
Factors Associated with an Increase in On-Site Time of Pediatric Trauma Patients in a Prehospital Setting: A Nationwide Observational Study in Japan
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Japan Trauma Data Bank
2.2. Study Setting and Emergency Medical Service System in Japan
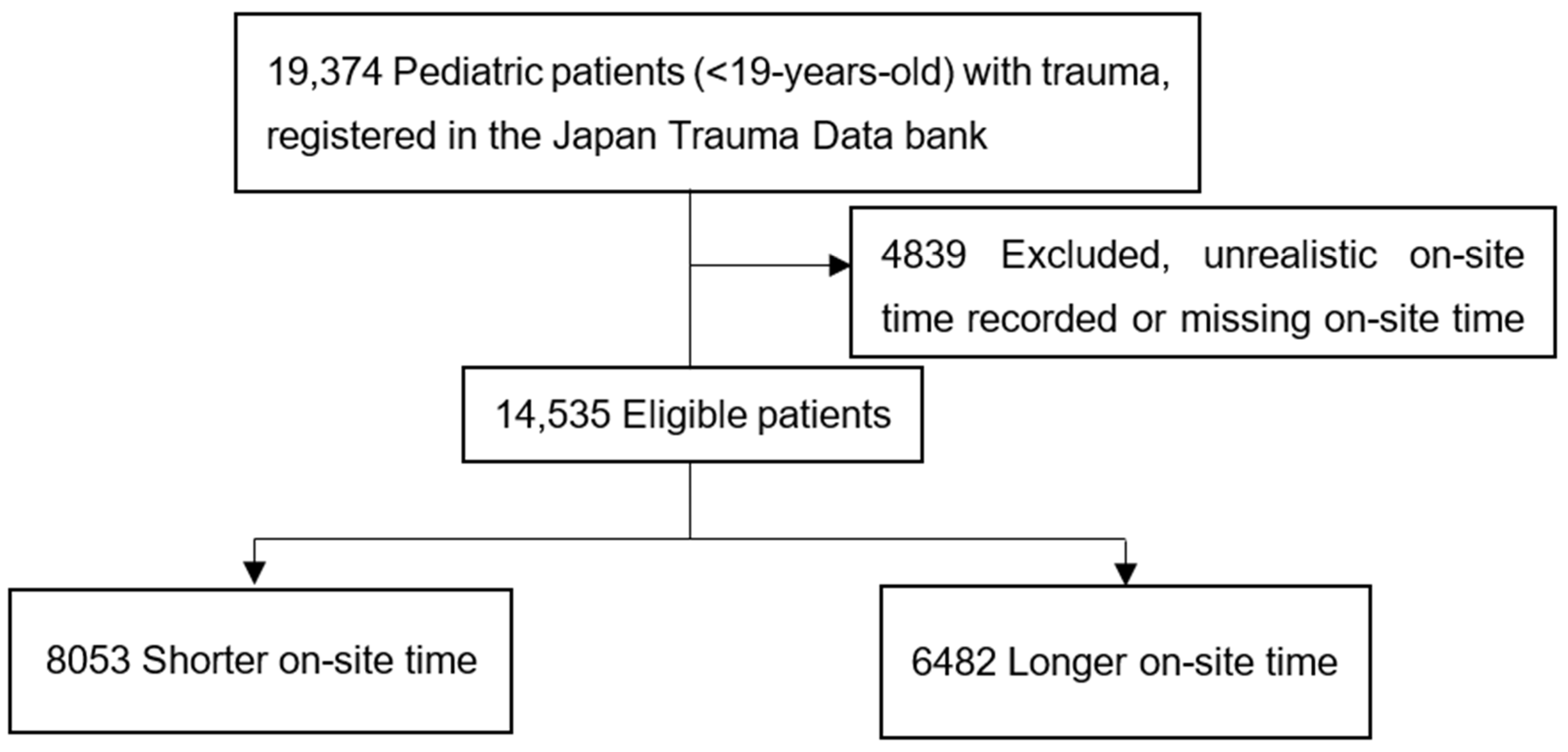
2.3. Patient Selection
2.4. Outcomes
2.5. Variables
2.6. Statistical Analysis
2.7. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sampalis, J.S.; Lavoie, A.; Williams, J.I.; Mulder, D.S.; Kalina, M. Impact of on-site care; prehospital time; and level of in-hospital care on survival in severely injured patients. J. Trauma 1993, 34, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Feero, S.; Hedges, J.R.; Simmons, E.; Irwin, L. Does out-of-hospital EMS time affect trauma survival? Am. J. Emerg. Med. 1995, 13, 133–135. [Google Scholar] [CrossRef]
- Gonzalez, R.P.; Cummings, G.R.; Phelan, H.A.; Mulekar, M.S.; Rodning, C.B. Does increased emergency medical services prehospital time affect patient mortality in rural motor vehicle crashes? A statewide analysis. Am. J. Surg. 2009, 197, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Tien, H.C.N.; Jung, V.; Pinto, R.; Mainprize, T.; Scales, D.C.; Rizoli, S.B. Reducing time-to-treatment decreases mortality of trauma patients with acute subdural hematoma. Ann. Surg. 2011, 253, 1178–1183. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.M.; Gao, Y.H.; Zeng, J.B.; Wang, J.B.; He, P.; Wei, G.B.; Xiang, Z. Polytrauma with thoracic and/or abdominal injuries: Experience in 1540 cases. Chin. J. Traumatol. 2006, 9, 108–114. [Google Scholar]
- Tomazin, I.; Vegnuti, M.; Ellerton, J.; Reisten, O.; Sumann, G.; Kersnik, J. Factors impacting on the activation and approach times of helicopter emergency medical services in four Alpine countries. Scand. J. Trauma Resusc. Emerg. Med. 2012, 20, 56. [Google Scholar] [CrossRef] [Green Version]
