
Evaluation and Treatment of Pain in Fetuses, Neonates and Children

 , and
, and
Abstract
:1. Introduction
2. Fetal Pain
2.1. Fetal Pain
2.2. Fetal Pain Evaluation
2.3. Treatment of Fetal Pain in Fetal Surgery
3. Neonatal Pain
4. Pain in Children
5. Pain Assessment
5.1. Concepts
- -
- The characteristics of the child: age, sex, sociocultural level and mood.
- -
- The characteristics of the pain: form of onset, intensity, evolution, duration, etiology and consequences that may be triggered [47].
5.2. Neonatal Pain Assessment Tools
5.3. Pain Assessment Tools for Children
5.3.1. Clinical Scales
- The visual analogue scale (VAS), which is represented on a 10 cm line between 0 (no pain) and 10 (worst pain imaginable). VAS < 4 indicates mild or mild–moderate pain, 4–6 indicates moderate–severe pain and >6 indicates severe pain.
- The verbal numeric scale (VNS): the child expresses their perception of pain from 0 (no pain) to 10 (worst pain imaginable).
- Graphic scales, which may consist of drawings of happy faces that change to sad according to the degree of pain, columns or thermometers that are more or less filled in, color ranges, etc.
- The FLACC scale (face, leg, activity, cry, consolability) (Table 3), which considers facial expression, leg attitude, spontaneous activity, the presence and characteristics of crying and the ability to comfort or consolability, with scores ranging between 0 and 2 points for each item. A value of 0 indicates no pain, and scores of 9–10 indicate unbearable pain.
- 2.
- MAPS scale (multidimensional assessment pain scale) (Table 4). This scale is based on the observation of body movements and facial expression. It is a multidimensional scale that also includes physiological parameters, such as breathing, changes in blood pressure (BP) and heart rate (HR). Similar to the FLACC scale, it classifies pain on a scale from 0 (no pain) to 9–10 (unbearable pain) [59].
5.3.2. Objective Pain Monitoring
6. Treatment
6.1. Non-Pharmacological Analgesia
6.2. Pharmacological Analgesia
6.2.1. Concepts
- Patient’s age and associated pathology (cardiorespiratory, renal and hepatic function);
- Check for interactions of analgesics with other medications the patient is receiving; and
- Prevent and treat the most common side effects of analgesics [97].
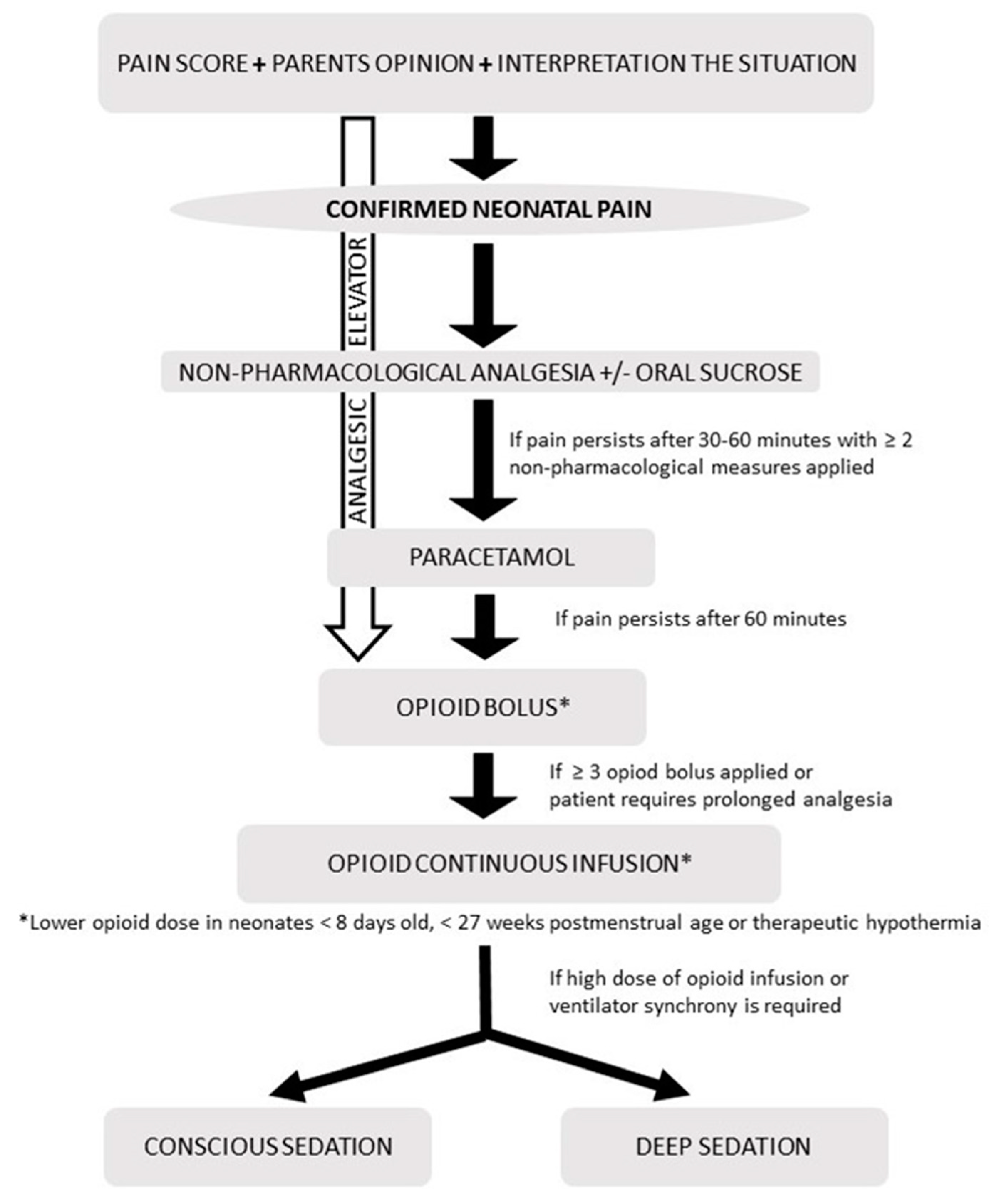
6.2.2. Pharmacological Analgesia in Neonates
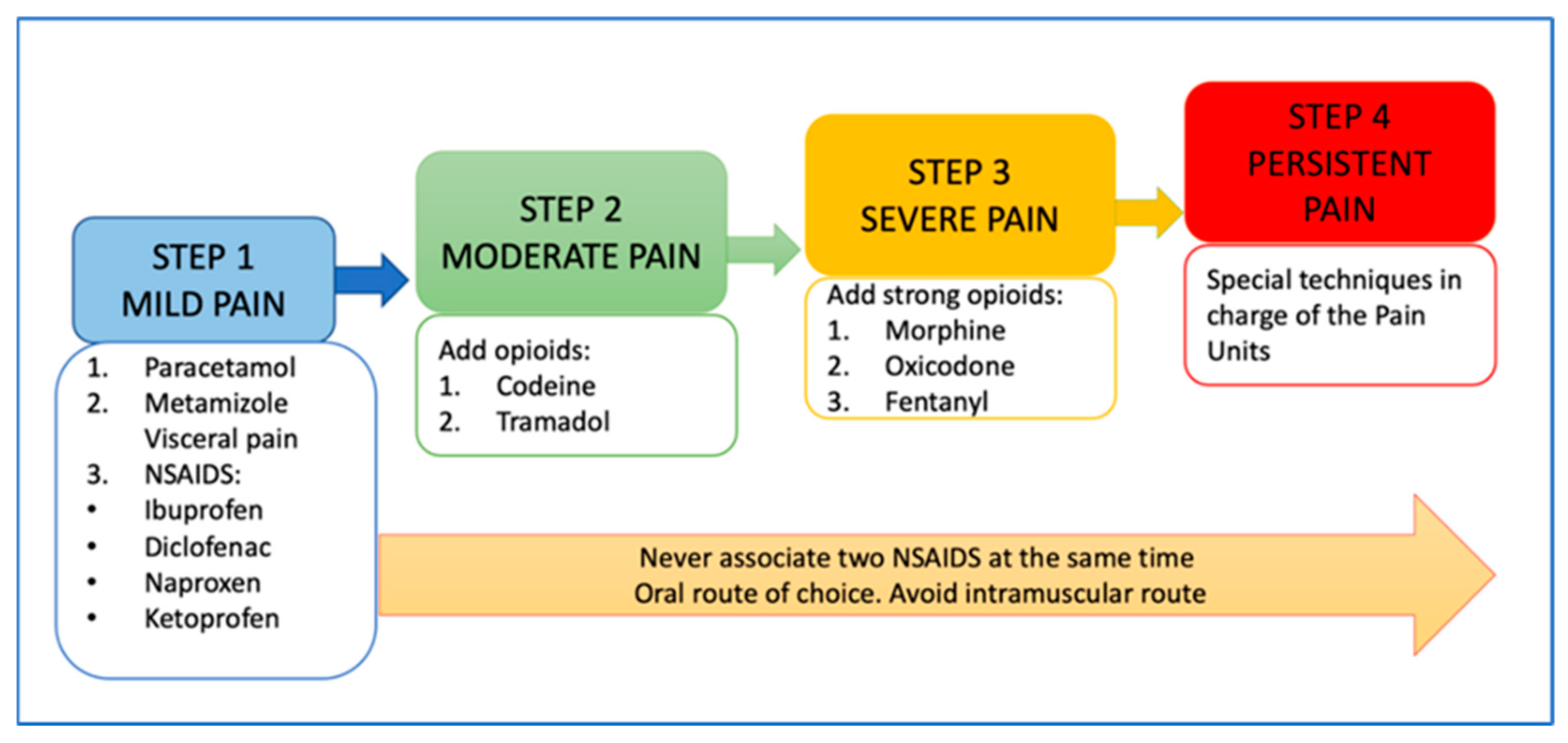
6.2.3. Pharmacological Analgesia in Children
6.3. Local Analgesia
6.4. Other Methods
6.4.1. PCA Pumps
6.4.2. Regional and Interventional Analgesia Techniques
7. Pain Assessment and Treatment Algorithm
8. Conclusions
Author Contributions
Funding
Acknowledgments
- -
- Garcia-Algar O, Neonatology Unit, ICGON, Hospital Clinic-Maternitat, BCNatal, Barcelona, Spain;
- -
- Andreu-Fernandez V, Grup de Recerca Infancia i Entorn (GRIE), Institut d’investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Madrid, Spain; Valencian International University (VIU), Valencia, Spain
- -
- Gomez-Roig MD, Institut de Recerca Sant Joan de Déu, Esplugues de Llobregat, Spain; BCNatal, Barcelona, Spain
- -
- Almeida L, Institut de Recerca Sant Joan de Déu, Esplugues de Llobregat, Spain; BCNatal, Barcelona, Spain.
- -
- Gerardo Rodríguez Growth, Exercise, Nutrition and Development (GENUD) Research Group, Universidad de Zaragoza, Spain. Instituto de Investigación Sanitaria Aragón (IIS Aragón), Spain
- -
- Iris Iglesia. Growth, Exercise, Nutrition and Development (GENUD) Research Group, Universidad de Zaragoza, Spain. Instituto de Investigación Sanitaria Aragón (IIS Aragón), Spain
- -
- María Cruz López Herrera. Department of Neonatology. Cruces University Hospital. Baracaldo (Vizcaya, Spain).
- -
- Margarita Ferrer. Department of Neonatology. Cruces University Hospital. Baracaldo (Vizcaya, Spain).
- -
- Fernando Cabañas Department of Paediatrics and Neonatology. Quironsalud Madrid University Hospital. Madrid
- -
- Manuela Lopez-Azorin. Department of Paediatrics and Neonatology. Quironsalud
- -
- Madrid University Hospital. Madrid
- -
- Carmen Pallas Alonso Department of Neonatology. 12 de Octubre University Hospital. Madrid.
- -
- Clara Alonso. Department of Neonatology. 12 de Octubre University Hospital. Madrid.
- -
- Santiago Mencía. Pediatric Intenisve Care Department. Hospital General Universitario Gregorio Marañón de Madrid.
- -
- Jesús López-Herce. Pediatric Intensive Care Department. Hospital General Universitario Gregorio Marañón de Madrid.
- -
- Raquel Cieza. Pediatric Intensive Care Department. Hospital General Universitario Gregorio Marañón de Madrid.
- -
- Jesús Cebrián. Sección de anestesia Pediátrica. Hospital General Universitario Gregorio Marañón de Madrid.
Conflicts of Interest
References
- Treede, R.D. The International Association for the Study of Pain definition of pain: As valid in 2018 as in 1979, but in need of regularly updated footnotes. Pain Rep. 2018, 3, e643. [Google Scholar] [CrossRef]
- Bondesson, E.; Olofsson, T.; Caverius, U.; Schelin, M.E.C.; Jöud, A. Consultation prevalence among children, adolescents and young adults with pain conditions: A description of age- and gender differences. Eur. J. Pain 2020, 24, 649–658. [Google Scholar] [CrossRef] [PubMed]
- Curtis, S.; Winger, A.; Ali, S. The Cochrane Library and procedural Pain in children: An overview of reviews. Evid. Based Child Health 2012, 7, 1363–1399. [Google Scholar] [CrossRef]
- Shah, P.; Siu, A. Considerations for neonatal and pediatric pain management. Am. J. Health Syst. Pharm. 2019, 76, 1511–1520. [Google Scholar] [CrossRef] [PubMed]
- Peng, P.; Stinson, J.N.; Choiniere, M.; Dion, D.; Intrater, H.; Lefort, S.; Lynch, M.; Ong, M.; Rashiq, S.; Tkachuk, G.; et al. Dedicated multidisciplinary pain management centres for children in Canada. Can. J. Anesth. 2007, 54, 985–991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, B.J.; Yamada, J.; Estabrooks, C.A.; Stinson, J.; Campbell, F.; Scott, S.D.; Cummings, G.; CIHR Team in Children’s Pain. Pain in hospitalized children: Effect of a multidimensional knowledge translation strategy on pain process and clinical outcomes. PAIN 2014, 155, 60–68. [Google Scholar] [CrossRef]
