Clinical, Cognitive and Neurodevelopmental Profile in Tetrasomies and Pentasomies: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Review Protocol
2.2. Literature Search
2.3. Inclusion and Exclusion Criteria
2.4. Quality Assessment
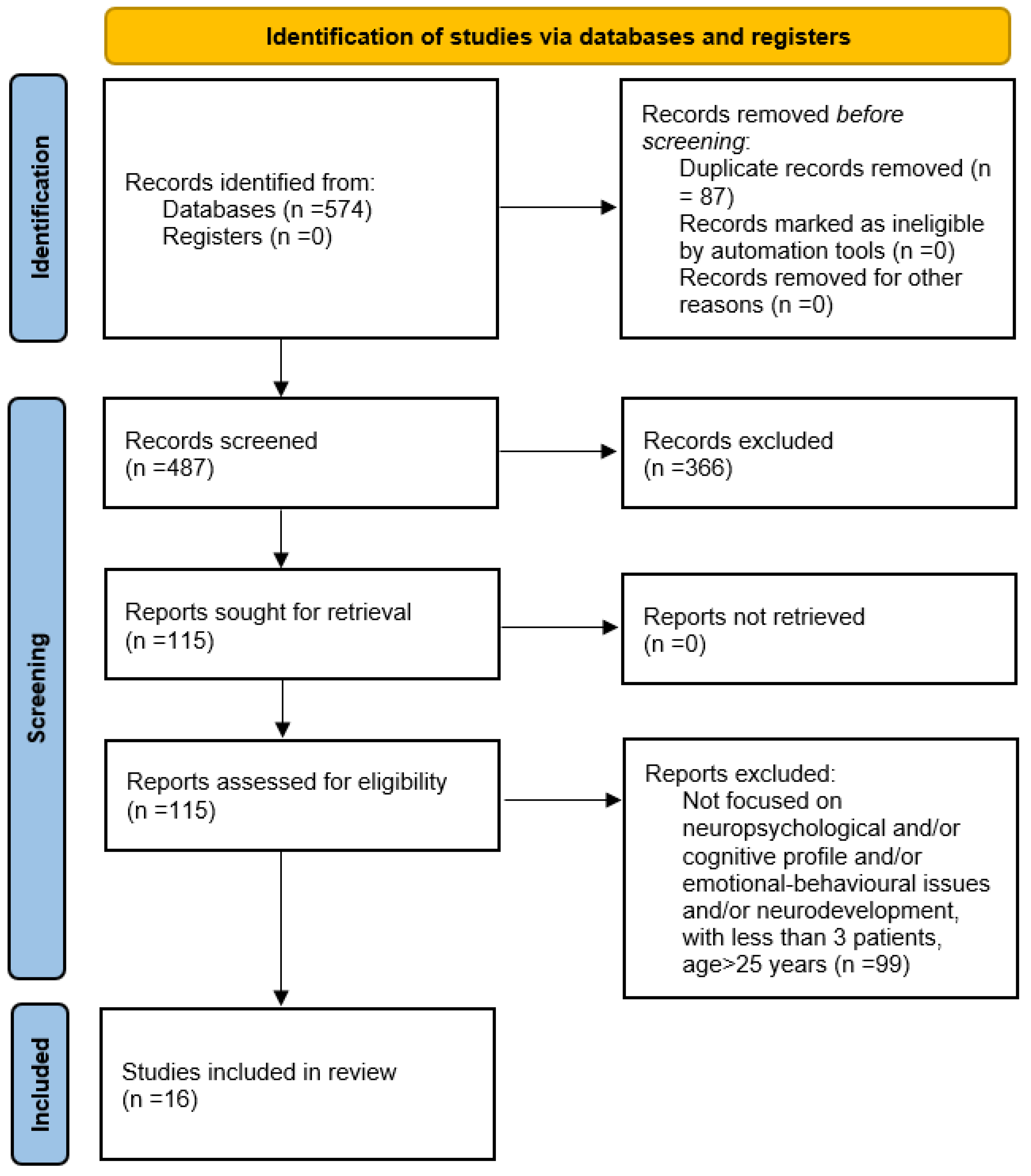
3. Results
Search Results
4. Discussion
4.1. 48, XXYY SYNDROME
4.1.1. Neurological Features
4.1.2. Medical Aspects
4.1.3. Psychosocial and Behavioural Aspects
4.1.4. Neurodevelopmental Aspects
4.1.5. Cognitive Phenotype
4.1.6. Structural Neuroimaging Studies
4.2. 49, XXXXY SYNDROME
4.2.1. Clinical Features and Neurological Examination
4.2.2. Cognitive Profile
4.2.3. Behavioural Profile
4.2.4. Neurodevelopmental Profile
4.2.5. Neuroimaging Features
4.2.6. Therapeutic Approaches
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thompson, T.; Howell, S.; Davis, S.; Wilson, R.; Janusz, J.; Boada, R.; Pyle, L.; Tartaglia, N. Current survey of early childhood intervention services in infants and young children with sex chromosome aneuploidies. Am. J. Med. Genet. Part C Semin. Med. Genet. 2020, 184, 414–427. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.R.; Wallace, G.L.; Adeyemi, E.I.; Lopez, K.C.; Blumenthal, J.D.; Clasen, L.S.; Giedd, J.N. Dosage effects of X and Y chromosomes on language and social functioning in children with supernumerary sex chromosome aneuploidies: Implications for idiopathic language impairment and autism spectrum disorders. J. Child Psychol. Psychiatry 2012, 53, 1072–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dulac, O.; Lassonde, M.; Sarnat, H.B. Cognitive and Medical Features of Chromosomal Aneuploidy—Handbook of Clinical Neurology, 3rd ed.; Pediatric Neurology Part I; Elsevier B.V.: Amsterdam, The Netherlands, 2013; Volume 111. [Google Scholar]
- Skuse, D.; Printzlau, F.; Wolstencroft, J. Sex chromosome aneuploidies. Handb. Clin. Neurol. 2018, 147, 355–376. [Google Scholar] [CrossRef] [PubMed]
- Singh, J. The portal for rare diseases and orphan drugs. J. Pharmacol. Pharmacother. 2013, 4, 168–169. [Google Scholar] [CrossRef] [PubMed]
- Gropman, A.; Samango-Sprouse, C.A. Neurocognitive variance and neurological underpinnings of the X and Y chromosomal variations. Am. J. Med. Genet. Part C Semin. Med. Genet. 2013, 163, 35–43. [Google Scholar] [CrossRef]
- Spaziani, M.; Mileno, B.; Rossi, F.; Granato, S.; Tahani, N.; Anzuini, A.; Lenzi, A.; Radicioni, A.F. Endocrine and metabolic evaluation of classic Klinefelter syndrome and high-grade aneuploidies of sexual chromosomes with male phenotype: Are they different clinical conditions? Eur. J. Endocrinol. 2018, 178, 343–352. [Google Scholar] [CrossRef] [Green Version]
- Tartaglia, N.R.; Ayari, N.; Hutaff-Lee, C.; Boada, R. Attention-deficit hyperactivity disorder symptoms in children and adolescents with sex chromosome aneuploidy: XXY, XXX, XYY, and XXYY. J. Dev. Behav. Pediatr. 2012, 33, 309–318. [Google Scholar] [CrossRef] [Green Version]
- Udhnani, M.; Maiman, M.; Blumenthal, J.D.; Clasen, L.S.; Wallace, G.L.; Giedd, J.N.; Raznahan, A.; Lee, N.R. Phonemic and Semantic Verbal Fluency in Sex Chromosome Aneuploidy: Contrasting the Effects of Supernumerary X versus Y Chromosomes on Performance. J. Int. Neuropsychol. Soc. 2018, 24, 917–992. [Google Scholar] [CrossRef] [Green Version]
- Gropman, A.L.; Rogol, A.; Fennoy, I.; Sadeghin, T.; Sinn, S.; Jameson, R.; Mitchell, F.; Clabaugh, J.; Lutz-Armstrong, M.; Samango-Sprouse, C.A. Clinical variability and novel neurodevelopmental findings in 49, XXXXY syndrome. Am. J. Med. Genet. Part A 2010, 152A, 1523–1530. [Google Scholar] [CrossRef]
- Samango-Sprouse, C.A.; Gropman, A.L.; Sadeghin, T.; Kingery, M.; Lutz-Armstrong, M.; Rogol, A. Effects of short-course androgen therapy on the neurodevelopmental profile of infants and children with 49,XXXXY syndrome. Acta Paediatr. 2011, 100, 861–865. [Google Scholar] [CrossRef]
