
Parents’ Perspectives on Adaptive Sports in Children with Profound Intellectual and Multiple Disabilities


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Selection Criteria
2.3. Questionnaire
2.4. Recruitment
2.5. Clinical Data
2.6. Statistics
3. Results
3.1. General Information
3.2. Effects of Adaptive Sports
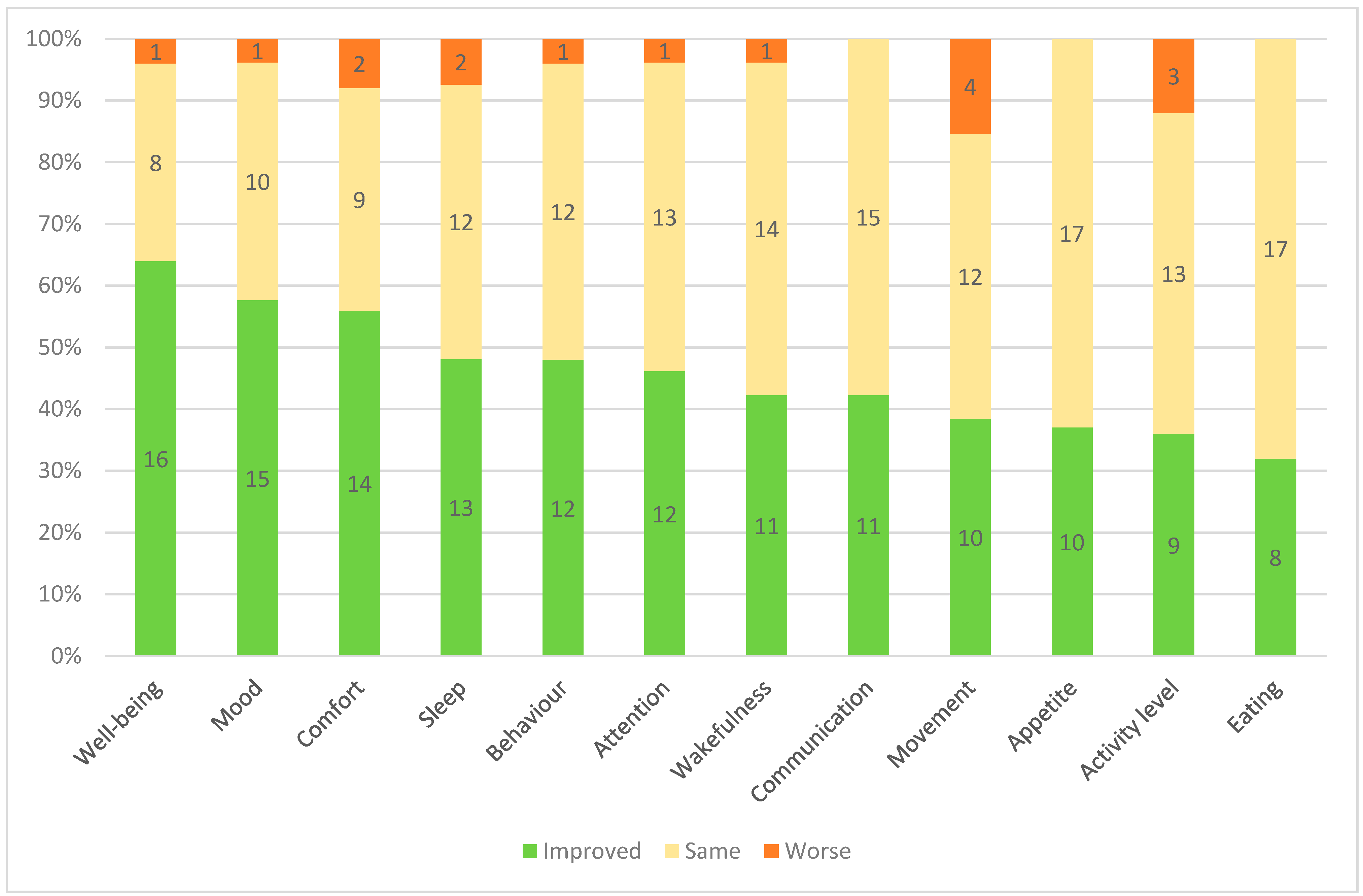
3.2.1. Effects by Domain
- Quality of life:
- Mental functions:
- Sleep and arousal:
- Appetite and eating:
- Spontaneous movement and activity:
3.2.2. Association Analyses
3.2.3. Ideal Duration and Frequency of Sessions
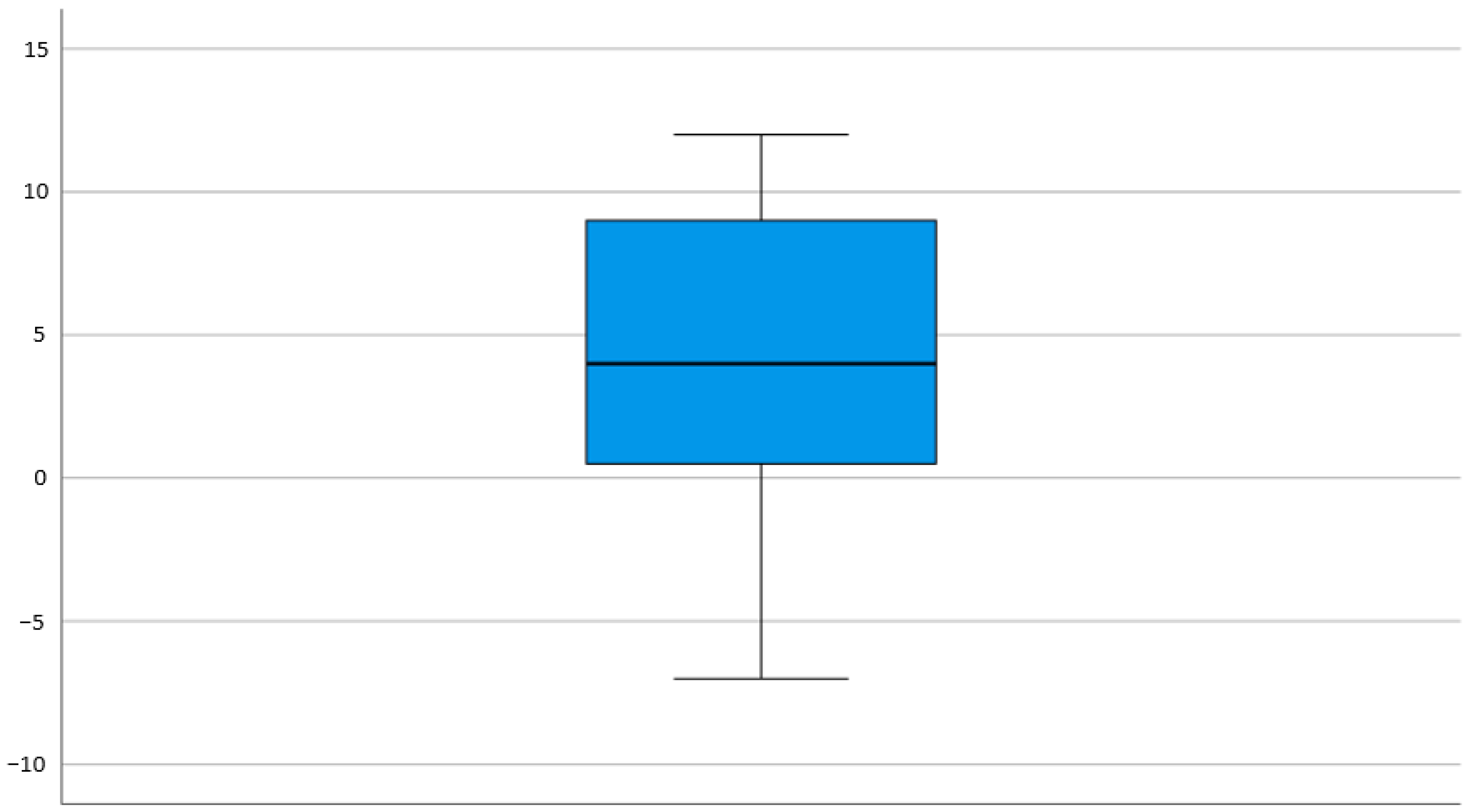
3.2.4. Composite Score
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jaarsma, E.A.; Dijkstra, P.U.; de Blecourt, A.C.; Geertzen, J.H.; Dekker, R. Barriers and facilitators of sports in children with physical disabilities: A mixed-method study. Disabil. Rehabil. 2015, 37, 1617–1623. [Google Scholar] [CrossRef]
- Emonson, C.; McGillivray, J.; Kothe, E.J.; Rinehart, N.; Papadopoulos, N. Class Time Physical Activity Programs for Primary School Aged Children at Specialist Schools: A Systematic Mapping Review. Int. J. Environ. Res. Public Health 2019, 16, 5140. [Google Scholar] [CrossRef] [Green Version]
- Shields, N.; Synnot, A.J. An exploratory study of how sports and recreation industry personnel perceive the barriers and facilitators of physical activity in children with disability. Disabil. Rehabil. 2014, 36, 2080–2084. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.; Roberts, R.; Bowman, G.; Crettenden, A. Barriers and facilitators to physical activity participation for children with physical disability: Comparing and contrasting the views of children, young people, and their clinicians. Disabil. Rehabil. 2019, 41, 1499–1507. [Google Scholar] [CrossRef] [PubMed]