- Anand, K.J.; Hickey, P.R. Pain and its effects in the human neonate and fetus. N. Engl. J. Med. 1987, 317, 1321–1329. [Google Scholar] [CrossRef] [Green Version]
- Derbyshire, S.W. Foetal pain? Best Pract. Res. Clin. Obstet. Gynaecol. 2010, 24, 647–655. [Google Scholar] [CrossRef]
- Anand, K.J.; Carr, D.B. The neuroanatomy, neurophysiology, and neurochemistry of pain, stress, and analgesia in newborns and children. Pediatr. Clin. N. Am. 1989, 36, 795–822. [Google Scholar] [CrossRef]
- Lee, S.J.; Ralston, H.J.P.; Drey, E.A.; Partridge, J.C.; Rosen, M.A. Fetal pain: A systematic multidisciplinary review of the evidence. JAMA 2005, 294, 947–954. [Google Scholar] [CrossRef]
- Lowery, C.L.; Hardman, M.P.; Manning, N.; Hall, R.W.; Anand, K.J.; Clancy, B. Neurodevelopmental changes of fetal pain. Semin. Perinatol. 2007, 31, 275–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanold, P.O.; Luhmann, H.J. The Subplate and Early Cortical Circuits. Annu. Rev. Neurosci. 2010, 33, 23–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sekulic, S.; Gebauer-Bukurov, K.; Cvijanovic, M.; Kopitovic, A.; Ilic, D.; Petrovic, D.; Capo, I.; Pericin-Starcevic, I.; Christ, O.; Topalidou, A. Appearance of fetal pain could be associated with maturation of the mesodiencephalic structures. J. Pain Res. 2016, 9, 1031–1038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouza, H. The impact of pain in the immature brain. J. Matern. Fetal Neonatal Med. 2009, 22, 722–732. [Google Scholar] [CrossRef]
- Bellieni, C.V. New insights into fetal pain. Semin. Fetal Neonatal Med. 2019, 24, 101001. [Google Scholar] [CrossRef]
- Reissland, N.; Francis, B.; Mason, J. Can healthy fetuses show facial expressions of “pain” or “distress”? PLoS ONE 2013, 8, e65530. [Google Scholar] [CrossRef] [Green Version]
- Jardri, R.; Pins, D.; Houfflin-Debarge, V.; Chaffiotte, C.; Rocourt, N.; Pruvo, J.P.; Steinling, M.; Delion, P.; Thomas, P. Fetal cortical activation to sound at 33 weeks of gestation: A functional MRI study. Neuroimage 2008, 42, 10–18. [Google Scholar] [CrossRef]
- Matuz, T.; Govindan, R.B.; Preissl, H.; Siegel, E.R.; Muenssinger, J.; Murphy, P.; Ware, M.; Lowery, C.L.; Eswaran, H. Habituation of visual evoked responses in neonates and fetuses: A MEG study. Dev. Cogn. Neurosci. 2012, 2, 303–316. [Google Scholar] [CrossRef]
- Bellieni, C.V.; Sisto, R.; Cordelli, D.M.; Buonocore, G. Cry features reflect pain intensity in term newborns: An alarm threshold. Pediatr. Res. 2004, 55, 142–146. [Google Scholar] [CrossRef] [Green Version]
- Gingras, J.L.; Mitchell, E.A.; Grattan, K.E. Fetal homologue of infant crying. Arch. Dis. Child Fetal Neonatal Ed. 2005, 90, F415–F418. [Google Scholar] [CrossRef]
- Bernardes, L.S.; Ottolia, J.F.; Cecchini, M.; de Amorim Filho, A.G.; Teixeira, M.J.; Francisco, R.P.V.; de Andrade, D.C.; Grupo de Estudo da Dor Fetal (Fetal Pain Study Group). On the feasibility of accessing acute pain–related facial expressions in the human fetus and its potential implications: A case report. Pain Rep. 2018, 3, e673. [Google Scholar] [CrossRef] [PubMed]
- Petrikovsky, B.M.; Kaplan, G.P. Fetal responses to inadvertent contact with the needle during amniocentesis. Fetal Diagn. Ther. 1995, 10, 83–85. [Google Scholar] [CrossRef] [PubMed]
- Giannakoulopoulos, X.; Glover, V.; Sepulveda, W.; Kourtis, P.; Fisk, N.M. Fetal plasma cortisol and β-endorphin response to intrauterine needling. Lancet 1994, 344, 77–81. [Google Scholar] [CrossRef]
- Schuller, C.; Känel, N.; Müller, O.; Kind, A.B.; Tinner, E.M.; Hösli, I.; Zimmermann, R.; Surbek, D. Stress and pain response of neonates after spontaneous birth and vacuum-assisted and cesarean delivery. Am. J. Obstet. Gynecol. 2012, 207, e1–e6. [Google Scholar] [CrossRef]
- Duci, M.; Pulvirenti, R.; Fascetti Leon, F.; Capolupo, I.; Veronese, P.; Gamba, P.; Tognon, C. Anesthesia for fetal operative procedures: A systematic review. Front. Pain Res. 2022, 3, 935427. [Google Scholar] [CrossRef]
- Braden, A.; Maani, C.; Nagy, C. Anesthetic management of an ex utero intrapartum treatment procedure: A novel balanced approach. J. Clin. Anesth. 2016, 31, 60–63. [Google Scholar] [CrossRef] [Green Version]
- Kornacki, J.; Szydłowski, J.; Skrzypczak, J.; Szczepańska, M.; Rajewski, M.; Koziołek, A.; Gaca, M.; Wender-Ożegowska, E. Use of ex utero intrapartum treatment procedure in fetal neck and high airway anomalies–report of four clinical cases. J. Matern. Fetal Neonatal Med. 2019, 32, 870–874. [Google Scholar] [CrossRef]
- Han, G.; Li, L.; Tian, Y.; Xue, H.; Zhao, P. Influences of different doses of midazolam on mother and fetus in fetoscopic surgery for twin-to-twin transfusion syndrome. Pharmacology 2015, 96, 151–154. [Google Scholar] [CrossRef]
- Ruano, R.; Yoshisaki, C.; Da Silva, M.; Ceccon, M.; Grasi, M.; Tannuri, U.; Zugaib, M. A randomized controlled trial of fetal endoscopic tracheal occlusion versus postnatal management of severe isolated congenital diaphragmatic hernia. Ultrasound Obstet. Gynecol. 2012, 39, 20–27. [Google Scholar] [CrossRef]
- Chmait, R.H.; Chon, A.H.; Anselmo, D.; Vanderbilt, D.L.; Townsend, J.; Julian-Wang, B.; Don, D. In utero fetal intubation for a large neck mass: A minimally invasive EXIT option. Fetal Diagn. Ther. 2019, 45, 275–280. [Google Scholar] [CrossRef]
- Pedreira, D.A.; Zanon, N.; Nishikuni, K.; de Sá, R.A.M.; Acacio, G.L.; Chmait, R.H.; Kontopoulos, E.V.; Quintero, R.A. Endoscopic surgery for the antenatal treatment of myelomeningocele: The CECAM trial. Am. J. Obstet. Gynecol. 2016, 214, e1–e111. [Google Scholar] [CrossRef] [PubMed]