- Cordeiro, L.; Tartaglia, N.; Roeltgen, D.; Ross, J. Social deficits in male children and adolescents with sex chromosome aneuploidy: A comparison of XXY, XYY, and XXYY syndromes. Res. Dev. Disabil. 2012, 33, 1254–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumenthal, J.D.; Baker, E.H.; Lee, N.R.; Wade, B.; Clasen, L.S.; Lenroot, R.K.; Giedd, J.N. Brain morphological abnormalities in 49,XXXXY syndrome: A pediatric magnetic resonance imaging study. NeuroImage Clin. 2013, 2, 197–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tartaglia, N.R.; Wilson, R.; Miller, J.S.; Rafalko, J.; Cordeiro, L.; Davis, S.; Hessl, D.; Ross, J. Autism spectrum disorder in males with sex chromosome aneuploidy: XXY/Klinefelter syndrome, XYY, and XXYY. J. Dev. Behav. Pediatr. 2017, 38, 197–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgemeister, A.L.; Daumiller, E.; du Bois, G.; Graul-Neumann, L.M.; Köhler, B.; Knecht, S.; Burgemeister, S.; Gronwald, S.; Maurer, M.H.; Zirn, B. Clinical report of 8 patients with 49,XXXXY syndrome: Delineation of the facial gestalt and depiction of the clinical spectrum. Eur. J. Med. Genet. 2018, 62, 210–216. [Google Scholar] [CrossRef]
- Srinivasan, R.; Wolstencroft, J.; Erwood, M.; Raymond, F.L.; Bree, M.; Hall, J.; Skuse, D. Mental health and behavioural problems in children with XXYY: A comparison with intellectual disabilities. J. Intellect. Disabil. Res. 2019, 63, 477–488. [Google Scholar] [CrossRef]
- Gropman, A.L.; Porter, G.F.; Lasutschinkow, P.C.; Sadeghin, T.; Tipton, E.S.; Powell, S.; Samango-Sprouse, C.A. Neurocognitive development and capabilities in boys with 49,XXXXY syndrome. Am. J. Med. Genet. Part A 2020, 185, 3541–3546. [Google Scholar] [CrossRef]
- Samango-Sprouse, C.; Lasutschinkow, P.C.; Mitchell, F.; Porter, G.F.; Hendrie, P.; Powell, S.; Sadeghin, T.; Gropman, A.A. 49, XXXXY syndrome: A study of neurological function in this uncommon X and Y chromosomal disorder. Am. J. Med. Genet. Part A 2020, 185, 3557–3566. [Google Scholar] [CrossRef]
- Lasutschinkow, P.C.; Gropman, A.L.; Porter, G.F.; Sadeghin, T.; Samango-Sprouse, C.A. Behavioural phenotype of 49, XXXXY syndrome: Presence of anxiety-related symptoms and intact social awareness. Am. J. Med. Genet. Part A 2020, 182, 974–986. [Google Scholar] [CrossRef]
- Samango-Sprouse, C.A.; Lasutschinkow, P.C.; McLeod, M.; Porter, G.F.; Powell, S.; Laurent, J.S.; Sadeghin, T.; Gropman, A. Speech and language development in children with 49, XXXXY syndrome. Am. J. Med. Genet. Part A 2021, 185, 3567–3575. [Google Scholar] [CrossRef]
- Lee, R.S.; Song, S.Q.; Garrison-Desany, H.M.; Carey, J.L.; Lasutschinkow, P.; Zabel, A.; Bressler, J.; Gropman, A.; Samango-Sprouse, C. DNA methylation and behavioural dysfunction in males with 47, XXY and 49, XXXXY: A pilot study. Clin. Epigenet. 2021, 13, 136. [Google Scholar] [CrossRef]
- Borgaonkar, D.S.; Mules, E.; Char, F. Do the 48, XXYY males have a characteristic phenotype? A review. Clin. Genet. 1970, 1, 272–293. [Google Scholar] [CrossRef]
- Linden, M.G.; Bender, B.G.; Robinson, A. Sex chromosome tetrasomy and pentasomy. Pediatrics 1995, 96, 672–682. [Google Scholar] [CrossRef] [PubMed]
- Tartaglia, N.; Ayari, N.; Howell, S.; D’Epagnier, C.; Zeitler, P. 48, XXYY, 48, XXXY and 49, XXXXY syndromes: Not just variants of Klinefelter syndrome. Acta Pædiatr. 2011, 100, 851–860. [Google Scholar] [CrossRef]
- Visootsak, J.; Rosner, B.; Dykens, E.; Tartaglia, N.; Graham, J.M., Jr. Behavioural phenotype of sex chromosome aneuploidies: 48, XXYY, 48, XXXY and 49, XXXXY. Am. J. Med. Genet. 2007, 143A, 1198–1203. [Google Scholar] [CrossRef] [PubMed]
- Tartaglia, N.; Davis, S.; Hench, A.; Nimishakavi, S.; Beauregard, R.; Reynolds, A.; Fenton, L.; Albrecht, L.; Ross, J.; Visootsak, J.; et al. A new look at XXYY syndrome: Medical and psychological features. Am. J. Med. Genet. Part A 2008, 146A, 1509–1522. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, K.; Nielsen, J.; Jacobsen, P.; Rølle, T. The 48, XXYY syndrome. J. Ment. Defic. Res. 1978, 22, 197–205. [Google Scholar] [PubMed]
