
Social, Academic and Health Status Impact of Long COVID on Children and Young People: An Observational, Descriptive, and Longitudinal Cohort Study
 , , , , ,
, , , , ,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Legal and Ethical Considerations
2.3. Participants and Setting
2.4. Study Procedures and Data Collection
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Sample
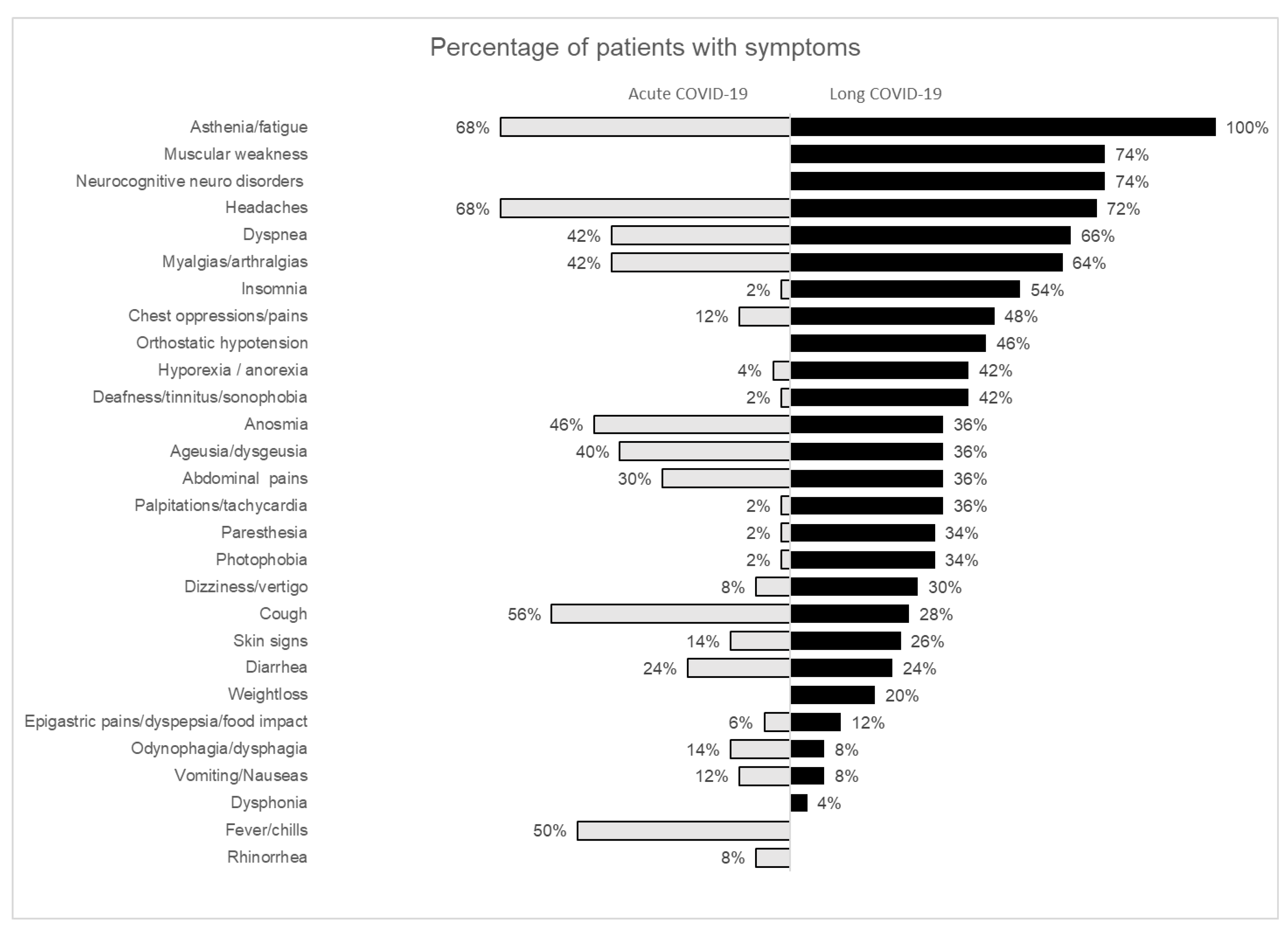
3.2. Clinical Characteristics
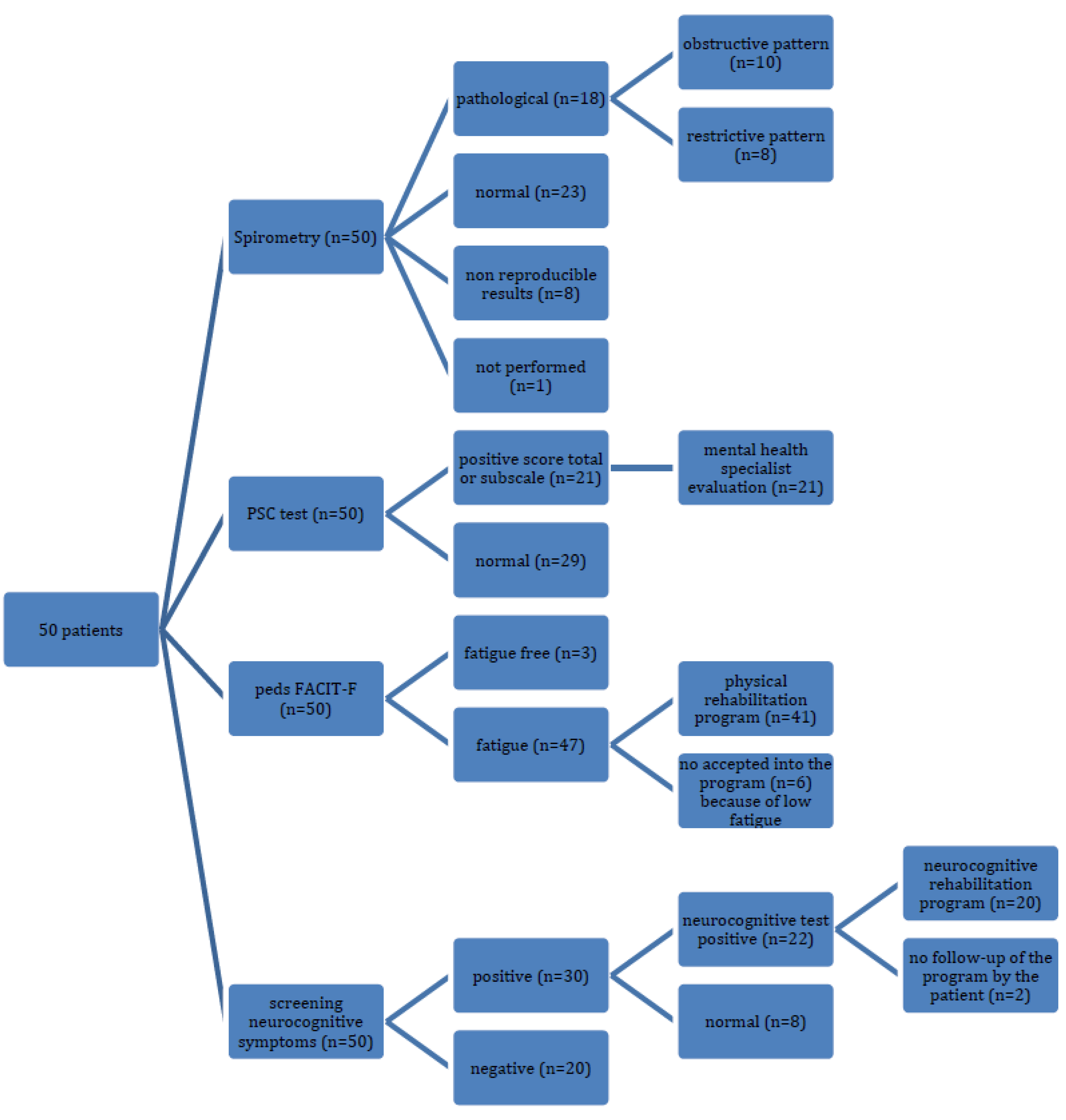
3.3. Abnormal Findings on Tests
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. A Clinical Case Definition of Post-COVID-19 Condition by a Delphi Consensus. 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 6 October 2021).