- Diguisto, C.; Winer, N.; Benoist, G.; Laurichesse-Delmas, H.; Potin, J.; Binet, A.; Lardy, H.; Morel, B.; Perrotin, F. In-utero aspiration vs expectant management of anechoic fetal ovarian cysts: Open randomized controlled trial. Ultrasound Obstet. Gynecol. 2018, 52, 159–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Said, S.M.; Qureshi, M.Y.; Taggart, N.W.; Anderson, H.N.; O’Leary, P.W.; Cetta, F.; Alrahmani, L.; Cofer, S.A.; Segura, L.G.; Pike, R.B.; et al. Innovative 2-step management strategy utilizing EXIT procedure for a fetus with hypoplastic left heart syndrome and intact atrial septum. Mayo Clin. Proc. 2019, 94, 356–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tkaczyk, M.; Stanczyk, M.; Krzeszowski, W.; Wojtera, J.; Litwinska, M.; Fortecka-Piestrzeniewicz, K.; Talar, T.; Pawlowska, B.; Olejniczak, D.; Podgorski, M.; et al. Neonatal survival and kidney function after prenatal interventions for obstructive uropathies. Ginekol. Pol. 2019, 90, 416–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baud, D.; Windrim, R.; Kachura, J.; Jefferies, A.; Pantazi, S.; Shah, P.; Langer, J.C.; Forsey, J.; Chaturvedi, R.R.; Jaeggi, E.; et al. Minimally invasive fetal therapy for hydropic lung masses: Three different approaches and review of the literature. Ultrasound Obstet. Gynecol. 2013, 42, 440–448. [Google Scholar] [CrossRef]
- Goksan, S.; Hartley, C.; Emery, F.; Cockrill, N.; Poorun, R.; Moultrie, F.; Rogers, R.; Campbell, J.; Sanders, M.; Adams, E.; et al. fMRI reveals neural activity overlap between adult and infant pain. Elife 2015, 4, e08663.2. [Google Scholar]
- McPherson, C.; Miller, S.P.; El-Dib, M.; Massaro, A.N.; Inder, T.E. The influence of pain, agitation, and their management on the immature brain. Pediatr. Res. 2020, 88, 168–175. [Google Scholar] [CrossRef]
- Doesburg, S.M.; Chau, C.M.; Cheung, T.P.; Moiseev, A.; Ribary, U.; Herdman, A.T.; Miller, S.P.; Cepeda, I.L.; Synnes, A.; Grunau, R.E. Neonatal pain-related stress, functional cortical activity and visual-perceptual abilities in school-age children born at extremely low gestational age. Pain 2013, 154, 1946–1952. [Google Scholar] [CrossRef] [Green Version]
- Ranger, M.; Chau, C.M.; Garg, A.; Woodward, T.S.; Beg, M.F.; Bjornson, B.; Poskitt, K.; Fitzpatrick, K.; Synnes, A.R.; Miller, S.P.; et al. Neonatal pain-related stress predicts cortical thickness at age 7 years in children born very preterm. PLoS ONE 2013, 8, e76702. [Google Scholar] [CrossRef] [Green Version]
- Moultrie, F.; Slater, R.; Hartley, C. Improving the treatment of infant pain. Curr. Opin. Support Paliat. Care 2017, 11, 112–117. [Google Scholar] [CrossRef] [Green Version]
- Tortora, D.; Severino, M.; Di Biase, C.; Malova, M.; Parodi, A.; Minghetti, D.; Traggiai, C.; Uccella, S.; Boeri, L.; Morana, G.; et al. Early Pain Exposure Influences Functional Brain Connectivity in Very Preterm Neonates. Front. Neurosci. 2019, 13, 899. [Google Scholar] [CrossRef] [PubMed]
- Vinall, J.; Miller, S.P.; Bjornson, B.H.; Fitzpatrick, K.P.; Poskitt, K.J.; Brant, R.; Synnes, A.R.; Cepeda, I.L.; Grunau, R.E. Invasive procedures in preterm children: Brain and cognitive development at school age. Pediatrics 2014, 133, 412–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Committee on Fetus and Newborn and Section on Anesthesiology and Pain Medicine. Prevention and Management of Procedural Pain in the Neonate: An Update. Pediatrics 2016, 137, e20154271. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Pediatrics; Committee on Psychosocial Aspects of Child and Family Health; Task Force on Pain in Infants, Children, and Adolescents. The assessment and management of acute pain in infants, children, and adolescents. Pediatrics 2001, 108, 793–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valdivieso Serna, A. Dolor agudo, analgesia y sedación en el niño (I): Detección y valoración. An. Esp. Pediatr. 1998, 48, 81–88. [Google Scholar]
- Baarslag, M.A.; Jhingoer, S.; Ista, E.; Allegaert, K.; Tibboel, D.; van Dijk, M. How often do we perform painful and stressful procedures in the paediatric intensive care unit? A prospective observational study. Aust. Crit. Care. 2019, 32, 4–10. [Google Scholar] [CrossRef]
- Maxwell, L.G.; Fraga, M.V.; Malavolta, C.P. Assessment of pain in the newborn: An Update. Clin. Perinatol. 2019, 46, 693–707. [Google Scholar] [CrossRef]
- Raeside, L. Physiologic measures of assessing infant pain: A literature review. Br. J. Nurs. 2011, 20, 1370–1376. [Google Scholar] [CrossRef]
- Anand, K.J.S. Pain assessment in preterm neonates. Pediatrics 2007, 119, 605. [Google Scholar] [CrossRef]
- Anand, K.J.S. Assessment of Neonatal Pain. 2019. Available online: www.uptodate.com (accessed on 8 September 2022).
- Perry, M.; Tan, Z.; Chen, J.; Weidig, T.; Xu, W.; Cong, X.S. Neonatal Pain: Perceptions and Current Practice. Crit. Care Nurs. Clin. N. Am. 2018, 30, 549–561. [Google Scholar] [CrossRef]
- Giordano, V.; Edobor, J.; Deindl, P.; Wildner, B.; Goeral, K.; Steinbauer, P.; Werther, T.; Berger, A.; Olischar, M. Pain and Sedation Scales for Neonatal and Pediatric Patients in a Preverbal Stage of Development: A Systematic Review. JAMA Pediatr. 2019, 173, 1186–1197. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.; Ramelet, A.S.; Van Dick, M.; Pokorna, P.; Wielenga, J.; Tume, L.; Tibboel, D.; Ista, E. Clinical recommendations for pain, sedation, withdrawall and delirium assessment in critically ill infants and children: An ESPINC position statement for health care professionals. Int. Care Med. 2016, 42, 972–986. [Google Scholar] [CrossRef] [PubMed]
- Hicks, C.L.; von Baeyer, C.L.; Spafford, P.A.; van Korlaar, I.; Goodenough, B. The Faces Pain Scale-Revised: Toward a common metric in pediatric pain measurement. Pain 2001, 93, 173–183. [Google Scholar] [CrossRef]
- Van Dijk, M.; de Boer, J.B.; Koot, H.M.; Duivenvoorden, H.J.; Passchier, J.; Bouw Meester, N.; Tibboel, D. The association between physiological and behavioral pain measures in 0 to 3 years old infants after major surgery. J. Pain Symptom Manag. 2001, 22, 600–609. [Google Scholar] [CrossRef]
- Voepel-Lewis, T.; Malviya, S.; Tait, A.R.; Merkel, S.; Foster, R.; Krane, E.J.; Davis, P.J. A comparison of clinical utility of pain assessment tools for children with cognitive impairment. Anesth. Analg. 2008, 106, 72–78. [Google Scholar] [CrossRef]
