
Improving Body Mass Index in Students with Excess Weight through a Physical Activity Programme

Abstract
:1. Introduction
2. Materials and Methods
2.1. Methodology of the Physical Activity Programme
2.2. Presentation of the Contents and Structure of the Physical Activity Programme (PAP) for Schoolchildren with Excess Weight
- A body preparation phase (warm-up) lasting 5–10 min, consisting of 4–5 min of brisk walking/running/cycling, etc., followed by dynamic joint mobility exercises, 5–6 min.
- A main part, lasting 20–30 min, in which exercises on a suitable energy substrate/activity are combined to develop fitness (depending on the module chosen).
- A body recovery phase after exercise (winding down), lasting 5–10 min, which is important for lowering the heart and breathing rates and is achieved by performing a active physical mobility exercises (stretching), static and/or dynamic, to avoid muscle pain.
2.3. Research Subjects, Inclusion/Exclusion Criteria
- Inclusion criteria: pupils from secondary school (grades V–VIII); obesity: BMI ≥ 95th percentile (+2SD) for gender and age; overweight: 85th percentile ≤ BMI < 95th percentile (+2SD) for gender and age; possibility of monitoring and evaluating the results by completing the proposed physical activity programme.
- Exclusion criteria: impossibility to monitor subjects; refusal of parents and/or students to participate in the study.
2.4. Statistical Methods Used in Research
3. Results
3.1. Identification of Subjects with Excess Weight at the Initial Measurement
