
Parents’ Awareness of Malocclusion and Orthodontic Consultation for Their Children: A Cross-Sectional Study

 ,
, 
Abstract
:1. Introduction
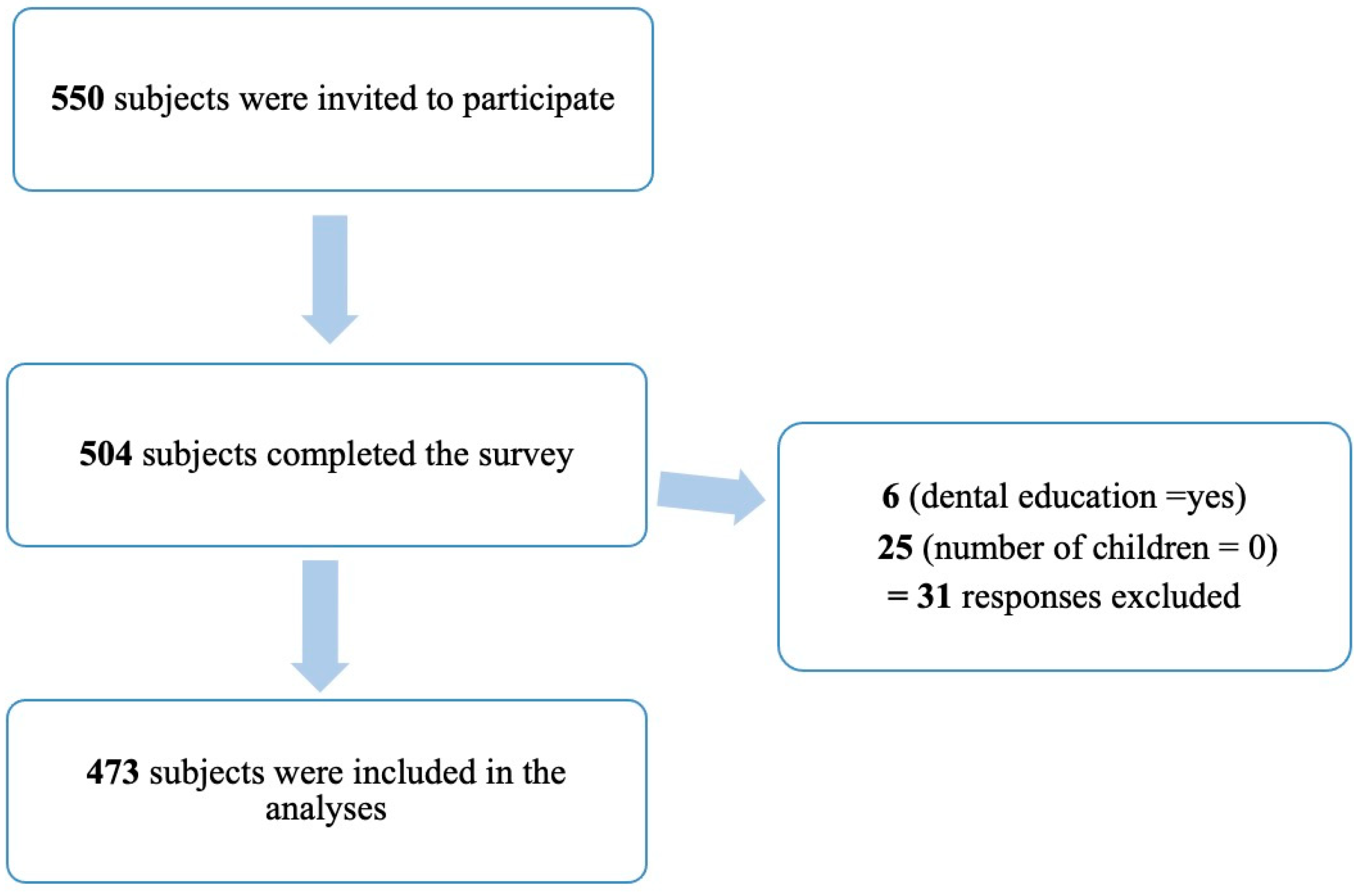
2. Materials and Methods
2.1. The Questionnaire
- Do you think a beautiful smile is important for the healthy development of a child’s personality? Answers were “Yes” or “No”.
