
The Effect of Robot-Led Distraction during Needle Procedures on Pain-Related Memory Bias in Children with Chronic Diseases: A Pilot and Feasibility Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
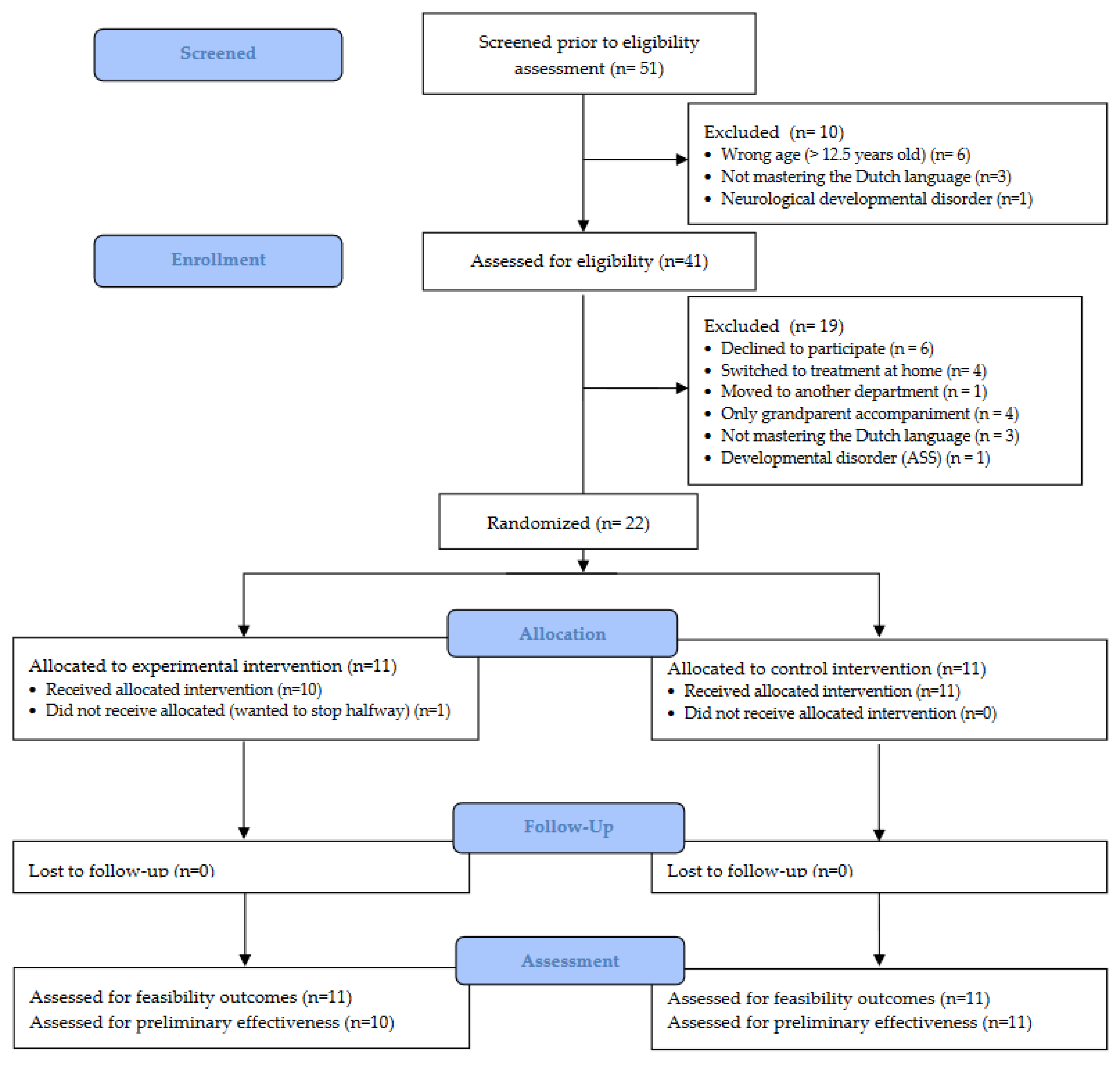
2.1. Study Design
2.2. Protocol Deviations
2.3. Participants
2.4. Procedure
2.5. Intervention
2.5.1. Control Group: Usual Care
2.5.2. Experimental Group: Robot-Led Distraction
2.6. Feasibility Outcomes
2.6.1. Study Procedures
2.6.2. Needle-Procedure-Related Characteristics
2.6.3. Intervention Fidelity
2.6.4. Intervention Acceptability
2.6.5. Nurse Perception of the Intervention
2.7. Clinical Outcomes
2.7.1. Pain Intensity
2.7.2. Pain-Related Fear
2.7.3. Self-Efficacy
2.7.4. State Pain Catastrophic Thoughts
2.7.5. Memory Bias
2.8. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Feasibility Outcomes
3.2.1. Study Procedures
3.2.2. Needle-Procedure-Related Characteristics
3.2.3. Intervention Fidelity
3.2.4. Intervention Acceptability
3.2.5. Nurse Perception of the Intervention
3.3. Clinical Outcomes
4. Discussion
4.1. Intervention Feasibility
4.2. Clinical Effectiveness
4.3. Recommendations and Future Directions
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Birnie, K.A.; Noel, M.; Chambers, C.T.; Uman, L.S.; Parker, J.A. Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database Syst. Rev. 2018, 10, Cd005179. [Google Scholar] [CrossRef] [PubMed]
- Farrier, C.E.; Pearson, J.D.R.; Beran, T.N. Children’s Fear and Pain During Medical Procedures: A Quality Improvement Study With a Humanoid Robot. Can. J. Nurs. Res. 2019, 52, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Jacobse, J.; Ten Voorde, W.; Rissmann, R.; Burggraaf, J.; Ten Cate, R.; Schrier, L. The effect of repeated methotrexate injections on the quality of life of children with rheumatic diseases. Eur. J. Pediatr. 2019, 178, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Aykanat Girgin, B.; Göl, İ. Reducing Pain and Fear in Children During Venipuncture: A Randomized Controlled Study. Pain Manag. Nurs 2020, 21, 276–282. [Google Scholar] [CrossRef]
- Sahiner, N.C.; Bal, M.D. The effects of three different distraction methods on pain and anxiety in children. J. Child Health Care 2016, 20, 277–285. [Google Scholar] [CrossRef]
- Liossi, C.; White, P.; Hatira, P. Randomized clinical trial of local anesthetic versus a combination of local anesthetic with self-hypnosis in the management of pediatric procedure-related pain. Health Psychol. 2006, 25, 307–315. [Google Scholar] [CrossRef] [Green Version]
- Loeffen, E.A.H.; Mulder, R.L.; Font-Gonzalez, A.; Leroy, P.; Dick, B.D.; Taddio, A.; Ljungman, G.; Jibb, L.A.; Tutelman, P.R.; Liossi, C.; et al. Reducing pain and distress related to needle procedures in children with cancer: A clinical practice guideline. Eur. J. Cancer 2020, 131, 53–67. [Google Scholar] [CrossRef]
- Lüllmann, B.; Leonhardt, J.; Metzelder, M.; Hoy, L.; Gerr, H.; Linderkamp, C.; Klein, C.; Grigull, L. Pain reduction in children during port-à-cath catheter puncture using local anaesthesia with EMLA™. Eur. J. Pediatr. 2010, 169, 1465–1469. [Google Scholar] [CrossRef]