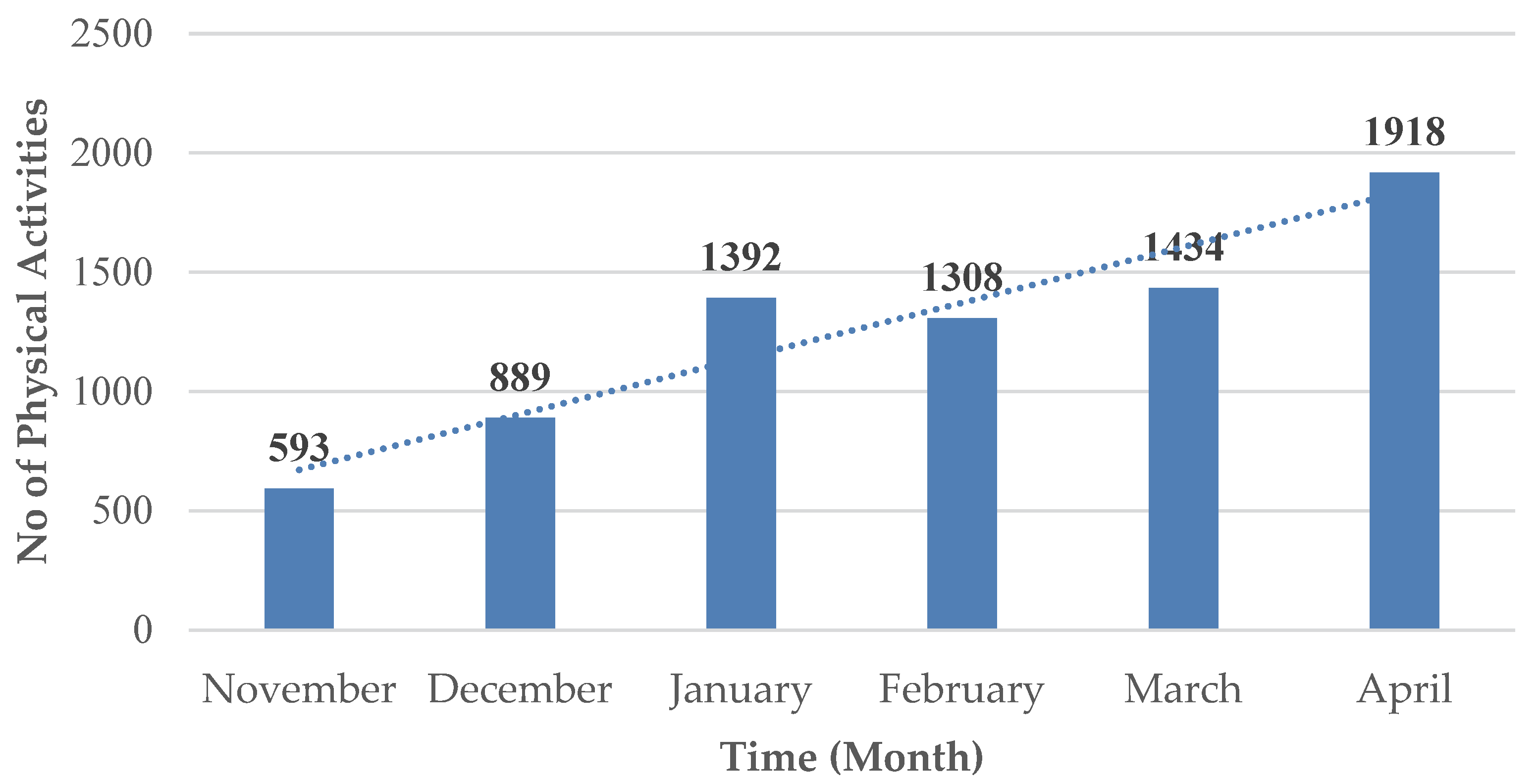
3.2. Average Volume/Frequency of Physical Activities Performed According to the Body Mass Index and Gender of Subjects, Post-Impact PAP
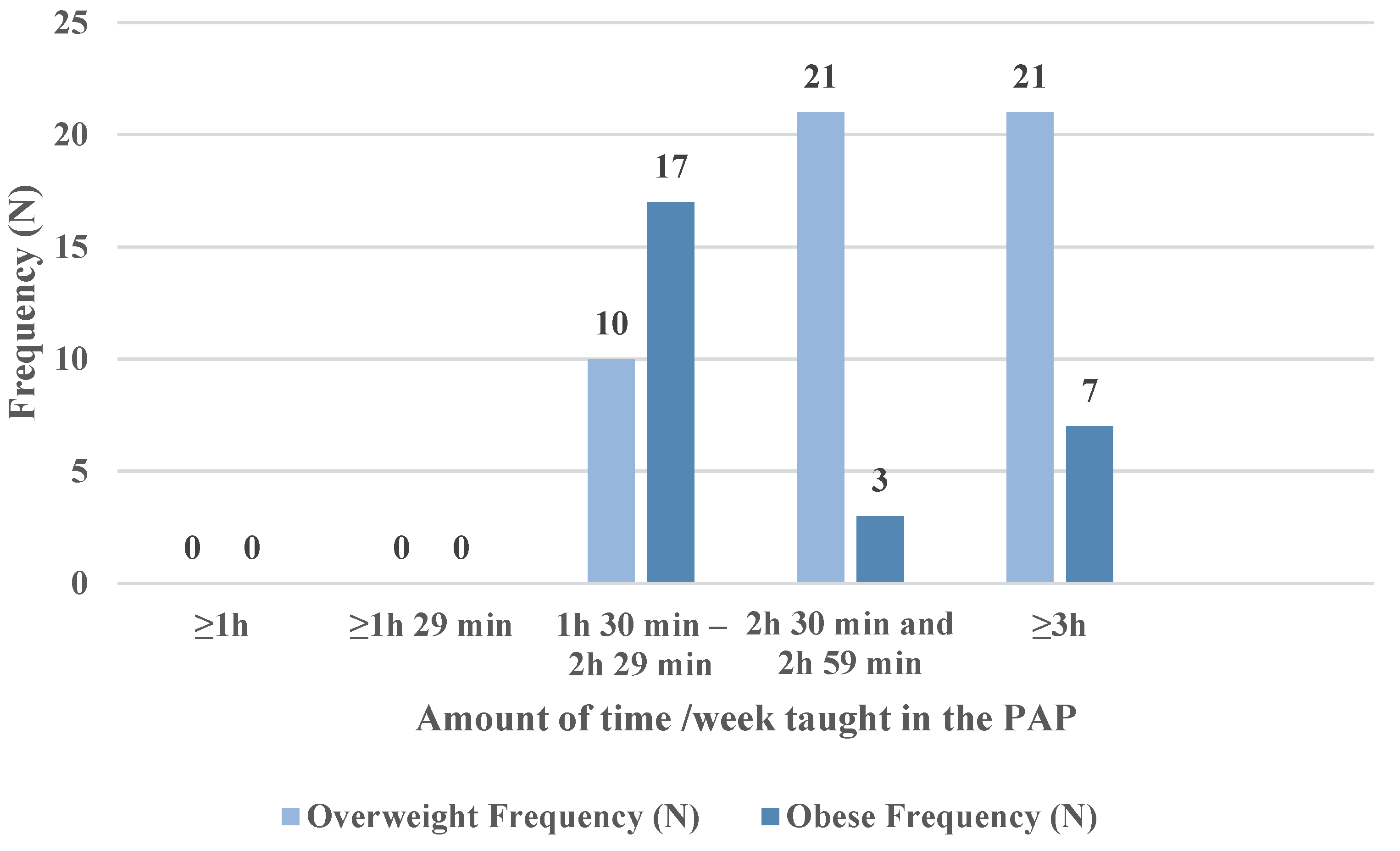
3.3. Averages/Subgroups of the Time Allocated to the PAP Sessions
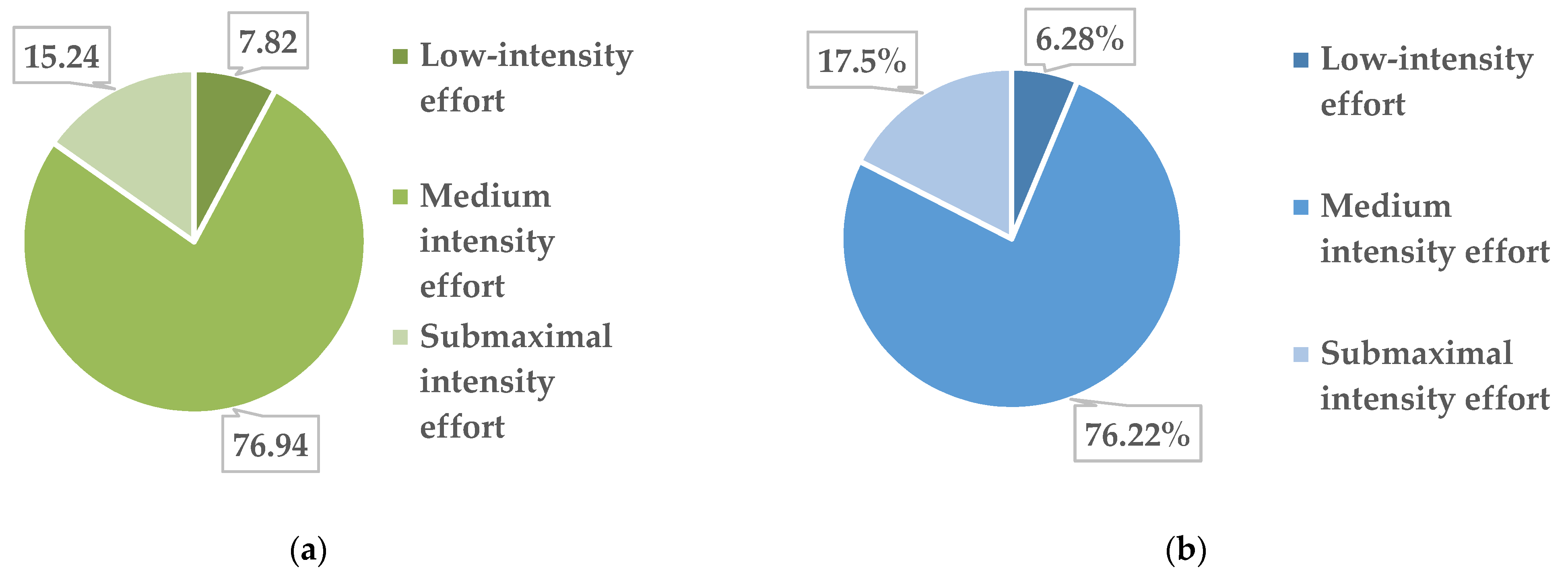
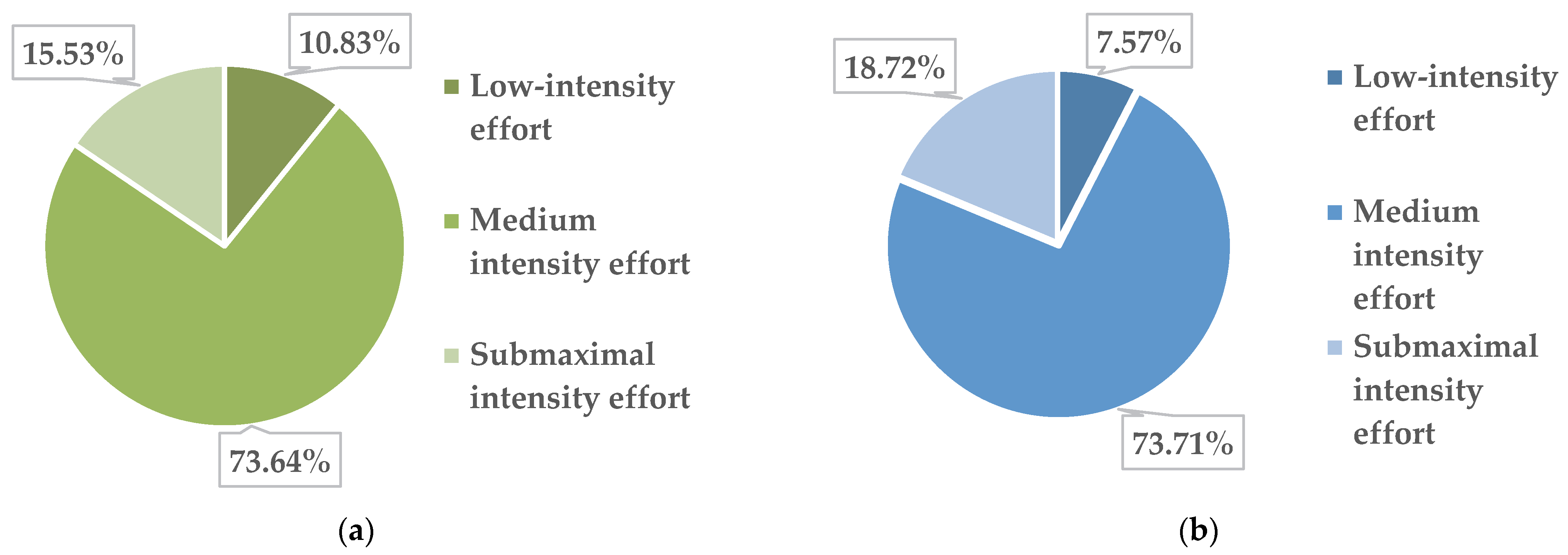
3.4. Averages/Subgroup Effort Intensity of the Physical Activities
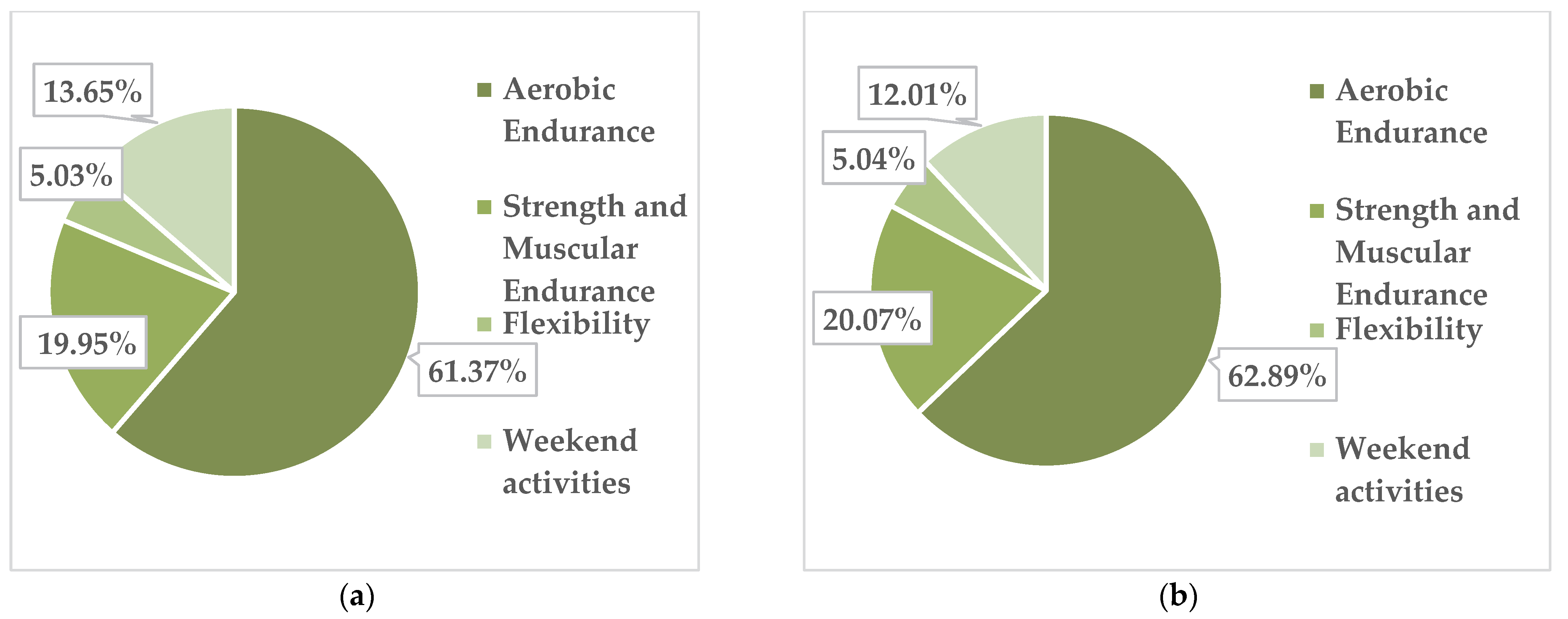
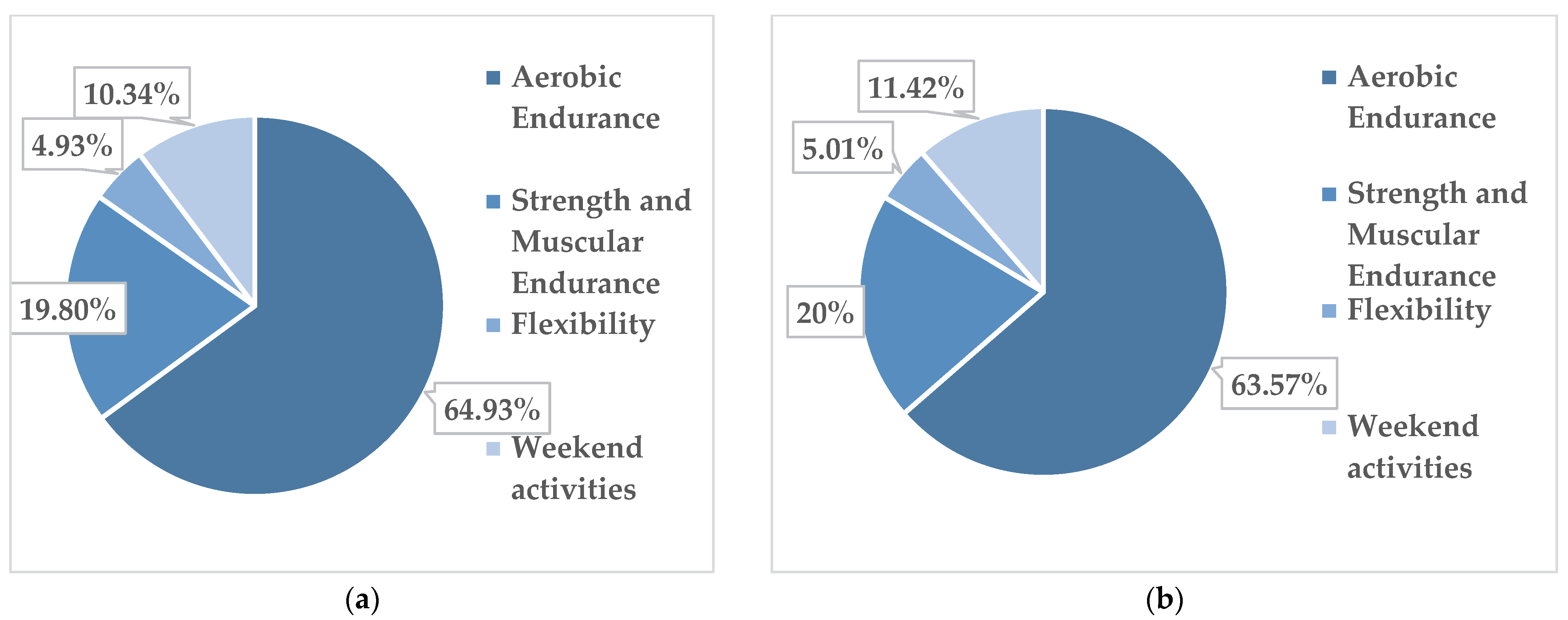
3.5. Types of Activities Chosen by the Study Subjects
3.6. Interpretation of Final Results
- In the final testing, the majority of the subjects measured, namely 75 subjects, had a normal stature index (Table 8).