- Kleczkowska, A.; Fryns, J.P.; Van den Berghe, H. X-chromosome polysomy in the male. The Leuven experience 1966–1987. Hum. Genet. 1988, 80, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Blumling, A.A.; Martyn, K.; Talboy, A.; Close, S. Rare sex chromosome variation 48, XXYY: An integrative review. Am. J. Med. Genet. Part C Semin. Med. Genet. 2020, 184, 386–403. [Google Scholar] [CrossRef]
- Frühmesser, A.; Kotzot, D. Chromosomal variants in klinefelter syndrome. Sex. Dev. 2011, 5, 109–123. [Google Scholar] [CrossRef]
- Swerdlow, A.J.; Schoemaker, M.J.; Higgins, C.D.; Wright, A.F.; Jacobs, P.A. Cancer incidence and mortality in men with Klinefelter syndrome: A cohort study. J. Natl. Cancer Inst. 2005, 97, 1204–1210. [Google Scholar] [CrossRef]
- Muldal, S.; Ockey, C.H. The “double male”: A new chromosome constitution in Klinefelter’s syndrome. Lancet 1960, 276, 492–493. [Google Scholar] [CrossRef]
- Lee, J.W. An XXYY male with schizophrenia. Aust. N. Z. J. Psychiatry 1996, 30, 553–556. [Google Scholar] [CrossRef] [PubMed]
- Borghgraef, M.; Fryns, J.P.; Van Den Berghe, H. The 48, XXYY syndrome. Follow-up data on clinical characteristics and psychological findings in 4 patients. Genet. Couns. 1991, 2, 103–108. [Google Scholar]
- Fryns, J.P.; Kleczkowska, A.; Kubień, E.; Berghe, H.V.D. XYY syndrome and other Y chromosome polysomies. Mental status and psychosocial functioning. Genet. Couns. 1995, 6, 197–206. [Google Scholar]
- Visootsak, J.; Graham, J.M. Social function in multiple X and Y chromosome disorders: XXY, XYY, XXYY, XXXY. Dev. Disabil. Res. Rev. 2009, 15, 328–332. [Google Scholar] [CrossRef] [Green Version]
- Visootsak, J.; Graham, J.M. Klinefelter syndrome and other sex chromosomal aneuploidies. Orphanet J. Rare Dis. 2006, 1, 42. [Google Scholar] [CrossRef] [Green Version]
- Van Rijn, S.; Swaab, H.; Aleman, A.; Kahn, R.S. Social Behaviour and Autism Traits in a Sex Chromosomal Disorder: Klinefelter (47XXY) Syndrome. J. Autism. Dev. Disord. 2008, 38, 1634–1641. [Google Scholar] [CrossRef]
- Geschwind, D.; Dykens, E. Neurobehavioural and psychosocial issues in klinefelter syndrome. Learn. Disabil. Res. Pract. 2004, 19, 166–173. [Google Scholar] [CrossRef]
- Tofani, M.; Scarcella, L.; Galeoto, G.; Giovannone, F.; Sogos, C. Behavioural gender differences across Pre-School Children with Autism Spectrum Disorders: A cross-sectional study. J. Autism. Dev. Disord. 2022. [Google Scholar] [CrossRef]
- Lenroot, R.K.; Lee, N.R.; Giedd, J.N. Effects of sex chromosome aneuploidies on brain development: Evidence from neuroimaging studies. Dev. Disabil. Res. Rev. 2009, 15, 318–327. [Google Scholar] [CrossRef] [Green Version]
- Polani, P.E. Abnormal sex chromosomes, behaviour and mental disorder. In Developments in Psychiatric Research; Tanner, J., Ed.; Hodder and Stoughton: London, UK, 1977; pp. 89–128. [Google Scholar]
- Netley, C.T. Summary overview of behavioural devel opment in individuals with neonatally identified X and Y aneuploidy. Birth Defects Orig. Artic. Ser. 1986, 22, 293–306. [Google Scholar] [PubMed]
- Printzlau, F.; Wolstencroft, J.; Skuse, D.H. Cognitive, behavioural, and neural consequences of sex chromosome aneuploidy. J. Neurosci. Res. 2017, 95, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Hanley, A.P.; Blumenthal, J.D.; Lee, N.R.; Baker, E.H.; Clasen, L.S.; Giedd, J.N. Brain and behaviour in 48, XXYY syndrome. NeuroImage Clin. 2015, 8, 133–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wade, B.S.C.; Joshi, S.H.; Reuter, M.; Blumenthal, J.D.; Toga, A.W.; Thompson, P.M.; Giedd, J.N. Effects of sex chromosome dosage on corpus callosum morphology in supernumerary sex chromo- some aneuploidies. Biol. Sex Differ. 2014, 5, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reardon, P.K.; Clasen, L.; Giedd, J.N.; Blumenthal, J.; Lerch, J.P.; Chakravarty, M.M.; Raznahan, A. An allometric analysis of sex and sex chromosome dosage effects on subcortical anatomy in humans. J. Neurosci. 2016, 36, 2438–2448. [Google Scholar] [CrossRef] [Green Version]
