
Tracheal Length Measurement in Intubated Neonates to Guide the Design and Use of Endotracheal Tube Glottic Depth Markings


Abstract
:1. Introduction
2. Materials and Methods
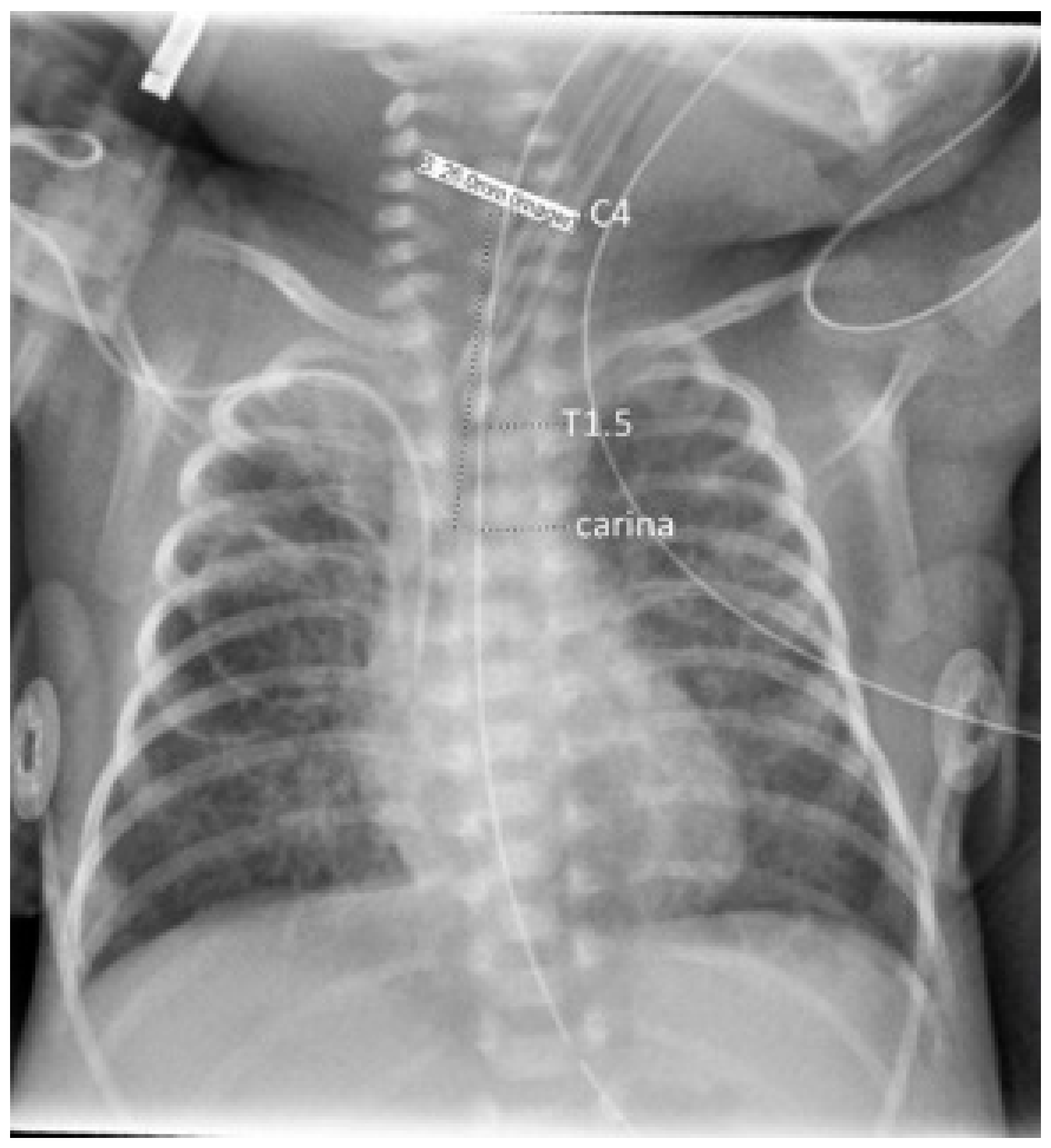
2.1. Measurement of Tracheal Length
2.2. Statistical Analysis
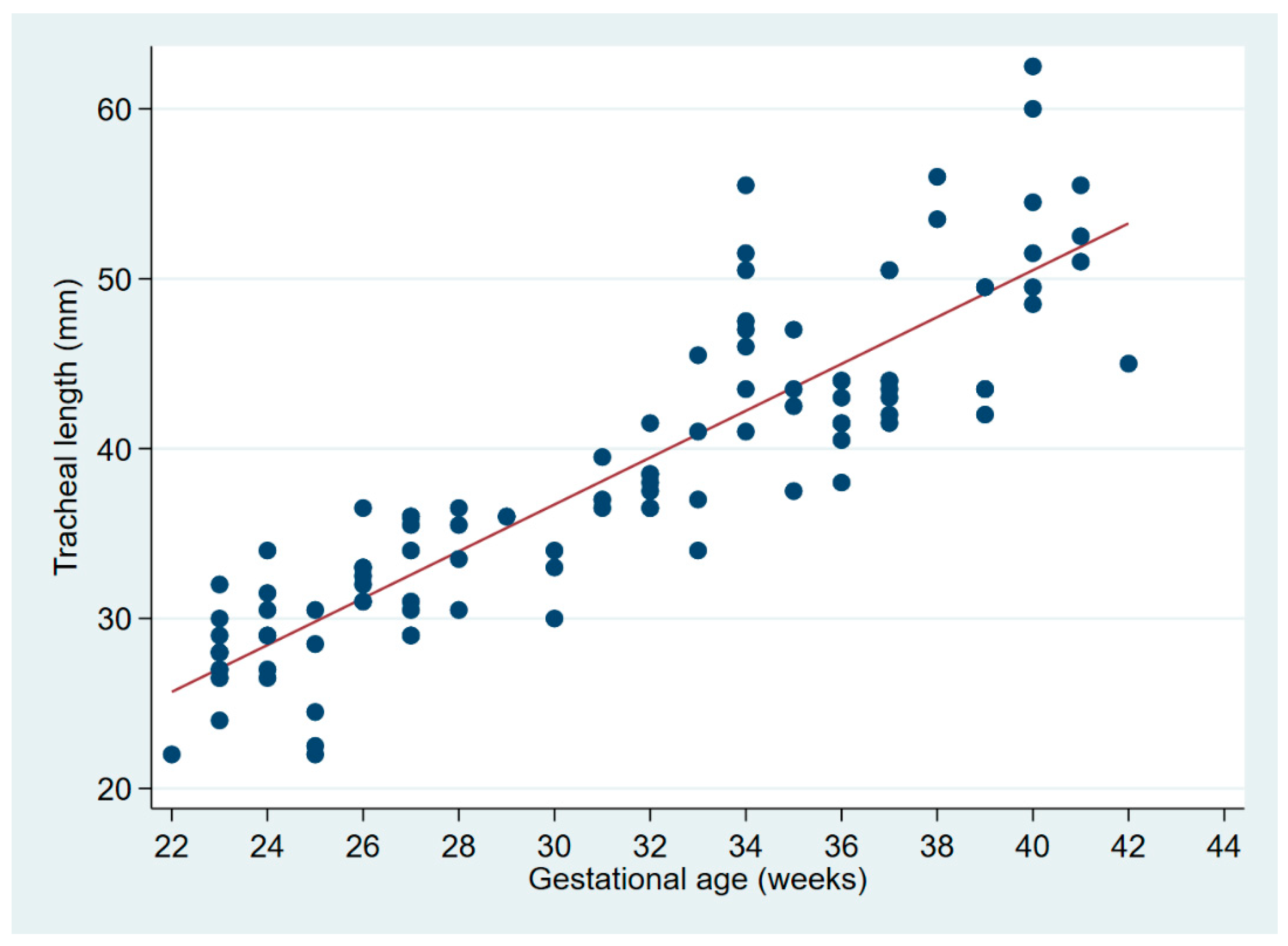
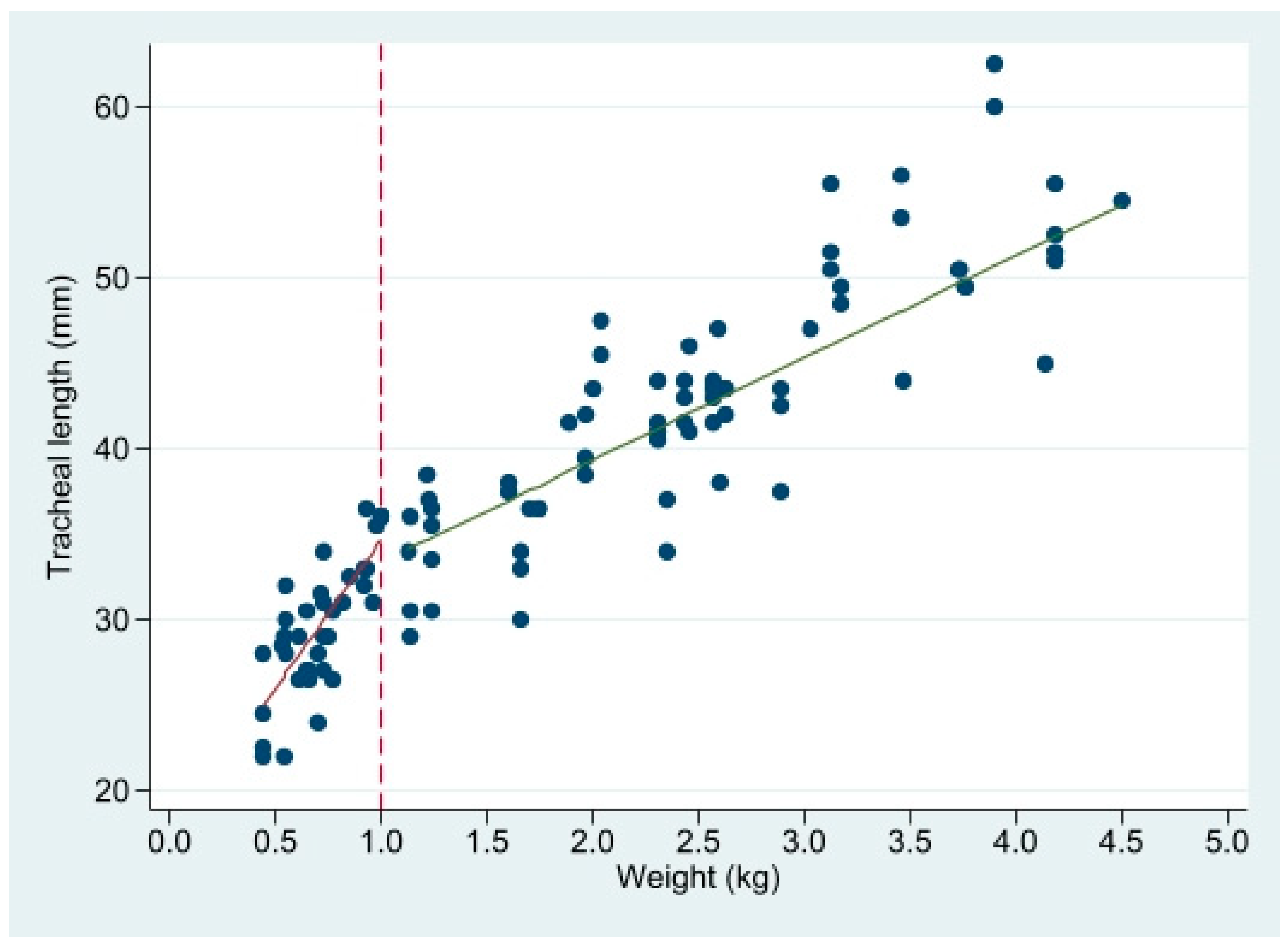
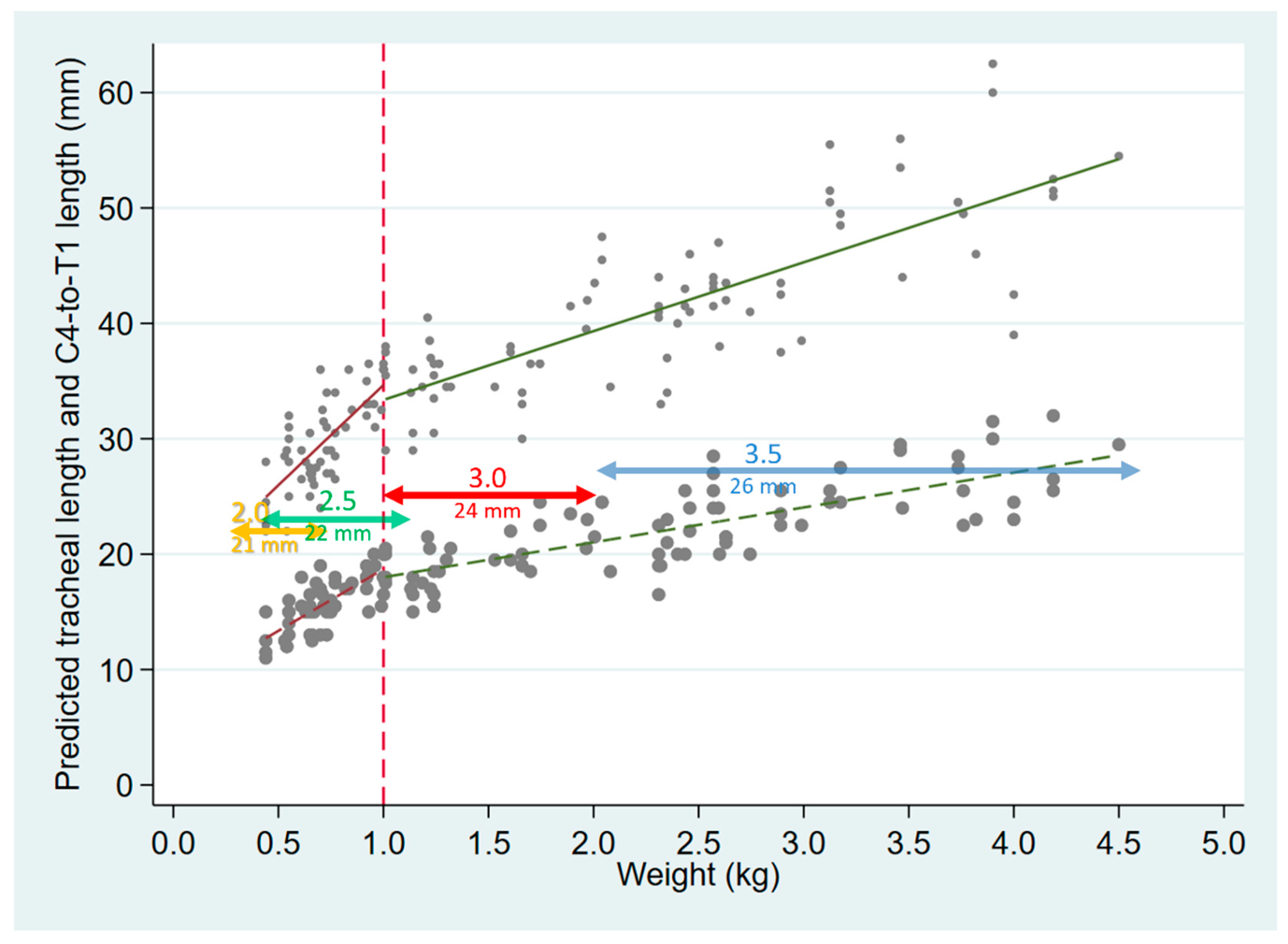
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bednarek, F.J.; Kuhns, L.R. Endotracheal tube placement in infants determined by suprasternal palpation: A new technique. Pediatrics 1975, 56, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Mainie, P.; Carmichael, A.; McCullough, S.; Kempley, S.T. Endotracheal tube position in neonates requiring emergency interhospital transfer. Am. J. Perinatol. 2006, 23, 121–124. [Google Scholar] [CrossRef] [PubMed]
- Subhedar, N.V.; Parry, H.A. Critical incident reporting in neonatal practice. Arch. Dis. Child. Fetal Neonatal Ed. 2010, 95, F378–F382. [Google Scholar] [CrossRef] [PubMed]
- Perlman, J.M.; Risser, R. Cardiopulmonary resuscitation in the delivery room: Associated clinical events. Arch. Pediatr. Adolesc. Med. 1995, 149, 20–25. [Google Scholar] [CrossRef]
- Fayoux, P.; Marciniak, B.; Devisme, L.; Storme, L. Prenatal and early postnatal morphogenesis and growth of human laryngotracheal structures. J. Anat. 2008, 213, 86–92. [Google Scholar] [CrossRef]
- Rotschild, A.; Chitayat, D.; Puterman, M.L.; Phang, M.S.; Ling, E.; Baldwin, V. Optimal positioning of endotracheal tubes for ventilation of preterm infants. Am. J. Dis. Child. 1991, 145, 1007–1012. [Google Scholar] [CrossRef]
- Molendijk, H.; Oetomo, S.B. Re: Rost et al. Describing the effects of neck position on endotracheal tube (ETT) location in low birth weight infants. Pediatr. Pulmonol. 2000, 29, 242–244. [Google Scholar] [CrossRef]