- National Institute for Health and Care and Excellence. COVID-19 Rapid Guideline: Managing COVID-19 [Internet]. 2022. Available online: https://www.nice.org.uk/guidance/ng191/resources/covid19-rapid-guideline-managing-covid19-pdf-51035553326 (accessed on 7 October 2022).
- Zimmermann, P.; Pittet, L.F.; Curtis, N. How Common is Long COVID in Children and Adolescents? Pediatr. Infect. Dis. J. 2021, 40, e482–e487. [Google Scholar] [CrossRef] [PubMed]
- Roessler, M.; Tesch, F.; Batram, M.; Jacob, J.; Loser, F.; Weidinger, O.; Wende, D.; Vivirito, A.; Toepfner, N.; Seifert, M.; et al. Post COVID-19 in children, adolescents, and adults: Results of a matched cohort study including more than 150,000 individuals with COVID-19. medRxiv 2021, arXiv:10.21.21265133. [Google Scholar]
- Stephenson, T.; Pereira, S.M.P.; Shafran, R.; De Stavola, B.L.; Rojas, N.; McOwat, K.; Simmons, R.; Zavala, M.; O’mahoney, L.; Chalder, T.; et al. Physical and mental health 3 months after SARS-CoV-2 infection (long COVID) among adolescents in England (CLoCk): A national matched cohort study. Lancet Child Adolesc. Health 2022, 6, 230–239. [Google Scholar] [CrossRef]
- Radtke, T.; Ulyte, A.; Puhan, M.A.; Kriemler, S. Long-term symptoms after SARS-CoV-2 infection in school children: Population-based cohort with 6-months follow-up. medRxiv 2021, arXiv:05.16.21257255. [Google Scholar]
- Blankenburg, J.; Wekenborg, M.K.; Reichert, J.; Kirsten, C.; Kahre, E.; Haag, L.; Schuum, L.; Czyborra, P.; Berner, R.; Armann, J.P. Comparison of mental health outcomes in seropositive and seronegative adolescents during the COVID19 pandemic. Sci. Rep. 2022, 12, 2246. [Google Scholar] [CrossRef]
- Molteni, E.; Sudre, C.H.; Canas, L.S.; Bhopal, S.S.; Hughes, R.C.; Antonelli, M.; Murray, B.; Kläser, K.; Kerfoot, E.; Chen, L.; et al. Illness duration and symptom profile in a large cohort of 1 symptomatic UK school-aged children tested for SARS-2 CoV-2. Lancet Child Adolesc. Health 2021, 5, 708–718. [Google Scholar] [CrossRef]
- Osmanov, I.M.; Spiridonova, E.; Bobkova, P.; Gamirova, A.; Shikhaleva, A.; Andreeva, M.; Blyuss, O.; El-Taravi, Y.; DunnGalvin, A.; Comberiati, P.; et al. Risk factors for post-COVID-19 condition in previously hospitalised children using the ISARIC Global follow-up protocol: A prospective cohort study. Eur. Respir. J. 2022, 59, 2101341. [Google Scholar] [CrossRef]
- Buonsenso, D.; Munblit, D.; De Rose, C.; Sinatti, D.; Ricchiuto, A.; Carfi, A.; Valentini, P. Preliminary evidence on long COVID in children. Acta Paediatr. 2021, 110, 2208–2211. [Google Scholar] [CrossRef]
- Miller, F.; Nguyen, V.; Navaratnam, A.M.; Shrotri, M.; Kovar, J.; Hayward, A.C.; Fragaszy, E.; Aldridge, R.W.; Hardelid, P. Prevalence of persistent symptoms in children during the COVID-19 pandemic: Evidence from a household cohort study in England and Wales. medRxiv 2021, arXiv:05.28.21257602. [Google Scholar] [CrossRef]
- Gurdasani, D.; Akrami, A.; Bradley, V.C.; Costello, A.; Greenhalgh, T.; Flaxman, S. Long COVID in children. Lancet Child Adolesc. Health 2022, 6, e2. [Google Scholar] [CrossRef]