- Nakken, H.; Vlaskamp, C. A Need for a Taxonomy for Profound Intellectual and Multiple Disabilities. J. Policy Pract. Intellect. Disabil. 2007, 4, 83–87. [Google Scholar] [CrossRef]
- Petigas, L.; Newman, C.J. Paediatricians’ Views on Pain in Children with Profound Intellectual and Multiple Disabilities. Brain Sci. 2021, 11, 408. [Google Scholar] [CrossRef] [PubMed]
- Arvio, M.; Sillanpaa, M. Prevalence, aetiology and comorbidity of severe and profound intellectual disability in Finland. J. Intellect. Disabil. Res. 2003, 47, 108–112. [Google Scholar] [CrossRef] [Green Version]
- Hogg, J.; Juhlberg, K.; Lambe, L. Policy, service pathways and mortality: A 10-year longitudinal study of people with profound intellectual and multiple disabilities. J. Intellect. Disabil. Res. 2007, 51, 366–376. [Google Scholar] [CrossRef] [PubMed]
- Holenweg-Gross, C.; Newman, C.J.; Faouzi, M.; Poirot-Hodgkinson, I.; Berard, C.; Roulet-Perez, E. Undernutrition in children with profound intellectual and multiple disabilities (PIMD): Its prevalence and influence on quality of life. Child Care Health Dev. 2014, 40, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Waninge, A.; van der Putten, A.A.; Stewart, R.E.; Steenbergen, B.; van Wijck, R.; van der Schans, C.P. Heart rate and physical activity patterns in persons with profound intellectual and multiple disabilities. J. Strength Cond. Res. 2013, 27, 3150–3158. [Google Scholar] [CrossRef] [PubMed]
- Ohwada, H.; Nakayama, T.; Ishikawa-Takata, K.; Iwasaki, N.; Kanaya, Y.; Tanaka, S. Total energy expenditure among children with motor, intellectual, visual, and hearing disabilities: A doubly labeled water method. Eur. J. Clin. Nutr. 2021. [Google Scholar] [CrossRef]
- Tow, S.; Gober, J.; Nelson, M.R. Adaptive Sports, Arts, Recreation, and Community Engagement. Phys. Med. Rehabil. Clin. N. Am. 2020, 31, 143–158. [Google Scholar] [CrossRef]