- Pinheiro, J.M.B.; Munshi, U.K. Factors contributing to endobronchial intubation in neonates. Pediatr. Crit. Care Med. 2015, 16, 54–58. [Google Scholar] [CrossRef]
- Whyte, K.L.; Levin, R.; Powls, A. Clinical audit: Optimal positioning of endotracheal tubes in neonates. Scott. Med. J. 2007, 52, 25–27. [Google Scholar] [CrossRef]
- Shukla, H.K.; Hendricks-Munoz, K.D.; Atakent, Y.; Rapaport, S. Rapid estimation of insertional length of endotracheal intubation in newborn infants. J. Pediatr. 1997, 131, 561–564. [Google Scholar] [CrossRef]
- Amarilyo, G.; Mimouni, F.B.; Oren, A.; Tsyrkin, S.; Mandel, D. Orotracheal tube insertion in extremely low birth weight infants. J. Pediatr. 2009, 154, 764–765. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, J.M.B. Orotracheal tube length in ELBW neonates. J. Pediatr. 2010, 156, 170. [Google Scholar] [CrossRef] [PubMed]
- Hewson, M.; Hewson, P. Endotracheal Tube & Umbilical Catheter Calculator. Available online: www.nicutools.org/ (accessed on 17 February 2021).
- Textbook of Neonatal Resuscitation, 7th ed.; American Academy of Pediatrics: Elk Grove Village, IL, USA, 2016.