- What are the causes of malocclusion in children? Responses were: “Heredity”, “Bad oral habits like mouth breathing or thumb sucking”, “Both” and “I don’t know”.
- If a primary tooth was lost prematurely due to decay. What should be done? Responses were: “Nothing. The permanent tooth will replace it”, “check if a space maintainer is needed” and “I don’t know”.
- Who will you first go to consult regarding orthodontic treatment for your child? Responses were: “a general physician/pediatrician”, “a general dentist”, “an orthodontist” and “I don’t know”.
- At what age should your child go to his/her first orthodontic consultation? Responses were: “7 years”, “10 years”, “13 years”, “18 years” and “I don’t know”.
- Do you think the age of a person when starting orthodontic treatment can affect the treatment outcome? Responses were: “Yes”, “No” or “I don’t know”.
- Do you think children can have orthodontic treatment during their growth period? Responses were: “Yes”, “No” or “I don’t know”.
2.2. Statistical Analysis
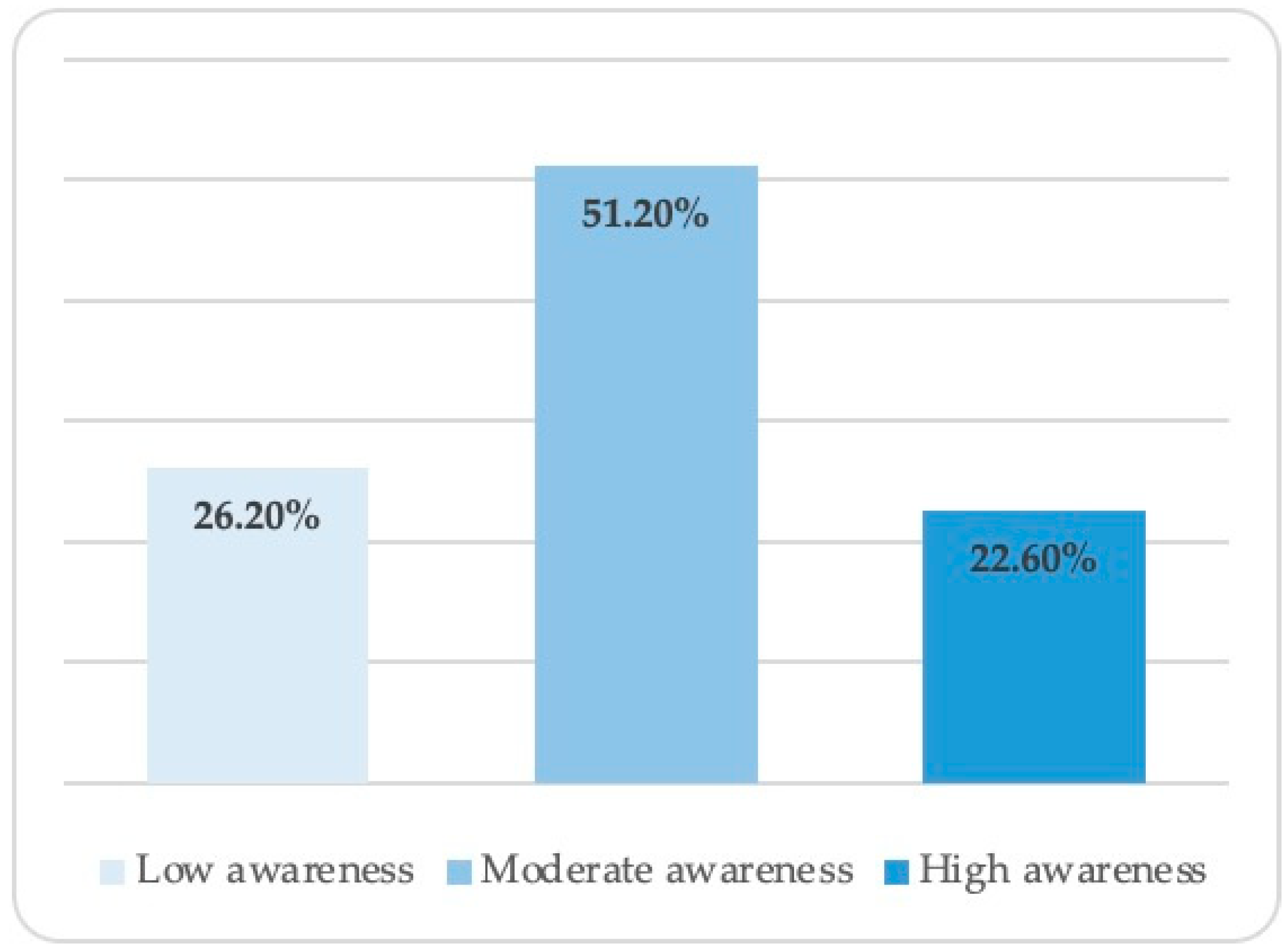
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Dental Association. National Commission on Recognition of Dental Specialties and Certifying Boards: Definitions of the recognized dental Specialties (Adopted May 2018). Available online: https://ncrdscb.ada.org/recognized-dental-specialties/ (accessed on 19 October 2022).
- Jung, M.-H. Evaluation of the effects of malocclusion and orthodontic treatment on self-esteem in an adolescent population. Am. J. Orthod. Dentofacial. Orthop. 2010, 138, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Javidi, H.; Vettore, M.; Benson, P.E. Does orthodontic treatment before the age of 18 years improve oral health-related quality of life? A systematic review and meta-analysis. Am. J. Orthod. Dentofacial. Orthop. 2017, 151, 644–655. [Google Scholar] [CrossRef] [PubMed]