- Geary, T.; Negus, A.; Anderson, B.; Zernikow, B. Perioperative management of the child on long-term opioids. Pediatric Anesthesia 2012, 22, 189–202. [Google Scholar] [CrossRef]
- Ramelet, A.S.; Rees, N.; McDonald, S.; Bulsara, M.; Abu-Saad, H.H. Development and preliminary psychometric testing of the Multidimensional Assessment of Pain Scale: MAPS. Paediatr. Anaesth. 2007, 17, 333–340. [Google Scholar] [CrossRef]
- Ledowski, T.; Averhoff, L.; Tiong, W.S.; Lee, C. Analgesia Nociception Index (ANI) to predict intraoperative haemodynamic changes: Results of a pilot investigation. Acta Anaesthesiol. Scand. 2014, 58, 74–79. [Google Scholar] [CrossRef]
- Migeon, A.; Desgranges, F.P.; Chassard, D.; Blaise, B.J.; De Queiroz, M.; Stewart, A.; Cejka, J.C.; Combet, S.; Rhondali, O. Pupillary reflex dilatation and analgesia nociception index monitoring to assess the effectiveness of regional anesthesia in children anesthetised with sevoflurane. Paediatr. Anaesth. 2013, 23, 1160–1165. [Google Scholar] [CrossRef]
- Solana, M.J.; Lopez-Herce, J.; Fernandez, S.; Gonzalez, R.; Urbano, J.; Lopez, J.; Bellon, J.M. Assessment of pain in critically ill children. Is cutaneous conductance a reliable tool? J. Crit. Care 2015, 30, 481–485. [Google Scholar] [CrossRef]
- Tiryaki, Ö.; Doğu, Ö.; Okumuş, G.Y.; Tuna, A.T.; Bayar, F. Analgesia Nociception Index Monitoring in the Evaluation of Postoperative Pain in Children: A Prospective Observational Pilot Study. J. Perianesth. Nurs. 2022. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Gadi, G.U.; Panigrahy, A.; Tam, E.W.Y. Using Neuroimaging to Study the Effects of Pain, Analgesia, and Anesthesia on Brain Development. J. Neurosurg. Anesthesiol. 2019, 31, 119–121. [Google Scholar] [CrossRef]
- Williams, G. What dilemmas do healthcare workers face looking after children with acute pain? Pain Manag. 2017, 7, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Lonnqvist, P.A. Pediatric pain review: What has happened since the First World Congress on Pediatric Pain in 1988? The past, the present and the future. Minerva Anestesiol. 2020, 86, 1205–1213. [Google Scholar] [CrossRef] [PubMed]
- Pitchon, D.N.; Dayan, A.C.; Schwenk, E.S.; Baratta, J.L.; Viscusi, E.R. Updates on Multimodal Analgesia for Orthopedic Surgery. Anesthesiol. Clin. 2018, 36, 361–373. [Google Scholar] [CrossRef] [PubMed]
- Gaglani, A.; Gross, T. Pediatric Pain Management. Emerg. Med. Clin. N. Am. 2018, 36, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Dancel, R.; Liles, E.A.; Fiore, D. Acute Pain Management in Hospitalized Children. Rev. Recent Clin. Trials 2017, 12, 277–283. [Google Scholar] [CrossRef]
- Williams, S.; Keogh, S.; Douglas, C. Improving paediatric pain management in the emergency department: An integrative literature review. Int. J. Nurs. Stud. 2019, 94, 9–20. [Google Scholar] [CrossRef]
- Palmer, G.M. Pain management in the acute care setting: Update and debates. J. Paediatr. Child Health 2016, 52, 213–220. [Google Scholar] [CrossRef]
- Wu, Y.; Zhao, Y.; Wu, L.; Zhang, P.; Yu, G. Non-pharmacological management for vaccine-related pain in children in the healthcare setting: A scoping review. J. Pain Res. 2022, 15, 2773–2782. [Google Scholar] [CrossRef]
- Pillai Riddell, R.R.; Racine, N.M.; Hennis, H.G.; Turcotte, K.; Uman, L.S.; Horton, R.E.; Kohut, S.A.; Stuart, J.H.; Stevens, B.; Lisi, D.M. Non-pharmacological management of infant and young child procedural pain. Cochrane Database Syst. Rev. 2015, 12, CD006275. [Google Scholar] [CrossRef]
- Keefe, K.R.; Byrne, K.J.; Levi, J.R. Treating pediatric post-tonsillectomy pain and nausea with complementary and alternative medicine. Laryngoscope 2018, 128, 2625–2634. [Google Scholar] [CrossRef]
- Uman, L.S.; Chambers, C.T.; McGrath, P.J.; Kisely, S.R. Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database Syst. Rev. 2013, 10, CD005179. [Google Scholar] [CrossRef] [Green Version]
- Bucsea, O.; Pillai Riddell, R. Non-pharmacological pain management in the neonatal intensive care unit: Managing neonatal pain without drugs. Semin. Fetal Neonatal Med. 2019, 24, 101017. [Google Scholar] [CrossRef]
- Lester, B.M.; Hawes, K.; Abar, B.; Sullivan, M.; Miller, R.; Bigsby, R.; Laptook, A.; Salisbury, A.; Taub, M.; Lagasse, L.L. Single-family room care and neurobehavioural and medical outcomes in preterm infants. Pediatrics 2014, 134, 754–760. [Google Scholar] [CrossRef] [Green Version]
- Mangat, A.K.; Oei, J.L.; Chen, K.; Quah-Smith, I.; Schmölzer, G.M. A Review of Non-Pharmacological Treatments for Pain Management in Newborn Infants. Children 2018, 5, 130. [Google Scholar] [CrossRef] [Green Version]
- Shah, P.S.; Herbozo, C.; Aliwalas, L.L.; Shah, V.S. Breastfeeding or breast milk for procedural pain in neonates. Cochrane Database Syst. Rev. 2012, 12, CD004950. [Google Scholar] [CrossRef]
- Collados-Gómez, L.; Ferrera-Camacho, P.; Fernández-Serrano, E.; Camacho-Vicente, V.; Flores-Herrero, C.; García-Pozo, A.M.; Jiménez-García, R. Randomised crossover trial showed that using breast milk or sucrose provided the same analgesic effect in preterm infants of at least 28 weeks. Acta Paediatr. 2018, 107, 436–441. [Google Scholar] [CrossRef]
- Ou-Yang, M.C.; Chen, I.L.; Chen, C.C.; Chung, M.Y.; Chen, F.S.; Huang, H.C. Expressed breast milk for procedural pain in preterm neonates: A randomized, double-blind, placebo-controlled trial. Acta Paediatr. 2013, 102, 15–21. [Google Scholar] [CrossRef]
- Stevens, B.; Yamada, J.; Ohlsson, A.; Haliburton, S.; Shorkey, A. Sucrose for analgesia in newborn infants undergoing painful procedures. Cochrane Database Syst. Rev. 2016, 7, CD001069. [Google Scholar] [CrossRef]