- Ashkenazi-Hoffnung, L.; Shmueli, E.; Ehrlich, S.; Ziv, A.; Bar-On, O.; Birk, E.; Lowenthal, A.; Prais, D. Long COVID in Children. Pediatr. Infect. Dis. J. 2021, 40, e509–e511. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Knight, M.; Buxton, M.; Husain, L. Management of post-acute COVID-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, F.M.; Lam, K.; Sounderajah, V.; Clarke, J.M.; Ashrafian, H.; Darzi, A. Characteristics and predictors of acute and chronic post-COVID syndrome: A systematic review and meta-analysis. EClinicalMedicine 2021, 36, 100899. [Google Scholar] [CrossRef]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 Long-term effects of COVID-19: A systematic review and meta-analysis. Sci Rep 2022, 11, 16144. [Google Scholar] [CrossRef] [PubMed]
- Groff, D.; Sun, A.; Ssentongo, A.E.; Ba, D.M.; Parsons, N.; Poudel, G.R.; Lekoubou, A.; Oh, J.S.; Ericson, J.E.; Ssentongo, P.; et al. Short-term and Long-term Rates of Postacute Sequelae of SARS-CoV-2 Infection: A Systematic Review. JAMA Netw. Open 2021, 4, e2128568. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’Em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef] [PubMed]
- López, J.N.; Grasa, C.; Calvo, C.; López-Hortelano, M.G. Long-term symptoms of COVID-19 in children. Acta Paediatr. 2021, 110, 2282–2283. [Google Scholar] [CrossRef] [PubMed]
- Crook, H.; Raza, S.; Nowell, J.; Young, M.; Edison, P. Long COVID—Mechanisms, risk factors, and management. BMJ 2021, 374, n1648. [Google Scholar] [CrossRef]
- Goh, D.; Lim, J.C.T.; Ferna´ındez, S.B.; Joseph, C.R.; Edwards, S.G.; Neo, Z.W.; Lee, J.N.; Caballero, S.G.; Lau, M.C.; Yeong, J.P.S. Case report: Persistence of residual antigen and RNA of the SARS-CoV-2 virus in tissues of two patients with long COVID. Front. Immunol. 2022, 13, 939989. [Google Scholar] [CrossRef]
- Nath, A. Long-Haul COVID. Neurology 2020, 95, 559–560. [Google Scholar] [CrossRef] [PubMed]
- Baig, A.M. Deleterious Outcomes in Long-Hauler COVID-19: The Effects of SARS-CoV-2 on the CNS in Chronic COVID Syndrome. ACS Chem. Neurosci. 2020, 11, 4017–4020. [Google Scholar] [CrossRef] [PubMed]
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef]
- Dani, M.; Dirksen, A.; Taraborrelli, P.; Torocastro, M.; Panagopoulos, D.; Sutton, R.; Lim, P.B. Autonomic dysfunction in ‘long COVID’: Rationale, physiology and management strategies. Clin. Med. 2021, 21, e63–e67. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Yuan, D.; Chen, D.G.; Ng, R.H.; Wang, K.; Choi, J.; Li, S.; Hong, S.; Zhang, R.; Xie, J.; et al. Multiple early factors anticipate post-acute COVID-19 sequelae. Cell 2022, 185, 881–895.e20. [Google Scholar] [CrossRef]
- Paterson, R.W.; Brown, R.L.; Benjamin, L.; Nortley, R.; Wiethoff, S.; Bharucha, T.; Jayaseelan, D.L.; Kumar, G.; Raftopoulos, R.E.; Zambreanu, L.; et al. The emerging spectrum of COVID-19 neurology: Clinical, radiological and laboratory findings. Brain 2020, 143, 3104–3120. [Google Scholar]
- Buonsenso, D.; Pujol, F.E.; Munblit, D.; Pata, D.; McFarland, S.; Simpson, F.K. Clinical characteristics, activity levels and mental health problems in children with long coronavirus disease: A survey of 510 children. Futur. Microbiol. 2022, 17, 577–588. [Google Scholar]
- Izquierdo-Pujol, J.; Moron-Lopez, S.; Dalmau, J.; Gonzalez-Aumatell, A.; Carreras-Abad, C.; Mendez, M.; Rodrigo, C.; Martinez-Picado, J. Post COVID-19 Condition in Children and Adolescents: An Emerging Problem. Front. Pediatr. 2022, 10, 607. [Google Scholar]
- Serra, J.D.; Franch, M.A.; López, L.G.; Costa, C.M.; Salinas, C.S. Childhood obesity. Recommendations of the Nutrition Committee of the Spanish Association of Pediatrics. Part II. Diagnosis. Comorbidities. Treatment. An. De Pediatría 2007, 66, 294–304. [Google Scholar] [CrossRef]