- Maeyama, H.; Naito, H.; Guyette, F.X.; Yorifuji, T.; Banshotani, Y.; Matsui, D.; Yumoto, T.; Nakao, A.; Kobayashi, M. Intubation during a medevac flight: Safety and effect on total prehospital time in the helicopter emergency medical service system. Scand. J. Trauma Resusc. Emerg. Med. 2020, 28, 89. [Google Scholar] [CrossRef]
- Smith, R.M.; Conn, A.K.T. Prehospital care–scoop and run or stay and play? Injury 2009, 40 (Suppl. 4), S23–S26. [Google Scholar] [CrossRef]
- Kidher, E.; Krasopoulos, G.; Coats, T.; Charitou, A.; Magee, P.; Uppal, R.; Athanasiou, T. The effect of prehospital time related variables on mortality following severe thoracic trauma. Injury 2012, 43, 1386–1392. [Google Scholar] [CrossRef]
- Katayama, Y.; Kitamura, T.; Kiyohara, K.; Iwami, T.; Kawamura, T.; Hayashida, S.; Ogura, H.; Shimazu, T. Evaluation of factors associated with the difficulty in finding receiving hospitals for traffic accident patients at the scene treated by emergency medical services: A population-based study in Osaka City; Japan. Acute Med. Surg. 2017, 4, 401–407. [Google Scholar] [CrossRef]
- Hosomi, S.; Kitamura, T.; Sobue, T.; Nakagawa, Y.; Ogura, H.; Shimazu, T. Association of pre-hospital helicopter transport with reduced mortality in traumatic brain injury in japan: A nationwide retrospective cohort study. J. Neurotrauma 2022, 39, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Nakao, S.; Katayama, Y.; Hirayama, A.; Hirose, T.; Ishida, K.; Umemura, Y.; Tachino, J.; Kiguchi, T.l.; Matsuyama, T.; Kiyohara, K.; et al. Characteristics and outcomes of pediatric blunt renal trauma: A nationwide cohort study in Japan. Eur. J. Trauma Emerg. Surg. 2022, 48, 2047–2057. [Google Scholar] [CrossRef] [PubMed]
- Kondo, Y.; Miyazato, A.; Okamoto, K.; Tanaka, H. Impact of sex differences on mortality in patients with sepsis after trauma: A nationwide cohort study. Front. Immunol. 2021, 12, 678156. [Google Scholar] [CrossRef] [PubMed]
- Tohira, H.; Jacobs, I.; Mountain, D.; Gibson, N.; Yeo, A. International comparison of regional trauma registries. Injury 2012, 43, 1924–1930. [Google Scholar] [CrossRef]
- Japan Trauma Data Bank Homepage. Available online: https://jtcr-jatec.org/traumabank/index.htm (accessed on 1 October 2022).
