
Individual and Contextual Risk and Protective Factors for Suicidal Thoughts and Behaviors among Black Adolescents with Arrest Histories

 , , , and
, , , and
Abstract
:1. Introduction
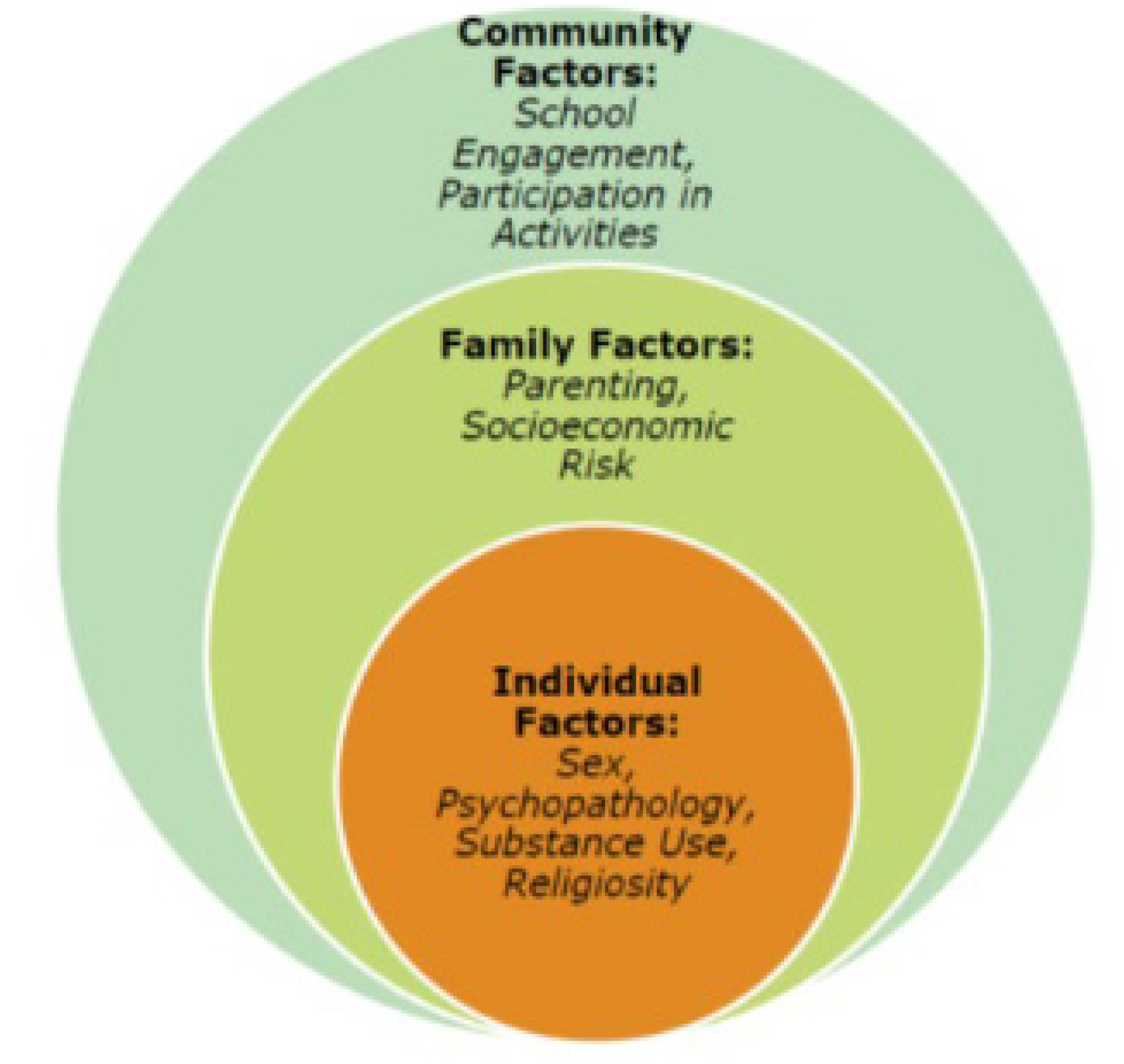
1.1. Theoretical Framework—Intersectionality and Bio-Ecological Model
1.2. Depression, Substance Misuse and Suicidal Behavior
1.3. Protective Factors for Suicidal Thoughts and Behavior
2. Current Study Aims and Hypotheses
3. Materials and Methods
3.1. Participants
3.2. Procedures
3.3. Measures
3.4. Data Analysis
4. Results
4.1. Preliminary Analyses
4.2. Univariate Logistic Regression Models
4.3. Multivariate Logistic Regression Models
5. Discussion
5.1. Limitations
5.2. Practice and Policy Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thompson, M.P.; Swartout, K. Epidemiology of Suicide Attempts among Youth Transitioning to Adulthood. J. Youth Adolesc. 2017, 47, 807–817. [Google Scholar] [CrossRef] [PubMed]
- Lindsey, M.A.; Sheftall, A.H.; Xiao, Y.; Joe, S. Trends of Suicidal Behaviors Among High School Students in the United States: 1991–2017. Pediatrics 2019, 144, e20191187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feigelman, W.; Cerel, J.; McIntosh, J.L.; Brent, D.; Gutin, N. Suicide exposures and bereavement among American adults: Evidence from the 2016 General Social Survey. J. Affect. Disord. 2018, 227, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Yahoo News. Young Black People Dying by Suicide on the Rise for the First Time in History. 2022. Available online: https://news.yahoo.com/young-black-people-dying-suicide-231731428.html?guccounter=1&guce_referrer=aHR0cHM6Ly93d3cuYmluZy5jb20v&guce_referrer_sig=AQAAAKBgWdIKezyJgb0sQIYxfD5FBLwOs83s85SF3bzmD4STUCy6uAZjhUhuYxtMCh1WzkcapNKV-Zt1nRmGWOGcRnWZ4j-Y-3lPnJ7Hv6oJuBmcZBnd7lsxZZlD5-7OJCfjeS0h8Pk2xb_wpHA93ZQAsS55Wi1AbBZM5BRwL4MKHtMb (accessed on 28 March 2022).
- Duprey, E.B.; Quinn, C.R.; Handley, E.D.; Ross, A.J.; Mitchell, M.; Cerulli, C. Risk and Protective Factors for Suicidal Ideation, Plans, and Attempts among Black Youth. Soc. Psychiatry Psychiatr. Epidemiol. 2022. submitted. [Google Scholar]
- Santos, P.H.D.; Neves, S.M.; Sant’Anna, D.O.; Oliveira, C.H.; Carvalho, H.D. The analytic hierarchy process supporting decision making for sustainable development: An overview of applications. J. Clean. Prod. 2019, 212, 119–138. [Google Scholar] [CrossRef]
- Romanelli, M.; Sheftall, A.H.; Irsheid, S.B.; Lindsey, M.A.; Grogan, T.M. Factors Associated with Distinct Patterns of Suicidal Thoughts, Suicide Plans, and Suicide Attempts Among US Adolescents. Prev. Sci. 2021, 23, 73–84. [Google Scholar] [CrossRef]