- Stoltz, P.; Manworren, R.C.B. Comparison of Children’s Venipuncture Fear and Pain: Randomized Controlled Trial of EMLA® and J-Tip Needleless Injection System®. J. Pediatr. Nurs. 2017, 37, 91–96. [Google Scholar] [CrossRef]
- McMurtry, C.M.; Pillai Riddell, R.; Taddio, A.; Racine, N.; Asmundson, G.J.; Noel, M.; Chambers, C.T.; Shah, V. Far From “Just a Poke”: Common Painful Needle Procedures and the Development of Needle Fear. Clin. J. Pain. 2015, 31, S3–S11. [Google Scholar] [CrossRef]
- Noel, M.; McMurtry, C.M.; Chambers, C.T.; McGrath, P.J. Children’s memory for painful procedures: The relationship of pain intensity, anxiety, and adult behaviors to subsequent recall. J. Pediatr. Psychol. 2010, 35, 626–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noel, M.; Chambers, C.T.; McGrath, P.J.; Klein, R.M.; Stewart, S.H. The influence of children’s pain memories on subsequent pain experience. Pain 2012, 153, 1563–1572. [Google Scholar] [CrossRef] [PubMed]
- Pate, J.T.; Blount, R.L.; Cohen, L.L.; Smith, A.J. Childhood Medical Experience and Temperament as Predictors of Adult Functioning in Medical Situations. Child. Health Care 1996, 25, 281–298. [Google Scholar] [CrossRef]
- Flor, H.; Turk, D.C. Psychophysiology of chronic pain: Do chronic pain patients exhibit symptom-specific psychophysiological responses? Psychol. Bull. 1989, 105, 215–259. [Google Scholar] [CrossRef]
- Chen, E.; Zeltzer, L.K.; Craske, M.G.; Katz, E.R. Children’s memories for painful cancer treatment procedures: Implications for distress. Child Dev. 2000, 71, 933–947. [Google Scholar] [CrossRef]
- Ornstein, P.A.; Manning, E.L.; Pelphrey, K.A. Children’s memory for pain. J. Dev. Behav. Pediatr. JDBP 1999, 20, 262–277. [Google Scholar] [CrossRef]
- Badali, M.A. Accuracy of Children’s and Parents’ Memory for a Novel Painful Experience. Pain Res. Manag. 2000, 5, 161–168. [Google Scholar] [CrossRef]
- Bruck, M.; Ceci, S.J.; Francoeur, E.; Barr, R. “I hardly cried when I got my shot!” Influencing children’s reports about a visit to their pediatrician. Child Dev. 1995, 66, 193–208. [Google Scholar] [CrossRef]
- Cohen, L.L.; Blount, R.L.; Cohen, R.J.; Ball, C.M.; McClellan, C.B.; Bernard, R.S. Children’s expectations and memories of acute distress: Short- and long-term efficacy of pain management interventions. J. Pediatr. Psychol. 2001, 26, 367–374. [Google Scholar] [CrossRef] [Green Version]
- Marche, T.A.; Briere, J.L.; von Baeyer, C.L. Children’s Forgetting of Pain-Related Memories. J. Pediatr. Psychol. 2016, 41, 220–231. [Google Scholar] [CrossRef]
- Noel, M.; Rabbitts, J.A.; Tai, G.G.; Palermo, T.M. Remembering pain after surgery: A longitudinal examination of the role of pain catastrophizing in children’s and parents’ recall. Pain 2015, 156, 800–808. [Google Scholar] [CrossRef] [PubMed]