- Fish, A.M.; Cachia, A.; Fischer, C.; Mankiw, C.; Reardon, P.; Clasen, L.S.; Blumenthal, J.D.; Greenstein, D.; Giedd, J.N.; Mangin, J.-F.; et al. Influences of brain size, sex, and sex chromsome complement on the architecture of human cortical folding. Cereb. Cortex 2016, 27, 5557–5567. [Google Scholar] [CrossRef] [Green Version]
- Lin, A.; Clasen, L.; Lee, N.R.; Wallace, G.L.; LaLonde, F.; Blumenthal, J.; Giedd, J.N.; Raznahan, A. Mapping the stability of human brain asymmetry across five sex-chromosome aneuploidies. J. Neurosci. 2015, 35, 140–145. [Google Scholar] [CrossRef] [Green Version]
- Peet, J.; Weaver, D.D.; Vance, G.H. 49, XXXXY: A distinct phenotype. Three new cases and review. J. Med. Genet. 1998, 35, 420–424. [Google Scholar] [CrossRef]
- Samango-Sprouse, C.A. The Mental development in polysomy X Klinefelter syndrome (47, XXY; 48, XXXY): Effects of incomplete X inactivation. Semin. Reprod. Med. 2001, 19, 193–202. [Google Scholar] [CrossRef]
- Samango-Sprouse, C.A. Frontal lobe development in childhood. In The Human Frontal Lobe: Functions and Disorders, 2nd ed.; Miller, B.L., Cummings, J.L., Eds.; Guilford Press: New York, NY, USA, 2007. [Google Scholar]
- Spaziani, M.; Tarantino, C.; Pozza, C.; Anzuini, A.; Panimolle, F.; Papi, G.; Gianfrilli, D.; Lenzi, A.; Radicioni, A.F. Adverse pathophysiological influence of early testosterone therapy on the testes of boys with higher grade sex chromosome aneuploidies (HGAs): A retrospective, cross-sectional study. J. Endocrinol. Investig. 2020, 44, 1483–1490. [Google Scholar] [CrossRef]
- Greco, C.; Romani, M.; Berardi, A.; De Vita, G.; Galeoto, G.; Giovannone, F.; Vigliante, M.; Sogos, C. Morphing Task: The Emotion Recognition Process in Children with Attention Deficit Hyperactivity Disorder and Autism Spectrum Disorder. Int. J. Environ. Res. Public Health 2021, 18, 13273. [Google Scholar] [CrossRef] [PubMed]
- Pittella, E.; Piuzzi, E.; Rizzuto, E.; del Prete, Z.; Fioriello, F.; Maugeri, A.; Sogos, C. Wereable Heart rate monitoring as stress report indicator in children with neurodevelopmental disorders. In Proceedings of the 2018 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Rome, IItaly, 11–13 June 2018; pp. 1–5. [Google Scholar] [CrossRef]


{kind=link}
| Article | 1. Was the Study Question or Objective Clearly Stated? | 2. Was the Study Population Clearly and Fully Described, Including a Case Definition? | 3. Were the Cases Consecutive? | 4. Were the Subjects Comparable? | 5. Was the Intervention Clearly Described? | |
| Gropman et al., 2010 [10] | YES | YES | YES | YES | YES | |
| Samango-Sprouse et al., 2011 [11] | YES | YES | YES | YES | YES | |
| Lee et al., 2012 [2] | YES | YES | YES | YES | YES | |
| Cordeiro et al., 2012 [12] | YES | YES | YES | YES | YES | |
| Tartaglia et al., 2012 [8] | YES | YES | YES | YES | YES | |
| Blumenthal et al., 2013 [13] | YES | YES | YES | YES | YES | |
| Tartaglia et al., 2017 [14] | YES | YES | YES | YES | YES | |
| Udhnani et al., 2018 [9] | YES | YES | YES | YES | YES | |
| Burgemeister et al., 2018 [15] | YES | YES | YES | YES | YES | |
| Srinivasan et al., 2019 [16] | YES | YES | YES | YES | YES | |
| Gropman et al., 2020 [17] | YES | YES | YES | YES | YES | |
| Samango-Sprouse et al., 2020 [18] | YES | YES | YES | YES | YES | |
| Lasutschinkow et al., 2020 [19] | YES | YES | YES | YES | YES | |
| Thompson et al., 2020 | YES | YES | YES | YES | YES | |
| Samango-Sprouse et al., 2021 [20] | YES | YES | YES | YES | YES | |
| Lee et al., 2021 [21] | YES | NO | YES | YES | YES | |