- Katayama, Y.; Kitamura, T.; Kiyohara, K.; Ishida, K.; Hirose, T.; Nakao, S.; Tachino, J.; Matsuyama, T.; Kiguchi, T.; Umemura, Y.; et al. Effect of fluid administration on scene to traffic accident patients by EMS personnel: A propensity score-matched study using population-based ambulance records and nationwide trauma registry in Japan. Eur. J. Trauma Emerg. Surg. 2022, 48, 999–1007. [Google Scholar] [CrossRef]
- Alvarez, B.D.; Razente, D.M.; Lacerda, D.A.M.; Lother, N.S.; VON-Bahten, L.C.; Stahlschmidt, C.M.M. Analysis of the Revised Trauma Score (RTS) in 200 victims of different trauma mechanisms. Rev. Col. Bras. Cir. 2016, 43, 334–340. [Google Scholar] [CrossRef] [Green Version]
- Champion, H.R.; Sacco, W.J.; Copes, W.S.; Gann, D.S.; Gennarelli, T.A.; Flanagan, M.E. A revision of the Trauma Score. J. Trauma 1989, 29, 623–629. [Google Scholar] [CrossRef]
- Parreira, J.G.; Martins, R.K.; Slongo, J.; Perlingeiro, J.A.G.; Soldá, S.C.; Assef, J.C. Comparative analysis of the frequency and the severity of diagnosed lesions between pedestrians struck by motor vehicles and other blunt trauma mechanisms victims. Rev. Col. Bras. Cir. 2015, 42, 253–258. [Google Scholar] [CrossRef] [Green Version]
- Giudici, R.; Lancioni, A.; Gay, H.; Bassi, G.; Chiara, O.; Mare, C.; Latronico, N.; Pesenti, A.; Faccincani, R.; Cabrini, L.; et al. Impact of the COVID-19 outbreak on severe trauma trends and healthcare system reassessment in Lombardia, Italy: An analysis from the regional trauma registry. World J. Emerg. Surg. 2021, 16, 39. [Google Scholar] [CrossRef]
- Mukonkole, S.N.; Hunter, L.; Möller, A.; McCaul, M.; Lahri, S.; Van Hoving, D.J. A comparison of trauma scoring systems for injuries presenting to a district-level urban public hospital in Western Cape. S. Afr. J. Surg. 2020, 58, 37–42. [Google Scholar] [CrossRef]
- Boyd, C.R.; Tolson, M.A.; Copes, W.S. Evaluating trauma care: The TRISS method. Trauma Score and the Injury Severity Score. J. Trauma 1987, 27, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Hirose, T.; Kitamura, T.; Katayama, Y.; Sado, J.; Kiguchi, T.; Matsuyama, T.; Kiyohara, K.; Takahashi, H.; Tachino, J.; Nakagawa, Y.; et al. Impact of nighttime and weekends on outcomes of emergency trauma patients. Medicine 2020, 99, e18687. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, M.; Muguruma, T.; Toida, C.; Gakumazawa, M.; Abe, T.; Takeuchi, I. Daytime admission is associated with higher 1-month survival for pediatric out-of-hospital cardiac arrest: Analysis of a nationwide multicenter observational study in Japan. PLoS ONE 2021, 16, e0246896. [Google Scholar] [CrossRef] [PubMed]
- Shigematsu, K.; Nakano, H.; Watanabe, Y. The eye response test alone is sufficient to predict stroke outcome—reintroduction of Japan Coma Scale: A cohort study. BMJ Open 2013, 3, e002736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohta, T.; Waga, S.; Handa, W.; Saito, I.; Takeuchi, K. New grading of level of disordered consciousness (author’s translation). No Shinkei Geka 1974, 2, 623–627. [Google Scholar]
- Ono, K.; Wada, K.; Takahara, T.; Shirotani, T. Indications for computed tomography in patients with mild head injury. Neurol. Med. Chir. 2007, 47, 291–298. [Google Scholar] [CrossRef] [Green Version]
- Maitland, K.; Kiguli, S.; Opoka, R.O.; Engoru, C.; Olupot-Olupot, P.; Akech, S.O.; Nyeko, R.; Mtove, G.; Reyburn, H.; Lang, T.; et al. Mortality after fluid bolus in African children with severe infection. N. Engl. J. Med. 2011, 364, 2483–2495. [Google Scholar] [CrossRef] [Green Version]
- Newgard, C.D.; Lin, A.; Goldhaber-Fiebert, J.D.; Marin, J.R.; Smith, M.; Cook, J.; Mohr, N.M.; Zonfrillo, M.R.; Puapong, D.; Papa, L.; et al. Association of emergency department pediatric readiness with mortality to 1 year among injured children treated at trauma centers. JAMA Surg. 2022, 157, e217419. [Google Scholar] [CrossRef]
- Naito, H.; Yumoto, T.; Yorifuji, T.; Nojima, T.; Yamamoto, H.; Yamada, T.; Tsukahara, K.; Inaba, M.; Nishimura, T.; Uehara, T.; et al. Association between emergency medical service transport time and survival in patients with traumatic cardiac arrest: A nationwide retrospective observational study. BMC Emerg. Med. 2021, 21, 104. [Google Scholar] [CrossRef]
- Endo, A.; Shiraishi, A.; Fushimi, K.; Murata, K.; Otomo, Y. Increased severe trauma patient volume is associated with survival benefit and reduced total health care costs: A retrospective observational study using a Japanese nationwide administrative database. Ann. Surg. 2018, 268, 1091–1096. [Google Scholar] [CrossRef]
- Gallaher, J.; Yohann, A.; Schneider, A.B.; Raff, L.; Reid, T.; Charles, A. The use of head computerized tomography in patients with GCS 15 following trauma: Less is more. Injury 2022, 53, 1645–1651. [Google Scholar] [CrossRef] [PubMed]
- Morita, K. Introduction to multiple imputation. Ann. Clin. Epidemiol. 2021, 3, 1–4. [Google Scholar] [CrossRef]
- Rubin, D.B.; Schenker, N. Multiple imputation in health-care databases: An overview and some applications. Stat. Med. 1991, 10, 585–598. [Google Scholar] [CrossRef] [PubMed]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.B. Multiple imputation after 18+ years. J. Am. Stat. Assoc. 1996, 91, 473–489. [Google Scholar] [CrossRef]
- Fire and Disaster Management Agency Homepge. Available online: https://www.fdma.go.jp/ (accessed on 1 October 2022).
