res. 2011, 5, 126–149. [Google Scholar] [CrossRef]
- Zimmerman, M.A.; Stoddard, S.A.; Eisman, A.B.; Caldwell, C.H.; Aiyer, S.M.; Miller, A. Adolescent resilience: Promotive factors that inform prevention. Child Dev. Perspect. 2013, 7, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Van Breda, A.D.; Theron, L.C. A critical review of South African child and youth resilience studies, 2009–2017. Child Youth Serv. Rev. 2018, 91, 237–247. [Google Scholar] [CrossRef]
- Rowhani, M.; Hatala, A.R. A systematic review of resilience research among Indigenous youth in contemporary Canadian contexts. Int. J. Health Well. Soc. 2017, 7, 45–58. [Google Scholar] [CrossRef]
- Akers, R.L. Criminological Theories: Introduction, Evaluation, and Application, 3rd ed.; Roxbury: Los Angeles, CA, USA, 2000. [Google Scholar]
- Tompsett, C.J.; Veits, G.M.; Amrhein, K.E. Peer delinquency and where adolescents spend time with peers: Mediation and moderation of home neighborhood effects on self-reported delinquency. J. Community Psychol. 2016, 44, 263–270. [Google Scholar] [CrossRef]
- Doosje, B.; Loseman, A.; Bos, K. Determinants of radicalization of Islamic youth in the Netherlands: Personal uncertainty, perceived injustice, and perceived group threat. J. Soc. Issues 2013, 69, 586–604. [Google Scholar] [CrossRef]
- Dejean, F.; Manaï, B.; Kapo, L.T. Students Faced with Religious Radicalization Leading to Violence: The More You Know, the More You Prevent; Collège de Maisonneuve: Institut de Recherche sur L’intégration Professionnelle des Immigrants: Montreal, PQ, Canada, 2016. [Google Scholar]
- Hogg, M.A. From uncertainty to extremism: Social categorization and identity processes. Curr. Dir. Psychol. Sci. 2014, 23, 338–342. [Google Scholar] [CrossRef]
- Brooks, C.M.; Daschuk, M.D.; Poudrier, J.; Almond, N. First Nations youth redefine resilience: Listening to artistic productions of ‘Thug Life’and hip-hop. J. Youth Stud. 2015, 18, 706–725. [Google Scholar] [CrossRef]
- Joshi, D.; Raina, P.; Tonmyr, L.; MacMillan, H.L.; Gonzalez, A. Prevalence of adverse childhood experiences among individuals aged 45 to 85 years: A cross-sectional analysis of the Canadian Longitudinal Study on Aging. CMAJ Open 2021, 9, E158–E166. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, C.; Oulhote, Y.; Lecompte, V.; Mekki-Berrada, A.; Hassan, G.; El Hage, H. Collective identity, social adversity and college student sympathy for violent radicalization. Transcult. Psychiatry 2021, 58, 654–668. [Google Scholar] [CrossRef] [PubMed]
- Graham-Bermann, S.A.; Gruber, G.; Howell, K.H.; Girz, L. Factors discriminating among profiles of resilience and psychopathology in children exposed to intimate partner violence (IPV). Child Abus. Negl. 2009, 33, 648–660. [Google Scholar] [CrossRef]
- Sianko, N.; Hedge, J.M.; McDonell, J.R. Differential adjustment among rural adolescents exposed to family violence. J. Interpers. Violence 2019, 34, 712–740. [Google Scholar] [CrossRef]
- Reising, M.M.; Watson, K.H.; Hardcastle, E.J.; Merchant, M.J.; Roberts, L.; Forehand, R.; Compas, B.E. Parental depression and economic disadvantage: The role of parenting in associations with internalizing and externalizing symptoms in children and adolescents. J. Child Fam. Stud. 2012, 22, 334–343. [Google Scholar] [CrossRef] [Green Version]
- Bolger, K.E.; Patterson, C.J. Sequelae of child maltreatment: Vulnerability and resilience. In Resilience and Vulnerability: Adaptation in the Context of Childhood Adversities; Luthar, S.S., Ed.; Cambridge University Press: New York, NY, USA, 2003. [Google Scholar]
- Campo, M. Children’s Exposure to Domestic and Family Violence; Child Family Community Australia (CFCA), Australian Institute of Family Studies: Melbourne, Australia, 2015. [Google Scholar]
- Thompson, R.A.; Flood, M.F.; Goodvin, R. Social support and developmental psychopathology. In Developmental Psychopathology: Risk, Disorder, and Adaptation; Cicchetti, D., Cohen, D.J., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2006; Volume 3. [Google Scholar]
- Wekerle, C.; Waechter, R.; Chung, R. Contexts of vulnerability and resilience: Childhood maltreatment, cognitive functioning and close relationships. In The Social Ecology of Resilience; Ungar, M., Ed.; Springer: New York, NY, USA.