- Coleman, B.; Emergency Taskforce on Black Youth Suicide and Mental Health. In Ring the Alarm: The Crisis of Black Youth Suicide in America. Available online: https://theactionalliance.org/resource/ring-alarm-crisis-black-youth-suicide-america (accessed on 1 March 2022).
- Ginther, D.K.; Schaffer, W.T.; Schnell, J.; Masimore, B.; Liu, F.; Haak, L.L.; Kington, R. Race, Ethnicity, and NIH Research Awards. Science 2011, 333, 1015–1019. [Google Scholar] [CrossRef] [Green Version]
- National Institutes of Health. Research Topic Contributes to Persistent Gap in NIH Research Grants to Black Scientists. 2019. Available online: https://www.nih.gov/news-events/news-releases/research-topic-contributes-persistent-gap-nih-research-grants-black-scientists (accessed on 9 February 2019).
- Beneby, D.R.; Glenn, J.W.; Taylor, L.C. An Assessment of the Hypercriminalization Thesis: Evidence from Juvenile Justice and Human Service Practitioners in the USA. J. Appl. Youth Stud. 2020, 3, 167–180. [Google Scholar] [CrossRef]
- Walton, G.M.; Okonofua, J.A.; Remington Cunningham, K.; Hurst, D.; Pinedo, A.; Weitz, E.; Eberhardt, J.L. Lifting the bar: A relationship-orienting intervention reduces recidivism among children reentering school from juvenile detention. Psychol. Sci. 2021, 32, 1747–1767. [Google Scholar] [CrossRef]
- Cole, H.; Cohen, R. Breaking down barriers: A case study of juvenile justice personnel perspectives on school reentry. J. Correct. Educ. 2013, 64, 13–35. [Google Scholar]
- Kubek, J.B.; Tindall-Biggins, C.; Reed, K.; Carr, L.E.; Fenning, P.A. A systematic literature review of school reentry practices among youth impacted by juvenile justice. Child. Youth Serv. Rev. 2020, 110, 104773. [Google Scholar] [CrossRef]
- Dorsey, M.S.; King, D.; Howard-Howell, T.; Dyson, Y. Culturally Responsive Sexual Health Interventions for Black Adolescent Females in the United States: A Systematic Review of the Literature, 2010-2020. Child. Youth Serv. Rev. 2022, 21, 106480. [Google Scholar] [CrossRef]
- Lee, C.S.; Wong, Y.J. Racial/ethnic and gender differences in the antecedents of youth suicide. Cult. Divers. Ethn. Minor. Psychol. 2020, 26, 532–543. [Google Scholar] [CrossRef] [PubMed]
- Puzzanchera, C. Juvenile Arrests, 2019. U.S. Department of Justice, Office of Justice Programs. 2021. Available online: https://ojjdp.ojp.gov/publications/juvenile-arrests-2019.pdf (accessed on 1 March 2022).