- Bennett, C.L.; Espinola, J.A.; Sullivan, A.F.; Boggs, K.M.; Clay, C.E.; Lee, M.O.; Samuels-Kalow, M.E.; Camargo, C.A., Jr. Evaluation of the 2020 pediatric emergency physician workforce in the US. JAMA Netw. Open 2021, 4, e2110084. [Google Scholar] [CrossRef]
- Ministry of Health. Labour and Welfare Homepage. Summary of Statistics on Physicians; Dentists; and Pharmacists in 2020 (Author’s Translation). Available online: https://www.mhlw.go.jp/toukei/saikin/hw/ishi/20/index.html (accessed on 1 October 2022).
- Bennett, C.L.; Sullivan, A.F.; Ginde, A.A.; Rogers, J.; Espinola, J.A.; Clay, C.E.; Camargo, C.A., Jr. National Study of the Emergency Physician Workforce; 2020. Ann. Emerg. Med. 2020, 76, 695–708. [Google Scholar] [CrossRef]
- The American Board of Pediatrics Homepage. 2020–2021 Pediatric Physicians Workforce Data Book. Available online: https://www.abp.org/content/recent-publications-annual-workforce-data-book-and-archived-data (accessed on 1 October 2022).
- Japan Medical Specialties Organization. Outline of the Japanese Medical Specialty System Medical Care (Author’s Translation). Available online: https://jmsb.or.jp/wp-content/uploads/2020/01/gaiho_2019.pdf (accessed on 1 October 2022).
- Clement, R.C.; Carr, B.G.; Kallan, M.J.; Reilly, P.M.; Mehta, S. Who needs an orthopedic trauma surgeon? An analysis of US national injury patterns. J. Trauma Acute Care Surg. 2013, 75, 687–692. [Google Scholar] [CrossRef]
- Sanders, C.L.; Barfield, W.R.; Simpson, K.N.; Colhoun, D.; Hartsock, L.A. The Effect of initiation of an orthopedic trauma service on patient outcomes and clinical enterprise financial performance. Duke Orthop. J. 2020, 10, 26–31. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total (n = 14,535) | |
|---|---|---|
| Age: years, median (IQR) | 13 | (7–17) |
| Age groups: years, n (%) | ||
| 0 | 308 | (2.1) |
| 1–3 | 1241 | (8.5) |
| 4–6 | 1434 | (9.7) |
| 7–12 | 3859 | (26.6) |
| 13–18 | 7693 | (52.9) |
| Sex, n (%) | ||
| Male | 10,485 | (72.1) |
| Female | 4046 | (27.8) |
| Missing | 4 | (<0.1) |
| Year, n (%) | ||
| 2004–2007 | 1148 | (7.9) |
| 2008–2010 | 1856 | (12.8) |
| 2011–2013 | 3599 | (24.8) |
| 2014–2016 | 4926 | (33.9) |
| 2017–2019 | 2978 | (20.5) |
| Missing | 28 | (0.2) |
| Month, n (%) | ||
| January–March | 2772 | (19.1) |
| April–June | 4167 | (28.7) |
| July–September | 4125 | (28.4) |
| October–December | 3443 | (23.7) |
| Missing | 28 | (0.2) |
| Days of week, n (%) | ||
| Weekdays | 9316 | (64.1) |
| Weekends/Holidays | 5218 | (35.9) |
| Missing | 1 | (<0.1) |
| Time, n (%) | ||
| Daytime | 6206 | (42.7) |
| Nighttime | 8239 | (56.7) |
| Missing | 90 | (0.6) |
| Type of trauma, n (%) | ||
| Traffic accident | 8934 | (61.5) |
| Fall | 3575 | (24.6) |
| Other blunt trauma | 1717 | (11.8) |
| Penetrating trauma | 192 | (1.3) |
| Missing | 117 | (0.8) |
| Cause of trauma, n (%) | ||
| Accident | 13,388 | (92.1) |
| Occupational injury | 83 | (0.6) |
| Suicide | 637 | (4.4) |
| Violence | 191 | (1.3) |
| Others | 78 | (0.5) |
| Unknown/Missing | 158 | (1.1) |