- Hall, K.; Richter, L.; Mokomane, Z.; Lake, L. (Eds.) South African Child Gauge 2018; Children’s Institute, University of Cape Town: Cape Town, South Africa, 2018. [Google Scholar]
- Das-Munshi, J.; Lund, C.; Mathews, C.; Clark, C.; Rothon, C.; Stansfeld, S. Mental health inequalities in adolescents growing up in post-apartheid South Africa: Cross-sectional survey, SHaW study. PLoS ONE 2016, 11, e0154478. [Google Scholar]
- du Plessis, B.; Kaminer, D.; Hardy, A.; Benjamin, A. The contribution of different forms of violence exposure to internalizing and externalizing symptoms among young South African adolescents. Child Abus. Negl. 2015, 45, 80–89. [Google Scholar] [CrossRef]
- North, A.; Donenberg, G.; Vermaak, R.; Kendall, A.; Mackesy-Amiti, M.E.; Simbayi, L.; Kagee, A.; Mthembu, J.; Ward, C.L.; Emerson, E.; et al. Pathways from witnessing community violence to mental health problems among South African adolescents. S. Afr. Med. J. 2020, 110, 145–153. [Google Scholar]
- Casale, M.; Cluver, L.; Crankshaw, T.; Kuo, C.; Lachman, J.M.; Wild, L.G. Direct and indirect effects of caregiver social support on adolescent psychological outcomes in two South African AIDS-affected communities. Am. J. Community Psychol. 2015, 55, 336–346. [Google Scholar] [CrossRef] [PubMed]
- Humm, A.; Kaminer, D.; Hardy, A. Social support, violence exposure and mental health among young South African adolescents. J. Child Adolesc. Ment. Health 2018, 30, 41–50. [Google Scholar] [CrossRef]
- Mosavel, M.; Ahmed, R.; Ports, K.A.; Simon, C. South African, urban youth narratives: Resilience within community. Int. J. Adolesc. Youth 2015, 20, 245–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scorgie, F.; Baron, D.; Stadler, J.; Venables, E.; Brahmbhatt, H.; Mmari, K.; Delany-Moretlwe, S. From fear to resilience: Adolescents’ experiences of violence in inner-city Johannesburg, South Africa. BMC Public Health 2017, 17, 51–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canham, H. Theorising community rage for decolonial action. S. Afr. J. Psychol. 2018, 48, 319–330. [Google Scholar] [CrossRef]
- Hendricks, G.; Savahl, S.; Mathews, K.; Raats, C.; Jaffer, L.; Matzdorff, A.; Dekel, B.; Larke, C.; Magodyo, T.; Van Gesselleen, M.; et al. Influences on life aspirations among adolescents in a low income community in Cape Town. South Africa. J. Psychol. Afr. 2015, 25, 320–326. [Google Scholar] [CrossRef]
- Madhavan, S.; Crowell, J. Who would you like to be like? Family, village, and national role models among black youth in rural South Africa. J. Adolesc. Res. 2014, 29, 716–737. [Google Scholar] [CrossRef] [Green Version]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; The Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Mitic, M.; Woodcock, K.A.; Amering, M.; Krammer, I.; Stiehl, K.A.M.; Zehetmayer, S.; Schrank, B. Toward an integrated model of supportive peer relationships in early adolescence: A systematic review and exploratory meta-analysis. Front. Psychol. 2021, 12, 589403. [Google Scholar] [CrossRef]
- Fransman, T.; Yu, D. Multidimensional poverty in South Africa in 2001–16. Dev. S. Afr. 2019, 36, 50–79. [Google Scholar] [CrossRef] [Green Version]
- Theron, L.; Rothmann, S.; Höltge, J.; Ungar, M. Differential adaptation to adversity: A latent profile analysis of youth engagement with resilience-enabling cultural resources and mental health outcomes in a stressed Canadian and South African community. J. Cross-Cult. Psychol. 2022. [Google Scholar] [CrossRef]
- Mathebula, S. Protesters Burn Down Mpumalanga Mall. Citizen. 2018. Available online: https://www.citizen.co.za/news/south-africa/1963615/protesters-burn-down-mpumalanga-mall/ (accessed on 21 March 2022).