- Aguilar, D.D. Tracing the Roots of Intersectionality. MR Online. Available online: https://mronline.org/2012/04/12/aguilar120412-html/ (accessed on 1 November 2021).
- Taylor, K.Y. Black feminism and the Combahee River collective. Mon. Rev.-Indep. Soc. Mag. 2019, 70, 20–28. [Google Scholar] [CrossRef]
- Waller, B.Y.; Harris, J.; Quinn, C.R. Caught in the Crossroad: An Intersectional Examination of African American Women Intimate Partner Violence Survivors’ Help Seeking. Trauma Violence Abus. 2021, 99, 1303. [Google Scholar] [CrossRef] [PubMed]
- Burgess-Proctor, A. Intersections of Race, Class, Gender, and Crime. Fem. Criminol. 2006, 1, 27–47. [Google Scholar] [CrossRef]
- Owen, B.; Wells, J.; Pollock, J. Search of Safety: Confronting Inequality in Women’s Imprisonment; Univ of California Press: Oak-land, CA, USA, 2017; Volume 3. [Google Scholar]
- Williams-Butler, A.; Liu, F.-Y.; Howell, T.; Menon, S.E.; Quinn, C.R. Racialized Gender Differences in Mental Health Service Use, Adverse Childhood Experiences, and Recidivism Among Justice-Involved African American Youth. Race Soc. Probl. 2022, 9, 1–14. [Google Scholar] [CrossRef]
- Bronfenbrenner, U.; Morris, P. The bioecological model of human development. In Handbook of Child Psychology, 6th ed.; Theoretical Models of Human, Development; Damon, W., Lerner, R.M., Eds.; John Wile: New York, NY, USA, 2006; Volume 1, pp. 793–828. [Google Scholar]
- Opara, I.; Assan, M.A.; Pierre, K.; Gunn, I.J.F.; Metzger, I.; Hamilton, J.; Arugu, E. Suicide among Black Children: An Integrated Model of the Interpersonal-Psychological Theory of Suicide and Intersectionality Theory for Researchers and Clinicians. J. Black Stud. 2020, 51, 611–631. [Google Scholar] [CrossRef]
- Stokes, M.L.; McCoy, K.P.; Abram, K.M.; Byck, G.R.; Teplin, L.A. Suicidal ideation and behavior in youth in the juvenile justice system: A review of the literature. J. Correct. Health Care 2015, 21, 222–242. [Google Scholar] [CrossRef]
- Teplin, L.A.; Abram, K.M.; McClelland, G.M.; Dulcan, M.K.; Mericle, A.A. Psychiatric Disorders in Youth in Juvenile Detention. Arch. Gen. Psychiatry 2002, 59, 1133–1143. [Google Scholar] [CrossRef]
- Quinn, C.R.; Liu, C.; Kothari, C.; Cerulli, C.; Thurston, S.W. Psychological Distress Among Youth Probationers: Using Social Determinants of Health to Assess Suicidal Thoughts and Behaviors. Adolesc. Psychiatry 2018, 7, 89–104. [Google Scholar] [CrossRef] [PubMed]
- Penn, J.V.; Thomas, C. Practice Parameter for the Assessment and Treatment of Youth in Juvenile Detention and Correctional Facilities. J. Am. Acad. Child Adolesc. Psychiatry 2005, 44, 1085–1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasserman, G.A.; McReynolds, L.S. Suicide Risk at Juvenile Justice Intake. Suicide Life-Threat. Behav. 2006, 36, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, G.A.; McReynolds, L.S.; Schwalbe, C.S.; Keating, J.M.; Jones, S.A. Psychiatric Disorder, Comorbidity, and Suicidal Behavior in Juvenile Justice Youth. Crim. Justice Behav. 2010, 37, 1361–1376. [Google Scholar] [CrossRef] [Green Version]
- Nock, M.K.; Green, J.; Hwang, I.; McLaughlin, K.; Sampson, N.A.; Zaslavsky, A.M.; Kessler, R.C. Prevalence, Correlates, and Treatment of Lifetime Suicidal Behavior Among Adolescents. JAMA Psychiatry 2013, 70, 300–310. [Google Scholar] [CrossRef] [Green Version]
- Ford, J.D.; Chapman, J.; Mack, J.M.; Pearson, G. Pathways from Traumatic Child Victimization to Delinquency: Implications for Juvenile and Permanency Court Proceedings and Decisions. Juv. Fam. Court J. 2006, 57, 13–26. [Google Scholar] [CrossRef]
- Ford, J.D.; Hartman, J.K.; Hawke, J.; Chapman, J.F. Traumatic victimization, posttraumatic stress disorder, suicidal ideation, and substance abuse risk among juvenile justice-involved youth. J. Child Adolesc. Trauma 2008, 1, 75–92. [Google Scholar] [CrossRef]