- Gao, H.; Gao, H.; Xu, G.; Li, M.; Du, S.; Li, F.; Zhang, H.; Wang, D. Efficacy and safety of repeated oral sucrose for repeated procedural pain in neonates: A systematic review. Int. J. Nurs. Stud. 2016, 62, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Johnston, C.; Campbell-Yeo, M.; Disher, T.; Benoit, B.; Fernandes, A.; Streiner, D.; Inglis, D.; Zee, R. Skin-to-skin care for procedural pain in neonates. Cochrane Database Syst. Rev. 2017, 2, CD008435. [Google Scholar] [CrossRef] [PubMed]
- Locatelli, C.; Bellieni, C.V. Sensorial saturation and neonatal pain: A review. J. Matern. Fetal Neonatal. Med. 2018, 31, 3209–3213. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Fu, Y.; Yang, Y.; Zhou, Y.E. Control effect of virtual reality technology on procedural pain in children’s wound: A meta-analysis. Medicine 2022, 101, e30961. [Google Scholar] [CrossRef]
- van der Heijden, M.J.; Oliai Araghi, S.; Jeekel, J.; Reiss, I.K.; Hunink, M.G.; van Dijk, M. Do hospitalized premature infants benefit from music interventions? A systematic review of randomized controlled trials. PLoS ONE 2016, 11, e0161848. [Google Scholar] [CrossRef] [Green Version]
- Chirico, G.; Cabano, R.; Villa, G.; Bigogno, A.; Ardesi, M.; Dioni, E. Randomised study showed that recorded maternal voices reduced pain in preterm infants undergoing heel lance procedures in a neonatal intensive care unit. Acta Paediatr. 2017, 106, 1564–1568. [Google Scholar] [CrossRef]
- Juneau, A.L.; Aita, M.; Héon, M. Review and Critical Analysis of Massage Studies for Term and Preterm Infants. Neonatal Netw 2015, 34, 165. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Hall, R.W.; Golianu, B.; Yates, C.; Williams, D.K.; Chang, J.; Anand, K.J. Does noninvasive electrical stimulation of acupuncture points reduce heelstick pain in neonates? Acta Paediatr. 2016, 105, 1434. [Google Scholar] [CrossRef] [Green Version]
- Feng, H.; König, J.; König, T.; Muensterer, O. A randomized, placebo-controlled study of magnetic acupuncture for supplementary analgesia after laparoscopic appendectomy in children. J. Pediatr. Surg. 2022. [Google Scholar] [CrossRef]
- Cerritelli, F.; Cicchitti, L.; Martelli, M.; Barlafante, G.; Renzetti, C.; Pizzolorusso, G.; Lupacchini, M.; D’Orazio, M.; Marinelli, B.; Cozzolino, V.; et al. Osteopathic manipulative treatment and pain in preterms: Study protocol for a randomised controlled trial. Trials 2015, 16, 84. [Google Scholar] [CrossRef] [Green Version]
- Gray, L.; Garza, E.; Zageris, D.; Heilman, K.J.; Porges, S.W. Prevention and treatment of neonatal pain. Sucrose and warmth for analgesia in healthy newborns: An RCT. Pediatrics 2015, 135, e607. [Google Scholar] [CrossRef] [Green Version]
- Turner, A.D.; Sullivan, T.; Drury, K.; Hall, T.A.; Williams, C.N.; Guilliams, K.P.; Murphy, S.; Iqbal O’Meara, A.M. Cognitive Dysfunction After Analgesia and Sedation: Out of the Operating Room and Into the Pediatric Intensive Care Unit. Front. Behav. Neurosci. 2021, 15, 713668. [Google Scholar] [CrossRef]
- Berde, C.B.; Sethna, N.F. Drug therapy: Analgesics for the treatment of pain in children. N. Engl. J. Med. 2002, 347, 1094–1103. [Google Scholar] [CrossRef]
- Saini, A.; Maher, K.O.; Deshpande, S.R. Nonopioid analgesics for perioperative and cardiac surgery pain in children: Current evidence and knowledge gaps. Ann. Pediatr. Cardiol. 2020, 13, 46–55. [Google Scholar]
- Zhu, A.; Benzon, H.A.; Anderson, T.A. Evidence for the Efficacy of Systemic Opioid-Sparing Analgesics in Pediatric Surgical Populations: A Systematic Review. Anesth. Analg. 2017, 125, 1569–1587. [Google Scholar] [CrossRef]
- Poonai, N.; Zhu, R. Analgesia for Children in Acute Pain in the Post-codeine Era. Curr. Pediatr. Rev. 2018, 14, 34–40. [Google Scholar] [CrossRef]
- Boric, K.; Dosenovic, S.; Jelicic, A.; Batinic, M.; Cavar, M.; Urlic, M.; Markovina, N.; Puljak, L. Interventions for postoperative pain in children: An overview of systematic reviews. Paediatr. Anaesth. 2017, 27, 893–904. [Google Scholar] [CrossRef]
- Hall, R.W.; Anand, K.J. Pain management in newborns. Clin. Perinatol. 2014, 41, 895–924. [Google Scholar] [CrossRef] [Green Version]
- Schiller, R.M.; Allegaert, K.; Hunfeld, M.; van den Bosch, G.E.; van den Anker, J.; Tibboel, D. Analgesics and Sedatives in Critically Ill Newborns and Infants: The Impact on Long-Term Neurodevelopment. J. Clin. Pharmacol. 2018, 58 (Suppl. S10), S140–S150. [Google Scholar] [CrossRef] [Green Version]
- Valeri, B.O.; Holsti, L.; Linhares, M.B.M. Neonatal pain and developmental outcomes in children born preterm: A systematic review. Clin. J. Pain 2015, 31, 355–362. [Google Scholar] [CrossRef]
- Zwicker, J.G.; Miller, S.P.; Grunau, R.E.; Chau, V.; Brant, R.; Studholme, C.; Liu, M.; Synnes, A.; Poskitt, K.J.; Stiver, M.L.; et al. Smaller Cerebellar Growth and Poorer Neurodevelopmental Outcomes in Very Preterm Infants Exposed to Neonatal Morphine. J. Pediatr. 2016, 172, 81–87.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rana, D.; Bellflower, B.; Sahni, J.; Kaplan, A.J.; Owens, N.T.; Arrindell, E.L., Jr.; Talati, A.J.; Dhanireddy, R. Reduced narcotic and sedative utilization in a NICU after implementation of pain management guidelines. J. Perinatol. 2017, 37, 1038–1042. [Google Scholar] [CrossRef] [PubMed]
- Thigpen, J.C.; Odle, B.L.; Harirforoosh, S. Opioids: A Review of Pharmacokinetics and Pharmacodynamics in Neonates, Infants, and Children. Eur. J. Drug Metab. Pharmacokinet. 2019, 44, 591–609. [Google Scholar] [CrossRef] [PubMed]
- McPherson, C.; Ortinau, C.M.; Vesoulis, Z. Practical approaches to sedation and analgesia in the newborn. J. Perinatol. 2020, 29, 1–13. [Google Scholar] [CrossRef]
- Ancora, G.; Lago, P.; Garetti, E.; Merazzi, D.; Savant Levet, P.; Bellieni, C.V.; Bellieni, C.V.; Pieragostini, L.; Pirelli, A. Evidence-based clinical guidelines on analgesia and sedation in newborn infants undergoing assisted ventilation and endotracheal intubation. Acta Paediatr. 2019, 108, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Squillaro, A.; Mahdi, E.M.; Tran, N.; Lakshmanan, A.; Kim, E.; Kelley-Quon, L.I. Managing Procedural Pain in the Neonate Using an Opioid-sparing Approach. Clin. Ther. 2019, 41, 1701–1713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carbajal, R.; Eriksson, M.; Courtois, E. Sedation and analgesia practices in neonatal intensive care units (EUROPAIN): Results from a prospective cohort study. Lancet Respir. Med. 2015, 3, 796–812. [Google Scholar] [CrossRef]