- Bethell, C.D.; Carle, A.; Hudziak, J.; Gombojav, N.; Powers, K.; Wade, R.; Braveman, P. Methods to assess adverse childhood experiences of children and families: Toward approaches to promote child well-being in policy and practice. Acad. Pediatr. 2017, 17, S51–S69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lerner, R.M.; Lerner, J.V.; Almerigi, J.B.; Theokas, C.; Phelps, E.; Gestsdottir, S.; Naudeau, S.; Jelicic, H.; Alberts, A.; Ma, L.; et al. Positive youth development, participation in community youth development programs, and community contributions of fifth-grade adolescents: Findings from the first wave of the 4-H study of positive youth development. J. Early Adolesc. 2005, 25, 17–71. [Google Scholar] [CrossRef]
- Geldhof, G.J.; Bowers, E.P.; Boyd, M.J.; Mueller, M.K.; Napolitano, C.M.; Schmid, K.L.; Lerner, J.V.; Lerner, R.M. The creation and validation of short and very short measures of PYD. J. Res. Adolesc. 2014, 24, 163–176. [Google Scholar] [CrossRef] [Green Version]
- IBM Corporation Released. IBM SPSS Statistics for Windows, Version 27.0; IBM Corporation: Armonk, NY, USA, 2020.
- Igartua, J.-J.; Hayes, A.F. Mediation, moderation, and conditional process analysis: Concepts, computations, and some common confusions. Span. J. Psychol. 2021, 24, e49. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 5th ed.; Sage: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Masten, A.S.; Palmer, A.R. Parenting to promote resilience in children. In Handbook of Parenting, 3rd ed.; Bornstein, M.H., Ed.; Routledge: London, UK, 2019; Volume 5, pp. 156–188. [Google Scholar]
- Luthar, S.S.; Ebbert, A.M.; Kumar, N.L. Risk and resilience during COVID-19: A new study in the Zigler paradigm of developmental science. Dev. Psychopathol. 2021, 33, 565–580. [Google Scholar] [CrossRef]
- Russell, P.; Liebenberg, L.; Ungar, M. White out: The invisibility of white North American culture and resilience processes. In Youth Resilience and Culture; Theron, L., Liebenberg, L., Ungar, M., Eds.; Springer: Dordrecht, The Netherlands, 2015; pp. 131–141. [Google Scholar]
- Lund, C.; Brooke-Sumner, C.; Baingana, F.; Baron, E.C.; Breuer, E.; Chandra, P.; Haushofer, J.; Herrman, H.; Jordans, M.; Kieling, C.; et al. Social determinants of mental disorders and the Sustainable Development Goals: A systematic review of reviews. Lancet Psychiatry 2018, 5, 357–369. [Google Scholar] [CrossRef]
- Lance, C.E.; Butts, M.M.; Michels, L.C. The sources of four commonly reported cutoff criteria: What did they really say? Org. Res. Meth. 2006, 9, 202–220. [Google Scholar] [CrossRef]
- Ahmad, F.; Jhajj, A.K.; Stewart, D.E.; Burghardt, M.; Bierman, A.S. Single item measures of self-rated mental health: A scoping review. BMC Health Serv. Res. 2014, 14, 398. [Google Scholar] [CrossRef] [Green Version]