- Anda, R.F.; Felitti, V.J.; Bremner, J.D.; Walker, J.D.; Whitfield, C.; Perry, B.D.; Dube, S.R.; Giles, W.H. The enduring effects of abuse and related adverse experiences in childhood: A convergence of evidence from neurobiology and epi-demiology. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 174–186. [Google Scholar] [CrossRef]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of child-hood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACES) study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Perez, N.M.; Jennings, W.G.; Piquero, A.R.; Baglivio, M.T. Adverse Childhood Experiences and Suicide Attempts: The Mediating Influence of Personality Development and Problem Behaviors. J. Youth Adolesc. 2016, 45, 1527–1545. [Google Scholar] [CrossRef]
- Capaldi, D.M.; Kim, H.K.; Richards, C.S.; O’Hara, M.W. Comorbidity of depression and conduct disorder. In The Oxford Handbook of Depression and Comorbidity; Oxford University Press: Oxford, UK, 2014; pp. 186–199. [Google Scholar]
- Reinke, W.M.; Eddy, J.M.; Dishion, T.J.; Reid, J.B. Joint Trajectories of Symptoms of Disruptive Behavior Problems and Depressive Symptoms During Early Adolescence and Adjustment Problems During Emerging Adulthood. J. Abnorm. Child Psychol. 2012, 40, 1123–1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatters, L.M.; Taylor, R.J.; Lincoln, K.D.; Nguyen, A.; Joe, S. Church-Based Social Support and Suicidality Among African Americans and Black Caribbeans. Arch. Suicide Res. 2011, 15, 337–353. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Moon, S.S.; Kim, Y.K.; Boyas, J. Protective factors of suicide: Religiosity and parental monitoring. Child. Youth Serv. Rev. 2020, 114, 105073. [Google Scholar] [CrossRef]
- Sheldrake, P. Spirituality: A Brief History, 2nd ed.; Wiley-Blackwell: West Sussex, UK, 2013. [Google Scholar]
- Graves, K.N.; Kaslow, N.J.; Frabutt, J.M. A culturally-informed approach to trauma, suicidal behavior, and overt aggression in African American adolescents. Aggress. Violent Behav. 2010, 15, 36–41. [Google Scholar] [CrossRef]
- Goldston, D.B.; Molock, S.D.; Whitbeck, L.B.; Murakami, J.L.; Zayas, L.H.; Hall, G.C.N. Cultural considerations in adolescent suicide prevention and psychosocial treatment. Am. Psychol. 2008, 63, 14–31. [Google Scholar] [CrossRef] [Green Version]
- Good, M.; Willoughby, T. Adolescence as a Sensitive Period for Spiritual Development. Child Dev. Perspect. 2008, 2, 32–37. [Google Scholar] [CrossRef]
- Hill, P.C.; Pargament, K.I. Advances in the conceptualization and measurement of religion and spirituality: Implications for physical and mental health research. Am. Psychol. 2003, 58, 64–74. [Google Scholar] [CrossRef] [Green Version]
- Miller, W.R.; Thoresen, C.E. Spirituality, religion, and health: An emerging research field. Am. Psychol. 2003, 58, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Adedoyin, A.C.; Salter, S.N. Mainstreaming black churches into suicide prevention among adolescents: A literature review. Ethn. Inequalities Health Soc. Care 2013, 6, 43–53. [Google Scholar] [CrossRef]
- Greening, L.; Ma, L.S. Religiosity, Attributional Style, and Social Support as Psychosocial Buffers for African American and White Adolescents’ Perceived Risk for Suicide. Suicide Life-Threat. Behav. 2002, 32, 404–417. [Google Scholar] [CrossRef]
- Rew, L.; Wong, Y.J. A systematic review of associations among religiosity/spirituality and adolescent health attitudes and behaviors. J. Adolesc. Health 2006, 38, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Kelly, P.E.; Polanin, J.; Jang, S.J.; Johnson, B.R. Religion, Delinquency, and Drug Use. Crim. Justice Rev. 2015, 40, 505–523. [Google Scholar] [CrossRef] [Green Version]
