
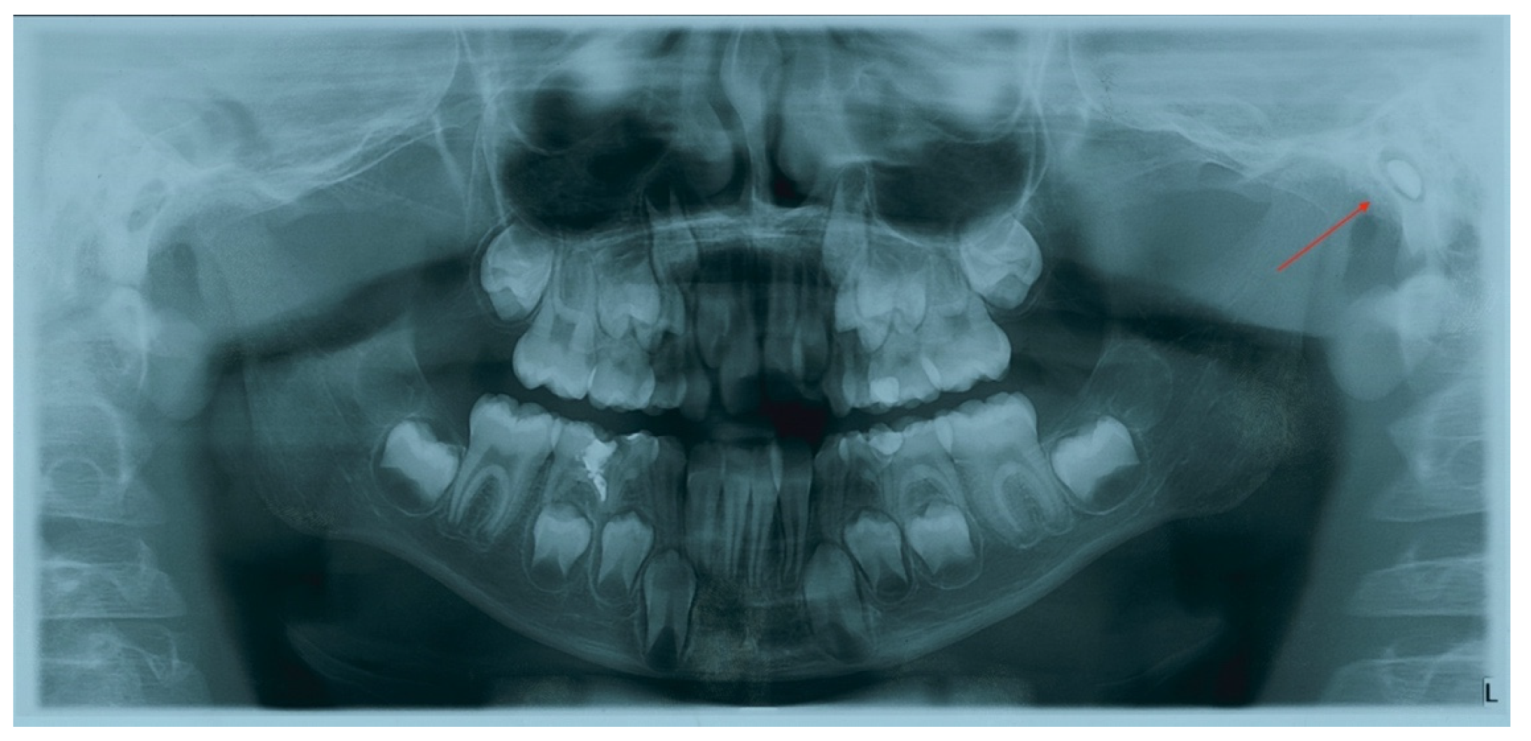
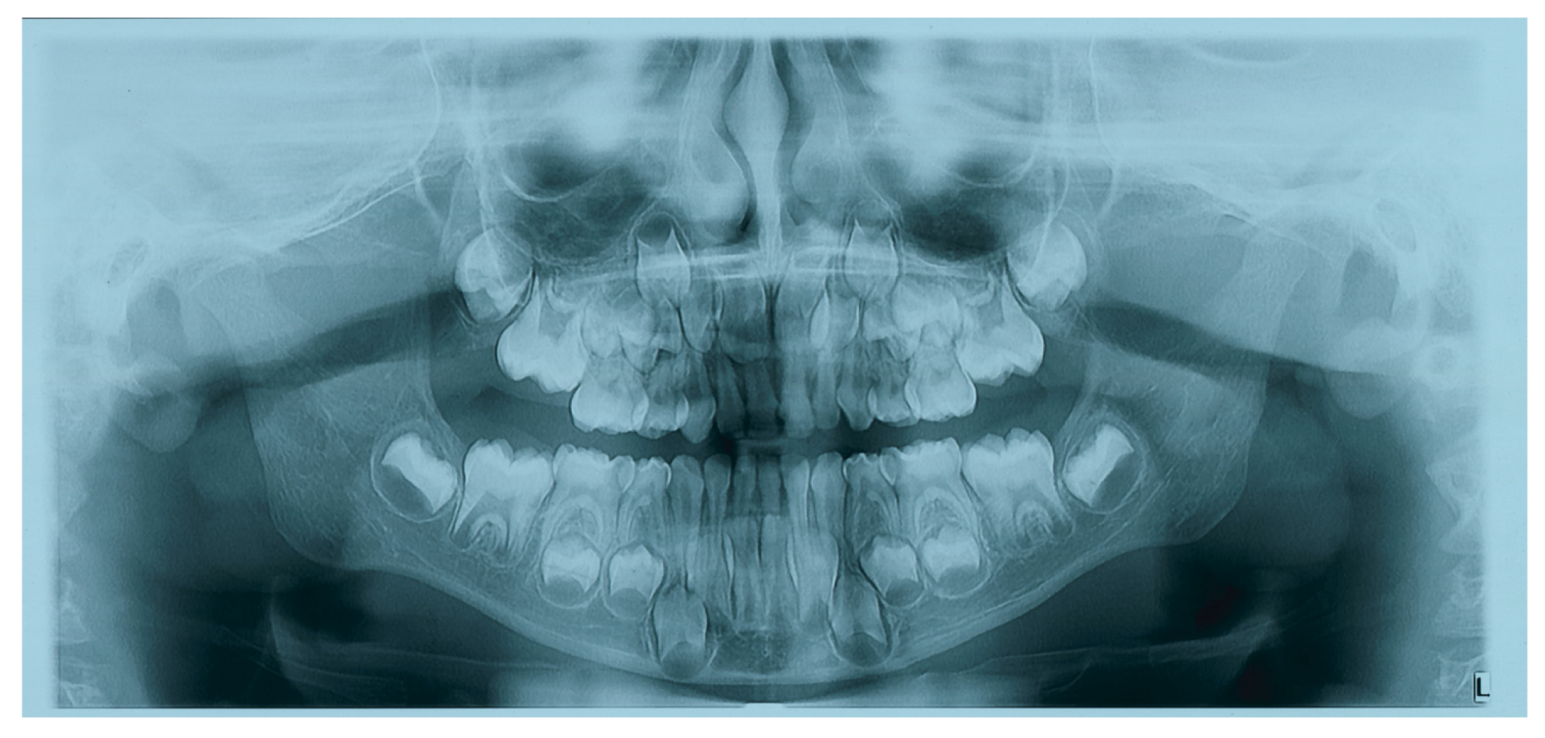
Incidental Finding in Pre-Orthodontic Treatment Radiographs of an Aural Foreign Body: A Case Report

 ,
,  ,
,  ,
,  ,
,  and
and 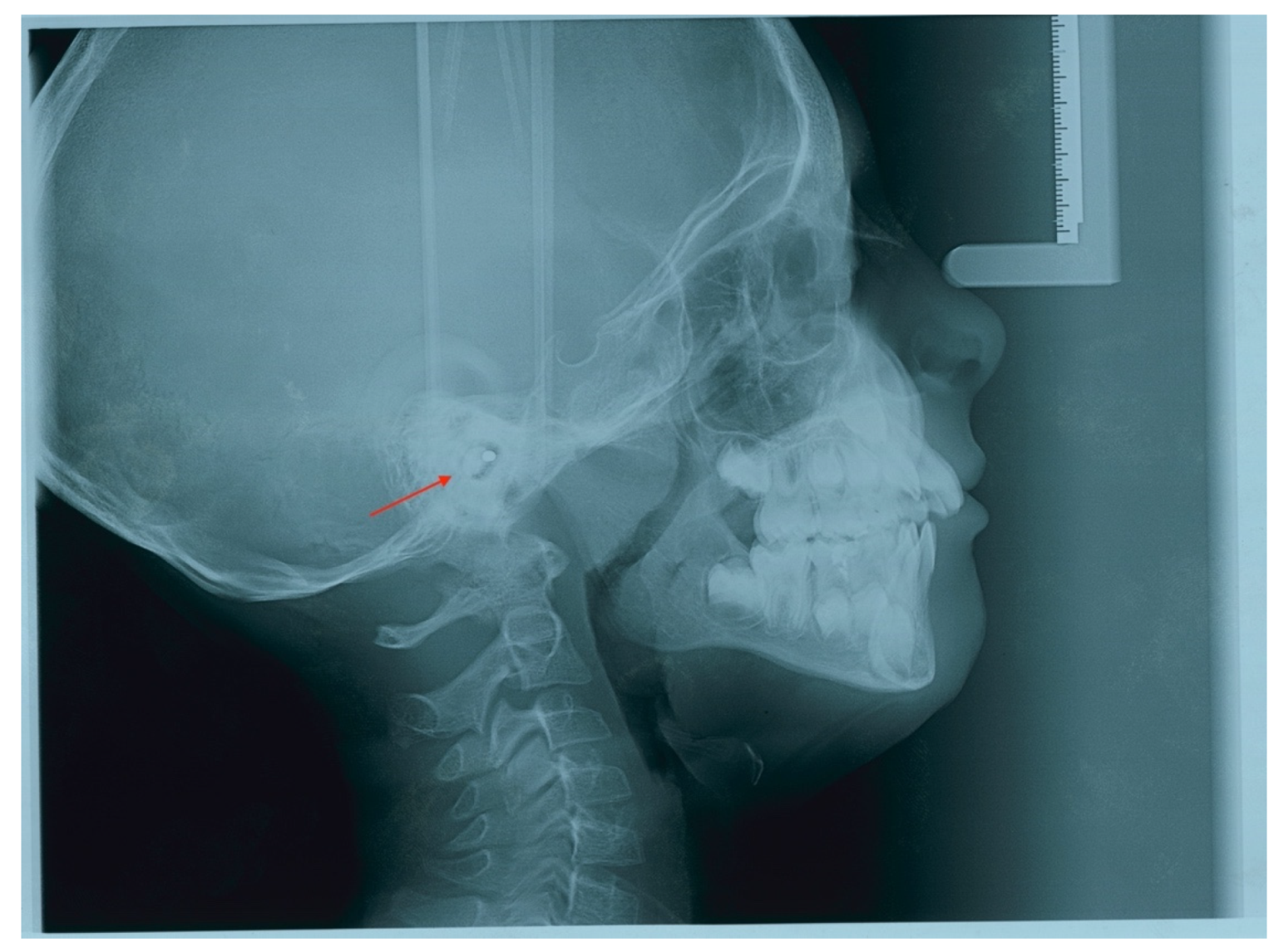{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chalishazar, U.K.; Singh, V. Correlation between a foreign body in the external auditory canal and otitis media with effusion. J. Laryngol. Otol. 2007, 121, 850–852. [Google Scholar] [CrossRef]
- Heim, S.W.; Maughan, K.L. Foreign bodies in the ear, nose, and throat. Am. Fam. Physician 2007, 76, 1185–1189. [Google Scholar] [PubMed]
- Celenk, F.; Gokcen, C.; Celenk, N.; Baysal, E.; Durucu, C.; Kanlikama, M. Association between the self-insertion of nasal and aural foreign bodies and attention-deficit/hyperactivity disorder in children. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 1291–1294. [Google Scholar] [CrossRef]
- Perera, H.; Fernando, S.M.; Yasawardena, A.; Karunaratne, I. Prevalence of attention deficit hyperactivity disorder (ADHD) in children presenting with self-inserted nasal and aural foreign bodies. Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 1362–1364. [Google Scholar] [CrossRef] [PubMed]
- Parelkar, K.; Shere, D.; Wallic, A.; Dave, V.; Rao, K. Impacted Incus Foreign Body in the Eustachian Tube. Iran. J. Otorhinolaryngol. 2019, 31, 123–126. [Google Scholar] [PubMed]