- Ang, L.; Eisend, M. Single versus multiple measurement of attitudes: A meta-analysis of advertising studies validates the single-item measure approach. J. Advert. Res. 2018, 58, 218–227. [Google Scholar] [CrossRef]
- Allen, M.S.; Iliescu, D.; Greiff, S. Single item measures in psychological science: A call to action. Eur. J. Psychol. Assess. 2022, 38, 1–5. [Google Scholar] [CrossRef]
- Ungar, M. The differential impact of social services on young people’s resilience. Child Abus. Negl. 2018, 78, 4–13. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| 1. Sex | - | 0.079 | −0.082 | 0.071 | −0.045 | 0.052 | 0.154 ** |
| 2. Age | 0.166 ** | - | 0.144 ** | −0.032 | −0.075 | −0.006 | 0.151 ** |
| 3. Family adversity | −0.059 | 0.140 ** | - | −0.242 ** | −0.122 * | −0.188 ** | 0.307 ** |
| 4. Family Caregiving | −0.004 | −0.004 | −0.151 ** | - | 0.283 ** | 0.524 ** | −0.206 ** |
| 5. Peer support | −0.072 | −0.104 * | −0.127 ** | 0.223 ** | - | 0.282 ** | −0.081 |
| 6. Appreciation for Community Traditions | 0.090 * | −0.023 | 0.016 | 0.321 ** | 0.204 ** | - | −0.201 ** |
| 7. Conduct problems | 0.313 ** | 0.054 | 0.206 ** | −0.098 * | −0.217 ** | −0.008 | - |
| Variable | Canada | South Africa | t | p | Cohen’s d | ||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | ||||
| Age | 16.16 | 1.38 | 15.97 | 1.19 | 1.81 | 0.070 | 0.316 |
| Family adversity | 2.17 | 2.05 | 1.88 | 1.60 | 1.88 | 0.061 | 0.327 |
| Family Caregiving | 21.86 | 5.86 | 22.71 | 4.67 | −1.91 | 0.057 | −0.006 |
| Peer support | 8.88 | 2.89 | 8.16 | 2.70 | 3.12 | 0.002 * | 0.422 |
| Appreciation for Community Traditions | 2.47 | 1.21 | 2.21 | 1.34 | 2.5 | 0.013 * | 0.199 |
| Conduct problems | 9.43 | 4.75 | 8.44 | 3.22 | 2.82 | 0.005 * | 0.419 |
| Canada | ||||||
|---|---|---|---|---|---|---|
| Family Caregiving (M) | Conduct problem (Y) | |||||
| Coeff b | bSE (b) | 95% bCI (b) | Coeff b | bSE (b) | 95% bCI (b) | |
| Constant | 22.788 | 4.430 | [14.067, 31.522] * | 17.672 | 5.253 | [5.583, 26.401] * |
| Family adversity (X) | −1.136 | 0.206 | [−1.540, −0.726] * | 0.953 | 0.196 | [0.565, 1.330] * |
| Family caregiving (M) | - | - | −0.603 | 0.163 | [−0.878, −0.232] * | |
| Peer support (W) | - | - | - | −1.260 | 0.435 | [−1.960, −0.269] * |
| M x W (interaction) | - | - | - | 0.057 | 0.018 | [0.016, 0.087] * |
| Age (covariate 1) | 0.040 | 0.268 | [−0.489, 0.562] | 0.035 | 0.210 | [−0.363, 0.452] |
| Sex (covariate 2) | 0.612 | 0.712 | [−0.824, 1.985] | 1.380 | 0.518 | [0.396, 2.410] * |
| R2 = 0.164 F(3226) = 10.708, p < 0.001 | R2 = 0.326 F(6223) = 10.899, p < 0.001 | |||||
| South Africa | ||||||
| Family Caregiving (M) | Conduct problem (Y) | |||||
| Coeff b | bSE (b) | 95% bCI (b) | Coeff b | bSE (b) | 95% bCI (b) | |
| Constant | 22.479 | 3.125 | [16.375, 28.692] * | 8.338 | 2.830 | [2.851, 13.891] * |
| Family adversity (X) | −0.454 | 0.146 | [−0.743, −0.172] * | 0.429 | 0.099 | [0.236, 0.628] * |
| Family caregiving (M) | - | - | - | −0.006 | 0.077 | [−0.156, 0.149] |