- Cole-Lewis, Y.C.; Gipson, P.Y.; Opperman, K.J.; Arango, A.; King, C.A. Protective Role of Religious Involvement Against Depression and Suicidal Ideation Among Youth with Interpersonal Problems. J. Relig. Health 2016, 55, 1172–1188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Planey, A.M.; Smith, S.M.; Moore, S.; Walker, T.D. Barriers and facilitators to mental health help-seeking among African American youth and their families: A systematic review study. Child. Youth Serv. Rev. 2019, 101, 190–200. [Google Scholar] [CrossRef]
- Samuel, I.A. Utilization of Mental Health Services Among African-American Male Adolescents Released from Juvenile Detention: Examining Reasons for Within-Group Disparities in Help-Seeking Behaviors. Infant Ment. Health J. 2014, 32, 33–43. [Google Scholar] [CrossRef]
- Breland-Noble, A.M.; Board, A.P.A.A.; Bell, C.C.; Burriss, A. “Mama just won’t accept this”: Adult Perspectives on Engaging Depressed African American Teens in Clinical Research and Treatment. J. Clin. Psychol. Med. Settings 2011, 18, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Breland-Noble, A.M.; Wong, M.J.; Childers, T.; Hankerson, S.; Sotomayor, J. Spirituality and religious coping in African-American youth with depressive illness. Ment. Health Relig. Cult. 2015, 18, 330–341. [Google Scholar] [CrossRef]
- Porch, L. A Study of Juvenile Delinquency and a Re-entry Program Back into the Community. Ph.D. Dissertation, DePaul University, Chicago, IL, USA, 2021. [Google Scholar]
- Lipsey, M.W.; Derzon, J.H. Predictors of violent or serious delinquency in adolescence and early adulthood: A synthesis of longitudinal research. In Serious and Violent Juvenile Offenders: Risk Factors and Successful Interventions; Loeber, R., Farrington, D.P., Eds.; Sage Publications, Inc.: New York, NY, USA, 1998; pp. 86–105. Available online: https://www.ojp.gov/ncjrs/virtual-library/abstracts/predictorsviolent- (accessed on 29 October 2014).
- Basch, C.E. Aggression and Violence and the Achievement Gap Among Urban Minority Youth. J. Sch. Health 2011, 81, 619–625. [Google Scholar] [CrossRef]
- Henderson, D.X.; Walker, L.; Barnes, R.R.; Lunsford, A.; Edwards, C.; Clark, C. A Framework for Race-Related Trauma in the Public Education System and Implications on Health for Black Youth. J. Sch. Health 2019, 89, 926–933. [Google Scholar] [CrossRef]
- Peguero, A.A. Violence, schools, and dropping out: Racial and ethnic disparities in the educational consequence of student victimization. J. Interpers. Violence 2011, 26, 3753–3772. [Google Scholar] [CrossRef]
- Quinn, C.R.; Boyd, D.T.; Kim, B.-K.E.; Menon, S.E.; Logan-Greene, P.; Asemota, E.; Diclemente, R.J.; Voisin, D. The Influence of Familial and Peer Social Support on Post-Traumatic Stress Disorder Among Black Girls in Juvenile Correctional Facilities. Crim. Justice Behav. 2021, 48, 867–883. [Google Scholar] [CrossRef]
- Arbona, C.; Power, T.G. Parental attachment, self-esteem, and antisocial behaviors among African American, Eu-ropean American, and Mexican American adolescents. J. Couns. Psychol. 2003, 50, 40–51. [Google Scholar] [CrossRef]
- Kiser, L.J.; Medoff, D.R.; Black, M.M. The role of family processes in childhood traumatic stress reactions for youths living in urban poverty. Traumatology 2010, 16, 33–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller-Graff, L.E. Frameworks for childhood PTSD treatment in conflict-affected settings. Peace Confl. J. Peace Psychol. 2016, 22, 262–271. [Google Scholar] [CrossRef]
- Hagan, M.J.; Browne, D.T.; Sulik, M.; Ippen, C.G.; Bush, N.; Lieberman, A.F. Parent and Child Trauma Symptoms During Child-Parent Psychotherapy: A Prospective Cohort Study of Dyadic Change. J. Trauma. Stress 2017, 30, 690–697. [Google Scholar] [CrossRef]