- Setlur, A.; Friedland, H. Treatment of pain with intranasal fentanyl in pediatric patients in an acute care setting: A systematic review. Pain Manag. 2018, 8, 341–352. [Google Scholar] [CrossRef]
- Grunauer, M.; Mikesell, C.; Bustamante, G.; Cobo, G.; Sánchez, S.; Román, A.M.; Icaza-Freire, A.P.; Gavilanes, A.W.D.; Wang, N.E.; PICU-MIC Research Group. PICU-MIC Research Group. Pain Assessment and Management in Pediatric Intensive Care Units Around the World, an International, Multicenter Study. Front. Pediatr. 2021, 9, 746489. [Google Scholar] [CrossRef]
- Alanazi, E. The Effectiveness of Ketamine Compared to Opioid Analgesics for management of acute pain in Children in The Emergency Department: Systematic Review. Am. J. Emerg. Med. 2022, 61, 143–151. [Google Scholar] [CrossRef]
- Valentine, K.; Kummick, J. Analgesia, Sedation, Paralytics, Delirium, and Iatrogenic Withdrawal. Pediatr. Clin. N. Am. 2022, 69, 531–546. [Google Scholar] [CrossRef]
- Iqbal, A.U.; Shuster, M.E.; Baum, C.R. Ketofol for Procedural Sedation and Analgesia in the Pediatric Population. Pediatr. Emerg. Care 2022, 38, 28–33. [Google Scholar] [CrossRef]
- Krmpotic, K.; Rieder, M.J.; Rosen, D. Recommendations for procedural sedation in infants, children, and adolescents. Paediatr. Child Health. 2021, 26, 128–129. [Google Scholar] [CrossRef] [PubMed]
- Egbuta, C.; Mason, K.P. Current State of Analgesia and Sedation in the Pediatric Intensive Care Unit. J. Clin. Med. 2021, 10, 1847. [Google Scholar] [CrossRef] [PubMed]
- Ramalho, C.E.; Bretas, P.M.C.; Schvartsman, C.; Reis, A.G. Sedation and analgesia for procedures in the pediatric emergency room. J. Pediatr. 2017, 93 (Suppl. S1), 2–18. [Google Scholar] [CrossRef] [PubMed]
- Daverio, M.; von Borell, F.; Ramelet, A.S.; Sperotto, F.; Pokorna, P.; Brenner, S.; Brenner, S.; Mondardini, M.C.; Tibboel, D.; Amigoni, A.; et al. Analgosedation CONSORTIUM on behalf of the Pharmacology Section and the Nurse Science Section of the European Society of Paediatric and Neonatal Intensive Care. Pain and sedation management and monitoring in pediatric intensive care units across Europe: An ESPNIC survey. Crit. Care 2022, 26, 88. [Google Scholar]
- Gupta, N.; Gupta, A.; Narayanan, M.R.V. Current status of nitrous oxide use in pediatric patients. World J. Clin. Pediatr. 2022, 11, 93–104. [Google Scholar] [CrossRef]
- Foster, J.P.; Taylor, C.; Spence, K. Topical anaesthesia for needle-related pain in newborn infants. Cochrane Database Syst. Rev. 2017, 2, CD010331. [Google Scholar] [CrossRef]
- Shahid, S.; Florez, I.D.; Mbuagbaw, L. Efficacy and safety of EMLA cream for pain control due to venipuncture in infants: A meta-analysis. Pediatrics 2019, 143, e20181173. [Google Scholar] [CrossRef] [Green Version]
- Sharara-Chami, R.; Lakissian, Z.; Charafeddine, L.; Milad, N.; El-Hout, Y. Combination Analgesia for Neonatal Circumcision: A Randomized Controlled Trial. Pediatrics 2017, 140, e20171935. [Google Scholar] [CrossRef]
- Kaur, H.; Negi, V.; Sharma, M.; Mahajan, G. Study of pain response in neonates during venipuncture with a view to analyse utility of topical anaesthetic agent for alleviating pain. Med. J. Armed Forces India 2019, 75, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Dilli, D.; İlarslan, N.E.; Kabataş, E.U.; Zenciroğlu, A.; Şimşek, Y.; Okumuş, N. Oral sucrose and non-nutritive sucking goes some way to reducing pain during retinopathy of prematurity eye examinations. Acta Paediatr. 2014, 103, e76–e79. [Google Scholar] [CrossRef] [PubMed]
- Suresh, S.; Ecoffey, C.; Bosenberg, A.; Lonnqvist, P.A.; de Oliveira, G.S., Jr.; de Leon Casasola, O.; de Andrés, J.; Ivani, G. The European Society of Regional Anaesthesia and Pain Therapy/American Society of Regional Anesthesia and Pain Medicine Recommendations on Local Anesthetics and Adjuvants Dosage in Pediatric Regional Anesthesia. Reg. Anesth. Pain Med. 2018, 43, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Stein, A.L.; Baumgard, D.; Del Rio, I.; Tutiven, J.L. Updates in Pediatric Regional Anesthesia and Its Role in the Treatment of Acute Pain in the Ambulatory Setting. Curr. Pain Headache Rep. 2017, 21, 11. [Google Scholar] [CrossRef]
- Deer, J.D.; Sawardekar, A.; Suresh, S. Day surgery regional anesthesia in children: Safety and improving outcomes, do they make a difference? Curr. Opin. Anaesthesiol. 2016, 29, 691–695. [Google Scholar] [CrossRef]
- Vargas, A.; Sawardekar, A.; Suresh, S. Updates on pediatric regional anesthesia safety data. Curr. Opin. Anaesthesiol. 2019, 32, 649–652. [Google Scholar] [CrossRef]
- Álvarez-Baena, L.; Hervías, M.; Ramos, S.; Cebrián, J.; Pita, A.; Hidalgo, I. Continuous thoracic paravertebral analgesia after minimally invasive atrial septal defect closure surgery in pediatric population: Effectiveness and safety analysis. Rev. Esp. Anestesiol. Reanim. 2022, 69, 259–265. [Google Scholar] [CrossRef]
- Fernández, S.N.; Toledo, B.; Cebrián, J.; Pérez-Caballero, R.; López-Herce, J.; Mencía, S. Continuous Incisional Lidocaine in Pediatric Patients following Open Heart Surgery. Biomed. Res. Int. 2022, 2022, 1403539. [Google Scholar] [CrossRef]
- van Dijk, M.; Tibboel, D. Update on pain assessment in sick neonates and infants. Pediatr. Clin. N. Am. 2012, 59, 1167–1181. [Google Scholar] [CrossRef]
- Ventafridda, V.; Saita, L.; Ripamonti, C.; De Conno, F. WHO guidelines for the use of analgesics in cancer pain. React. Int. J. Tissue 1985, 7, 93–96. [Google Scholar]



{kind=link}
{kind=link}
| Neonates and Infants | Children | Adults | |
|---|---|---|---|
| Development of pain sensitivity | Yes, undefined | Yes, defined | Yes, defined |
| Location of pain | No | No; Yes in older children | Yes |
| Verbal expression | Cry | Verbal; Could be non-specific | Verbal and specific |