| Article | 6. Were the Outcome Measures Clearly Defined, Valid, Reliable, and Implemented Consistently across All Study Participants? | 7. Was the Length of Follow-Up Adequate? | 8. Were the Statistical Methods Well-Described? | 9. Were the Results Well-Described? | Reviewer 1 | Reviewer 2 |
| Gropman et al., 2010 [10] | YES | YES | YES | YES | GOOD | GOOD |
| Samango-Sprouse et al., 2011 [11] | YES | YES | YES | YES | GOOD | GOOD |
| Lee et al., 2012 [2] | YES | NO | YES | YES | FAIR | FAIR |
| Cordeiro et al., 2012 [12] | YES | NO | YES | YES | FAIR | FAIR |
| Tartaglia et al., 2012 [8] | YES | YES | YES | YES | GOOD | GOOD |
| Blumenthal et al., 2013 [13] | YES | NO | YES | YES | FAIR | FAIR |
| Tartaglia et al., 2017 [14] | YES | NO | YES | YES | FAIR | FAIR |
| Udhnani et al., 2018 [9] | YES | NO | YES | YES | FAIR | FAIR |
| Burgemeister et al., 2018 [15] | YES | YES | YES | YES | GOOD | GOOD |
| Srinivasan et al., 2019 [16] | YES | YES | YES | YES | GOOD | GOOD |
| Gropman et al., 2020 [17] | YES | NO | YES | YES | ||
| Samango-Sprouse et al., 2020 [18] | YES | YES | YES | YES | GOOD | GOOD |
| Lasutschinkow et al., 2020 [19] | YES | YES | YES | YES | GOOD | GOOD |
| Thompson et al., 2020 [1] | YES | NO | YES | YES | ||
| Samango-Sprouse et al., 2021 [20] | YES | YES | YES | YES | GOOD | GOOD |
| Lee et al., 2021 [21] | YES | NO | YES | YES | FAIR | FAIR |
| Study | Recruitment | N | Age | Methods | Results |
|---|---|---|---|---|---|
| Gropman et al., 2010 [10] | Patients evaluated during consecutive summers (July 2004, 2005, 2006 and 2007) at the Neurodevelopmental Diagnostic Center for Young Children (NDCYC) in Davidsonville, Maryland. | 20 boys with 49, XXXXY | Age 11 months–7 years | Leiter International Performance Scale-Revised (LIPS-R), Bayley Scales of Infant and Toddler Development, 3rd/Edition, Preschool Language Scale-3 or 4 (PLS-3/4), Peabody Motor Scale (GM, VM, total), Beery–Buktenica Developmental Test of Visual-Motor Integration, Fifth Edition (VMI), Gilliam Autism Rating Scale (GARS-2), Receptive One Word Picture Vocabulary Test-, Revised (ROWPVT-R), Expressive One Word Picture Vocabulary Test, Revised (EOWPVT-R), Dunn’s Sensory Profile for Infants and Toddlers Caregiver Questionnaire and The Sensory Profile Care- giver Questionnaire for Children (3–10 years). | Severe mental retardation (MR) in addition to craniofacial, genital, endocrine, and heart abnormalities. Previously unappreciated intact nonverbal skills are evident in conjunction with moderate to severe developmental dyspraxia. |
| Samango-Sprouse et al., 2011 [11] | A multidisciplinary clinic was held during six consecutive years (July 2004–2009) at the Neurodevelopmental Diagnostic Center for Young Children in Davidsonville. | 22 boys 49, XXXXY with or without hormonal treatment. | The mean age of treatment for: Group 1 was 12 months with the mean age of first evaluation 74 months. The mean age of first evaluation for Group 2 was 87 months. | Leiter International Performance Scale-Revised (LIPS-R), Preschool Language Scales-4 (PLS-4), the Receptive One Word Vocabulary Test (ROW- PVT-R), Expressive One Word Picture Vocabulary Test- Revised (EOWPVT-R), MacArthur Communication Developmental Inventory (CDI), Gilliam Autism Rating Scale-2 (GARS-2). | Significant positive treatment effect in speech and language domain, gestural communication and vocabulary development. No treatment effect was seen in nonverbal capacities. |
| Lee et al., 2012 [2] | Patients recruited through advertisements via the NIH website and parent-support groups across North America. Controls were recruited from the US in a brain development study. | 110 youth with X/Y-aneuploidies (32 female) and 52 with typical development (25 female) | Mean age ~12 years | Wechsler Abbreviated Scale of Intelligence (WASI), Wechsler Preschool and Primary Scale of Intelligence–Third Edition (WPPSI-III), Children’s Communication Checklist-2, Social Responsiveness Scale. | Both supernumerary X- and Y-chromosomes were related to depressed structural and pragmatic language abilities and increased autistic traits. An additional Y-chromosome had a greater impact on pragmatic language; the addition of one or more X-chromosomes had a greater impact on structural language. |
