
Positive Attention Bias Trained during the Rethink Therapeutic Online Game and Related Improvements in Children and Adolescents’ Mental Health
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Procedure
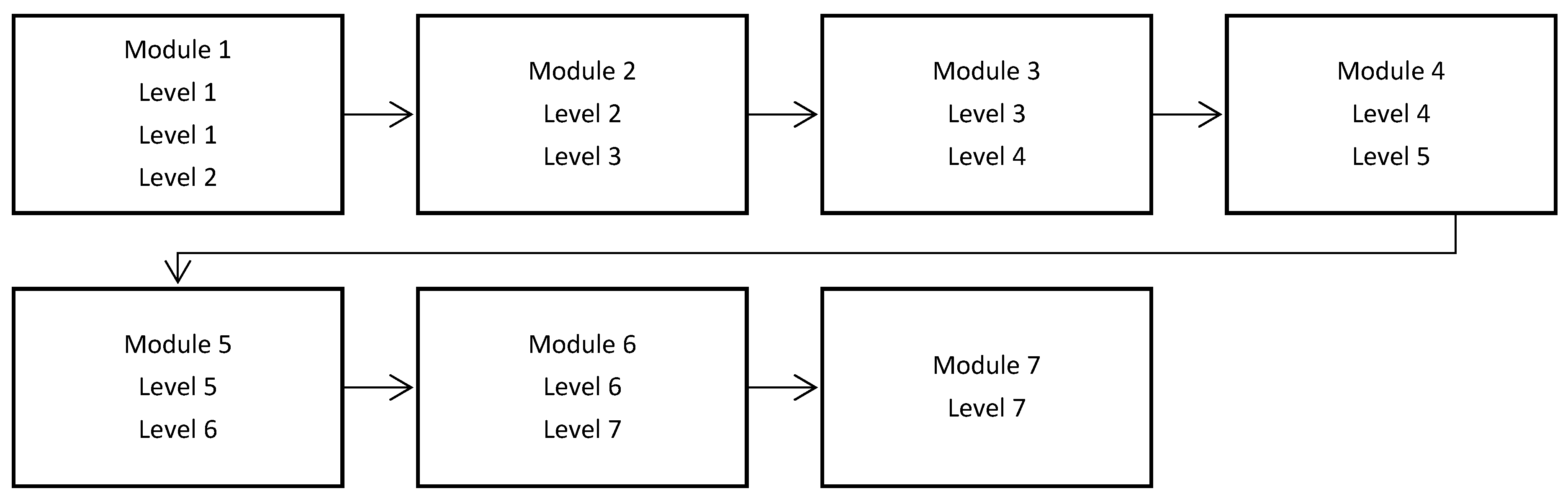
2.2.1. REThink Game
2.2.2. Attentional Bias Training
2.3. Measures
3. Results
3.1. Attentional Bias
3.2. Changes in Attentional Bias and Changes in Psychological Functioning
4. Discussion
5. Limitations and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bar-Haim, Y.; Lamy, D.; Pergamin, L.; Bakermans-Kranenburg, M.J.; van IJzendoorn, M.H. Threat-related attentional bias in anxious and nonanxious individuals: A meta-analytic study. Psychol. Bull. 2007, 133, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Bockstaele, B.; Verschuere, B.; Tibboel, H.; De Houwer, J.; Crombez, G.; Koster, E.H. A review of current evidence for the causal impact of attentional bias on fear and anxiety. Psychol. Bull. 2014, 140, 682. [Google Scholar] [CrossRef] [PubMed]
- Mogg, K.; Waters, A.M.; Bradley, B.P. Attention Bias Modification (ABM): Review of Effects of Multisession ABM Training on Anxiety and Threat-Related Attention in High-Anxious Individuals. Clin. Psychol. Sci. 2017, 5, 698–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mogoaşe, C.; David, D.; Koster, E.H. Clinical efficacy of attentional bias modification procedures: An updated meta-analysis. J. Clin. Psychol. 2014, 70, 1133–1157. [Google Scholar] [CrossRef] [Green Version]
- Carr, I.; Szabó, M. Worry in Children Changing Associations with Fear, Thinking, and Problem-Solving. J. Early Adolesc. 2015, 35, 120–135. [Google Scholar] [CrossRef]
- Dash, S.R.; Meeten, F.; Davey, G.C.L. Systematic information processing style and perseverative worry. Clin. Psychol. Rev. 2013, 33, 1041–1056. [Google Scholar] [CrossRef]
- Kuzucu, Y.; Sariot Ertürk, O.; Şimşek, O.F. Cognitive distortions and problematic internet use connection: Examining the mediator roles of loneliness and social anxiety by partialling out the effects of social desirability. J. Evid.-Based Psychother. 2020, 21, 21–36. [Google Scholar] [CrossRef]
- Stroian, P. Emotional Needs and Schematic Functioning in Depression: A Narrative Review. J. Evid.-Based Psychother. 2021, 21, 21–36. [Google Scholar] [CrossRef]
- Liu, X.; Wang, S.; Zhou, J.; Cai, H. Attention bias training for reducing smartphone addiction in Chinese college student. J. Evid.-Based Psychother. 2020, 20, 1–24. [Google Scholar] [CrossRef]
- Sylvain, H.; Gilbertson, J.; Carlson, M. Single session positive attention bias modification training enhances reward-related electrocortical responses in females. Int. J. Psychophysiol. 2020, 156, 10–17. [Google Scholar] [CrossRef]
- Thoern, H.A.; Grueschow, M.; Ehlert, U.; Ruff, C.C.; Kleim, B. Attentional Bias towards Positive Emotion Predicts Stress Resilience. PLoS ONE 2016, 11, e0148368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dandeneau, S.D.; Baldwin, M.W.; Baccus, J.R.; Sakellaropoulo, M.; Pruessner, J.C. Cutting stress off at the pass: Reducing vigilance and responsiveness to social threat by manipulating attention. J. Pers. Soc. Psychol. 2007, 93, 651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bar-Haim, Y.; Morag, I.; Glickman, S. Training anxious children to disengage attention from threat: A randomized controlled trial. J. Child. Psychol. Psychiatry 2011, 52, 861–869. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association Task Force: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Waters, A.M.; Pittaway, M.; Mogg, K.; Bradley, B.P.; Pine, D.S. Attention training towards positive stimuli in clinically anxious children. Dev. Cogn. Neurosci. 2013, 4, 77–84. [Google Scholar] [CrossRef]
