
Use of Virtual Reality in Children with Dyslexia
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Design of the Study
2.3. Neuropsychological Assessment
2.4. Virtual Reality Neurorehabilitation Treatment (VRNT) with Khymeia VRRS
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saralegui, I.; Ontañón, J.M.; Fernandez-Ruanova, B.; Garcia-Zapirain, B.; Basterra, A.; Sanz-Arigita, E.J. Reading networks in children with dyslexia compared to children with ocular motility disturbances revealed by fMRI. Front. Hum. Neurosci. 2014, 8, 936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyon, G.R.; Shaywitz, S.E.; Shaywitz, B.A. Una definizione di dislessia. Ann. Dyslexia 2003, 53, 1–14. [Google Scholar]
- Pennington, B.F. Diagnosi dei Disturbi Dell’apprendimento. In Un Quadro Neuropsicologico, 2nd ed.; Guilford Press: New York, NY, USA, 2009. [Google Scholar]
- Fletcher, J.M.; Lione, G.R.; Fuchs, L.S.; Barnes, M.A. Disturbi Dell’Apprendimento: Dall’Identificazione All’Intervento; Guilford: New York, NY, USA, 2007. [Google Scholar]
- Rutter, M.; Caspi, A.; Fergusson, D.; Horwood, L.J.; Goodman, R.; Maughn, B.; Moffitt, T.E.; Meltzer, H.; Carroll, J. Differenze sessuali nella disabilità di lettura dello sviluppo. Nuovi risultati da 4 studi epidemiologici. JAMA 2004, 291, 2007–2012. [Google Scholar] [CrossRef] [PubMed]
- Willcutt, E.G.; Pennington, B.F. Psychiatric comorbidity in children and adolescents with reading disability. J. Child Psychol. Psychiatry 2000, 41, 1039–1048. [Google Scholar] [CrossRef] [PubMed]
- Ramus, F. A neurological model of dyslexia and other domain-specific developmental disorders with an associated sensorimotor syndrome. In The Dyslexic Brain: New Pathways in Neuroscience; Rosen, G.D., Ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2006; pp. 75–101. [Google Scholar]
- Démonet, J.F.; Taylor, M.J.; Chaix, Y. Developmental dyslexia. Lancet 2004, 363, 1451–1460. [Google Scholar] [CrossRef]
- Serrano, F.; Delfior, S. Dyslexia in Spanish: The state of the matter. Electron. J. Res. Educ. Psycol. 2004, 2, 13–34. [Google Scholar]
- Galaburda, A.M.; Sherman, G.F.; Rosen, G.D.; Aboitiz, F.; Geschwind, N. Developmental dyslexia: Four consecutive patients with cortical anomalies. Ann. Neurol. 1985, 18, 222–233. [Google Scholar] [CrossRef]
- Shaywitz, S.E.; Shaywitz, B.A.; Pugh, K.R.; Fulbright, R.K.; Constable, R.T.; Mencl, W.E.; Shankweiler, D.P.; Liberman, A.M.; Skudlarski, P.; Fletcher, J.M.; et al. Functional disruption in the organization of the brain for reading in dyslexia. Proc. Natl. Acad. Sci. USA 1998, 95, 2636–2641. [Google Scholar] [CrossRef] [Green Version]
- Snowling, M.J.; Hulme, C. Evidence-based interventions for reading and language difficulties: Creating a virtuous circle. Br. J. Educ. Psychol. 2011, 81 Pt 1, 1–23. [Google Scholar] [CrossRef]
- Paulesu, E.; Démonet, J.F.; Fazio, F.; McCrory, E.; Chanoine, V.; Brunswick, N.; Cappa, S.F.; Cossu, G.; Habib, M.; Frith, C.D.; et al. Dyslexia: Cultural diversity and biological unity. Science 2001, 291, 2165–2167. [Google Scholar] [CrossRef] [Green Version]
- Tallal, P.; Miller, S.L.; Bedi, G.; Byma, G.; Wang, X.; Nagarajan, S.S.; Schreiner, C.; Jenkins, W.M.; Merzenich, M.M. Language comprehension in language-learning impaired children improved with acoustically modified speech. Science 1996, 271, 81–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolson, R.I.; Fawcett, A.J.; Dean, P. Dyslexia, development and the cerebellum. Trends. Neurosci. 2001, 24, 508–511. [Google Scholar] [CrossRef]
- Roach, N.W.; Hogben, J.H. Attentional modulation of visual processing in adult dyslexia a spatial-cuing deficit. Psychol. Sci. 2004, 15, 650–654. [Google Scholar] [CrossRef] [PubMed]
- Facoetti, A.; Zorzi, M.; Cestnick, L.; Lorusso, M.; Molteni, M.; Paganoni, P.; Umiltà, C.; Mascetti, G.G. The relationship between visuo-spatial attention and nonword reading in developmental dyslexia. Cogn. Neuropsychol. 2006, 23, 841–855. [Google Scholar] [CrossRef] [PubMed]