- Farronato, G.; Giannini, L.; Galbiati, G.; Cannalire, P.; Martinelli, G.; Tubertini, I.; Maspero, C. Oral tissues and orthodontic treatment: Common side effects | Tessuti orali e trattamento ortodontico: Effetti avversi più comuni. Minerva Stomatol. 2013, 62, 431–446. [Google Scholar]
- DiMuzio, J., Jr.; Deschler, D.G. Emergency department management of foreign bodies of the external ear canal in children. Otol. Neurotol. 2002, 23, 473–475. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.; Denmark, T.K.; Wittlake, W.A.; Vargas, E.J.; Watson, T.; Crabb, J.W. Procedural sedation use in the ED: Management of pediatric ear and nose foreign bodies. Am. J. Emerg. Med. 2004, 22, 310–314. [Google Scholar]
- Ibekwe, T.; Folorunsho, D.; Oreh, A. Actualities of management of aural, nasal, and throat foreign bodies. Ann. Med. Health Sci. Res. 2015, 5, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Ansley, J.F.; Cunningham, M.J. Treatment of aural foreign bodies in children. Pediatrics 1998, 101, 638–641. [Google Scholar] [CrossRef]
- Abate, A.; Cavagnetto, D.; Rusconi, F.M.E.; Paolo, C.; Luca, E. Safety and Effects of the Rapid Maxillary Expander on Temporomandibular Joint in Subjects Affected by Juvenile Idiopathic Arthritis: A Retrospective Study. Children 2021, 8, 33. [Google Scholar] [CrossRef] [PubMed]