- Tochen, M.L. Orotracheal intubation in the newborn infant: A method for determining depth of tube insertion. J. Pediatr. 1979, 95, 1050–1051. [Google Scholar] [CrossRef]
- Chung, H.W.; Lee, W.T.; Chen, H.L. Reexamining the ideal depth of endotracheal tube in neonates. Pediatr. Neonatol. 2018, 59, 258–262. [Google Scholar] [CrossRef] [Green Version]
- Loew, A.; Thibeault, D.W. A new and safe method to control the depth of endotracheal intubation in neonates. Pediatrics 1974, 54, 506–508. [Google Scholar] [CrossRef]
- Molendijk, H. Use of the black area on the tubetip for rapid estimation of insertional depth of endotracheal tubes in neonates: A potential hazard. Arch. Dis. Child. Fetal Neonatal Ed. 2001, 85, F77. [Google Scholar] [CrossRef] [Green Version]
- Goel, S.; Lim, S.L. The intubation depth marker: The confusion of the black line. Paediatr. Anaesth. 2003, 13, 579–583. [Google Scholar] [CrossRef]
- Cordero, L.; Dzwonczyk, R.; Timan, C. Inconsistencies of endotracheal tube markings: Clinical implications for neonates. Neonatal Intensive Care 2001, 14, 13–16. [Google Scholar]
- Gill, I.; O’Donnell, C.P. Vocal cord guides on neonatal endotracheal tubes. Arch. Dis. Child. Fetal Neonatal Ed. 2014, 99, F344. [Google Scholar] [CrossRef]
- Sinha, R.; Ranjan Ray, B. Confusion due to site of tracheal tube size marking. Anaesthesia 2012, 67, 72. [Google Scholar] [CrossRef]
- Rigo, V.; Fayoux, P. Distances from vocal cords to mid-trachea for optimizing endotracheal tubes depth markers according to gestational age. Paediatr. Anaesth. 2018, 28, 361–366. [Google Scholar] [CrossRef]
- Griscom, N.T.; Wohl, M.E. Dimensions of the growing trachea related to age and gender. AJR Am. J. Roentgenol. 1986, 146, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Wells, T.R.; Landing, B.H.; Padua, E.M. The question of parallax-effect on radiographic assessment of short trachea in infants and children. Pediatr. Radiol. 1991, 21, 490–493. [Google Scholar] [CrossRef] [PubMed]
- Szpinda, M.; Daroszewski, M.; Szpinda, A.; Wozniak, A.; Wisniewski, M.; Mila-Kierzenkowska, C.; Baumgart, M.; Paruszewska-Achtel, M. New quantitative patterns of the growing trachea in human fetuses. Med. Sci. Monit. 2012, 18, H63–H70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fearon, B.; Whalen, J.S. Tracheal dimensions in the living infant (preliminary report). Ann. Otol. Rhinol. Laryngol. 1967, 76, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Awsar, S.; Brown, K. Novel markings on the unit package of uncuffed pediatric tracheal tubes. Can. J. Anaesth. 2019, 66, 840–841. [Google Scholar] [CrossRef] [Green Version]
- Sirisopana, M.; Saint-Martin, C.; Wang, N.N.; Manoukian, J.; Nguyen, L.H.; Brown, K.A. Novel measurements of the length of the subglottic airway in infants and young children. Anesth. Analg. 2013, 117, 462–470. [Google Scholar] [CrossRef]
- Noback, G.J. The developmental topography of the larynx, trachea and lungs in the fetus, newborn, infant and child. Am. J. Dis. Child. 1923, 26, 515–533. [Google Scholar]
- Westhorpe, R.N. The position of the larynx in children and its relationship to the ease of intubation. Anaesth. Intensive Care 1987, 15, 384–388. [Google Scholar] [CrossRef] [Green Version]
- Thayyil, S.; Nagakumar, P.; Gowers, H.; Sinha, A. Optimal endotracheal tube tip position in extremely premature infants. Am. J. Perinatol. 2008, 25, 13–16. [Google Scholar] [CrossRef]