- Pallegama, R.W.; Ariyasinghe, S.; Perera, E.D.; Treede, R.D. Influence of Catastrophizing and Personality Traits on Recalled Ratings of Acute Pain Experience in Healthy Young Adults. Pain Med. 2017, 18, 49–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noel, M.; Rabbitts, J.A.; Fales, J.; Chorney, J.; Palermo, T.M. The influence of pain memories on children’s and adolescents’ post-surgical pain experience: A longitudinal dyadic analysis. Health Psychol. 2017, 36, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Fischer, S.; Vinall, J.; Pavlova, M.; Graham, S.; Jordan, A.; Chorney, J.; Rasic, N.; Brookes, J.T.; Hoy, M.; Yunker, W.K.; et al. Role of anxiety in young children’s pain memory development after surgery. Pain 2019, 160, 965–972. [Google Scholar] [CrossRef]
- Noel, M.; Pavlova, M.; Lund, T.; Jordan, A.; Chorney, J.; Rasic, N.; Brookes, J.; Hoy, M.; Yunker, W.K.; Graham, S. The role of narrative in the development of children’s pain memories: Influences of father- and mother-child reminiscing on children’s recall of pain. Pain 2019, 160, 1866–1875. [Google Scholar] [CrossRef]
- Cohen, L.L.; Blount, R.L.; Chorney, J.; Zempsky, W.T.; Rodrigues, N.; Cousins, L. Management of pain and distress due to medical procedures. In Handbook of Pediatric Psychology, 5th ed.; Roberts, M.C., Steele, R., Eds.; Guilford Press: New York, NY, USA, 2017; pp. 146–160. [Google Scholar]
- Erdogan, B.; Aytekin Ozdemir, A. The Effect of Three Different Methods on Venipuncture Pain and Anxiety in Children: Distraction Cards, Virtual Reality, and Buzzy® (Randomized Controlled Trial). J. Pediatr. Nurs. 2021, 58, e54–e62. [Google Scholar] [CrossRef]
- Beran, T.N.; Ramirez-Serrano, A.; Vanderkooi, O.G.; Kuhn, S. Reducing children’s pain and distress towards flu vaccinations: A novel and effective application of humanoid robotics. Vaccine 2013, 31, 2772–2777. [Google Scholar] [CrossRef]
- Jibb, L.A.; Birnie, K.A.; Nathan, P.C.; Beran, T.N.; Hum, V.; Victor, J.C.; Stinson, J.N. Using the MEDiPORT humanoid robot to reduce procedural pain and distress in children with cancer: A pilot randomized controlled trial. Pediatr. Blood Cancer 2018, 65, e27242. [Google Scholar] [CrossRef]
- Ali, S.; Manaloor, R.; Ma, K.; Sivakumar, M.; Beran, T.; Scott, S.D.; Vandermeer, B.; Beirnes, N.; Graham, T.A.D.; Curtis, S.; et al. A randomized trial of robot-based distraction to reduce children’s distress and pain during intravenous insertion in the emergency department. Can. J. Emerg. Med. 2021, 23, 85–93. [Google Scholar] [CrossRef]
- Lee-Krueger, R.C.W.; Pearson, J.R.; Spencer, A.; Noel, M.; Bell-Graham, L.; Beran, T.N. Children’s Pain During IV Induction: A Randomized-Controlled Trial With the MEDi® Robot. J. Pediatr. Psychol. 2021, 46, 991–1000. [Google Scholar] [CrossRef]
- Butchart, J.A.-O.; Harrison, R.; Ritchie, J.; Martí, F.A.-O.; McCarthy, C.; Knight, S.; Scheinberg, A. Child and parent perceptions of acceptability and therapeutic value of a socially assistive robot used during pediatric rehabilitation. Disabil. Rehabil. 2021, 43, 163–170. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. Jama 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braithwaite, F.A.; Noel, M.; Jones, H.G.; Wiese, M.D.; Nania, C.G.; Watson, E.; Stanton, T.R. Reframe the pain: Divided attention and positive memory reframing to reduce needle pain and distress in children-A feasibility randomized controlled trial. Eur. J. Pain 2022, 26, 1702–1722. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crombez, G.; Bijttebier, P.; Eccleston, C.; Mascagni, T.; Mertens, G.; Goubert, L.; Verstraeten, K. The child version of the pain catastrophizing scale (PCS-C): A preliminary validation. Pain 2003, 104, 639–646. [Google Scholar] [CrossRef]
- Goubert, L.; Eccleston, C.; Vervoort, T.; Jordan, A.; Crombez, G. Parental catastrophizing about their child’s pain. The parent version of the Pain Catastrophizing Scale (PCS-P): A preliminary validation. Pain 2006, 123, 254–263. [Google Scholar] [CrossRef]
- Taddio, A.; McMurtry, C.M.; Shah, V.; Riddell, R.P.; Chambers, C.T.; Noel, M.; MacDonald, N.E.; Rogers, J.; Bucci, L.M.; Mousmanis, P.; et al. Reducing pain during vaccine injections: Clinical practice guideline. Cmaj 2015, 187, 975–982. [Google Scholar] [CrossRef] [Green Version]
- Birnie, K.A.; Noel, M.; Parker, J.A.; Chambers, C.T.; Uman, L.S.; Kisely, S.R.; McGrath, P.J. Systematic review and meta-analysis of distraction and hypnosis for needle-related pain and distress in children and adolescents. J. Pediatr. Psychol. 2014, 39, 783–808. [Google Scholar] [CrossRef] [Green Version]
- Hicks, C.L.; von Baeyer, C.L.; Spafford, P.A.; van Korlaar, I.; Goodenough, B. The Faces Pain Scale-Revised: Toward a common metric in pediatric pain measurement. Pain 2001, 93, 173–183. [Google Scholar] [CrossRef]
- Birnie, K.A.; Hundert, A.S.; Lalloo, C.; Nguyen, C.; Stinson, J.N. Recommendations for selection of self-report pain intensity measures in children and adolescents: A systematic review and quality assessment of measurement properties. Pain 2019, 160, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Pavlova, M.; Lund, T.; Nania, C.; Kennedy, M.; Graham, S.; Noel, M. Reframe the Pain: A Randomized Controlled Trial of a Parent-Led Memory-Reframing Intervention. J. Pain 2022, 23, 263–275. [Google Scholar] [CrossRef] [PubMed]
- McMurtry, C.M.; Noel, M.; Chambers, C.T.; McGrath, P.J. Children’s fear during procedural pain: Preliminary investigation of the Children’s Fear Scale. Health Psychol. 2011, 30, 780–788. [Google Scholar] [CrossRef] [PubMed]
- Stahlschmidt, L.; Hübner-Möhler, B.; Dogan, M.; Wager, J. Pain Self-Efficacy Measures for Children and Adolescents: A Systematic Review. J. Pediatr. Psychol. 2019, 44, 530–541. [Google Scholar] [CrossRef] [PubMed]
- Durand, H.; Birnie, K.A.; Noel, M.; Vervoort, T.; Goubert, L.; Boerner, K.E.; Chambers, C.T.; Caes, L. State Versus Trait: Validating State Assessment of Child and Parental Catastrophic Thinking About Children’s Acute Pain. J. Pain 2017, 18, 385–395. [Google Scholar] [CrossRef]
- Birnie, K.A.; Chambers, C.T.; Chorney, J.; Fernandez, C.V.; McGrath, P.J. Dyadic analysis of child and parent trait and state pain catastrophizing in the process of children’s pain communication. Pain 2016, 157, 938–948. [Google Scholar] [CrossRef]