| Prehospital vital signs | ||
| Japan coma scale, n (%) | ||
| 0 | 6821 | (46.9) |
| 1–3 | 3766 | (25.9) |
| 10–30 | 1286 | (8.9) |
| 100–300 | 1873 | (12.9) |
| Unknown/Missing | 789 | (5.4) |
| Pulse rate: bpm, median (IQR) | 95 | (80–110) |
| Missing, n (%) | 1046 | (7.2) |
| Systolic blood pressure: mmHg, median (IQR) | 121 | (110–135) |
| Hypotension | 77 | (0.5) |
| Missing, n (%) | 2437 | (16.8) |
| Respiratory rate, median (IQR) | 24 | (20–30) |
| Missing, n (%) | 2136 | (14.7) |
| Cardiopulmonary arrest | 441 | (3.0) |
| Severity of trauma | ||
| RTS, median (IQR) | 7.84 | (7.55–7.84) |
| Missing, n (%) | 2265 | (15.6) |
| AIS | ||
| AIS1 ≥ 3, n (%) | 4552 | (31.3) |
| AIS2 ≥ 3, n (%) | 127 | (0.9) |
| AIS3 ≥ 3, n (%) | 31 | (0.2) |
| AIS4 ≥ 3, n (%) | 2721 | (18.7) |
| AIS5 ≥ 3, n (%) | 742 | (5.1) |
| AIS6 ≥ 3, n (%) | 557 | (3.8) |
| AIS7 ≥ 3, n (%) | 1109 | (7.6) |
| AIS8 ≥ 3, n (%) | 2331 | (16.0) |
| AIS9 ≥ 3, n (%) | 10 | (0.1) |
| ISS, median (IQR) | 10 | (5–17) |
| ISS > 15 | 4692 | (32.3) |
| ISS < 16 | 8737 | (60.1) |
| Missing, n (%) | 1106 | (7.6) |
| TRISS, median (IQR) | 0.99 | (0.98–1.00) |
| Missing, n (%) | 3333 | (22.9) |
| Interventions before hospital arrival | ||
| Oxygen | 6933 | (47.7) |
| Immobilization | 8740 | (60.1) |
| Chest compression | 378 | (2.6) |
| Intravenous line placement | 156 | (1.1) |
| Defibrillation | 18 | (0.1) |
| Intubation | 67 | (0.5) |
| Missing | 826 | (5.7) |
| Comorbidities | ||
| Mental disease | 272 | (1.9) |
| Mental retardation | 149 | (1.0) |
| Physical disease | 44 | (0.3) |
| On-site time, median (IQR) | 13 | (9–18) |
| Univariate Analysis | |||||
|---|---|---|---|---|---|
| Variables | Shorter On-Site Time (n = 8053) | Longer On-Site Time (n = 6482) | p-Value | ||
| Age: years, median (IQR) | 12 | (7–16) | 14 | (9–17) | <0.001 |
| Age groups: years, n (%) | <0.001 | ||||
| 0 | 213 | (2.6) | 95 | (1.5) | |
| 1–3 | 868 | (10.8) | 373 | (5.8) | |
| 4–6 | 916 | (11.4) | 518 | (8.0) | |
| 7–12 | 2171 | (27.0) | 1688 | (26.0) | |
| 13–18 | 3885 | (48.2) | 3808 | (58.7) | |
| Sex, n (%) | 0.07 | ||||
| Male | 2224 | (27.6) | 1822 | (28.1) | |
| Female | 5829 | (72.4) | 4656 | (71.8) | |
| Missing | 0 | (0.0) | 4 | (0.1) | |
| Year, n (%) | <0.001 | ||||
| 2004–2007 | 740 | (9.2) | 408 | (6.3) | |
| 2008–2010 | 1055 | (13.1) | 801 | (12.4) | |
| 2011–2013 | 2044 | (25.4) | 1555 | (24.0) | |
| 2014–2016 | 2638 | (32.8) | 2288 | (35.3) | |
| 2017–2019 | 1562 | (19.4) | 1416 | (21.8) | |
| Missing | 14 | (0.2) | 14 | (0.2) | |
| Month, n (%) | 0.80 | ||||
| January–March | 1520 | (18.9) | 1252 | (19.3) | |
| April–June | 2336 | (29.0) | 1831 | (28.2) | |
| July–September | 2289 | (28.4) | 1836 | (28.3) | |
| October–December | 1894 | (23.5) | 1549 | (23.9) | |
| Missing | 14 | (0.2) | 14 | (0.2) | |
| Days of week, n (%) | |||||
| Weekdays | 5177 | (64.3) | 4139 | (63.9) | 0.47 |
| Weekends/Holidays | 2876 | (35.7) | 2342 | (36.1) | |
| Missing | 0 | (0.0) | 1 | (<1) | |
| Call time, n (%) | <0.001 | ||||
| Daytime | 3589 | (44.6) | 2617 | (40.4) | |