- Blayney, M.P.; Logan, D.R. First thoracic vertebral body as reference for endotracheal tube placement. Arch. Dis. Child. Fetal Neonatal Ed. 1994, 71, F32–F35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balu, R.; Bustani, P. Are we focusing on the wrong end of neonatal endotracheal tube? Arch. Dis. Child 2010, 95, A89. [Google Scholar] [CrossRef]
- Gill, I.; Stafford, A.; Murphy, M.C.; Geoghegan, A.R.; Crealey, M.; Laffan, E.; O’Donnell, C.P.F. Randomised trial of estimating oral endotracheal tube insertion depth in newborns using weight or vocal cord guide. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F312–F316. [Google Scholar] [CrossRef] [PubMed]
- Tupprasoot, R.; Langan, D.; Hutchinson, J.C.; Barrett, H.; Sury, M.R.J.; Arthurs, O.J. Three-dimensional imaging-based web application for predicting tracheal tube depth in preterm neonates. Neonatology 2017, 111, 376–382. [Google Scholar] [CrossRef] [Green Version]
- Embleton, N.D.; Deshpande, S.A.; Scott, D.; Wright, C.; Milligan, D.W. Foot length, an accurate predictor of nasotracheal tube length in neonates. Arch. Dis. Child. Fetal Neonatal Ed. 2001, 85, F60–F64. [Google Scholar] [CrossRef]
- Hipolito, R.B.; Milstein, J.M.; Sherman, J.; Sherman, M.P. Neonatal endotracheal tubes and prevention of bronchial intubation. J Paediatr. Neonatal Dis. 2015, 1, 101. [Google Scholar]
- Kempley, S.T.; Moreiras, J.W.; Petrone, F.L. Endotracheal tube length for neonatal intubation. Resuscitation 2008, 77, 369–373. [Google Scholar] [CrossRef]
- Kempley, S.T. Neonatal endotracheal intubation: The 7-8-9 rule. Arch. Dis. Child. Educ. Pract. Ed. 2009, 94, 29. [Google Scholar]
- Bartle, R.M.; Miller, A.G.; Diez, A.J.; Smith, P.B.; Gentile, M.A.; Puia-Dumitrescu, M. Evaluating endotracheal tube depth in infants weighing less than 1 kilogram. Respiratory Care 2018, 64, 243–247. [Google Scholar] [CrossRef]
- Takeuchi, S.; Arai, J.; Nagafuji, M.; Hinata, A.; Kamakura, T.; Hoshino, Y.; Yukitake, Y. Ideal endotracheal tube insertion depth in neonates with a birth weight less than 750 g. Pediatr. Int. 2020, 62, 932–936. [Google Scholar] [CrossRef]
- Wood, A.J.; Raynes-Greenow, C.H.; Carberry, A.E.; Jeffery, H.E. Neonatal length inaccuracies in clinical practice and related percentile discrepancies detected by a simple length-board. J. Paediatr. Child. Health 2013, 49, 199–203. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | Coefficient | Std Err | p | (95% CI) |
|---|---|---|---|---|
| Weight < 1 kg | 17.3 | 2.9 | <0.001 | (11.6, 23.2) |
| Weight > 1 kg | 6.0 | 0.4 | <0.001 | (5.2, 6.8) |
| Intercept2 | −1.3 | 1.2 | 0.267 | (−3.6, 1.0) |
| Constant | 17.3 | 2.2 | <0.001 | (12.9, 21.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cerone, J.B.; Pinheiro, J.M.B. Tracheal Length Measurement in Intubated Neonates to Guide the Design and Use of Endotracheal Tube Glottic Depth Markings. Children 2022, 9, 169. https://doi.org/10.3390/children9020169
Cerone JB, Pinheiro JMB. Tracheal Length Measurement in Intubated Neonates to Guide the Design and Use of Endotracheal Tube Glottic Depth Markings. Children. 2022; 9(2):169. https://doi.org/10.3390/children9020169
Chicago/Turabian StyleCerone, Jennifer B., and Joaquim M. B. Pinheiro. 2022. "Tracheal Length Measurement in Intubated Neonates to Guide the Design and Use of Endotracheal Tube Glottic Depth Markings" Children 9, no. 2: 169. https://doi.org/10.3390/children9020169