- Vaseemuddin, S. Incidental findings on panoramic radiograph: A clinical study. J. Adv. Med. Dent. Sci. Res. 2016, 4, 223–226. [Google Scholar]
- American Dental Association-Council on Scientific Affairs. Dental Radiographic Examinations: Recommendations for Patient Selection and Limiting Radiation Exposure; US Department of Health and Human Services, Public Health Service Food and Drug Administration; American Dental Association-Council on Scientific Affairs: Silver Spring, ML, USA, 2012. [Google Scholar]
- Tetradis, S.; Kantor, M.L. Prevalence of skeletal and dental anomalies and normal variants seen in cephalometric and other radiographs of orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 1999, 116, 572–577. [Google Scholar] [CrossRef]
- Bondemark, L.; Jeppsson, M.; Lindh-Ingildsen, L.; Rangne, K. Incidental findings of pathology and abnormality in pretreatment orthodontic panoramic radiographs. Angle Orthod. 2006, 76, 98–102. [Google Scholar] [PubMed]
- Cavagnetto, D.; Abate, A.; Caprioglio, A.; Cressoni, P.; Maspero, C. Three-dimensional volumetric evaluation of the different mandibular segments using CBCT in patients affected by juvenile idiopathic arthritis: A cross-sectional study. Prog. Orthod. 2021, 22, 32. [Google Scholar] [CrossRef] [PubMed]