| Cordeiro et al., 2012 [12] | Children’s Hospital Colorado (Denver), Thomas Jefferson University-Philadelphia (TJU). | 102 Males with XXY 40 XYY 32 XXYY | XXY: Mean age 10.8 years XYY: Mean age 9.93 years XXYY: Mean age 11.57 years | (1) Social Responsiveness Scale: Parent Report Questionnaire (SRS-P); (2) Cognitive testing: TJU—Differential Ability Scales–2nd edition (DAS-2). Denver—Wechsler Abbreviated Scale of Intelligence(WASI); Wechsler Intelligence Scale for Children–4th Edition (WISC-IV). | An additional Y chromosome may contribute to increased risk of autistic behaviours. |
| Tartaglia et al., 2012 [8] | Patients seen from 2004 to 2010 at the University of California—Davis MIND Institute and at Children’s Hospital Colorado. | 167 participants (XXY n = 56, XYY n = 33, XXX n = 25, XXYY n = 53) | Age 6–20 years | (1) Cognitive levels: Wechsler Abbreviated Scale of Intelligence (WASI), Wechsler Intelligence Scale for Children–Third Edition (WISC III), Wechsler Intelligence Scale for Children– Fourth Edition (WISC IV), Wechsler Adult Intelligence Scale–Third Edition (WAIS III); (2) Adaptive functioning: Vineland Adaptive Behaviour Scales-II, Adaptive Behaviour Assessment System—Second Edition (ABAS-II), Scales of Independent Behaviour—Revised (SIB-R); (3) ADHD: Conners’ Rating Scale, Swanson, Nolan, and Pelham Questionnaire—Fourth Edition (SNAP-IV). | 58% met DSM-IV criteria for ADHD on parent-report questionnaires. The Inattentive subtype was most common in XXY and XXX, whereas the XYY and XXYY groups were more likely to also have hyperactive/impulsive symptoms. Psychopharmacologic treatment with stimulants was effective in 78.6% (66/84). |
| Blumenthal et al., 2013 [13] | Patients recruited with the help of Neurodevelopmental Diagnostic Center for Young Children and a parent advocacy group; controls recruited from the community through the National Institutes of Health (NIH) Normal Volunteer Office, newspaper advertisements, and outreach to schools in the Washington, DC area. | 14 patients with 49, XXXXY 42 healthy controls | Mean age: 11.6 years | Wechsler Abbreviated Scale of Intelligence (WASI), Peabody Picture Vocabulary Test-4 (PPVT-4), Physical And Neurological Examination for Soft Signs (PANESS), Adaptive Behaviour Assessment System (ABAS), Child Behaviour Checklist (CBCL), MRI. | Increased dosage of genes on the X chromosome has adverse effects on white matter development. |
| Tartaglia et al., 2017 [14] | Participants from two sites (University of California (UC) Davis MIND Institute in Sacramento, California and Thomas Jefferson University (TJU) in Philadelphia, Pennsylvania) | XXY/KS (n = 20) XYY (n = 57) XXYY (n = 21) | Age 3–25 years. | (1) Cognitive levels—UC: Mullen Scales of Early Learning (MSEL), Wechsler Abbreviated Scale of Intelligence (WASI); TJU: Differential Abilities Scale-2nd Edition (DAS-2) (2) Adaptive functioning: Vineland Adaptive Behaviour Scales, 2nd Edition Interview Edition; (3) ASD: the Social Communication Questionnaire (SCQ), the Social Responsiveness Scale (SRS), and the Autism Diagnostic Observation Schedule (ADOS). the Autism Diagnostic Interview-Revised (ADI-R). | Males with Y chromosome aneuploidy (XYY and XXYY) were 4.8 times more likely to have a diagnosis of ASD than the XXY/KS group, and 20 times more likely than males in the general population. |