- Lai, J.S.; Cella, D.; Kupst, M.J.; Holm, S.; Kelly, M.E.; Bode, R.K.; Goldman, S. Measuring Fatigue for Children With Cancer: Development and Validation of the Pediatric Functional Assessment of Chronic Illness Therapy-Fatigue (pedsFACIT-F). J. Pediatr. Hematol. Oncol. 2007, 29, 471–479. [Google Scholar]
- Jellinek, M.S.; Murphy, J.M.; Little, M.; Pagano, M.E.; Comer, D.M.; Kelleher, K.J. Use of the pediatric symptom checklist to screen for psychosocial problems in pediatric primary care: A national feasibility study. Arch. Pediatr. Adolesc. Med. 1999, 153, 254–260. [Google Scholar] [CrossRef] [Green Version]
- Whitney, S.L.; Wrisley, D.M.; Marchetti, G.F.; Gee, M.A.; Redfern, M.S.; Furman, J.M. Clinical Measurement of Sit-to-Stand Performance in People With Balance Disorders: Validity of Data for the Five-Times-Sit-to-Stand Test. Phys. Ther. 2005, 85, 1035–1045. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.H.; Liao, H.F.; Peng, Y.C. Reliability and validity of the five-repetition sit-to-stand test for children with cerebral palsy. Clin. Rehabil. 2012, 26, 664–671. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS Statement: Guidelines for the Six-Minute Walk Test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Serrano, M.M.; Collazos, J.R.; Romero, S.M.; Santurino, M.M.; Armesilla, M.C.; Del Cerro, J.P.; de Espinosa, M.G.M. Handgrip strength in children and teenagers aged from 6 to 18 years: Reference values and relationship with size and body composition. An. De Pediatr. 2009, 70, 340–348. [Google Scholar]
- Gąsior, J.S.; Pawłowski, M.; Jeleń, P.J.; Rameckers, E.A.; Williams, C.A.; Makuch, R.; Werner, B. Test–retest reliability of handgrip strength measurement in children and preadolescents. Int. J. Environ. Res. Public Health 2020, 17, 8026. [Google Scholar] [CrossRef]
- García-Molina, A.; Espiña-Bou, M.; Rodríguez-Rajo, P.; Sánchez-Carrión, R.; Enseñat-Cantallops, A. Programa de rehabilitación neuropsicológica en pacientes con síndrome post-COVID-19: Una experiencia clínica. Neurología 2021, 36, 548–576. [Google Scholar] [CrossRef]
- National Institutes of Health. Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19). Nih [Internet]. 2021, 2019, 1–243. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 17 October 2022).
- de Bont, J.; Bennett, M.; León-Muñoz, L.M.; Duarte-Salles, T. The prevalence and incidence rate of overweight and obesity among 2.5 million children and adolescents in Spain. Rev. Española De Cardiol. 2022, 75, 300–307. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F. Persistent symptoms in patients after acute COVID-19. JAMA J. Am. Med. Assoc. 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Pazukhina, E.; Andreeva, M.; Spiridonova, E.; Bobkova, P.; Shikhaleva, A.; El-Taravi, Y.; Rumyantsev, M.; Gamirova, A.; Bairashevskaia, A.; Petrova, P.; et al. Prevalence and risk factors of post-COVID-19 condition in adults and children at 6 and 12 months after hospital discharge: A prospective, cohort study in Moscow (StopCOVID). BMC Med. 2022, 20, 244. [Google Scholar] [CrossRef] [PubMed]