- Vervoort, T.; Goubert, L.; Vandenbossche, H.; Van Aken, S.; Matthys, D.; Crombez, G. Child’s and parents’ catastrophizing about pain is associated with procedural fear in children: A study in children with diabetes and their mothers. Psychol. Rep. 2011, 109, 879–895. [Google Scholar] [CrossRef] [Green Version]
- Vervoort, T.; Goubert, L.; Crombez, G. The relationship between high catastrophizing children’s facial display of pain and parental judgment of their child’s pain. Pain 2009, 142, 142–148. [Google Scholar] [CrossRef]
- Rheel, E.; Ickmans, K.; Wauters, A.; Van Ryckeghem, D.M.L.; Malfliet, A.; Vervoort, T. The effect of a pain educational video intervention upon child pain-related outcomes: A randomized controlled study. Eur. J. Pain 2021, 25, 2094–2111. [Google Scholar] [CrossRef]
- Caes, L.; Vervoort, T.; Eccleston, C.; Vandenhende, M.; Goubert, L. Parental catastrophizing about child’s pain and its relationship with activity restriction: The mediating role of parental distress. Pain 2011, 152, 212–222. [Google Scholar] [CrossRef]
- Caes, L.; Vervoort, T.; Devos, P.; Verlooy, J.; Benoit, Y.; Goubert, L. Parental Distress and Catastrophic Thoughts About Child Pain Implications for Parental Protective Behavior in the Context of Child Leukemia-related Medical Procedures. Clin. J. Pain 2014, 30, 787–799. [Google Scholar] [CrossRef]
- Goubert, L.; Vervoort, T.; Cano, A.; Crombez, G. Catastrophizing about their children’s pain is related to higher parent-child congruency in pain ratings: An experimental investigation. Eur. J. Pain 2009, 13, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Caes, L.; Goubert, L.; Devos, P.; Verlooy, J.; Benoit, Y.; Vervoort, T. The relationship between parental catastrophizing about child pain and distress in response to medical procedures in the context of childhood cancer treatment: A longitudinal analysis. J. Pediatr. Psychol. 2014, 39, 677–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wauters, A.; Noel, M.; Van Ryckeghem, D.M.L.; Soltani, S.; Vervoort, T. The Moderating Role of Attention Control in the Relationship Between Pain Catastrophizing and Negatively-Biased Pain Memories in Youth With Chronic Pain. J. Pain. 2021, 22, 1303–1314. [Google Scholar] [CrossRef] [PubMed]
- Wauters, A.; Noel, M.; Van Ryckeghem, D.M.L.; Sanchez-Lopez, A.; Vervoort, T. Parental (non-)pain attending verbalizations moderate the relationship between child attention and memory bias for pain. Eur. J. Pain 2020, 24, 1797–1811. [Google Scholar] [CrossRef] [PubMed]
- Rheel, E.; Ickmans, K.; Wauters, A.; Van Ryckeghem, D.M.L.; Barbé, K.; Malfliet, A.; Vervoort, T. The Effect of a Pain Educational Video Upon Child Pain-Related Memory and the Moderating Role of Parental Pain- and Non-Pain-Attending Verbalizations: An Experimental Lab-Based Study. J. Pediatr. Psychol. 2022, 47, 1057–1070. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Grissom, R.J.; Kim, J.J. Effect Sizes for Research: A Broad Practical Approach; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2005; p. xv, 253. [Google Scholar]