| Pain response | Important and generalized (tachycardia, tachypnea, hypertension–hypotension, severe stress and agitation) | Important in toddlers;Moderate in older children | Mild |
| Difference between anxiety and pain | No | Only older children | Yes |
| Clinical evaluation | Physiological scales | Physiological and verbal scales, non-numerical | Numerical scales |
| Analgesic drugs | Very few studies; Empirical off-label treatment for most drugs; Undefined doses | Few studies; Empirical off-label treatment for most drugs | Many studies; Well-defined doses |
| Side effects of analgesic drugs | Severe systemic side effects (bradycardia, hypotension and respiratory arrest) Psychomotor development effect? | Moderate systemic side effects Psychomotor development effect? | Mild systemic side effects |
| Pain Scale | Gestational Age | Parameters | Type of Pain | Scale Metric |
|---|---|---|---|---|
| PIPP-R (premature infant pain profile-revised) | 26 weeks to term | Heart rate and oxygen saturation. Alertness, brow bulge, eye squeeze and nasolabial furrow | Procedural and postoperative | 0–21 |
| CRIES (cries, requires oxygen, increased vital signs, expression, sleeplessness) | 32–56 weeks | Blood pressure, heart rate, oxygen saturation. Cry, expression and sleeplessness | Postoperative | 0–10 |
| NIPS (neonatal infant pain scale) | 28–38 weeks | Breathing pattern. Facial expression, cry, arms, legs and alertness | Procedural | 0–7 |
| COMFORT neo | 24–42 weeks | Respiratory response, blood pressure and heart rate. Alertness, agitation, physical movements, muscle tone and facial tension | Prolonged | 8–40 |
| NFCS (neonatal facial coding system) | 25 weeks to term | Brow bulge, eye squeeze, nasolabial furrow, open lips, stretched mouth, lip purse, taut tongue and chin quiver | Procedural | 0–10 |
| N-PASS (neonatal pain, agitation and sedation scale) | 0–100 days | Heart rate, respiratory rate, blood pressure and oxygen saturation. Crying or irritability, behavior state, facial expression, extremities or tone | Acute and prolonged pain. Also assesses sedation | Pain 0–10 Sedation −10–0 |
| EDIN (échelle de la douleur inconfort noveau-né) | 25–36 weeks | Facial activity, body movements, quality of sleep, quality of contact with nurses and consolability | Prolonged | 0–15 |
| BPSN (Bernese pain scale for neonates) | 27–41 weeks | Respiratory pattern, heart rate and oxygen saturation. Alertness, duration of cry, time to calm, skin color, brow bulge with eye squeeze and posture | Procedural | 0–27 |
| 0 | 1 | 2 | |
|---|---|---|---|
| Face | No particular expression or smile | Occasional grimace or frown, withdrawn, disinterested. | Frequent to constant quivering chin, clenched jaw |
| Legs | Normal position or relaxed | Uneasy, restless, tense | Kicking or legs drawn up |
| Activity | Crying quietly, normal position, moves easily. | Squirming, shifting back and forth, tense. | Arched, rigid or jerking. |
| Cry | No cry (awake or asleep) | Moans or whimpers; occasional complaint. | Crying steadily, screams or sobs, frequent complaints. |
| Consolability | Content, relaxed. | Reassured by occasional touching, hugging or being talk to; distractible. | Difficult to console or comfort. |
| 0 | 1 | 2 | |
|---|---|---|---|
| Vital signs: HR and/or BP | Within baseline | More than 10 bpm increase and/or more than 10 mmHg increase | More than 10 bpm decrease and/or more than 10 mmHg decrease |
| Breathing pattern | No change | Development or increase in respiratory distress | Severe respiratory distress |
| Facial expression | Relaxed | Grimace | Grimace associated with silent or weak cry |
| Body movements | No movements or purposeful movements | Restless | Rigid and/or limited body movements |
| State of arousal | Calm or asleep | Hyperreactive | Shut down |
| Drug | Dose | Pharmacology | Indications | Adverse Effects |
|---|---|---|---|---|
| Morphine | Boluses: 30–50 mcg/kg, maximum 100 mcg/kg over 15–30 min Infusion: 30–100 mcg/kg bolus followed by 10 mcg/kg/h A lower initial dose is recommended. Therapeutic hypothermia: Bolus of 50 mcg/kg, followed by 5 mcg/kg/h infusion | Action of 5 min. Peak effectiveness: 15 min. Half-life: 6–12 h | Analgesia and sedation in mechanical ventilation; postoperative pain control; sedation during therapeutic hypothermia. Not be used in preterm infants less than 27 weeks and neonates with hemodynamic instability | Hypotension, respiratory arrest, urinary retention, tolerance, withdrawal, risk of periventricular leukomalacia and/or death; poor long-term neurodevelopmental outcomes |
| Fentanyl | Bolus of 0.5–2.0 μg/kg Infusion: 0.5–2.0 μg/kg/h Preterm neonates born before 32 w g reduced by 50% during days 0–4, Therapeutic hypothermia 1–2 mcg/kg over one hour and then infusion to 0.5–1 mcg/kg/h | Action of 1–2 min. Duration of action: 60 min. Half-life: 3.1–9.5 h | Short procedures. Analgesia and sedation in mechanical ventilation; sedation during therapeutic hypothermia | Respiratory arrest, chest wall rigidity, laryngospasm, tolerance withdrawal, delayed meconium passage. Cerebellar hypoplasia; decrease in eye and hand coordination skills at two years |
| Remifentanil | Endotracheal intubation:1–2 μg/kg. Percutaneous central venous catheter: 0.25 μg/kg/min Sedation and analgesia in mechanical ventilation: 0.15 μg/kg/min | Action: 1 min Half-life: 3.5–5 min. | Short procedures: endotracheal intubation, laser surgery for retinopathy of prematurity | Bradycardia, hypotension, chest wall rigidity, tolerance and withdrawal; no studies of long-term outcome in neonates |
| Paracetamol | Oral dose: 25 mg/kg/day in at 30 w, 45 mg/kg/day at 34 w, 60 mg/kg/day in term n Intravenous: 20 mg/kg loading dose, followed by a 10 mg/kg maintenance dose every six hours. 28 to 31 wg, to 12 h | IV action: 5 min. Peak effectiveness: 15 min Oral peak effectiveness: 1 h Enteral and rectal: variable absorption | Mild to moderate pain;reduction in morphine requirements after major surgery | Hardly causes hepatic or renal toxicity in newborns; minor hemodynamic effects have been found following IV; Following neonatal exposure to paracetamol remains limited; possible link with risks for atopy, fertility and neurobehavioral problems |