- Feu, D.; Miguel, J.A.M.; Celeste, R.K.; Oliveira, B.H. Effect of orthodontic treatment on oral health–related quality of life. Angle Orthod. 2013, 83, 892–898. [Google Scholar] [CrossRef] [PubMed]
- Dimberg, L.; Arnrup, K.; Bondemark, L. The impact of malocclusion on the quality of life among children and adolescents: A systematic review of quantitative studies. Eur. J. Orthod. 2014, 37, 238–247. [Google Scholar] [CrossRef]
- Basha, S.; Mohamed, R.N.; Swamy, H.S.; Parameshwarappa, P. Untreated Gross Dental Malocclusion in Adolescents: Psychological Impact and Effect on Academic Performance in School. Oral Health Prev. Dent. 2016, 14, 63–69. [Google Scholar] [CrossRef]
- Taibah, S.M.; Al-Hummayani, F.M. Effect of malocclusion on the self-esteem of adolescents. J. Orthod. Sci. 2017, 6, 123–128. [Google Scholar] [CrossRef]
- Grippaudo, M.M.; Quinzi, V.; Manai, A.; Paolantonio, E.G.; Valente, F.; La Torre, G.; Marzo, G. Orthodontic treatment need and timing: Assessment of evolutive malocclusion conditions and associated risk factors. Eur. J. Paediatr. Dent. 2020, 21, 203–208. [Google Scholar] [CrossRef]
- Grippaudo, C.; Pantanali, F.; Paolantonio, E.G.; Saulle, R.; Latorre, G.; Deli, R. Orthodontic treatment timing in growing patients. Eur. J. Paediatr. Dent. 2013, 14, 231–236. [Google Scholar]
- Wong, M.L.; Che Fatimah, A.; Ng, L.K.; Norlian, D.; Rashidah Dato, B.; Gere, M.J. Role of interceptive orthodontics in early mixed dentition. Singapore Dent. J. 2004, 26, 10–14. [Google Scholar]
- American Association of Orthodontics [Homepage on the Internet]. St. Louis Missouri: The Association. The First Visit. Available online: https://www3.aaoinfo.org/blog/parent-s-guide-post/first-visit/ (accessed on 10 September 2022).