- Jaaniste, T.; Noel, M.; Yee, R.D.; Bang, J.; Tan, A.C.; Champion, G.D. Why Unidimensional Pain Measurement Prevails in the Pediatric Acute Pain Context and What Multidimensional Self-Report Methods Can Offer. Children 2019, 6, 132. [Google Scholar] [CrossRef] [Green Version]
- Noel, M.; Pavlova, M.; McCallum, L.; Vinall, J. Remembering the hurt of childhood: A psychological review and call for future research. Can. Psychol. Psychol. Can. 2017, 58, 58–68. [Google Scholar] [CrossRef]
- Wauters, A.; Vervoort, T.; Noel, M.; Rheel, E.; Van Ryckeghem, D.M.L. The relation between children’s attention bias to pain and children’s pain-related memory biases is moderated by parental narrative style. Behav. Res. 2022, 159, 104202. [Google Scholar] [CrossRef]
- Pope, N.; Tallon, M.; McConigley, R.; Wilson, S. The experiences of acute non-surgical pain of children who present to a healthcare facility for treatment: A systematic review protocol. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Beraldo, G.; Menegatti, E.; Tommasi, V.D.; Mancin, R.; Benini, F. A preliminary investigation of using humanoid social robots as non-pharmacological techniques with children. In Proceedings of the 2019 IEEE International Conference on Advanced Robotics and its Social Impacts (ARSO), Beijing, China, 31 October–2 November 2019; pp. 393–400. [Google Scholar]
- DeMore, M.; Cohen, L.L. Distraction for Pediatric Immunization Pain: A Critical Review. J. Clin. Psychol. Med. Settings 2005, 12, 281–291. [Google Scholar] [CrossRef]
- McCaul, K.D.; Malott, J.M. Distraction and coping with pain. Psychol. Bull. 1984, 95, 516–533. [Google Scholar] [CrossRef]
- Roser, T.; Samson, A.; Humphreys, P.; Cruz-Valdivieso, E. Co-creation: New Pathways to Value: An Overview. Promise LSE Enterp. 2009. [Google Scholar]
- Huijnen, C.A.G.J.; Lexis, M.A.S.; Jansens, R.; de Witte, L.P. How to Implement Robots in Interventions for Children with Autism? A Co-creation Study Involving People with Autism, Parents and Professionals. J. Autism Dev. Disord. 2017, 47, 3079–3096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanders, E.B.N.; Stappers, P.J. Co-creation and the new landscapes of design. CoDesign 2008, 4, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Koller, D.; Goldman, R.D. Distraction techniques for children undergoing procedures: A critical review of pediatric research. J. Pediatr. Nurs. 2012, 27, 652–681. [Google Scholar] [CrossRef]
- Kolahi, J.; Bang, H.; Park, J. Towards a proposal for assessment of blinding success in clinical trials: Up-to-date review. Community Dent. Oral Epidemiol. 2009, 37, 477–484. [Google Scholar] [CrossRef]


{kind=link}
| Control Intervention (i.e., Usual Care) | Experimental Intervention (i.e., Robot-Led Distraction) |
|---|---|