| Dexmedetomidine | Bolus 0.05–0.2 mg/kg over 15 min followed by maintenance 0.47 ± 0.21 mg/kg/h Therapeutic hypothermia 0.3 mcg/kg/h (range 0.2–0.5 mcg/kg/h) | Half-life: 7.6 h preterm and 3.2 h in term infants | Alternative agent for sedation in mechanical ventilation. Sedation of term neonates during therapeutic hypothermia; no studies in neonates | Hypotension and bradycardia generally self-limiting; reduced dosed withdrawal (weaned by decreasing the infusion by 0.1 mcg/kg/h every 12 to 24 h) |
| Ketamine | Bolus 1–2 mg/kg | Action:1–2 min; short duration:15–30 min. | Short painful procedures; hemodynamically unstable patients; no studies in neonates | Possible Neurotoxicity; no studies of long-term outcome in neonates |
| Drug | Dose | Indications | Comments and Main Side Effects |
|---|---|---|---|
| Acetaminophen | po/pr: 5–10 mg/kg/h IV: 10–15 mg/kg/6 h (<10 kg: 7.5 mg/kg/6 h) <1 year: 7.5 mg/kg | Moderate pain Hyperthermia |
|
| Ibuprofen | po: 5–10 mg/kg/6 h IV: 5–10 mg/kg/6 h | Moderate pain Hyperthermia |
|
| Metamizole | po: 10–15 mg/kg/6–8 h IV: 10–20 mg/kg/6–8 h | Moderate–severe pain Hyperthermia |
|
| Dexketoprofen | po: 0.5–1 mg/kg/8 h IV/im: 10–40 mg/kg/8 h | Moderate–severe pain Anti-inflammatory |
|
| Ketorolac | po: 0.5 mg/kg/6–8 h IV, im: 0.2–1 mg/kg/6–8 h | Moderate–severe pain Anti-inflammatory |
|
| Naproxen | po/pr/im: 5 mg/kg/8–12 h | Mild–moderate pain Anti-inflammatory |
|
| Diclofenac | po: 0.5–1.5 mg/kg/8 h | Mild–moderate pain Spasmolytic |
|
| Tramadol | po/pr/sc: 1–2 mg/kg/4–6 h iv: 1–2 mg/kg/4–6 h | Acute pain |
|
| Meperidine | IV/im/sc: 0.5–2 mg/kg/4–6 h | Acute pain Spasmolytic |
|
| Morphine | po: 0.2–0.5 mg/kg/6–8 h IV/im/sc: 0.1–0.2 mg/kg/4–6 h CII: 10–50 mcg/kg/h | Analgosedation in conventional mechanical ventilation Acute or chronic pain Pulmonary edema |
|
| Fentanyl | IV/sc/sl/in: 1–3 mcg/kg CII: 1–10 mcg/kg/h | Procedural pain Analgosedation in conventional mechanical ventilation Acute or chronic pain Pulmonary edema |
|
| Nitrous oxide | 20–70% with oxygen | Procedural pain Endoscopy and venipunctures | Nausea, vomiting Myocardial dysfunctionNeurodevelopment effects? |
| Age | Mild Pain | Moderate Pain | Severe Pain |
|---|---|---|---|
| <1 year old | Adequate oral tolerance
| Adequate oral tolerance
No oral tolerance
| Intravenous
|
| >1 year old | Adequate oral tolerance
| Adequate oral tolerance
| Intravenous
|
| Drug | Dose | Indications | Adverse Effects |
|---|---|---|---|
| EMLA (lidocaine 2.5%-prilocaine 2.5%). | 0.5 g to 1.0 g applied to the procedural site; anesthesia within 60–90 min | Lumbar puncture, venipuncture, circumcision | Methemoglobinemia |
| Tetracaine gel. | Applied to the procedural site | Intramuscular injection and heel sticks | Transient local erythema |
| Liposomal lidocaine 4% cream (LMX4) | Applied to the procedural site; anesthesia within 30 min | Venipuncture, skin biopsies, lesion removal and electrocautery | No risk of methemoglobinemia |
| Lidocaine | Subcutaneous infiltration; 0.5 mL/kg of 1% or 0.25 mL/kg of 2% | Lumbar puncture, circumcision, percutaneous venous or arterial catheter placement | In neonates, avoid combination with epinephrine (risk of tissue necrosis and tachyarrhythmias) |
| Proparacaine anesthetic eye drops (alcaine) 0.5% | 30 s before eye examination | Retinopathy of prematurity screening | Eye redness |
| Technique | Pediatric Experience | Indications | Guided |
|---|---|---|---|
| Neuroaxial block | Very extensive | Oncological pain, neuropathic pain, complex regional pain, refractive phantom limb | Loss of resistance US, Radioscopy |
| Peripheral nerve block | Extensive | Oncological pain, neuropathic pain, complex regional pain, refractive phantom limb Chronic abdominal wall pain | US Electric stimulation |
| Sympathetic block | Less extensive | Complex regional pain, herpes, visceral pain | US, Radioscopy |
| Major occipital nerve | Less extensive | Occipital neuralgia, post-traumatic headache, migraine | US |
| Fascial blocks: TPA (transversal plane abdomen), rectus fascia, iliac fascia, and ilioinguinal fascia | Less extensive | Abdominal wall pain Post herniorrhaphy neuralgia Cutaneous nerve entrapment syndrome Myofascial pain | US |
| IV block (Bier) | Less extensive | Neuropathic pain, complex regional pain | |
| Chemical neurolysis | Short experience | Oncological pain spasticity | Radioscopy, US |
| Radiofrequency | Short experience | Refractory neuropathic pain, joint pain, oncological pain | |
| Transcutaneous electrical nerve stimulation (TENS); spinal cord, brain | Very extensive Less extensive; very short experience | Neuropathic pain, complex regional pain | Radioscopy, US Radioscopy + surgery |
| Intrathecal baclofen | Extensive | Infantile spastic cerebral palsy, dystonia | Radioscopy, US |
| Intra-articular | Extensive | Juvenile idiopathic rheumatoid arthritis, spondylitis | US |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mencía, S.; Alonso, C.; Pallás-Alonso, C.; López-Herce, J.; Maternal and Child Health and Development Network II (SAMID II). Evaluation and Treatment of Pain in Fetuses, Neonates and Children. Children 2022, 9, 1688. https://doi.org/10.3390/children9111688
Mencía S, Alonso C, Pallás-Alonso C, López-Herce J, Maternal and Child Health and Development Network II (SAMID II). Evaluation and Treatment of Pain in Fetuses, Neonates and Children. Children. 2022; 9(11):1688. https://doi.org/10.3390/children9111688
Chicago/Turabian StyleMencía, Santiago, Clara Alonso, Carmen Pallás-Alonso, Jesús López-Herce, and Maternal and Child Health and Development Network II (SAMID II). 2022. "Evaluation and Treatment of Pain in Fetuses, Neonates and Children" Children 9, no. 11: 1688. https://doi.org/10.3390/children9111688