| Udhnani et al., 2018 [9] | Patients included in the Research program conducted at the National Institute of Mental Health (NIMH) Intramural Research Program. | 79 youth with SCAs and 42 typically developing controls | Age 6.60–22.60 years | Phonemic and semantic fluency conditions, Wechsler Abbreviated Scale of Intelligence, Wechsler Preschool and Primary Scale of Intelligence—Third edition. | Both supernumerary X and Y chromosomes were associated with verbal fluency deficits relative to controls. These impairments increased as a function of the number of extra X chromosomes. Whereas one supernumerary Y chromosome was associated with similar performance across fluency conditions, one supernumerary X chromosome was associated with relatively stronger semantic than phonemic fluency skills. |
| Burgemeister et al., 2018 [15] | 6/8 patients were participants of the 2015 and 2017 annual meetings of families with boys and men with 49,XXXXY syndrome; 1/8 was evaluated at the genetikum genetic practice in Stuttgart and one patient was seen and evaluated at the Institute of Human Genetics in Berlin. | 8 boys and men with 49, XXXXY | Age 3–24 years | HAWIK IV (Hamburg Wechsler Intelligence Test for Children, Version IV), SON-R (Snijders-Oomen Nonverbal Intelligence Test), K-ABC (Kaufmann Assessment Battery for Children), neurological and physical examination | Increasingly perceptible distinct facial gestalt over time; muscular hypotonia, radioulnar synostosis, white matter anomalies, fifth-finger clinodactyly, recurrent respiratory infections in early childhood and teeth anomalies. IQ scores ranged between 40–70. |
| Srinivasan et al., 2019 [16] | IMAGINE ID project | 15 children with XXYY and 30 controls; | 4–14 years | (1) Development and Well-being Assessment; (2) Strengths and Difficulties Questionnaire; (3)Everyday Feelings Questionnaire | Children with XXYY experienced significantly more frequent and intense temper outbursts than the control group. |
| Gropman et al., 2020 [17] | Patients received clinical evaluation as part of an annual conference for children diagnosed with 49,XXXXY and their families. | 67 boys with 49, XXXXY | Age 5 months–10 years | The Mental Development Index (MDI)/Cognitive domain of the Bayley Scales of Infant and Toddler Development (BSID), Second or Third Edition; Leiter International Performance Scale (LIPS), Revised or Third Edition; Wechsler Scales of Intelligence for Verbal IQ. | Higher neurocognitive capacities, both verbally and non-verbally, than previously reported. Infant boys who received early hormonal therapy had significantly higher scores on the cognitive domain of the Bayley Scales of Infant Development. |
| Samango-Sprouse et al., 2020 [18] | Patients evaluated by The Focus Foundation in collaboration with the Neurodevelopmental Diagnostic Center for Children; not every child was in attendance each year. | 72 boys with 49, XXXXY | Preschool/School-aged/Adolescence | Beery Buktenica Developmental Test of Visual-Motor Integration, Sixth Edition, the Bayley Scales of Infant and Toddler Development, Third Edition (BSID-III), and the Bruininks–Oseretsky Test of Motor Proficiency, Second Edition. | Truncal and extremity hypotonia significantly impact on motor milestones and ambulation; dysmorphic features include epicanthal folds, frontal bossing and synophrys. Visual perception skills are mildly impaired and cranial nerves are typically intact. Preschool boys treated with testosterone replacement had significantly increased scores on the BSID-III Psychomotor Development Index. |
| Lasutschinkow et al., 2020 [19] | Patients received clinical evaluation by The Focus Foundation in collaboration with the Neurodevelopmental Diagnostic Center for Children from 2004 until 2018. | 69 boys 49, XXXXY | Preschool/School-aged/Adolescence | Child Behaviour Checklist (CBCL), Social Responsiveness Scale, second edition (SRS-2), Behaviour Rating Inventory for Executive Function, second edition (BRIEF-2), Behaviour Rating Inventory for Executive Function-Preschool Edition (BRIEF-P). | Deficits in social cognition and communication beginning in preschool, with consistent social awareness and motivation for social activities; signs of anxiety presented during preschool years and increased in severity with age, particularly in internalizing problems. |