| Nighttime | 4415 | (54.8) | 3824 | (59.0) | |
| Missing | 49 | (0.6) | 41 | (0.6) | |
| Type of trauma, n (%) | <0.001 | ||||
| Traffic accident | 4756 | (59.1) | 4178 | (64.5) | |
| Fall | 2150 | (26.7) | 1425 | (22.0) | |
| Other blunt trauma | 992 | (12.3) | 725 | (11.2) | |
| Penetrating trauma | 100 | (1.2) | 92 | (1.4) | |
| Missing | 55 | (0.7) | 62 | (1.0) | |
| Cause of trauma, n (%) | 0.22 | ||||
| Accident | 7443 | (92.4) | 5945 | (91.7) | |
| Occupational injury | 38 | (0.5) | 45 | (0.7) | |
| Suicide | 344 | (4.3) | 293 | (4.5) | |
| Violence | 94 | (1.2) | 97 | (1.5) | |
| Others | 44 | (0.5) | 34 | (0.5) | |
| Unknown/Missing | 90 | (1.1) | 68 | (1.0) | |
| Prehospital vital signs | |||||
| Japan Coma Scale, n (%) | <0.001 | ||||
| 0 | 3510 | (43.6) | 3311 | (51.1) | |
| 1–3 | 1900 | (23.6) | 1866 | (28.8) | |
| 10–30 | 777 | (9.6) | 509 | (7.9) | |
| 100–300 | 1430 | (17.8) | 443 | (6.8) | |
| Unknown/missing | 436 | (5.4) | 353 | (5.4) | |
| Pulse rate: bpm, median (IQR) | 96 | (81–113) | 94 | (80–109) | <0.001 |
| Missing, n (%) | 660 | (8.2) | 386 | (6.0) | |
| Systolic blood pressure: mmHg, median (IQR) | 121 | (110–135) | 122 | (110–136) | 0.03 |
| Hypotension | 44 | (0.5) | 33 | (0.5) | <0.001 |
| Missing, n (%) | 1666 | (20.7) | 771 | (11.9) | |
| Respiratory rate, median (IQR) | 24 | (20–30) | 24 | (20–28) | <0.001 |
| Missing, n (%) | 1335 | (16.6) | 801 | (12.4) | |
| Cardiopulmonary arrest | 346 | (4.3) | 95 | (1.5) | <0.001 |
| Severity of trauma | |||||
| RTS, median (IQR) | 7.84 | (6.90–7.84) | 7.841 | (7.55–7.84) | <0.001 |
| Missing, n (%) | 1358 | (16.9) | 907 | (14.0) | |
| AIS | |||||
| AIS1 ≥ 3, n (%) | 2909 | (36.1) | 1643 | (25.3) | <0.001 |
| AIS2 ≥ 3, n (%) | 74 | (0.9) | 53 | (0.8) | 0.51 |
| AIS3 ≥ 3, n (%) | 18 | (0.2) | 13 | (0.2) | 0.77 |
| AIS4 ≥ 3, n (%) | 1657 | (20.6) | 1064 | (16.4) | <0.001 |
| AIS5 ≥ 3, n (%) | 450 | (5.6) | 292 | (4.5) | 0.003 |
| AIS6 ≥ 3, n (%) | 266 | (3.3) | 291 | (4.5) | <0.001 |
| AIS7 ≥ 3, n (%) | 557 | (6.9) | 552 | (8.5) | <0.001 |
| AIS8 ≥ 3, n (%) | 1149 | (14.3) | 1182 | (18.2) | <0.001 |
| AIS9 ≥ 3, n (%) | 8 | (0.1) | 2 | (< 0.1) | 0.12 |
| ISS, median (IQR) | 10 | (5–20) | 9 | (5–16) | <0.001 |
| ISS > 15 | 2929 | (36.4) | 1763 | (27.2) | <0.001 |
| ISS < 16 | 4407 | (54.7) | 4330 | (66.8) | |
| Missing, n (%) | 717 | (8.9) | 389 | (6.0) | |
| TRISS, median (IQR) | 0.965 | (0.870–0.978) | 0.968 | (0.938–0.988) | <0.001 |
| Missing, n (%) | 2045 | (25.5) | 1288 | (19.9) | |
| Interventions before hospital arrival | |||||
| Oxygen | 3970 | (49.3) | 2963 | (45.7) | <0.001 |
| Immobilization | 4715 | (58.5) | 4025 | (62.1) | <0.001 |
| Chest compression | 300 | (3.7) | 78 | (1.2) | <0.001 |
| Intravenous line placement | 87 | (1.1) | 69 | (1.1) | 0.93 |
| Defibrillation | 13 | (0.2) | 5 | (0.1) | 0.15 |
| Intubation | 44 | (0.5) | 23 | (0.4) | 0.10 |
| Missing | 476 | (5.9) | 350 | (5.4) | |
| Comorbidities | |||||
| Mental disease | 140 | (1.7) | 132 | (2.0) | 0.19 |
| Mental retardation | 69 | (0.9) | 80 | (1.2) | 0.03 |