- In the final measurement of weight, the students showed an average body weight of 66.57 kg, and the results deviate from the average by 12.13 kg. The majority of the subjects measured (77 subjects) had a normal body weight, and only 2 subjects still had a high body weight relative to age (Table 9).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Statural Classification | Frequency | Percentage | Percentage of Measured Subjects | Cumulative Percentage | |
|---|---|---|---|---|---|
| Height (cm) | Hyperstatural | 1 | 1.30 | 1.30 | 1.30 |
| Normostatural | 75 | 94.90 | 94.90 | 96.20 | |
| Hypostatural | 3 | 3.80 | 3.80 | 100 | |
| Total | 79 | 100 | 100 | ||
| Body Weight Classification | Frequency | Percentage | Percentage of Measured Subjects | Cumulative Percentage | |
|---|---|---|---|---|---|
| Weight (kg) | Extra Heavy Weight | 2 | 2.50 | 2.50 | 2.50 |
| Normal weight | 77 | 97.50 | 97.50 | 100 | |
| Very low weight | 0 | 0.00 | 0.00 | ||
| Total | 79 | 100 | 100 | ||
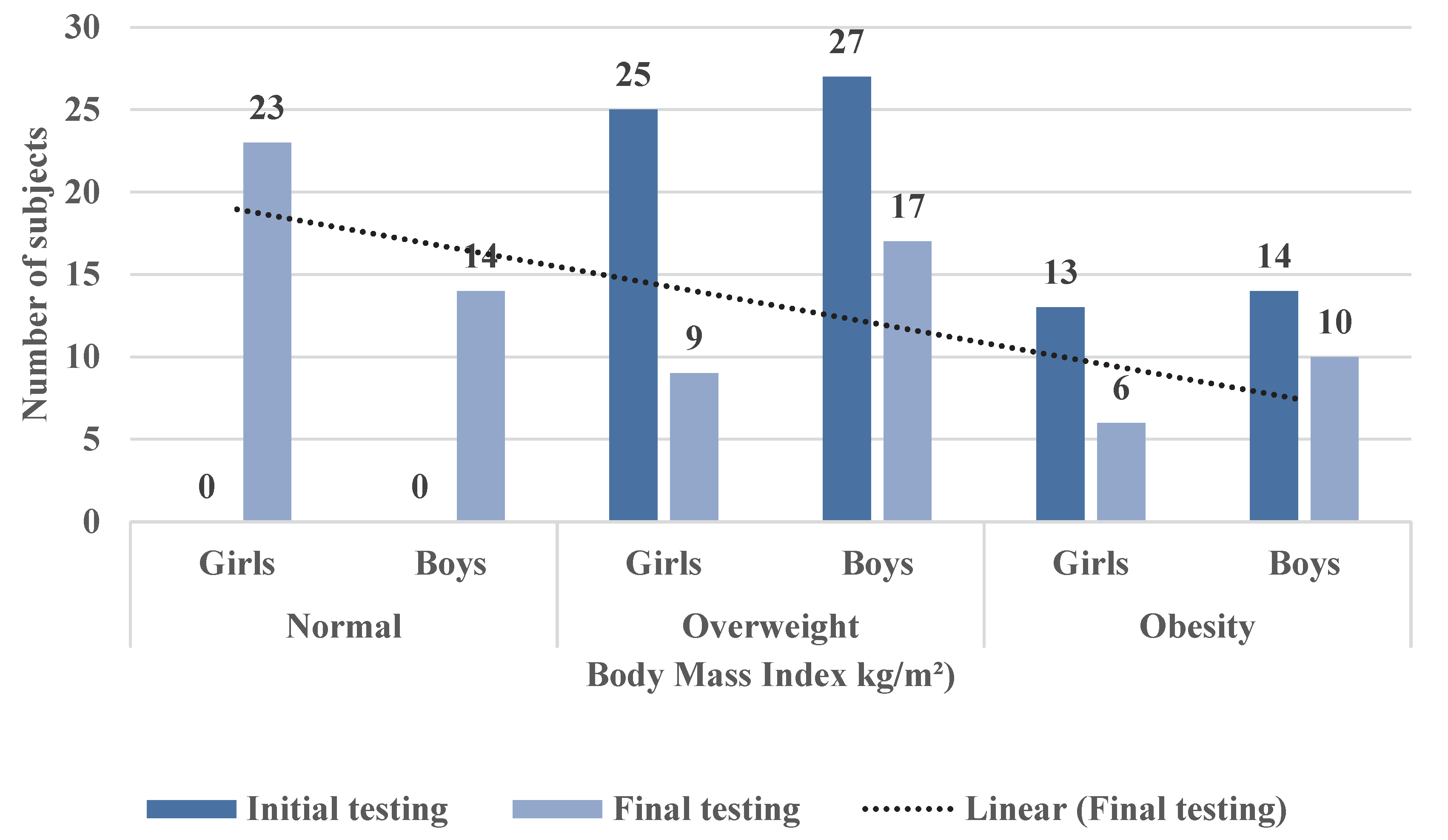
- The analysis of the body mass index at final testing reveals the BMI at the time of final testing by gender. Basically, in order to centralize the results, we defined the categories of subjects according to the new body mass indices obtained after participating in the PAP. Out of the total of 38 girls identified at the initial testing as having excess weight (25 overweight girls and 13 obese girls; see Table 4), at the final testing (Table 10) after completing the PAP, 23 girls acquired a healthy BMI, 9 girls were classified as overweight and 6 girls were obese. In boys, out of the total of 41, initially 27 overweight and 14 obese (Table 4) in the final testing (after completing the PAP), 14 boys reached a healthy BMI, 17 boys were classified as overweight and 10 boys as obese.
| BMI Classification | Frequency | Percentage | Percentage of Evaluated Subjects | Cumulative Percentage | |
|---|---|---|---|---|---|
| BMI (kg/m2) | healthy | 37 | 46.80 | 46.80 | 46.80 |
| overweight | 26 | 32.90 | 32.90 | 79.70 | |
| obesity | 16 | 20.30 | 20.30 | 100 | |
| Total | 79 | 100 | 100 | ||
- In the initial testing, 25 girls were identified as overweight, while in the final testing, only 9 girls were still overweight;
- In the case of overweight boys, in the initial testing, 27 boys were overweight, and in the final testing, 17 boys with overweight were identified;
- In the case of obese girls, 13 girls were recorded with obesity at the initial testing, and 6 girls were obese at the final testing;
- For obese boys, 14 were identified in the initial testing, while in the final testing, only 10 boys had obesity;
- Out of the total number of subjects (79), at the final testing, 37 subjects with a healthy body mass index were reported (23 girls and 14 boys).