- Bosse, M.; Tainturier, M.; Valdois, S. Developmental dyslexia: The visual attention span deficit hypothesis. Cognition 2007, 104, 198–230. [Google Scholar] [CrossRef] [Green Version]
- Lobier, M.; Zoubrinetzky, R.; Valdois, S. The visual attention span deficit in dyslexia is visual and not verbal. Cortex 2012, 48, 768–773. [Google Scholar] [CrossRef]
- Livingstone, M.S.; Rosen, G.D.; Drislane, F.W.; Galaburda, A.M. Physiological and anatomical evidence for a magnocellular defect in developmental dyslexia. Proc. Natl. Acad. Sci. USA 1991, 88, 7943–7947. [Google Scholar] [CrossRef] [Green Version]
- Stein, J.F.; Walsh, V. To see but not to read; the magnocellular theory of dyslexia. Trends. Neurosci. 1997, 20, 147–152. [Google Scholar] [CrossRef]
- Vidyasagar, T.R.; Pammer, K. Dyslexia: A deficit in visuo-spatial attention, not in phonological processing. Trends Cogn. Sci.. 2009, 14, 57–63. [Google Scholar] [CrossRef]
- Fletcher, J.M. Dyslexia: The evolution of a scientific concept. J. Int. Neuropsychol. Soc. 2009, 15, 501–508. [Google Scholar] [CrossRef] [Green Version]
- Vellutino, F.R.; Fletcher, J.M.; Snowling, M.J.; Scanlon, D.M. Specific reading disability (dyslexia): What have we learned in the past four decades? J. Child Psychol. Psychiatry 2004, 45, 2–40. [Google Scholar] [CrossRef] [PubMed]
- Irlen, H. Successful treatment of learning difficulties. In Proceedings of the 91st Annual Convention of the American Psychological Association, Anaheim, CA, USA, 12 December 1983. [Google Scholar]
- Solan, H.A.; Ficarra, A.; Brannan, J.R.; Rucker, F. Eye movement efficiency in normal and reading disabled elementary school children: Effects of varying luminance and wavelength. J. Am. Optom. Assoc. 1998, 69, 455–464. [Google Scholar] [PubMed]
- Grisham, J.D.; Sheppard, M.M.; Tran, W.U. Visual symptoms and reading performance. Optom. Vis. Sci. 1993, 70, 384–391. [Google Scholar] [CrossRef]
- Hall, S.; Wick, B. The relationship between ocular functions and reading achievement. J. Pediatr. Ophthalmol. Strabismus. 1991, 28, 17–19. [Google Scholar]
- Laver, K.E.; George, S.; Thomas, S.; Deutsch, J.E.; Crotty, M. Virtual reality for stroke rehabilitation. Cochrane Database Syst. Rev. 2015, 2015, CD008349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turolla, A.; Dam, M.; Ventura, L.; Tonin, P.; Agostini, M.; Zucconi, C.; Kiper, P.; Cagnin, A.; Piron, L. Virtual reality for the rehabilitation of the upper limb motor function after stroke: A prospective controlled trial. J. Neuroeng. Rehabil. 2013, 10, 85. [Google Scholar] [CrossRef] [PubMed]
- Forteza-Forteza, D.; Rodríguez-Martín, A.; Álvarez-Arregui, E.; Menéndez Álvarez-Hevia, D. Inclusion, dyslexia, emotional state and learning: Perceptions of Ibero-American children with dyslexia and their parents during the COVID-19 lockdown. Sustainability 2021, 13, 2739. [Google Scholar] [CrossRef]
- Jacobs, L.; Parke, A.; Ziegler, F.; Headleand, C.; De Angeli, A. Learning at school through to university: The educational experiences of students with dyslexia at one UK higher education institution. Disabil. Soc. 2022, 37, 662–683. [Google Scholar] [CrossRef]
- Orsini, A.; Pezzuti, L.; Picone, L. WISC-IV: Contributo Alla Taratura Italiana (WISC-IV Italian); Giunti, O.S.: Florence, Italy, 2012. [Google Scholar]
- Sartori, G.; Job, R. DDE-2: Batteria per la Valutazione della Dislessia e della Disortografia Evolutiva-2 [Assessment Battery for Developmental Reading and Spelling Disorders]; Giunti O.S.: Florence, Italy, 2007. [Google Scholar]
- Istituto Superiore di Sanità. Consensus Conference on Learning Disabilities. 2011. Available online: http://www.snlg-iss.it/cms/files/Cc_Disturbi_Apprendimento_sito.pdf (accessed on 25 July 2022).