| 1. Standardized positioning of child, parent, nurse(s), and investigator in the procedure room 2. Exclusively non-intensive distraction (e.g., counting, blowing, singing, …) 3. Normal interaction between nurse, child, and parent 4. Nurse ending with “You did very well!” | 1. Standardized positioning of child, parent, nurse(s), investigator, and robot in the procedure room 2. Correct timing of initiating robot intervention (i.e., nurse closed door after entering procedure room) 3. Robot-led distraction throughout full duration of needle procedure (before, during, and after needle insertion) 4. Minimal interaction between nurse, child, and parent 5. Robot ending with “You did very well!” |
| Characteristic | EG (n = 11) | CG (n = 11) | Total (N = 22) | |
|---|---|---|---|---|
| Child age; M (SD) | 9.36 (1.36) | 9.45 (1.37) | 9.41 (1.33) | |
| Child sex; n (%) | Boys Girls | 6 (54.55) 5 (45.45) | 4 (36.36) 7 (63.64) | 10 (45.45) 12 (54.54) |
| Diagnosis; n (%) | Chronic immune deficiency Auto-immune/-inflammatory disease Metabolic disease Inflammatory bowel disease Combination | 6 (54.55) 3 (27.27) 0 (0.00) 1 (9.09) 0 (0.00) | 6 (54.55) 2 (18.18) 3 (27.27) 0 (0.00) 1 (9.09) | 12 (54.55) 5 (22.73) 3 (13.64) 1 (13.64) 1 (13.64) |
| Time since diagnosis (months); M (SD) | 58.45 (30.86) | 54.55 (29.35) | 56.50 (29.46) | |
| Pain in the last 2 weeks child; n (%) | Yes No | 7 (63.64) 4 (36.36) | 7 (63.64) 4 (36.36) | 14 (63.64) 8 (36.36) |
| Pain intensity last 2 weeks child; n (%) | No pain Little pain Moderate pain Much pain Very much pain | 4 (36.36) 0 (0.00) 6 (54.55) 1 (9.09) 0 (0.00) | 4 (36.36) 1 (9.09) 6 (54.55) 0 (0.00) 0 (0.00) | 8 (36.36) 1 (4.55) 12 (54.54) 1 (4.55) 0 (0.00) |
| Pain frequency last 2 weeks child; n (%) | Never Once Few times Often Continuously | 4 (36.36) 1 (9.09) 4 (36.36) 2 (18.18) 0 (0.00) | 4 (36.36) 0 (0.00) 7 (63.64) 0 (0.00) 0 (0.00) | 8 (36.36) 1 (4.55) 11 (50.00) 2 (9.09) 0 (0.00) |
| Chronic pain child (> 3 months); n (%) | Yes No | 2 (18.18) 9 (81.82) | 4 (36.36) 7 (63.64) | 6 (27.27) 16 (72.73) |
| Characteristic | EG (n = 11) | CG (n = 11) | Total (N = 22) | |
|---|---|---|---|---|
| Parent age; M (SD) | 39.82 (4.26) | 40.27 (5.27) | 40.05 (4.69) | |
| Parent sex; n (%) | Fathers Mothers | 2 (18.18) 9 (81.82) | 1 (9.09) 10 (90.91) | 3 (13.64) 19 (86.36) |
| Health status parent; n (%) | Excellent Very good Good Moderate Poor | 1 (9.09) 5 (45.45) 5 (45.45) 0 (0.00) 0 (0.00) | 1 (9.09) 4 (36.36) 5 (45.45) 1 (9.09) 0 (0.00) | 2 (9.09) 9 (40.91) 10 (45.45) 1 (4.55) 0 (0.00) |
| Family status; n (%) | Married or cohabiting Divorced Widow(er) Single parent or unmarried Newly assembled family | 7 (63.64) 3 (27.27) 0 (0.00) 1 (9.09) 0 (0.00) | 11 (100.00) 0 (0.00) 0 (0.00) 0 (0.00) 0 (0.00) | 18 (81.82) 3 (13.64) 0 (0.00) 1 (4.55) 0 (0.00) |
| Education level parent; n (%) | Primary education (≤ 12yo) Lower secondary education (≤ 14yo) Higher secondary education (≤ 18yo) Higher education (bachelor/master) | 2 (18.18) 0 (0.00) 4 (36.36) 5 (45.45) | 1 (9.09) 0 (0.00) 4 (36.36) 6 (54.55) | 3 (13.64) 0 (0.00) 8 (36.36) 11 (50.00) |
| Occupation parent; n (%) | Housewife/househusband Laborer Employee Liberal profession Self-employed Manager position Unemployed | 0 (0.00) 1 (9.09) 6 (54.55) 0 (0.00) 2 (18.18) 1 (9.09%) 1 (9.09%) | 0 (0.00) 1 (9.09) 4 (36.36) 0 (0.00) 3 (27.27) 3 (27.27%) 0 (0.00%) | 0 (0.00) 2 (9.09) 10 (45.45) 0 (0.00) 5 (22.73) 4 (18.18) 1 (4.55) |