- David, O.A.; Costescu, C.; Cardos, R.; Mogoase, C. How Effective are Serious Games for Promoting Mental Health and Health Behavioral Change in Children and Adolescents? A Systematic Review and Meta-analysis. Child Youth Care Forum 2020, 49, 817–838. [Google Scholar] [CrossRef]
- Diaz-Orueta, U. Serious Games and Gamified Tools for Psychological Intervention: A Review. In Integrating Technology in Positive Psychology Practice. IGI Global: Spain, 2016; pp. 290–314. [Google Scholar] [CrossRef]
- Boendermaker, W.J.; Maceiras, S.S.; Boffo, M.; Wiers, R.W. Attentional bias modification with serious game elements: Evaluating the shots game. JMIR Serious Games 2016, 4, e20. [Google Scholar] [CrossRef] [Green Version]
- Fauth, P. Cognitive bias modification-attention: Training at home with multiple sessions. EWU Masters Thesis Collect. 2016, 342. [Google Scholar]
- Ellis, A. Changing rational-emotive therapy (RET) to rational emotive behavior therapy (REBT). J. Ration. Emot. Cogn. Behav. Ther. 1995, 13, 85–89. [Google Scholar] [CrossRef]
- David, O.A.; Cardos, R.A.I.; Matu, S.A. Is REThink therapeutic game effective in preventing emotional disorders in children and adolescents? Outcomes of a randomized clinical trial. Eur. Child. Adolesc Psychiatry 2019, 28, 111–122. [Google Scholar] [CrossRef]
- David, O.A.; Cardos, R.A.I.; Matu, S.A. Changes in irrational beliefs are responsible for the efficacy of the REThink therapeutic game in preventing emotional disorders in children and adolescents: Mechanisms of change analysis of a randomized clinical trial. Eur Child. Adolesc Psychiatry 2019, 28, 307–318. [Google Scholar] [CrossRef]
- David, O.A.; Stroian, P.I.; Predatu, R.; Maffei, A. State anxiety and frontal alpha asymmetry effects of the REThink online video game for children and adolescents: A six-month follow-up. Personal. Individ. Differ. 2022, 27, R713–R715. [Google Scholar] [CrossRef]
- Staugaard, S.R. Reliability of two versions of the dot-probe task using photographic faces. Psychol. Sci. Q 2009, 51, 339–350. [Google Scholar]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child. Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R.; Meltzer, H.; Bailey, V. The Strengths and Difficulties Questionnaire: A pilot study on the validity of the self-report version. Eur. Child. Adolesc. Psychiatry 1998, 7, 125–130. [Google Scholar] [CrossRef]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef] [Green Version]
- Neamtu, G.M.; David, O.A. Coaching emotional abilities in fostered adolescents through Rational Emotive and Cognitive-Behavioral education: Efficacy and mechanisms of change of using therapeutic stories. J. Evid.-Based Psychother. Spec. Issue Life Coach. 2016, 16, 33–56. [Google Scholar]
- David, D.; Montgomery, G.H.; Macavei, B.; Bovbjerg, D.H. An empirical investigation of Albert Ellis’s binary model of distress. J. Clin. Psychol. 2005, 61, 499–516. [Google Scholar] [CrossRef]
- Notebaert, L.; Grafton, B.; Clarke, P.J.; Rudaizky, D.; Chen, N.T.; MacLeod, C. Emotion-in-Motion, a Novel Approach for the Modification of Attentional Bias: An Experimental Proof-of-Concept Study. JMIR Serious Games 2018, 6, e10993. [Google Scholar] [CrossRef]
- Hakamata, Y.; Lissek, S.; Bar-Haim, Y.; Britton, J.C.; Fox, N.A.; Leibenluft, E.; Ernst, M.; Pine, D.S. Attention bias modification treatment: A meta-analysis toward the establishment of novel treatment for anxiety. Biol. Psychiatry 2010, 68, 982–990. [Google Scholar] [CrossRef] [Green Version]
- Remmerswaal, D.; Muris, P.; Huijding, J. Transmission of Cognitive Bias and Fear From Parents to Children: An Experimental Study. J. Clin. Child. Adolesc Psychol 2015, 45, 642–654. [Google Scholar] [CrossRef]