- Boyd, D.T.; Quinn, C.R.; Jones, K.V.; Beer, O.W.J. Suicidal ideations and Attempts Within the Family Context: The Role of Parent Support, Bonding, and Peer Experiences with Suicidal Behaviors. J. Racial Ethn. Health Disparities 2021, 7, 1–10. [Google Scholar] [CrossRef]
- Marraccini, M.E.; Griffin, D.; O’Neill, J.C.; Martinez, R.R.; Chin, A.J.; Toole, E.N.; Grapin, S.L.; Naser, S.C. School Risk and Protective Factors of Suicide: A Cultural Model of Suicide Risk and Protective Factors in Schools. Sch. Psychol. Rev. 2021, 5, 1–24. [Google Scholar] [CrossRef]
- Piña-Watson, B.; Castillo, L.G.; Rodriguez, K.M.; Ray, S. Familial factors related to suicidal ideation of Latina ado-lescents in the United States. Arch. Suicide Res. 2014, 18, 213–220. [Google Scholar] [CrossRef]
- Wang, C.; La Salle, T.; Wu, C.; Do, K.A.; Sullivan, K.E. School climate and parental involvement buffer the risk of peer victimization on suicidal thoughts and behaviors among Asian American middle school students. Asian Am. J. Psychol. 2018, 9, 296–307. [Google Scholar] [CrossRef]
- Wang, Q.; Ren, L.; Wang, W.; Xu, W.; Wang, Y. The relationship between post-traumatic stress disorder and sui-cidal ideation among shidu parents: The role of stigma and social support. BMC Psychiatry 2019, 19, 1–9. [Google Scholar] [CrossRef] [Green Version]
- United States Department of Health and Human Services (USDHHS). National Survey of Drug Use and Health (NSDUH) Releases [Data Fi006Ce]. 2019. Available online: https://www.samhsa.gov/data/release/2019-national-survey-drug-use-and-health-nsduh-releases (accessed on 11 December 2020).
- Kissinger, P.; Rice, J.; Farley, T.; Trim, S.; Jewitt, K.; Margavio, V.; Martin, D.H. Application of Computer-assisted Interviews to Sexual Behavior Research. Am. J. Epidemiol. 1999, 149, 950–954. [Google Scholar] [CrossRef] [PubMed]
- Leon, A.C.; Olfson, M.; Portera, L.; Farber, L.; Sheehan, D.V. Assessing Psychiatric Impairment in Primary Care with the Sheehan Disability Scale. Int. J. Psychiatry Med. 1997, 27, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Kemp, K.; Poindexter, B.; Ng, M.Y.; Correia, V.; Marshall, B.D.; Koinis-Mitchell, D.; Tolou-Shams, M. Early Identification of Suicide Risk Factors Among Justice-Involved Youth. Crim. Justice Behav. 2021, 49, 730–744. [Google Scholar] [CrossRef]
- Quinn, C.R.; Beer, O.W.J.; Boyd, D.; Tirmazi, T.; Nebbitt, V.; Joe, S. An Assessment of the Role of Parental Incar-ceration and Substance Misuse in Suicidal Planning of African American Youth and Young Adults. J. Racial Ethn. Health Disparities 2021, 5, 1–13. [Google Scholar] [CrossRef]
- Infante, D.A. Corporal punishment of children: A communication-theory perspective. In Corporal Punishment of Children in Theoretical Perspective; Donnelly, M., Straus, M.A., Eds.; Oxford University Press: Oxford, UK, 2005; pp. 183–198. [Google Scholar]
- McLoyd, V.C.; Kaplan, R.; Hardaway, C.R.; Wood, D. Does endorsement of physical discipline matter? Assessing moderating influences on the maternal and child psychological correlates of physical discipline in African American families. J. Fam. Psychol. 2007, 21, 165–175. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance System—United States, 2011. Morb. Mortal. Wkly. Rep. 2012, 61, 1–162. [Google Scholar]
- Quinn, C.R.; Boyd, D.; Beaujolais, B.; Hughley, A.; Mitchell, M.; DiClemente, R.J.; Voisin, D.R. Perceptions of sexual risk and HIV/STI prevention among Black adolescent girls in a detention center: An investigation of the role of parents and peers. J. Racial Ethn. Health Disparities 2022, in press.
- Pope, C.; Lovell, R.; Hsia, H. Disproportionate Minority Confinement: A Review of the Research Literature from 1989 through 2001; Office of Juvenile Justice and Delinquency Prevention: Washington, DC, USA, 2002.