| Physical disease | 24 | (0.3) | 20 | (0.3) | 0.91 |
| On-site time, median (IQR) | 9 | (7–11) | 19 | (16–24) | <0.001 |
| Variables | Odds Ratio | 95% Confidence Interval | p-Value | ||
|---|---|---|---|---|---|
| Age groups: years | |||||
| 0 | Ref | ||||
| 1–3 | 0.78 | 0.59 | to | 1.03 | 0.08 |
| 4–6 | 0.88 | 0.66 | to | 1.16 | 0.35 |
| 7–12 | 1.19 | 0.92 | to | 1.56 | 0.19 |
| 13–18 | 1.53 | 1.17 | to | 1.99 | 0.002 |
| Sex | |||||
| Male | 0.93 | 0.86 | to | 1.01 | 0.07 |
| Year | |||||
| 2004–2007 | Ref | ||||
| 2008–2010 | 1.28 | 1.09 | to | 1.49 | 0.002 |
| 2011–2013 | 1.26 | 1.09 | to | 1.46 | 0.002 |
| 2014–2016 | 1.40 | 1.22 | to | 1.61 | <0.001 |
| 2017–2019 | 1.47 | 1.26 | to | 1.70 | <0.001 |
| Month | |||||
| January–March | Ref | ||||
| April–June | 0.96 | 0.87 | to | 1.06 | 0.47 |
| July–September | 0.97 | 0.88 | to | 1.07 | 0.53 |
| October–December | 1.00 | 0.90 | to | 1.11 | 1.00 |
| Days of week | |||||
| Weekdays | Ref | ||||
| Weekends/Holidays | 1.06 | 0.99 | to | 1.14 | 0.09 |
| Time | |||||
| Daytime | 0.89 | 0.83 | to | 0.96 | 0.002 |
| Type of trauma | |||||
| Traffic accident | Ref | ||||
| Fall | 0.80 | 0.73 | to | 0.88 | <0.001 |
| Other blunt trauma | 0.69 | 0.61 | to | 0.78 | <0.001 |
| Penetrating trauma | 0.90 | 0.66 | to | 1.23 | 0.52 |
| Cause of trauma | |||||
| Accident | Ref | ||||
| Occupational injury | 1.37 | 0.88 | to | 2.14 | 0.17 |
| Suicide | 1.27 | 1.03 | to | 1.57 | 0.03 |
| Violence | 1.74 | 1.27 | to | 2.38 | 0.001 |
| Others | 1.11 | 0.70 | to | 1.76 | 0.67 |
| Prehospital vital signs | |||||
| Hypotension | 1.52 | 0.92 | to | 2.50 | 0.10 |
| Severity of trauma | |||||
| RTS | 1.251 | 1.194 | to | 1.309 | <0.001 |
| AIS | |||||
| AIS1 ≥ 3 | 0.77 | 0.71 | to | 0.84 | <0.001 |
| AIS2 ≥ 3 | 0.97 | 0.67 | to | 1.41 | 0.89 |
| AIS3 ≥ 3 | 1.05 | 0.49 | to | 2.25 | 0.90 |
| AIS4 ≥ 3 | 0.84 | 0.76 | to | 0.92 | <0.001 |
| AIS5 ≥ 3 | 0.84 | 0.72 | to | 0.99 | 0.04 |
| AIS6 ≥3 | 1.25 | 1.04 | to | 1.50 | 0.02 |
| AIS7 ≥ 3 | 1.26 | 1.11 | to | 1.44 | 0.001 |
| AIS8 ≥ 3 | 1.25 | 1.14 | to | 1.37 | <0.001 |
| AIS9 ≥ 3 | 0.50 | 0.10 | to | 2.47 | 0.39 |
| Interventions before hospital arrival | |||||
| Oxygen | 0.85 | 0.78 | to | 0.93 | <0.001 |
| Immobilization | 1.16 | 1.06 | to | 1.27 | 0.001 |
| Chest compression | 1.15 | 0.75 | to | 1.75 | 0.52 |
| Intravenous line placement | 1.41 | 1.00 | to | 2.01 | 0.05 |
| Defibrillation | 1.05 | 0.32 | to | 3.43 | 0.94 |
| Intubation | 1.73 | 0.99 | to | 3.03 | 0.05 |
| Comorbidities | |||||
| Mental disease | 0.94 | 0.71 | to | 1.24 | 0.67 |
| Mental retardation | 1.56 | 1.11 | to | 2.18 | 0.009 |
| Physical disease | 1.02 | 0.55 | to | 1.88 | 0.96 |
| Variables | Odds Ratio | 95% Confidence Interval | p-Value | ||
|---|---|---|---|---|---|
| Age groups: years | |||||
| 0 | Ref | ||||
| 1–3 | 0.64 | 0.34 | to | 1.22 | 0.18 |
| 4–6 | 0.56 | 0.30 | to | 1.04 | 0.07 |
| 7–12 | 0.75 | 0.41 | to | 1.39 | 0.37 |
| 13–18 | 0.99 | 0.54 | to | 1.83 | 0.98 |
| Sex | |||||
| Male | 0.88 | 0.80 | to | 0.96 | 0.007 |
| Year | |||||