- Muris, P.; Debipersad, S.; Mayer, B. Searching for Danger: On the Link Between Worry and Threat-Related Confirmation Bias in Children. J. Child. Fam Stud. 2013, 23, 604–609. [Google Scholar] [CrossRef]
- Montagner, R.; Mogg, K.; Bradley, B.P.; Pine, D.S.; Czykiel, M.S.; Miguel, E.C.; Rohde, L.A.; Manfro, G.G.; Salum, G.A. Attentional bias to threat in children at-risk for emotional disorders: Role of gender and type of maternal emotional disorder. Eur Child. Adolesc Psychiatry 2015, 25, 735–742. [Google Scholar] [CrossRef] [PubMed]
- David, O.A. The Rational Parenting Coach App: Rethink Parenting! A Mobile Parenting Program for Offering Evidence-Based Personalized Support in the Prevention of Child Externalizing and Internalizing Disorders. J. Evid.-Based Psychother. 2019, 19, 97–108. [Google Scholar]
- Barrio, M.; Martinez-Pampliega, A.; Merino Ramos, L. Mindful Parenting: A Pilot Study of The “Brief Mindfulness Intervention Program” (Bmip) in the Educational Context. J. Evid.-Based Psychother. 2020, 20, 23–36. [Google Scholar] [CrossRef]
- David, O.A.; Predatu, R.; Cardos, R. A pilot study of the REThink online video game applied for coaching emotional understanding in children and adolescents in the therapeutic video game environment: The Feeling Better resources game. J. Evid.-Based Psychother. 2018, 18, 57–68. [Google Scholar] [CrossRef]
- David, O.A.; Magurean, S.; Tomoiagă, C. Do Improvements in Therapeutic Game-Based Skills Transfer to Real Life Improvements in Children’s Emotion-Regulation Abilities and Mental Health? A Pilot Study That Offers Preliminary Validity of the REThink In-game Performance Scoring. Front. Psychiatry 2022, 13, 828. [Google Scholar] [CrossRef]
- Shima, T.; Inoue, K.; Muto, T.; Kumano, H. Measuring momentary experiential avoidance in daily life: A preliminary investigation for a new contingency-based measurement framework. J. Evid.-Based Psychother. 2021, 20, 24–32. [Google Scholar] [CrossRef]
- Bintaş-Zörer, P.; Yorulmaz, O. A new instrument for assessment of emotion regulation: The emotion regulation interview-revised form. J. Evid.-Based Psychother. 2021, 20, 32–40. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | M1(SD) | M2(SD) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | AB | -- | 4.13 (0.96) | 3.96 (1.00) | ||||||||
| 2 | SDQ-ES | 0.14 | -- | |||||||||
| 3 | SDQ-CP | 0.48 ** | 0.49 ** | -- | ||||||||
| 4 | SDQ-H | 0.33 * | 0.41 ** | 0.51 ** | -- | |||||||
| 5 | SDQ-PR | 0.36 * | 0.40 ** | 0.37 * | 0.31 * | -- | ||||||
| 6 | SDQ-PS | 0.09 | −0.07 | −0.23 | −0.14 | −0.23 | -- | |||||
| 7 | FD-CMS-F | −0.09 | 0.49 ** | −0.18 | 0.04 | 0.15 | 0.29 * | -- | ||||
| 8 | FD-CMS-DF | −0.28 * | 0.16 | −0.24 | −0.08 | −0.04 | 0.26 | 0.40 ** | -- | |||
| 9 | FD-CMS-P | −0.02 | −0.26 | −0.17 | −0.13 | −0.18 | 0.50 ** | 0.05 | 0.05 | -- |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
David, O.A.; Magurean, S. Positive Attention Bias Trained during the Rethink Therapeutic Online Game and Related Improvements in Children and Adolescents’ Mental Health. Children 2022, 9, 1600. https://doi.org/10.3390/children9111600
David OA, Magurean S. Positive Attention Bias Trained during the Rethink Therapeutic Online Game and Related Improvements in Children and Adolescents’ Mental Health. Children. 2022; 9(11):1600. https://doi.org/10.3390/children9111600
Chicago/Turabian StyleDavid, Oana A., and Silvia Magurean. 2022. "Positive Attention Bias Trained during the Rethink Therapeutic Online Game and Related Improvements in Children and Adolescents’ Mental Health" Children 9, no. 11: 1600. https://doi.org/10.3390/children9111600