- Domalanta, D.D.; Risser, W.L.; Roberts, R.E.; Risser, J.M.H. Prevalence of depression and other psychiatric dis-orders among incarcerated youths. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 477–484. [Google Scholar] [CrossRef]
- Shaffer, D.; Gould, M.; Hicks, R.C. Worsening suicide rate in black teenagers. Am. J. Psychiatry 1994, 151, 1810–1812. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance—United States, 2019. MMWR Suppl. 2020, 69, 1–83. [Google Scholar] [CrossRef]
- Boyd, D.T.; Jones, K.V.; Quinn, C.R.; Gale, A.; Williams, E.-D.G.; Lateef, H. The Mental Health of Black Youth Affected by Community Violence: Family and School Context as Pathways to Resilience. Children 2022, 9, 259. [Google Scholar] [CrossRef] [PubMed]
- Quinn, C.R.; Duron, J.; Simmons-Horton, S.; Boyd, D.T. Exploring structural and systemic barriers affecting system-involved youth and families: Implications for policy and practice. In Child and Family Serving Systems: A Compendium of Policy and Practice; Denby, R.W., Ingram, C., Eds.; Child Welfare League of America: Washington, DC, USA, 2017. [Google Scholar]
- Espinosa, E.M.; Sorensen, J.R.; Lopez, M.A. Youth Pathways to Placement: The Influence of Gender, Mental Health Need and Trauma on Confinement in the Juvenile Justice System. J. Youth Adolesc. 2013, 42, 1824–1836. [Google Scholar] [CrossRef] [PubMed]
- Duron, J.F.; Williams-Butler, A.; Liu, F.Y.Y.; Nesi, D.; Fay, K.P.; Kim, B.K.E. The influence of adverse childhood experiences (ACEs) on the functional impairment of justice-involved adolescents: A comparison of baseline to follow-up re-ports of adversity. Youth Violence Juv. Justice 2021, 19, 384–401. [Google Scholar] [CrossRef]
- Duron, J.F.; Williams-Butler, A.; Mattson, P.; Boxer, P. Trauma exposure and mental health needs among adoles-cents involved with the juvenile justice system. J. Interpers. Violence 2021, 88, 62605211016358. [Google Scholar]
- Sheftall, A.H.; Vakil, F.; Ruch, D.A.; Boyd, R.C.; Lindsey, M.A.; Bridge, J.A. Black Youth Suicide: Investigation of Current Trends and Precipitating Circumstances. J. Am. Acad. Child Adolesc. Psychiatry 2021, 8, 21. [Google Scholar] [CrossRef]


{kind=link}
| Predictor | Mean | Standard Error | Range | Unweighted N |
|---|---|---|---|---|
| Socioeconomic risk | 1.50 | 0.07 | 0–3 | 415 |
| Depression severity | 0.48 | 0.07 | 0–5 | 513 |
| Substance use | 0.48 | 0.04 | 0–3 | 513 |
| Positive parenting | 3.25 | 0.05 | 1–4 | 505 |
| School engagement | 3.00 | 0.04 | 1–4 | 465 |
| Activities | 4.47 | 0.19 | 0–12 | 503 |
| Religiosity | 2.67 | 0.05 | 1–4 | 498 |
| Suicidal Ideation | Suicide Plan | Suicide Attempt | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Predictor | N | B | SE B | OR | 95% CI OR | N | B | SE B | OR | 95% CI OR | N | B | SE B | OR | 95% CI OR |
| Demographics | |||||||||||||||
| Sex (male) | 495 | −2.35 | 0.43 | 0.10 *** | [0.10, 0.04] | 495 | −2.14 | 0.47 | 0.12 *** | [0.05, 0.30] | 494 | −2.32 | 0.49 | 0.10 *** | [0.04, 0.26] |
| SES Risk | 495 | 0.49 | 0.38 | 1.63 | [0.75, 2.54] | 495 | 0.05 | 0.48 | 1.06 | [0.40, 2.76] | 494 | 0.37 | 0.49 | 1.45 | [0.55, 3.84] |
| Individual risk factors | |||||||||||||||