- Denckla, M.B.; Rudel, R.G. Rapid “automatized” naming (RAN): Dyslexia differentiated from other learning disabilities. Neuropsychologia 1976, 14, 471–479. [Google Scholar] [CrossRef]
- Poblano, A.; Valadéz-Tepec, T.; Arias, M.D.L.; García-Pedroza, F. Phonological and visuo-spatial working memory alterations in dyslexic children. Arch. Med. Res. 2000, 31, 493–496. [Google Scholar] [CrossRef]
- Rose, F.D.; Brooks, B.M.; Rizzo, A. A Virtual reality in brain damage rehabilitation: Review. Cyberpsychol. Behav. 2005, 8, 241–262. [Google Scholar] [CrossRef] [PubMed]
- Kiper, P.; Szczudlik, A.; Mirek, E.; Nowobilski, R.; Opara, J.; Agostini, M.; Turolla, A. The application of virtual reality in neuro-rehabilitation: Motor re-learning supported by innovative technologies. Med. Rehabil. 2013, 17, 29–36. [Google Scholar] [CrossRef]
- Bohil, C.J.; Alicea, B.; Biocca, F.A. Virtual reality in neuroscience research and therapy. Nat. Rev. Neurosci. 2011, 12, 752–762. [Google Scholar] [CrossRef] [PubMed]
- Anis, M.Y.N.; Normah, C.D.; Mahadir, A.; Norhayati, I.; Rogayah, A.R.; Dzalani, H. Interventions for children with dyslexia: A review on current intervention methods. Med. J. Malays. 2018, 73, 311–320. [Google Scholar]
- Snowling, M.J. Early identification and interventions for dyslexia: A contemporary view. J. Res. Spec. Educ. Needs 2013, 13, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Pecini, C.; Spoglianti, S.; Bonetti, S.; Di Lieto, M.C.; Guaran, F.; Martinelli, A.; Gasperini, F.; Cristofani, P.; Casalini, C.; Mazzotti, S.; et al. Training RAN or reading? A telerehabilitation study on developmental dyslexia. Dyslexia 2019, 25, 318–331. [Google Scholar] [CrossRef]
- Tucci, R.; Savoia, V.; Bertolo, L.; Vio, C.; Tressoldi, P.E. Efficacy and efficiency outcomes of a training to ameliorate developmental dyslexia using the online software Reading Trainer®. BPA-Appl. Psychol. Bull. 2015, 63, 53–60. [Google Scholar]
- Olofsson, Å.; Taube, K.; Ahl, A. Academic Achievement of University Students with Dyslexia. Dyslexia 2015, 21, 338–349. [Google Scholar] [CrossRef]