- Farronato, M.; Maspero, C.; Abate, A.; Grippaudo, C.; Connelly, S.T.; Tartaglia, G.M. 3D cephalometry on reduced FOV CBCT: Skeletal class assessment through AF-BF on Frankfurt plane-validity and reliability through comparison with 2D measurements. Eur. Radiol. 2020, 30, 6295–6302. [Google Scholar] [CrossRef] [PubMed]
- Abate, A.; Gaffuri, F.; Lanteri, V.; Fama, A.; Ugolini, A.; Mannina, L.; Maspero, C. A CBCT based analysis of the correlation between volumetric morphology of the frontal sinuses and the facial growth pattern in caucasian subjects. A cross-sectional study. Head Face Med. 2022, 18, 4. [Google Scholar] [CrossRef] [PubMed]
- Cağlayan, F.; Tozoğlu, U. Incidental findings in the maxillofacial region detected by cone beam CT. Diagn. Interv. Radiol. 2012, 18, 159–163. [Google Scholar]
- Edwards, R.; Alsufyani, N.; Heo, G.; Flores-Mir, C. The frequency and nature of incidental findings in large-field cone beam computed tomography scans of an orthodontic sample. Prog. Orthod. 2014, 15, 37. [Google Scholar] [CrossRef] [Green Version]
- Sancar, M. Impacted earring clip visible on panoramic radiograph. Dentomaxillofacial Radiol. 2006, 35, 36–37. [Google Scholar] [CrossRef]
- Schafer, T.; Riggs, B.; Murakaru, J.; Kalathingal, S. Incidental Finding of a Foreign Object on a Panoramic Radiograph. Paediatr. Dent. 2015, 37, 453–454. [Google Scholar]