- Felemban, O.; Alharbi, N.; AAlamoudi, R.; Alturki, G.; Helal, N. Factors influencing the desire for orthodontic treatment among patients and parents in Saudi Arabia: A cross-sectional study. J. Orthod. Sci. 2022, 11, 25. [Google Scholar] [CrossRef]
- Marques, L.S.; Pordeus, I.A.; Ramos-Jorge, M.L.; Filogônio, C.A.; Filogônio, C.B.; Pereira, L.J.; Paiva, S.M. Factors associated with the desire for orthodontic treatment among Brazilian adolescents and their parents. BMC Oral. Health 2009, 9, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zakirulla, M.; Almubarak, H.; Fageeh, S.N.; Alghothimi, A.A.; Alqahtani, S.K.; Alqahtani, F.M.; Alshahrani, F.T. Awareness and Behaviour Related to Orthodontic Treatment among School Children in Aseer Region, Kingdom of Saudi Arabia. Open J. Stomatol. 2019, 09, 8. [Google Scholar] [CrossRef]
- Basri, O.; Alghamdi, E.; Amoudi, A.; Filimban, L.; Darwish, H.; Alsaman, F.; Alzahrani, K. Evaluation of parent’s knowledge and awareness towards early orthodontic treatment for their children among Saudi Arabia. Med. Sci. 2021, 25, 3409–3416. [Google Scholar]
- Aldweesh, A.H.; Ben Gassem, A.A.; AlShehri, B.M.; AlTowaijri, A.A.; Albarakati, S.F. Parents’ Awareness of Early Orthodontic Consultation: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 1800. [Google Scholar] [CrossRef] [PubMed]
- Tabbaa, M.Y.; Albarkheel, A.R.; Al Mubarak, S. Parents’ Knowledge and Awareness of Orthodontics and Orthodontic Treatment in Saudi Arabia. Int. J. Sci. Res. 2020, 9, 599–604. [Google Scholar] [CrossRef]
- Alnaafa, M.; Altamimi, Y.; Alajlan, S.; Alateeq, N.; Almarshedi, A.; Alsaleh, M.; Alsuwailem, R.; Patil, S.; Alam, M.K. The parental awareness regarding early orthodontic treatment in Hail city. Int. Med. J. 2020, 27, 220–223. [Google Scholar]
- Järvinen, S. Incisal overjet and traumatic injuries to upper permanent incisors. A retrospective study. Acta Odontol. Scand. 1978, 36, 359–362. [Google Scholar] [CrossRef]
- Arraj, G.P.; Rossi-Fedele, G.; Doğramacı, E.J. The association of overjet size and traumatic dental injuries-A systematic review and meta-analysis. Dent. Traumatol. 2019, 35, 217–232. [Google Scholar] [CrossRef] [Green Version]
- Alhummayani, F.M.; Taibah, S.M. Orthodontic treatment needs in Saudi young adults and manpower requirements. Saudi Med. J. 2018, 39, 822–828. [Google Scholar] [CrossRef]
- Linjawi, A.I.; Alajlan, S.A.; Bahammam, H.A.; Alabbadi, A.M.; Bahammam, M.A. Space maintainers: Knowledge and awareness among Saudi adult population. J. Int. Oral Health 2016, 8, 733. [Google Scholar]
- Almarhoumi, A.; Alharbi, M.; Saib, S.; Albalawi, S.; Alalawi, A.; Albahith, S. Parental Knowledge and Practice Regarding their Children’s Malocclusion and Orthodontic Care in Al-Madinah, Saudi Arabia: A Cross-sectional Study. J. Oral Health Comm. Dent. 2022, 16, 57. [Google Scholar]