- Pedroli, E.; Padula, P.; Guala, A.; Meardi, M.T.; Riva, G.; Albani, G. A Psychometric Tool for a Virtual Reality Rehabilitation Approach for Dyslexia. Comput. Math. Methods Med. 2017, 2017, 7048676. [Google Scholar] [CrossRef] [Green Version]
- Cacciante, L.; Pietà, C.D.; Rutkowski, S.; Cieślik, B.; Szczepańska-Gieracha, J.; Agostini, M.; Kiper, P. Cognitive telerehabilitation in neurological patients: Systematic review and meta-analysis. Neurol. Sci. 2021, 43, 1–16. [Google Scholar]
- Maresca, G.; Maggio, M.G.; De Luca, R.; Manuli, A.; Tonin, P.; Pignolo, L.; Calabrò, R.S. Tele-Neuro-Rehabilitation in Italy: State of the Art and Future Perspectives. Front. Neurol. 2020, 11, 563375. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All | EG | CG | p-Value | |
|---|---|---|---|---|
| Participants | 28 | 14 (50.0) | 14 (50.0) | - |
| Male | 13 (46.3) | 7 (50.0) | 6 (42.9) | 0.99 |
| Age (years) | 10.3 (2.0) | 10.5 (2.1) | 10.1 (2.0) | 0.61 |
| Education (years) | 5.2 (1.9) | 5.4 (1.8) | 5.1 (2.0) | 0.67 |
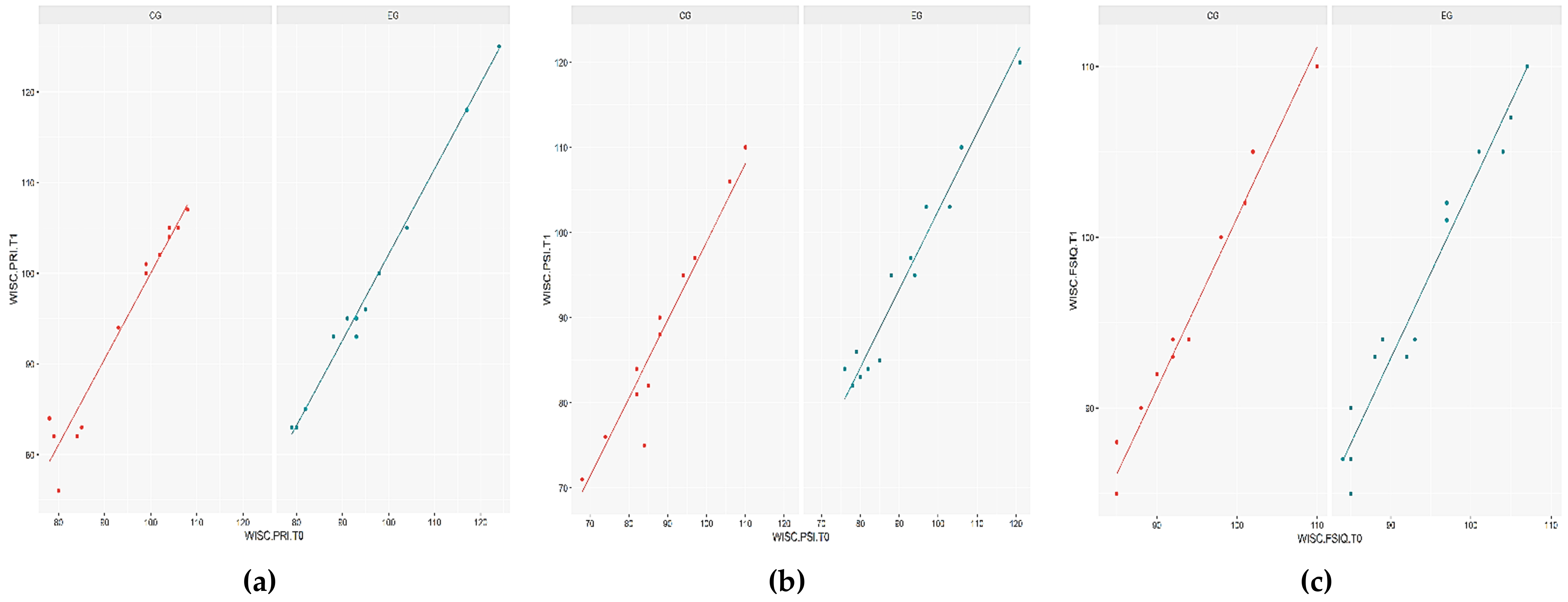
| Clinical Assessment | Group Coefficient | Adjusted R2 | |||
|---|---|---|---|---|---|
| Estimate | Std. Error | t Value | p Value | ||
| VCI | 0.355 | 0.579 | 0.613 | 0.545 | 0.976 |
| PRI | 1.467 | 0.522 | 2.809 | 0.009 | 0.970 |
| WMI | 0.240 | 0.569 | 0.422 | 0.676 | 0.956 |
| PSI | 2.560 | 0.764 | 3.352 | 0.002 | 0.943 |
| FSIQ | 1.263 | 0.411 | 3.071 | 0.005 | 0.965 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maresca, G.; Leonardi, S.; De Cola, M.C.; Giliberto, S.; Di Cara, M.; Corallo, F.; Quartarone, A.; Pidalà, A. Use of Virtual Reality in Children with Dyslexia. Children 2022, 9, 1621. https://doi.org/10.3390/children9111621
Maresca G, Leonardi S, De Cola MC, Giliberto S, Di Cara M, Corallo F, Quartarone A, Pidalà A. Use of Virtual Reality in Children with Dyslexia. Children. 2022; 9(11):1621. https://doi.org/10.3390/children9111621
Chicago/Turabian StyleMaresca, Giuseppa, Simona Leonardi, Maria Cristina De Cola, Silvia Giliberto, Marcella Di Cara, Francesco Corallo, Angelo Quartarone, and Alessandra Pidalà. 2022. "Use of Virtual Reality in Children with Dyslexia" Children 9, no. 11: 1621. https://doi.org/10.3390/children9111621