- Svider, P.F.; Vong, A.; Sheyn, A.; Bojrab, D.I.; Hong, R.S.; Eloy, J.A.; Folbe, A.J. What are we putting in our ears? A consumer product analysis of aural foreign bodies. Laryngoscope 2015, 125, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Peyvandi, A.A.; Jamilian, A.; Moradi, E. Relationship between conductive hearing loss and maxillary constriction. J. Laryngol. Otol. 2014, 128, 765–767. [Google Scholar] [CrossRef] [PubMed]
- Kilic, N.; Kiki, A.; Oktay, H.; Selimoglu, E. Effects of rapid maxillary expansion on conductive hearing loss. Angle Orthod. 2008, 78, 409–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maspero, C.; Abate, A.; Inchingolo, F.; Dolci, C.; Cagetti, M.G.; Tartaglia, G.M. Incidental Finding in Pre-Orthodontic Treatment Radiographs of an Aural Foreign Body: A Case Report. Children 2022, 9, 421. https://doi.org/10.3390/children9030421
Maspero C, Abate A, Inchingolo F, Dolci C, Cagetti MG, Tartaglia GM. Incidental Finding in Pre-Orthodontic Treatment Radiographs of an Aural Foreign Body: A Case Report. Children. 2022; 9(3):421. https://doi.org/10.3390/children9030421
Chicago/Turabian StyleMaspero, Cinzia, Andrea Abate, Francesco Inchingolo, Claudia Dolci, Maria Grazia Cagetti, and Gianluca Martino Tartaglia. 2022. "Incidental Finding in Pre-Orthodontic Treatment Radiographs of an Aural Foreign Body: A Case Report" Children 9, no. 3: 421. https://doi.org/10.3390/children9030421