- Al-Khalifa, K.S.; AlDabbus, H.R.; Almadih, A.I.; Alaqeeli, H.M.; Almarshoud, A.A.; Muhana, M.H.; Alzaidani, S.; Nassar, E. Comparison of orthodontic treatment need among professionals and parents in Dammam, Saudi Arabia. Niger. J. Clin. Pract. 2021, 24, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Moshkelgosha, V.; Kazemi, M.; Pakshir, H.; Safari, R. Parental knowledge and attitude towards early orthodontic treatment for their primary school children. Iran J. Orthod. 2017, 12, e7377. [Google Scholar] [CrossRef]
- Pratelli, P.; Gelbier, S.; Gibbons, D. Parental perceptions and attitudes on orthodontic care. Br. J. Orthod. 1998, 25, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Bos, A.; Hoogstraten, J.; Prahl-Andersen, B. Attitudes towards orthodontic treatment: A comparison of treated and untreated subjects. Eur. J. Orthod. 2005, 27, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Prithiviraj, D.; Siddiqui, N.R.; Smyth, R.S.; Hodges, S.J.; Sharif, M.O. The awareness and usage of orthodontic apps and social media by orthodontists in the UK: A questionnaire-based study. J. Orthod. 2022, 2022, 14653125221094334. [Google Scholar] [CrossRef]
- Siddiqui, N.; Chia, M.; Sharif, M.O. Social media and orthodontics: Are our patients scrolling? J. Orthod. 2022, 49, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Scribante, A.; Gallo, S.; Bertino, K.; Meles, S.; Gandini, P.; Sfondrini, M.F. The Effect of Chairside Verbal Instructions Matched with Instagram Social Media on Oral Hygiene of Young Orthodontic Patients: A Randomized Clinical Trial. Appl. Sci. 2021, 11, 706. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | n (%) |
|---|---|
| Gender | |
| Male | 201(42.5) |
| Female | 272 (57.5) |
| Age group | |
| 18–29 years | 76 (16.1) |
| 30–39 years | 204 (43.1) |
| 40 and above | 193 (40.8) |
| Education | |
| <High school diploma | 31 (6.6) |
| High school diploma | 156 (33.0) |
| Bachelor’s degree | 269 (56.9) |
| Postgraduate degree | 17 (3.6) |
| Marital Status | |
| Married | 439 (92.8) |
| Divorced | 22 (4.7) |
| Widowed | 12 (2.5) |
| Employment | |
| Unemployed | 165 (34.9) |
| Employed | 308 (65.1) |
| Number of children | |
| 1 | 85 (18.0) |
| 2 | 124 (26.2) |
| 3 | 95 (20.1) |
| ≥4 | 169 (35.7) |
| Previous or current orthodontic treatment | |
| Yes | 126 (26.6) |
| No | 347 (73.4) |
| Variable | n (%) |
|---|---|
| A beautiful smile is important for healthy development of the child’s personality. | |
| Yes | 462 (97.7) |
| No | 11 (2.3) |
| The causes of malocclusion in children are: | |
| Heredity | 47 (9.9) |
| Bad oral habits like mouth breathing or thumb sucking | 79 (16.7) |
| Both * | 244 (51.6) |
| I don’t know | 103 (21.8) |
| If a primary tooth was lost prematurely due to decay. What should be done? | |
| Nothing. The permanent tooth will replace it | 241 (51.0) |
| Check if a space maintainer is needed * | 181 (38.3) |
| I don’t know | 51 (10.8) |
| Who will you first go to consult regarding orthodontic treatment for your child? | |
| General physician/pediatrician | 34 (7.2) |
| General dentist | 81 (17.1) |
| Orthodontist * | 332 (70.2) |
| I don’t know | 26 (5.5) |