| Thompson et al., 2020 [1] | This study was part of an international survey to assess early therapies, school supports, and educational outcomes for children with SCA conditions. Participants were recruited through social media websites and email lists for the eXtraordinarY Kids Clinic of Children’s Hospital Colorado and the Association for X and Y Chromosome Variations (AXYS). Data were collected between 15 May and 15 July 2019. | n = 105 | Children not yet entered into Kindergarten | Closed-ended and multiple-choice questions to describe the supports for clinical population with demographic questions. Open-ended questions were also included to suggest questions about parent perspectives on supports for young children with SCAs. | Public early childhood intervention services with speech therapy as the most common service. Parents described interventions as desirable and effective yet also difficult to obtain due to issues with the SCA phenotype, lack of provider knowledge, and challenges navigating the intervention systems. |
| Samango-Sprouse et al., 2021 [20] | Patients eeceived clinical evaluation over the last 16 years as part of an annual conference for children and families hosted by the Focus Foundation in collaboration with the Neurodevelopmental Diagnostic Center for Children. | 85 boys with 49, XXXXY | Age 3 months–10.7 years | The Bayley Scales of Infant and Toddler Development; The Preschool Language Scales (PLS); The Expressive One-Word Picture Vocabulary Test (EOWPVT); Receptive One-Word Picture Vocabulary Test (ROWPVT); The Early Language Milestones Scale-2 (ELM-2). | Increased incidence (91.8%) of Childhood Apraxia of Speech. Differences were demonstrated between boys who received early hormonal treatment and untreated boys on the language scales of the Bayley Scales of Infants and Toddlers and on the Expressive One Word Picture Vocabulary Test. |
| Lee et al., 2021 [21] | Patients referred by their physicians for comprehensive neurodevelopmental evaluations. | 29: 47, XXY, 27: 49, XXXXY, 14: 46, XY | XXY: Mean age 12 years XXXXY: Mean age 8.6 years XY: no data | Behaviour Rating Inventory of Executive Function (BRIEF) and Child Behaviour Checklist (CBCL). Assays to compare saliva DNA between the 49,XXXXY and neurotypical 46, XY groups for methylation diferences in a small selection of genes on the X chromosome. | Higher levels of CpG methylation at regulatory intronic regions in X-linked genes encoding the androgen receptor (AR) and monoamine oxidase A (MAOA) may be linked to (externalizing) behaviour in boys with 49, XXXXY. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ricciardi, G.; Cammisa, L.; Bove, R.; Picchiotti, G.; Spaziani, M.; Isidori, A.M.; Aceti, F.; Giacchetti, N.; Romani, M.; Sogos, C. Clinical, Cognitive and Neurodevelopmental Profile in Tetrasomies and Pentasomies: A Systematic Review. Children 2022, 9, 1719. https://doi.org/10.3390/children9111719
Ricciardi G, Cammisa L, Bove R, Picchiotti G, Spaziani M, Isidori AM, Aceti F, Giacchetti N, Romani M, Sogos C. Clinical, Cognitive and Neurodevelopmental Profile in Tetrasomies and Pentasomies: A Systematic Review. Children. 2022; 9(11):1719. https://doi.org/10.3390/children9111719
Chicago/Turabian StyleRicciardi, Giacomina, Luca Cammisa, Rossella Bove, Giorgia Picchiotti, Matteo Spaziani, Andrea M. Isidori, Franca Aceti, Nicoletta Giacchetti, Maria Romani, and Carla Sogos. 2022. "Clinical, Cognitive and Neurodevelopmental Profile in Tetrasomies and Pentasomies: A Systematic Review" Children 9, no. 11: 1719. https://doi.org/10.3390/children9111719