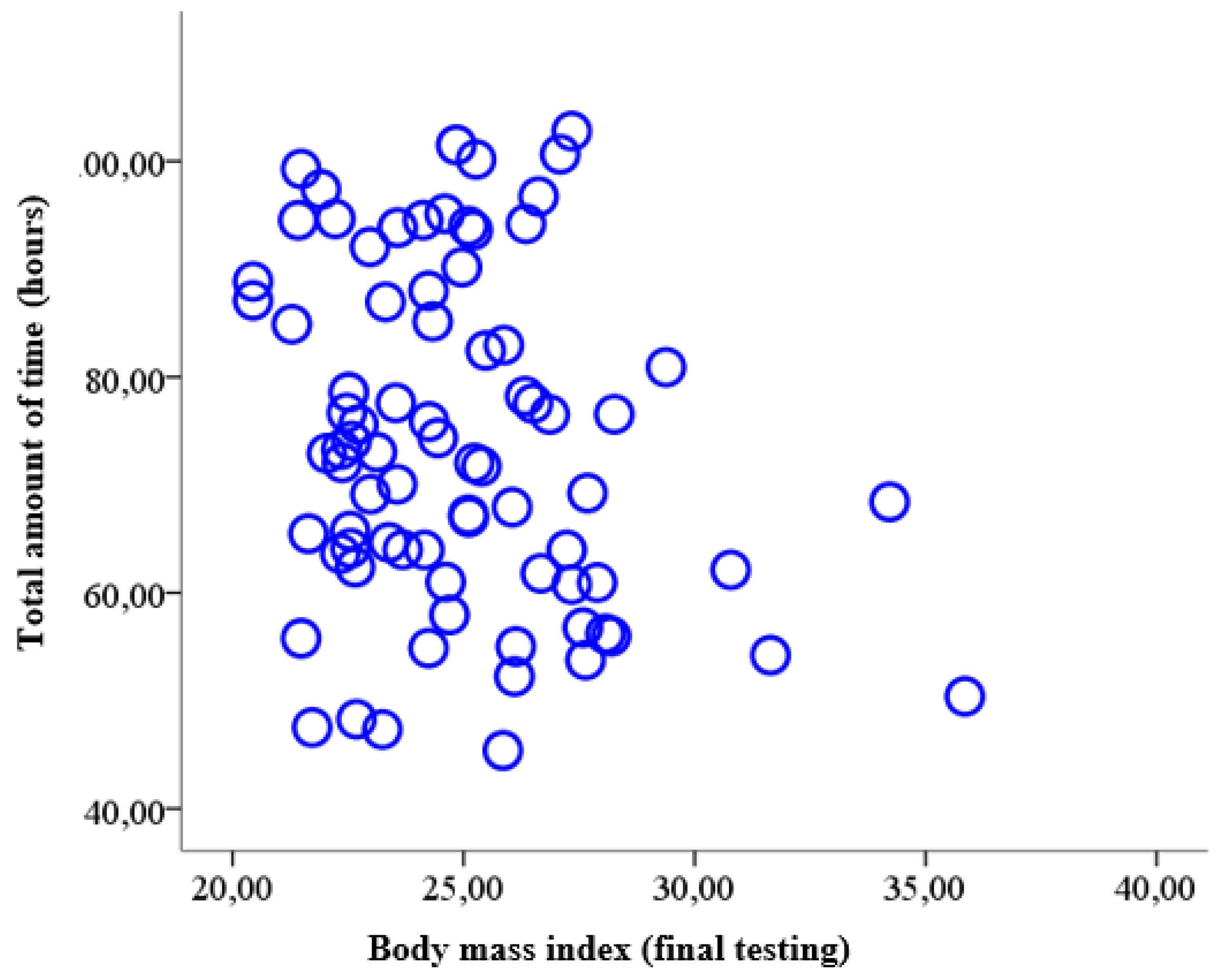
- In concluding this study, we wanted to determine whether there was a relationship between body mass index (acquired at the time of final testing) and the total amount of time allocated by the subjects with excess weight to the physical activity programme (PAP). Thus, the materiality threshold (p = 0.04) obtained in the bivariate analysis between the BMI determined at the final testing on the one hand and the total amount of time devoted to PAP on the other hand shows that there is a statistically significant correlation. As we can see, this correlation is reversed (r = −0.23), which allows us to state that in the entire sample (79 subjects with overweight and obesity), a higher body mass index was associated with less time dedicated to the physical activity program (PAP) (Table 11 and Figure 9).
| BMI-TF | VT. PAP | ||
|---|---|---|---|
| BMI-TF | Correlation coefficient | 1 | −0.23 |
| Materiality threshold (p) | 0.04 | ||
| N | 79 | 79 | |
| VT. PAP | Correlation coefficient | −0.23 | 1 |
| Materiality threshold (p) | 0.04 | ||
| df | 79 | 79 | |
4. Discussion
5. Research Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Valverde, J. Valoración de la Asignatura de Educación Física y su Relación con los Niveles de Actividad Física Habitual en Adolescentes Escolarizados de la Región de Murcia. Ph.D. Thesis, Universidad de Murcia, Murcia, Spain, 20 May 2008. [Google Scholar]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- López-Sánchez, G.; Emeljanovas, A.; Miežienė, B.; Díaz-Suárez, A.; Sánchez-Castillo, S.; Yang, L.; Roberts, J.; Smith, L. Levels of Physical Activity in Lithuanian Adolescents. Medicina 2018, 54, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aznar, S.; Webster, T. Actividad física y salud en la infancia y la adolescencia. In Guía para Todas las Personas que Participan en su Educación; Grafo, S.A.: Madrid, Spain, 2006; pp. 42–47. Available online: https://www.sanidad.gob.es/ciudadanos/proteccionSalud/adultos/actiFisica/docs/ActividadFisicaSaludEspanol.pdf (accessed on 11 December 2018).