| Peer support (W) | - | - | - | −0.152 | 0.217 | [−0.566, 0.293] |
| M x W (interaction) | - | - | - | −0.002 | 0.009 | [−0.020, 0.015] |
| Age (covariate 1) | 0.079 | 0.198 | [−0.314, 0.458] | −0.157 | 0.119 | [−0.223, 0.279] |
| Sex (covariate 2) | −0.134 | 0.469 | [−1.056, 0.782] | 2.579 | 0.337 | [1.924, 3.253] * |
| R2 = 0.023 F(3417) = 3.212, p < 0.05 | R2 = 0.224 F(6414) = 13.892, p < 0.001 | |||||
| Canada | ||||||
|---|---|---|---|---|---|---|
| Family Caregiving (M) | Conduct problem (Y) | |||||
| Coeff b | bSE (b) | 95% bCI (b) | Coeff b | bSE (b) | 95% bCI (b) | |
| Constant | 22.788 | 4.525 | [13.871, 31.705] * | 10.419 | 5.352 | [−0.129, 20.966] |
| Family adversity (X) | −1.136 | 0.214 | [−1.557, −0.714] * | 0.943 | 0.220 | [0.509, 1.378] * |
| Family caregiving (M) | - | - | - | −0.265 | 0.166 | [−0.593, 0.063] |
| AfCT (W) | - | - | - | −1.589 | 1.407 | [−4.361, 1.184] |
| M x W (interaction) | - | - | - | 0.064 | 0.060 | [−0.054, 0.182] |
| Age (covariate 1) | 0.040 | 0.274 | [−0.500, 0.581] | 0.037 | 0.227 | [−0.410, 0.485] |
| Sex (covariate 2) | 0.612 | 0.717 | [−0.800, 2.024] | 1.657 | 0.510 | [0.652, 2.661] * |
| R2 = 0.164 F(3226) = 10.708, p < 0.001 | R2 = 0.283 F(6223) = 8.637, p < 0.001 | |||||
| South Africa | ||||||
| Family Caregiving (M) | Conduct problem (Y) | |||||
| Coeff b | bSE (b) | 95% bCI (b) | Coeff b | bSE (b) | 95% bCI (b) | |
| Constant | 22.479 | 3.142 | [16.303, 28.655] * | 4.178 | 2.061 | [0.127, 8.230] * |
| Family adversity (X) | −0.454 | 0.148 | [−0.744, −0.163] * | 0.451 | 0.105 | [0.244, 0.658] * |
| Family caregiving (M) | - | - | - | 0.082 | 0.043 | [−0.002, 0.167] |
| AfCT (W) | - | - | - | 1.320 | 0.454 | [0.426, 2.213] * |
| M x W (interaction) | - | - | - | −0.063 | 0.019 | [−0.101, −0.024] * |
| Age (covariate 1) | 0.079 | 0.198 | [−0.314, 0.458] | −0.111 | 0.119 | [−0.345, 0.123] |
| Sex (covariate 2) | −0.134 | 0.469 | [−1.056, 0.782] | 2.682 | 0.346 | [2.001, 3.363] * |
| R2 = 0.023 F(3417) = 3.212, p = 0.02 | R2 = 0.217 F(6414) = 13.494, p < 0.001 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cameranesi, M.; Theron, L.; Höltge, J.; Jefferies, P.; Ungar, M. Understanding the Mechanisms through Which Family Risk Affects Adolescent Mental Health: A Model of Multisystemic Resilience in Context. Children 2022, 9, 546. https://doi.org/10.3390/children9040546
Cameranesi M, Theron L, Höltge J, Jefferies P, Ungar M. Understanding the Mechanisms through Which Family Risk Affects Adolescent Mental Health: A Model of Multisystemic Resilience in Context. Children. 2022; 9(4):546. https://doi.org/10.3390/children9040546
Chicago/Turabian StyleCameranesi, Margherita, Linda Theron, Jan Höltge, Philip Jefferies, and Michael Ungar. 2022. "Understanding the Mechanisms through Which Family Risk Affects Adolescent Mental Health: A Model of Multisystemic Resilience in Context" Children 9, no. 4: 546. https://doi.org/10.3390/children9040546