- Jirout, J.; LoCasale-Crouch, J.; Turnbull, K.; Gu, Y.; Cubides, M. How lifestyle factors affect cognitive and executive function and the ability to learn in children. Nutrients 2019, 11, 1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bidzan-Bluma, I.; Lipowska, M. Physical Activity and Cognitive Functioning of Children: A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 800. [Google Scholar] [CrossRef]
- Suris, J.C.; Michaud, P.A.; Viner, R. The adolescent with a chronic condition. Part I: Developmental issues. Arch. Dis. Child. 2004, 89, 938–942. [Google Scholar] [PubMed]
- Michaud, P.A.; Suris, J.C.; Viner, R. The adolescent with a chronic condition. Part II: Healthcare provision. Arch. Dis. Child. 2004, 89, 943–949. [Google Scholar] [CrossRef] [Green Version]
- Buonsenso, D.; Di Giuda, D.; Sigfrid, L.; Pizzuto, D.A.; Di Sante, G.; De Rose, C.; Lazzareschi, I.; Sali, M.; Baldi, F.; Chieffo, D.P.R.; et al. Evidence of lung perfusion defects and ongoing inflammation in an adolescent with post-acute sequelae of SARS-CoV-2 infection. Lancet Child Adolesc. Health 2021, 5, 677–680. [Google Scholar] [CrossRef]
- Grist, J.T.; Collier, G.J.; Walters, H.; Kim, M.; Chen, M.; Abu Eid, G.; Laws, A.; Matthews, V.; Jacob, K.; Cross, S.; et al. Lung Abnormalities Depicted with Hyperpolarized Xenon MRI in Patients with Long COVID. Radiology 2022, 220069. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Age, median (IQR) | 14.1 (12.2–15.8) |
| Age at evaluation > 5 and ≤11 years, n (%) | 6 (12) |
| Age > 12 and ≤15 years | 32 (64) |
| Age > 16 and ≤18 years | 12 (24) |
| Female sex, n (%) | 33 (66) |
| Background medical conditions before COVID-19 infection, n (%) | |
| Chronic urticaria | 1 (2) |
| Allergic rhinitis | 3 (6) |
| Atopic dermatitis | 12 (24) |
| Recurrent headache | 6 (12) |
| Attention deficit hyperactivity disorder | 4 (8) |
| Asthma | 3 (6) |
| Others a | 2 (4) |
| Family background, n (%) | |
| Long COVID | 17 (34) |
| Autoimmune diseases | 11 (22) |
| Fibromyalgia | 4 (8) |
| Acute COVID-19 characteristics | |
| Positive diagnostic tests for SARS-CoV-2, n (%) | |
| RT-qPCR | 26 (52) |
| Rapid antigen detection tests | 6 (12) |
| Serological tests b | 30 (60) |
| Cellular immunity c | 6 (12) |
| No microbiological/immunological confirmation d | 6 (12) |
| Acute COVID-19 symptoms, n (%) | |
| None | 1 (2) |
| 1 or 2 | 3 (6) |
| ≥3 | 46 (92) |
| Number of acute symptoms, median (IQR) | 6 (4–8) |
| Days of duration of acute symptoms, median (IQR) | 10 (4.8–20.3) |
| Hospitalization during the acute illness, n (%) | 1 (2) |
| Long COVID follow-up characteristics | |
| Time since acute phase of COVID-19, n (%) | |
| <6 months | 32 (64) |
| 6–12 months | 15 (30) |
| >12 months | 3 (6) |
| Patients with symptom-free intervals, n (%) | 8 (16) |
| Days of symptom-free time, median (IQR) | 60 (15–118.8) |
| Cause of worsening symptoms, n (%) | |
| Physical or mental overexertion | 32 (64) |
| Intercurrent episode e | 3 (6) |
| Post-acute COVID-19 symptoms, n (%) | |
| ≥3 | 50 (100) |
| Number of symptoms, median (IQR) | 10 (7–16) |
| Functional Assessment of Chronic Illness Therapy (pedsFACIT-F), n (%) | |
| Fatigue-free (45–52 score) | 3 (6) |
| Low degree of fatigue (31–44 score) | 13 (26) |
| Moderate degree of fatigue (21–30 score) | 16 (33) |
| High degree of fatigue (0–20 score) | 18 (37) |
| Assessment of Mental Health Pediatric Symptom Checklist (PSC), n (%) | |
| ≥30 scores in the total PSC | 15 (30) |
| ≥7 scores in the attention subscale | 6 (12) |
| ≥5 scores in the anxiety/depression subscale | 19 (38) |