- Ingram, D.K. Age-related decline in physical activity: Generalization to nonhumans. Med. Sci. Sport. Exerc. 2000, 32, 1623–1629. [Google Scholar] [CrossRef]
- Sallis, J.F.; Prochaska, J.J.; Taylor, W.C. A review of correlates of physical activity of children and adolescents. Med. Sci. Sport. Exerc. 2000, 32, 963–975. [Google Scholar] [CrossRef] [PubMed]
- Lasheras, L.; Aznar, S.; Merino, B.; López, E.G. Factors Associated with Physical Activity among Spanish Youth through the National Health Survey. Prev. Med. 2001, 32, 455–464. [Google Scholar] [CrossRef]
- Corder, K.; Winpenny, E.; Love, R.; Brown, H.E.; White, M.; Sluijs, E.V. Change in physical activity from adolescence to early adulthood: A systematic review and meta-analysis of longitudinal cohort studies. Br. J. Sport. Med. 2019, 53, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Nader, P.R.; Bradley, R.H.; Houts, R.M.; McRitchie, S.L.; O’Brien, M. Moderate-to-vigorous physical activity from ages 9 to 15 years. J. Am. Med. Asoc. 2008, 300, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Lau, E.Y.; Dowda, M.; McIver, K.L.; Pate, R.R. Changes in physical activity in the school, afterschool, and evening periods during the transition from elementary to middle school. J. Sch. Health 2017, 87, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Lee, I.M.; Martin, C.K.; Blair, S.N. Epidemiology of Physical Activity and Exercise Training in the United States. Prog. Cardiovasc. Dis. 2017, 60, 3–10. [Google Scholar] [CrossRef]
- Castillo-Fernández, I.; Balaguer-Solá, I. Dimensiones de los motivos de práctica deportiva de los adolescentes valencianos escolarizados. Apunt. Educ. Física Esports 2001, 63, 22–29. [Google Scholar]
- Rowlands, A.V.; Pilgrim, E.L.; Eston, R.G. Patterns of habitual activity across weekdays and weekend days in 9–11-year-old children. Prev. Med. 2007, 46, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F. Age-related decline in physical activity: A synthesis of human and animal studies. Med. Sci. Sport. Exerc. 2000, 32, 1598–1600. [Google Scholar] [CrossRef] [PubMed]
- Riddoch, C.J.; Andersen, L.B.; Wedderkopp, N.; Harro, M.; Klasson-Heggebo, L.; Sardinha, L.B.; Cooper, A.R.; Ekelund, U.L.F. Physical activity levels and patterns of 9-and 15-yr-old European children. Med. Sci. Sport. Exerc. 2004, 36, 86–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitt-Glover, M.C.; Taylor, W.C.; Floyd, M.F.; Yore, M.M.; Yancey, A.K.; Matthews, C.E. Disparities in Physical Activity and Sedentary Behaviors Among US Children and Adolescents: Prevalence, Correlates, and Intervention Implications. J. Public Health Policy 2009, 30, S309–S334. [Google Scholar] [CrossRef]
- Slater, A.; Tiggemann, M. “Uncool to do sport”: A focus group study of adolescent girls’ reasons for withdrawing from physical activity. Psychol. Sport Exerc. 2010, 11, 619–626. [Google Scholar] [CrossRef]
- Butt, J.; Weinberg, R.S.; Breckon, J.D.; Claytor, R.P. Adolescent physical activity participation and motivational determinants across gender, age, and race. J. Phys. Act. Health 2011, 8, 1074–1083. [Google Scholar] [CrossRef] [PubMed]
- Bailey, D.; Fairclough, S.; Savory, L.; Denton, S.; Pang, D.; Deane, C.; Kerr, C. Accelerometry-assessed sedentary behaviour and physical activity levels during the segmented school day in 10–14-year-old children: The HAPPY study. Eur. J. Pediatr. 2012, 171, 1805–1813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumith, S.C.; Gigante, D.P.; Domingues, M.R.; Hallal, P.C.; Menezes, A.M.B.; Kohl, H.W. Predictors of physical activity change during adolescence: A 3.5-year follow-up. Public Health Nutr. 2012, 15, 2237–2245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, A.R.; Goodman, A.; Page, A.S.; Sherar, L.B.; Esliger, D.W.; van Sluijs, E.; Andersen, L.B.; Anderssen, S.; Cardon, G.; Davey, R.; et al. Objectively measured physical activity and sedentary time in youth: The international children’s accelerometry database (ICAD). Int. J. Behav. Nutr. Phys. Act. 2015, 12, 113. [Google Scholar] [CrossRef] [Green Version]
- Van Hecke, L.; Loyen, A.; Verloigne, M.; Van der Ploeg, H.P.; Lakerveld, J.; Brug, J.; de Bourdeaudhuij, I.; Ekelund, U.; Donnelly, A.; Hendriksen, I.; et al. Variation in population levels of physical activity in European children and adolescents according to cross-European studies: A systematic literature review within DEDIPAC. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 70. [Google Scholar] [CrossRef] [Green Version]
- Varo, J.J.; Martínez-González, M.A.; de Irala-Estévez, J.; Kearney, J.; Gibney, M.; Martínez, J.A. Distribution and determinants of sedentary lifestyles in the European Union. Int. J. Epidemiol. 2003, 32, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Boyce, W.F.; Simpson, K.; Pickett, W. Influence of individual-and area-level measures of socioeconomic status on obesity, unhealthy eating, and physical inactivity in Canadian adolescents. Am. J. Clin. Nutr. 2006, 83, 139–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodenburg, G.; Oenema, A.; Pasma, M.; Kremers, S.P.J.; van de Mheen, D. Clustering of food and activity preferences in primary school children. Appetite 2013, 60, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Gubbels, J.S.; van Assema, P.; Kremers, S.P.J. Physical Activity, Sedentary Behavior, and Dietary Patterns among Children. Curr. Nutr. Rep. 2013, 2, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Perez-Villagrán, S.; Novalbos-Ruiz, J.P.; Rodríguez-Martín, A.; Martínez-Nieto, J.M.; Lechuga-Sancho, A.M. Implications of family socioeconomic level on risk behaviors in child-youth obesity. Nutr. Hosp. 2013, 28, 1951–1960. [Google Scholar] [CrossRef]
- Baquet, G.; Ridgers, N.D.; Blaes, A.; Aucouturier, J.; Van Praagh, E.; Berthoin, S. Objectively assessed recess physical activity in girls and boys from high and low socioeconomic backgrounds. BMC Public Health 2014, 14, 192. [Google Scholar] [CrossRef] [Green Version]
- Fernández, I.; Canet, O.; Giné-Garriga, M. Assessment of physical activity levels, fitness and perceived barriers to physical activity practice in adolescents: Cross-sectional study. Eur. J. Pediatr. 2016, 176, 57–65. [Google Scholar] [CrossRef]
- Hankonen, N.; Heino, M.T.J.; Kujala, E.; Hynynen, S.; Absetz, P.; Araújo-Soares, V.; Haukkala, A. What explains the socioeconomic status gap in activity? educational differences in determinants of physical activity and screentime. BMC Public Health 2017, 17, 144. [Google Scholar] [CrossRef] [Green Version]
- Al-Hazzaa, H.M. Physical inactivity in Saudi Arabia revisited: A systematic review of inactivity prevalence and perceived barriers to active living. Int. J. Health Sci. 2018, 12, 50–64. [Google Scholar]