| Outcome | Total Sample (N = 21) M (SD) | EG (n = 10) M (SD) | CG (n = 11) M (SD) | p-Value | 95% CI (Lower Upper) | Hedges’ g |
|---|---|---|---|---|---|---|
| Experienced pain intensity (t2) | 2.10 (2.64) | 3.00 (3.43) | 1.27 (1.35) | 0.163 | (−4.27, 0.81) | −0.50 |
| Experienced pain-related fear (t2) | 0.71 (1.01) | 1.10 (1.29) | 0.36 (0.51) | 0.117 | (−1.69, 0.215) | −0.74 |
| Experienced self-efficacy (t2) | 7.57 (2.94) | 8.30 (1.77) | 6.91 (3.67) | 0.280 | (−4.04, 1.26) | −0.46 |
| Experienced pain catastrophizing (t2) | 2.16 (2.47) | 2.80 (3.27) | 1.58 (1.36) | 0.293 | (−3.65, 1.20) | −0.48 |
| Recalled pain intensity (t3) | 2.67 (2.13) | 3.00 (2.71) | 2.36 (1.50) | 0.522 | (−2.72, 1.45) | −0.28 |
| Recalled pain-related fear (t3) | 1.05 (1.12) | 1.40 (1.35) | 0.73 (0.79) | 0.174 | (−1.67, 0.32) | −0.59 |
| Future pain intensity (t3) | 2.95 (2.42) | 3.20 (2.70) | 2.73 (2.24) | 0.666 | (−2.73, 1.79) | −0.18 |
| Future pain-related fear (t3) | 1.05 (1.16) | 1.30 (1.50) | 0.82 (0.75) | 0.375 | (−1.61, 0.65) | −0.40 |
| Future self-efficacy (t3) | 8.24 (1.84) | 7.80 (2.20) | 8.64 (1.43) | 0.311 | (−0.84, 2.52) | 0.44 |
| MB pain intensity (t3 − t2) | 0.57 (1.57) | 0.00 (1.33) | 1.09 (1.64) | 0.113 | (−0.28, 2.47) | 0.70 |
| MB pain-related fear (t3 − t2) | 0.33 (.66) | 0.30 (.82) | 0.36 (.50) | 0.831 | (−0.55, 0.71) | 0.09 |
| Outcome | Total Sample (N = 21) n (%) | EG (n = 10) n (%) | CG (n = 11) n (%) | |
|---|---|---|---|---|
| MB pain intensity | Negative (+ value) | 8 (38.10) | 2 (20.00) | 6 (54.55) |
| Accurate (zero) | 10 (47.62) | 6 (60.00) | 4 (36.36) | |
| Positive (− value) | 3 (14.29) | 2 (20.00) | 1 (9.09) | |
| MB pain-related fear | Negative (+ value) | 7 (33.33) | 3 (30.00) | 4 (36.36) |
| Accurate (zero) | 13 (61.90) | 6 (60.00) | 7 (63.64) | |
| Positive (− value) | 1 (4.76) | 1 (10.00) | 0 (0.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rheel, E.; Vervoort, T.; Malfliet, A.; van der Werff ten Bosch, J.; Debulpaep, S.; Robberechts, W.; Maes, E.; Mostaqim, K.; Noel, M.; Ickmans, K. The Effect of Robot-Led Distraction during Needle Procedures on Pain-Related Memory Bias in Children with Chronic Diseases: A Pilot and Feasibility Study. Children 2022, 9, 1762. https://doi.org/10.3390/children9111762
Rheel E, Vervoort T, Malfliet A, van der Werff ten Bosch J, Debulpaep S, Robberechts W, Maes E, Mostaqim K, Noel M, Ickmans K. The Effect of Robot-Led Distraction during Needle Procedures on Pain-Related Memory Bias in Children with Chronic Diseases: A Pilot and Feasibility Study. Children. 2022; 9(11):1762. https://doi.org/10.3390/children9111762
Chicago/Turabian StyleRheel, Emma, Tine Vervoort, Anneleen Malfliet, Jutte van der Werff ten Bosch, Sara Debulpaep, Wiert Robberechts, Evelyn Maes, Kenza Mostaqim, Melanie Noel, and Kelly Ickmans. 2022. "The Effect of Robot-Led Distraction during Needle Procedures on Pain-Related Memory Bias in Children with Chronic Diseases: A Pilot and Feasibility Study" Children 9, no. 11: 1762. https://doi.org/10.3390/children9111762