| Depression severity | 495 | 0.94 | 0.12 | 2.57 *** | [2.04, 3.24] | 495 | 0.86 | 0.12 | 2.36 *** | [1.85, 3.02] | 494 | 0.87 | 0.12 | 2.38 *** | [1.87, 3.03] |
| Substance use | 495 | −0.13 | 0.17 | 0.88 | [0.63, 0.12] | 495 | −0.04 | 0.22 | 0.96 | [0.62, 1.48] | 494 | −0.10 | 0.23 | 0.91 | [0.58, 1.43] |
| Protective factors | |||||||||||||||
| Positive parenting | 493 | −0.50 | 0.16 | 0.61 ** | [0.44, 0.84] | 493 | −0.62 | 0.16 | 0.54 *** | [0.39, 0.74] | 492 | −0.68 | 0.18 | 0.51 *** | [0.36, 0.72] |
| School engagement | 454 | −0.76 | 0.23 | 0.47 ** | [0.30, 0.74] | 454 | −0.49 | 0.20 | 0.61 * | [0.41, 0.92] | 453 | −0.86 | 0.27 | 0.42 ** | [0.24, 0.73] |
| Activities | 494 | 0.01 | 0.06 | 1.01 | [0.89, 1.14] | 494 | 0.04 | 0.07 | 1.04 | [0.91, 1.18] | 493 | 0.03 | 0.08 | 1.03 | [0.88, 1.20] |
| Religiosity | 488 | 0.00 | 0.19 | 1.00 | [0.68, 1.46] | 488 | −0.06 | 0.21 | 0.94 | [0.61, 1.44] | 487 | −0.01 | 0.23 | 0.99 | [0.62, 1.57] |
| Suicidal Ideation (n = 449) | Suicide Plan (n = 449) | Suicide Attempt (n = 448) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Predictor | B | SE B | OR | 95% CI OR | B | SE B | OR | 95% CI OR | B | SE B | OR | 95% CI OR |
| Demographics | ||||||||||||
| Sex (male) | −1.75 | 0.53 | 0.17 ** | [0.06, 0.50] | −1.19 | 0.51 | 0.30 * | [0.11, 0.84] | −1.38 | 0.47 | 0.25 ** | [0.10, 0.65] |
| SES Risk | 0.39 | 0.66 | 1.48 | [0.40, 5.52] | −0.54 | 0.62 | 0.59 | [0.17, 2.05] | 0.07 | 0.75 | 1.08 | [0.24, 4.88] |
| Individual risk factors | ||||||||||||
| Depression severity | 0.92 | 0.16 | 2.51 *** | [1.82, 3.45] | 0.85 | 0.17 | 2.33 *** | [1.65, 3.30] | 0.77 | 0.16 | 2.17 *** | [1.58, 2.97] |
| Substance use | −0.56 | 0.44 | 0.57 | [0.24, 1.38] | −0.22 | 0.32 | 0.80 | [0.42, 1.54] | −0.47 | 0.36 | 0.63 | [0.30, 1.30] |
| Protective factors | ||||||||||||
| Positive parenting | −0.34 | 0.31 | 0.71 | [0.38, 1.33] | −0.66 | 0.29 | 0.52 * | [0.29, 0.93] | −0.55 | 0.33 | 0.58 | [0.30, 1.13] |
| School engagement | −0.34 | 0.32 | 0.71 | [0.38, 1.35] | 0.49 | 0.46 | 1.63 | [0.65, 4.13] | −0.26 | 0.34 | 0.77 | [0.39, 1.52] |
| Activities | 0.13 | 0.08 | 1.13 | [0.97, 1.32] | 0.14 | 0.09 | 1.15 | [0.96, 1.39] | 0.14 | 0.09 | 1.15 | [0.95, 1.37] |
| Religiosity | 0.52 | 0.28 | 1.68 | [0.97, 2.92] | 0.40 | 0.33 | 1.50 | [0.78, 2.88] | 0.37 | 0.42 | 1.45 | [0.62, 3.36] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quinn, C.R.; Duprey, E.B.; Boyd, D.T.; Lynch, R.; Mitchell, M.; Ross, A.; Handley, E.D.; Cerulli, C. Individual and Contextual Risk and Protective Factors for Suicidal Thoughts and Behaviors among Black Adolescents with Arrest Histories. Children 2022, 9, 522. https://doi.org/10.3390/children9040522
Quinn CR, Duprey EB, Boyd DT, Lynch R, Mitchell M, Ross A, Handley ED, Cerulli C. Individual and Contextual Risk and Protective Factors for Suicidal Thoughts and Behaviors among Black Adolescents with Arrest Histories. Children. 2022; 9(4):522. https://doi.org/10.3390/children9040522
Chicago/Turabian StyleQuinn, Camille R., Erinn B. Duprey, Donte T. Boyd, Raven Lynch, Micah Mitchell, Andrew Ross, Elizabeth D. Handley, and Catherine Cerulli. 2022. "Individual and Contextual Risk and Protective Factors for Suicidal Thoughts and Behaviors among Black Adolescents with Arrest Histories" Children 9, no. 4: 522. https://doi.org/10.3390/children9040522