- Moreno-Murcia, J.A.; Cervelló, E.; Huéscar, E.; Llamas, L. Relación de los motivos de práctica deportiva en adolescentes con la percepción de competencia, imagen corporal y hábitos saludables. Cult. Educ. 2011, 23, 533–542. [Google Scholar] [CrossRef]
- Molina, J. Un Estudio Sobre la Práctica de Actividad Física, la Adiposidad Corporal y el Bienestar Psicológico en Universitarios. Ph.D. Thesis, Universidad de Valencia, Valencia, Spain, 18 June 2007. [Google Scholar]
- Garzón, P.C.; Fernández, M.D.; Sánchez, P.T.; Gross, M.G. Actividad físico-deportiva en escolares adolescentes. Retos Nuevas Tend. Educ. Física Deporte Recreación 2002, 3, 5–12. [Google Scholar] [CrossRef]
- Casterad, J.Z.; Puyal, J.R.S.; Gurrola, O.C.; Lanaspa, E.G.; Ostariz, E.S.; Clemente, J.A.J. Los factores ambientales y su influencia en los patrones de actividad física en adolescentes. RICYDE Rev. Int. Cienc. Deporte 2006, 2, 1–14. [Google Scholar] [CrossRef]
- Narciso, J.; Silva, A.J.; Rodrigues, V.; Monteiro, M.J.; Almeida, A.; Saavedra, R.; Costa, A.M. Behavioral, contextual and biological factors associated with obesity during adolescence: A systematic review. PLoS ONE 2019, 14, e0214941. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Loprinzi, P.D. Exercise—Promoting healthy lifestyles in children and adolescents. J. Clin. Lipidol. 2008, 2, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Melnyk, B.M.; Jacobson, D.; Kelly, S.; Belyea, M.; Shaibi, G.; Small, L.; Marsiglia, F.F. Promoting Healthy Lifestyles in High School Adolescents. Am. J. Prev. Med. 2013, 45, 407–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bădicu, G. Contribution to the Improvement of the Quality of Life in Adults through the Implementation of Leisure Sports Programs. Ph.D. Thesis, Transilvania University of Brașov, Brașov, Romania, 17 July 2015. [Google Scholar]
- Jakicic, J.M.; Otto, A.D. Physical activity considerations for the treatment and prevention of obesity. Am. J. Clin. Nutr. 2005, 82, 226S–229S. [Google Scholar] [CrossRef]
- Arocha Rodulfo, J.I. Sedentarism, a disease from XXI century. Clínica Investig. Arterioscler. 2019, 31, 233–240. [Google Scholar] [CrossRef]
- Tur, J.A.; Martinez, J.A. Guide and advances on childhood obesity determinants: Setting the research agenda. Obes. Rev. 2021, 23, e13379. [Google Scholar] [CrossRef]
- Garcia-Pastor, T.; Salinero, J.J.; Sanz-Frias, D.; Pertusa, G.; Del Coso, J. Body fat percentage is more associated with low physical fitness than with sedentarism and diet in male and female adolescents. Physiol. Behav. 2016, 165, 166–172. [Google Scholar] [CrossRef]
- Gutin, B.; Yin, Z.; Humphries, M.C.; Barbeau, P. Relations of moderate and vigorous physical activity to fitness and fatness in adolescents. Am. J. Clin. Nutr. 2005, 81, 746–750. [Google Scholar] [CrossRef] [Green Version]
- Ortega, F.B.; Tresaco, B.; Ruiz, J.R.; Moreno, L.A.; Martin-Matillas, M.; Mesa, J.L.; Warnberg, J.; Bueno, M.; Tercedor, P.; Gutiérrez, A.; et al. Cardiorespiratory fitness and sedentary activities are associated with adiposity in adolescents. Obesity 2007, 15, 1589–1599. [Google Scholar] [CrossRef] [PubMed]
- An, R. Diet quality and physical activity in relation to childhood obesity. Int. J. Adolesc. Med. Health 2017, 29, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ying-Xiu, Z.; Jin-Shan, Z.; Jing-Yang, Z.; Zun-Hua, C.; Guang-Jian, W. Comparison on physical activity among adolescents with different weight status in Shandong, China. J. Trop. Pediatr. 2013, 59, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Lagestad, P.; Van den Tillaar, R.; Mamen, A. Longitudinal changes in physical activity level, body mass index, and oxygen uptake among norwegian adolescents. Front. Public Health 2018, 6, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vălean, C.; Tătar, S.; Nanulescu, M.; Leucuța, A.; Ichim, G. Prevalence of obesity and overweight among school schildren in Cluj-Napoca. Acta Endocrinol. 2009, 5, 213–219. [Google Scholar] [CrossRef]
- Chiriță-Emandi, A.C.; Puiu, M.; Gafencu, M.; Pienar, C. Growth references for school aged children in western Romania. Acta Endocrinol. 2012, 8, 133–152. [Google Scholar] [CrossRef]
- Chiriță-Emandi, A.; Barbu, C.G.; Cinteza, E.E.; Chesaru, B.I.; Gafencu, M.; Mocanu, V.; Pascanu, I.M.; Tatar, S.A.; Balgradean, M.; Dobre, M.; et al. Overweight and Underweight Prevalence Trends in Children from Romania—Pooled Analysis of Cross-Sectional Studies between 2006 and 2015. Obes. Facts 2016, 9, 206–220. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines on Physical Activity and Sedentary Behaviour. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/336656/9789240015128-eng.pdf?sequence=1&isAllowed=y (accessed on 23 January 2019).
- Gutin, B.; Barbeau, P.; Owens, S.; Lemmon, C.R.; Bauman, M.; Allison, J.; Kang, K.S.; Litaker, M.S. Effects of exercise intensity on cardiovascular fitness, total body composition, and visceral adiposity of obese adolescents. Am. J. Clin. Nutr. 2002, 75, 818–826. [Google Scholar] [CrossRef] [Green Version]
- Obert, P.; Mandigouts, S.; Nottin, S.; Vinet, A.; N’Guyen, L.D.; Lecoq, A.M. Cardiovascular responses to endurance training in children: Effect of gender. Eur. J. Clin. Investig. 2003, 33, 199–208. [Google Scholar] [CrossRef]
- Bar, O.; Rowland, W.T. Paediatric Exercise Medicine from Physiological Principles to Health Care Application; Human Kinetics: Champaign, IL, USA, 2004; pp. 500–501. [Google Scholar]
- Malina, R.M. Weight Training in Youth-Growth, Maturation, and Safety: An Evidence-Based Review. Clin. J. Sport Med. 2006, 16, 478–487. [Google Scholar] [CrossRef]
- MacKelvie, K.J.; Petit, M.A.; Khan, K.M.; Beck, T.J.; McKay, H.A. Bone mass and structure are enhanced following a 2-year randomized controlled trial of exercise in prepubertal boys. Bone 2004, 34, 755–764. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, H.M.; Kontulainen, S.A.; Khan, K.M.; McKay, H.A. Is a School-Based Physical Activity Intervention Effective for Increasing Tibial Bone Strength in Boys and Girls? J. Bone Miner. Res. 2006, 22, 434–446. [Google Scholar] [CrossRef] [PubMed]
- România–Documente. Evaluarea Nivelului de Dezvoltare Fizică și a Stării de Sănătate. Available online: https://documente.net/document/evaluarea-nivelului-de-dezvoltare-fizica-si-a-starii-de-inspgovrositescnepsswp-contentuploads201805raport-national.html?page=13 (accessed on 16 June 2019).
- World Obesity Federation. Childhood Obesity Atlas Report. Available online: https://s3-eu-west-1.amazonaws.com/wof-files/WOF_Childhood_Obesity_Atlas_Report_Oct19_V2.pdf (accessed on 26 May 2019).