| 2004–2007 | Ref | ||||
| 2008–2010 | 1.30 | 1.08 | to | 1.56 | 0.005 |
| 2011–2013 | 1.38 | 1.16 | to | 1.63 | <0.001 |
| 2014–2016 | 1.48 | 1.25 | to | 1.75 | <0.001 |
| 2017–2019 | 1.46 | 1.23 | to | 1.74 | <0.001 |
| Month | |||||
| January–March | Ref | ||||
| April–June | 0.93 | 0.82 | to | 1.05 | 0.23 |
| July–September | 0.92 | 0.82 | to | 1.04 | 0.21 |
| October–December | 0.98 | 0.86 | to | 1.11 | 0.71 |
| Days of week | |||||
| Weekdays | Ref | ||||
| Weekends/Holidays | 1.10 | 1.00 | to | 1.20 | 0.04 |
| Time | |||||
| Daytime | 0.91 | 0.83 | to | 0.99 | 0.03 |
| Type of trauma | |||||
| Traffic accident | Ref | ||||
| Fall | 0.89 | 0.79 | to | 1.01 | 0.06 |
| Other blunt trauma | 0.63 | 0.54 | to | 0.74 | <0.001 |
| Penetrating trauma | 1.04 | 0.67 | to | 1.61 | 0.86 |
| Cause of trauma | |||||
| Accident | Ref | ||||
| Occupational injury | 1.19 | 0.73 | to | 1.94 | 0.48 |
| Suicide | 1.06 | 0.81 | to | 1.37 | 0.68 |
| Violence | 1.70 | 1.14 | to | 2.53 | 0.009 |
| Others | 1.18 | 0.65 | to | 2.13 | 0.59 |
| Prehospital vital signs | |||||
| Hypotension | 1.42 | 0.77 | to | 2.59 | 0.259 |
| Severity of Trauma | |||||
| RTS | 1.270 | 1.197 | to | 1.348 | <0.001 |
| AIS | |||||
| AIS1 ≥ 3 | 0.76 | 0.69 | to | 0.85 | <0.001 |
| AIS2 ≥ 3 | 0.79 | 0.51 | to | 1.24 | 0.31 |
| AIS3 ≥ 3 | 1.14 | 0.38 | to | 3.40 | 0.81 |
| AIS4 ≥ 3 | 0.85 | 0.76 | to | 0.95 | 0.004 |
| AIS5 ≥ 3 | 0.86 | 0.72 | to | 1.04 | 0.13 |
| AIS6 ≥ 3 | 1.48 | 1.20 | to | 1.83 | <0.001 |
| AIS7 ≥ 3 | 1.26 | 1.07 | to | 1.49 | 0.007 |
| AIS8 ≥ 3 | 1.22 | 1.09 | to | 1.37 | 0.001 |
| AIS9 ≥ 3 | 1.28 | 0.10 | to | 15.56 | 0.85 |
| Interventions before hospital arrival | |||||
| Oxygen | 0.81 | 0.73 | to | 0.90 | <0.001 |
| Immobilization | 1.07 | 0.96 | to | 1.19 | 0.21 |
| Chest compression | 1.96 | 0.81 | to | 4.72 | 0.13 |
| Intravenous line placement | 1.20 | 0.74 | to | 1.93 | 0.46 |
| Intubation | 1.78 | 0.65 | to | 4.85 | 0.26 |
| Comorbidities | |||||
| Mental disease | 0.89 | 0.64 | to | 1.24 | 0.49 |
| Mental retardation | 1.52 | 1.04 | to | 2.23 | 0.03 |
| Physical disease | 0.94 | 0.46 | to | 1.93 | 0.87 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otaka, S.; Ohbe, H.; Igeta, R.; Chiba, T.; Ikeda, S.; Shiga, T. Factors Associated with an Increase in On-Site Time of Pediatric Trauma Patients in a Prehospital Setting: A Nationwide Observational Study in Japan. Children 2022, 9, 1658. https://doi.org/10.3390/children9111658
Otaka S, Ohbe H, Igeta R, Chiba T, Ikeda S, Shiga T. Factors Associated with an Increase in On-Site Time of Pediatric Trauma Patients in a Prehospital Setting: A Nationwide Observational Study in Japan. Children. 2022; 9(11):1658. https://doi.org/10.3390/children9111658
Chicago/Turabian StyleOtaka, Shunichi, Hiroyuki Ohbe, Ryuhei Igeta, Takuyo Chiba, Shunya Ikeda, and Takashi Shiga. 2022. "Factors Associated with an Increase in On-Site Time of Pediatric Trauma Patients in a Prehospital Setting: A Nationwide Observational Study in Japan" Children 9, no. 11: 1658. https://doi.org/10.3390/children9111658