| ≥7 scores in the conduct subscale | 2 (4) |
| Effect of long COVID on school performance and extracurricular activities, n (%) | |
| Not able to attend to regular school schedule like before the infection | 17 (34) |
| School dropout | 9 (18) |
| Decreased school performance | 33 (66) |
| Stopped sport activities | 36 (72) |
| Stopped extracurricular activities | 34 (68) |
| Medical evaluation, n (%) | |
| Positive findings on neurological physical examination f | 6 (12) |
| BMI g percentile by growth charts > 85% | 2 (4) |
| BMI percentile by growth charts > 97% | 8 (16) |
| Positive findings on laboratory investigation h, n (%) | |
| Vitamin D < 20 ng/mL | 17 (34) |
| Folic acid < 5.3 ng/mL | 16 (32) |
| Pulmonary evaluation, n (%) | |
| Chest radiograph changes (Finding: infiltrate) | 1 (2) |
| Cardiac evaluation, n (%) | |
| Abnormal findings on electrocardiograph | 0 (0) |
| Physical Rehabilitation Program (n = 41) | |
|---|---|
| Five-Times-Sit-to-Stand Test (XSST) | |
| Normal strength (<11.2 s), n (%) | 25 (61.0) |
| Slight decrease in strength (11.2–13.7 s), n (%) | 7 (17.1) |
| Moderate decrease in strength (13.7–16.7 s), n (%) | 4 (9.8) |
| Severe decrease in strength (>16.7 s), n (%) | 5 (12.1) |
| Very severe decrease in strength (>60 s), n (%) | 0 (0) |
| Handgrip strength by Dynamometer | |
| Decreased strength in dominant hand (Pc < 80%), n (%) | 13 (31.7) |
| Decreased strength in non-dominant hand (Pc < 80%), n (%) | 16 (39.0) |
| 6-Minute Walking Test (6-MWT) | |
| 6-MWD meters, median [IQR] | 480 [418–550] |
| Dyspnea basal score, median [IQR] | 0 [0–0.5] |
| Dyspnea final score, median [IQR] | 3 [2–6] |
| Dyspnea perception after the 6-MWT, n (%) | 33 (80.5) |
| Fatigue basal score, median [IQR] | 0 [0–3] |
| Fatigue final score, median [IQR] | 3 [3–7] |
| Basal HR, bpm, median [IQR] | 81 [73–91] |
| Final HR, bpm, median [IQR] | 111 [87–127] |
| Basal SpO2 %, median [IQR] | 99 [98–99] |
| Final SpO2 %, median [IQR] | 98 [97–99] |
| SpO2 in 6-MWT < 95%, n (%) | 1 (2.4) |
| Lowest SpO2, % | 93 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonzalez-Aumatell, A.; Bovo, M.V.; Carreras-Abad, C.; Cuso-Perez, S.; Domènech Marsal, È.; Coll-Fernández, R.; Goicoechea Calvo, A.; Giralt-López, M.; Enseñat Cantallops, A.; Moron-Lopez, S.; et al. Social, Academic and Health Status Impact of Long COVID on Children and Young People: An Observational, Descriptive, and Longitudinal Cohort Study. Children 2022, 9, 1677. https://doi.org/10.3390/children9111677
Gonzalez-Aumatell A, Bovo MV, Carreras-Abad C, Cuso-Perez S, Domènech Marsal È, Coll-Fernández R, Goicoechea Calvo A, Giralt-López M, Enseñat Cantallops A, Moron-Lopez S, et al. Social, Academic and Health Status Impact of Long COVID on Children and Young People: An Observational, Descriptive, and Longitudinal Cohort Study. Children. 2022; 9(11):1677. https://doi.org/10.3390/children9111677
Chicago/Turabian StyleGonzalez-Aumatell, Alba, Maria Victoria Bovo, Clara Carreras-Abad, Sara Cuso-Perez, Èlia Domènech Marsal, Roser Coll-Fernández, Aroia Goicoechea Calvo, Maria Giralt-López, Antonia Enseñat Cantallops, Sara Moron-Lopez, and et al. 2022. "Social, Academic and Health Status Impact of Long COVID on Children and Young People: An Observational, Descriptive, and Longitudinal Cohort Study" Children 9, no. 11: 1677. https://doi.org/10.3390/children9111677