- Tremblay, M.S.; Carson, V.; Chaput, J.P.; Gorber, S.C.; Dinh, T.; Duggan, M.; Faulkner, G.; Gray, C.E.; Gruber, R.; Janson, K.; et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metabolism. 2016, 416 (Suppl. 3), S311–S327. [Google Scholar] [CrossRef] [PubMed]









| PAP—Aerobic Endurance Module | |||
|---|---|---|---|
| Session Frequency | Intensity | Dosing | Type of Activity |
| 5–7 times/week | Moderate-high 130–150 heartbeats/min. 155–170 heartbeats/min. | 15–60 min/session (With an upward dynamic in volume) | Running, skating, cycling, swimming, cross-country skiing or any other cyclical physical activity |
| PAP—Strength and Muscular Endurance module | |||
| Session frequency | Intensity | Dosing | Type of activity |
| at least 3 times/week | Moderate 130–150 heartbeats/min. | 8–10 repetitions; 8 to 10 exercises/set of exercises | A wide range of exercises for harmonious physical development, toning and muscle trophicity. |
| PAP—Flexibility module | |||
| Session frequency | Intensity/Amplitude | Dosing | Type of activity |
| at least ≥3 times/week | There must be no pain | Dynamic exercises—Position must be held for 4–5 s, 3–5 repetitions Static exercises—Position must be held for 10–20 s. | Pilates stretching (Active and combined) |
| PAP—Weekend activities module | |||
| Session frequency | Intensity | Dosing | Type of activity |
| 1 time/week | Moderate 130–150 heartbeats/min. | Depending on the chosen route (2 to 4.2 km) | Hiking, Theme parks |
| Statural Classification | Frequency | Percentage | Percentage of Measured Subjects | Cumulative Percentage | |
|---|---|---|---|---|---|
| Height (cm) | Hyperstatural | 1 | 1.30 | 1.30 | 1.30 |
| Normostatural | 74 | 93.70 | 93.70 | 94.90 | |
| Hypostatural | 4 | 5.10 | 5.10 | 100 | |
| Total | 79 | 100 | 100 | ||
| Body Weight Classification | Frequency | Percentage | Percentage of Measured Subjects | Cumulative Percentage | |
|---|---|---|---|---|---|
| Weight (kg) | Extra Heavy Weight | 23 | 29.10 | 29.10 | 29.10 |
| Healthy weight | 56 | 70.90 | 70.90 | 100 | |
| Very low weight | 0 | 0.00 | 0.00 | ||
| Total | 79 | 100 | 100 | ||
| BMI (kg/m2) | Total | ||||
|---|---|---|---|---|---|
| Overweight | Obesity | ||||
| Gender | Girls | Frequency | 25 | 13 | 38 |
| Percentage (%) | 65.80% | 34.20% | 100% | ||
| Boys | Frequency | 27 | 14 | 41 | |
| Percentage (%) | 65.90% | 34.10% | 100% | ||
| Total | Frequency | 52 | 27 | 79 | |
| Percentage (%) | 65.80% | 34.20% | 100% | ||
| BMI | Gender | N | Frequency Average | Standard Deviation | Average Standard Error | 95% Conf. Range | Minimum | Maximum | |
|---|---|---|---|---|---|---|---|---|---|
| Min. | Max. | ||||||||
| O | Girls | 13 | 96.38 | 21.02 | 5.83 | 83.68 | 109.09 | 73 | 123 |
| Boys | 14 | 85.07 | 13.30 | 3.55 | 77.39 | 92.75 | 69 | 123 | |
| Total | 27 | 90.72 | 18.04 | 3.47 | 83.38 | 97.66 | 69 | 123 | |
| SP | Girls | 25 | 100.60 | 13.92 | 2.78 | 94.85 | 106.35 | 75 | 124 |
| Boys | 27 | 95.37 | 18.87 | 3.63 | 87.91 | 102.83 | 64 | 124 | |
| Total | 52 | 97.98 | 16.72 | 2.32 | 93.23 | 102.54 | 64 | 124 | |
| BMI (kg/m2) Quantitative Indicators | Average Time Volume/Week Dedicated to the Physical Activity Programme by Subject/Group | Total | ||||||
|---|---|---|---|---|---|---|---|---|
| ≥1 h | ≥1 h 29 min | 1 h 30 min–2 h 29 min | 2 h 30 min and 2 h 59 min | ≥3 h | ||||
| Groups | Overweight | Frequency (N) | 0 | 0 | 10 | 21 | 21 | 52 |
| Percentage (%) | 0.00% | 0.00% | 19.20% | 40.40% | 40.40% | 100% | ||
| Obese | Frequency (N) | 0 | 0 | 17 | 3 | 7 | 27 | |
| Percentage (%) | 0.00% | 0.00% | 63.00% | 11.10% | 25.90% | 100% | ||
| Total | Frequency (N) | 0 | 0 | 27 | 24 | 28 | 79 | |
| Percentage (%) | 0.00% | 0.00% | 34.20% | 30.40% | 35.40% | 100% | ||
| BMI (kg/m2) | Gender | No. of Subjects | Freq. N/AF | Total | ||
|---|---|---|---|---|---|---|
| A | B | C | ||||
| overweight | Girls | 25 | No. AF | 158 | 1917 | 440 |
| % | 6.28% | 76.22% | 17.50% | |||
| Boys | 27 | No. AF | 195 | 1898 | 482 | |
| % | 7.57% | 73.71% | 18.72% | |||
| Total | 52 | No. AF | 353 | 3815 | 922 | |
| % | 6.94% | 74.95% | 18.11% | |||
| obesity | Girls | 13 | No. AF | 98 | 964 | 191 |
| % | 7.82% | 76.94% | 15.24% | |||
| Boys | 14 | No. AF | 129 | 877 | 185 | |
| % | 10.83% | 73.64% | 15.53% | |||
| Total | 27 | No. AF | 227 | 1841 | 376 | |
| % | 9.29% | 75.33% | 15.38% | |||
| Total | 79 | No. AF | 580 | 5656 | 1298 | |
| % | 7.70% | 75.07% | 17.23% | |||
| Value | Degrees of Freedom | p | |
|---|---|---|---|
| Pearson Chi-Square | 16.01 | 2 | 0.001 |
| Fisher’s Exact Test | 15.53 | 0.001 | |
| Valid responses | 79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scurt, M.D.; Balint, L.; Mijaică, R. Improving Body Mass Index in Students with Excess Weight through a Physical Activity Programme. Children 2022, 9, 1638. https://doi.org/10.3390/children9111638
Scurt MD, Balint L, Mijaică R. Improving Body Mass Index in Students with Excess Weight through a Physical Activity Programme. Children. 2022; 9(11):1638. https://doi.org/10.3390/children9111638
Chicago/Turabian StyleScurt, Mădălina Doiniţa, Lorand Balint, and Raluca Mijaică. 2022. "Improving Body Mass Index in Students with Excess Weight through a Physical Activity Programme" Children 9, no. 11: 1638. https://doi.org/10.3390/children9111638