| At what age should your child go to his/her first orthodontic consult? | |
| 7 years * | 135 (28.5) |
| 10 years | 56 (11.8) |
| 13 years | 113 (23.9) |
| 18 years | 77 (16.3) |
| I don’t know | 92 (19.5) |
| Do you think the age of a person when starting orthodontic treatment can affect the treatment outcome? | |
| No | 100 (21.1) |
| Yes * | 323 (68.3) |
| I don’t know | 50 (10.6) |
| Do you think children can have orthodontic treatment during their growth period? | |
| No | 248 (52.4) |
| Yes * | 167 (35.3) |
| I don’t know | 58 (12.3) |
| Variable | Awareness Level | p Value | ||
|---|---|---|---|---|
| Low | Moderate | High | ||
| Gender | ||||
| Male | 35.30% | 45.80% | 18.90% | <0.001 |
| Female | 19.50% | 55.10% | 25.40% | |
| Age group | ||||
| 18–29 years | 25.00% | 57.90% | 17.10% | 0.32 |
| 30–39 years | 29.90% | 48.00% | 22.10% | |
| 40 and above | 26.20% | 51.80% | 25.40% | |
| Education | ||||
| ≤High school diploma | 35.30% | 49.70% | 15.00% | <0.001 |
| ≥Bachelor’s degree | 20.30% | 52.10% | 27.60% | |
| Marital Status | ||||
| Married | 26.20% | 50.60% | 23.20% | 0.1 |
| Divorced | 34.80% | 43.50% | 21.70% | |
| Widowed | 9.10% | 90.90% | 0.00% | |
| Employment | ||||
| Unemployed | 27.30% | 53.90% | 18.80% | 0.34 |
| Employed | 25.60% | 49.70% | 24.70% | |
| Number of children | ||||
| 1 | 35.30% | 52.90% | 11.80% | 0.07 |
| 2 | 26.60% | 49.20% | 24.20% | |
| 3 | 28.40% | 49.50% | 22.10% | |
| ≥4 | 20.10% | 52.70% | 27.20% | |
| Previous or current orthodontic treatment | ||||
| Yes | 19.80% | 38.90% | 41.30% | <0.001 |
| No | 28.50% | 55.60% | 15.90% | |
| Adjusted Odds Ratio (95% Confidence Interval) | |||
|---|---|---|---|
| Predictors | Low Awareness | Moderate Awareness | High Awareness |
| Age group | Reference | ||
| 18–29 years | Ref. | Ref | |
| 30–39 years | 1.5 (0.8–2.8) | 1.6 (0.8–3.5) | |
| 40 and above | 1.2 (0.6–2.2) | 1.7 (0.8–3.5) | |
| Gender | |||
| Male | Ref. | Ref. | |
| female | 3.3 (1.8–5.8) *** | 0.9 (0.5–1.6) | |
| Employment | Ref. | ||
| employed | Ref. | 0.6 (0.4–1.2) | |
| unemployed | 2.1 (1.1–3.8) * | ||
| Previous or current orthodontic treatment | |||
| No | Ref. | Ref. | |
| Yes | 1.2 (0.7–2.1) | 3.9 (2.4–6.5) *** | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsaggaf, D.H.; Alqarni, M.Z.; Barayan, S.A.; Assaggaf, A.A.; Alansari, R.A. Parents’ Awareness of Malocclusion and Orthodontic Consultation for Their Children: A Cross-Sectional Study. Children 2022, 9, 1974. https://doi.org/10.3390/children9121974
Alsaggaf DH, Alqarni MZ, Barayan SA, Assaggaf AA, Alansari RA. Parents’ Awareness of Malocclusion and Orthodontic Consultation for Their Children: A Cross-Sectional Study. Children. 2022; 9(12):1974. https://doi.org/10.3390/children9121974
Chicago/Turabian StyleAlsaggaf, Doaa H., Manal Z. Alqarni, Shroouq A. Barayan, Abdullah A. Assaggaf, and Reem A. Alansari. 2022. "Parents’ Awareness of Malocclusion and Orthodontic Consultation for Their Children: A Cross-Sectional Study" Children 9, no. 12: 1974. https://doi.org/10.3390/children9121974