- Barak, S.; Mendoza-Laiz, N.; Fuentes, M.T.G.; Rubiera, M.; Huyzler, Y. Psychosocial effects of competitive Boccia program in persons with severe chronic disability. J. Rehabil. Res. Dev. 2016, 53, 973–988. [Google Scholar] [CrossRef]
- Lai, C.J.; Liu, W.Y.; Yang, T.F.; Chen, C.L.; Wu, C.Y.; Chan, R.C. Pediatric aquatic therapy on motor function and enjoyment in children diagnosed with cerebral palsy of various motor severities. J. Child Neurol. 2015, 30, 200–208. [Google Scholar] [CrossRef]
- Dirienzo, L.N.; Dirienzo, L.T.; Baceski, D.A. Heart rate response to therapeutic riding in children with cerebral palsy: An exploratory study. Pediatr. Phys. Ther. Off. Publ. Sect. Pediatrics Am. Phys. Ther. Assoc. 2007, 19, 160–165. [Google Scholar] [CrossRef]
- Degache, F.; Bonjour, A.; Michaud, D.; Mondada, L.; Newman, C.J. The effects of tandem skiing on posture and heart rate in children with profound intellectual and multiple disabilities. Dev. Neurorehabil. 2019, 22, 234–239. [Google Scholar] [CrossRef]
- Conatser, P.; James, E.; Karabulut, U. Adapted Aquatics for Children with Severe Motor Impairments. Int. J. Aquat. Res. Educ. 2018, 10, 5. [Google Scholar] [CrossRef] [Green Version]
- Joelette. Available online: https://www.joeletteandco.com/en/exclusive-manufacturer-of-the-joelette-all-terrain-chair/joelette-monoroue/ (accessed on 6 September 2021).
- Kruithof, K.; Willems, D.; van Etten-Jamaludin, F.; Olsman, E. Parents’ knowledge of their child with profound intellectual and multiple disabilities: An interpretative synthesis. J. Appl. Res. Intellect. Disabil. 2020, 33, 1141–1150. [Google Scholar] [CrossRef] [PubMed]
- Diener, E.; Napa Scollon, C.; Lucas, R.E. The Evolving Concept of Subjective Well-Being: The Multifaceted Nature of Happiness. In Assessing Well-Being: The Collected Works of Ed Diener; Diener, E., Ed.; Springer: Dordrecht, The Netherlands, 2009; pp. 67–100. [Google Scholar] [CrossRef]
- Aitchison, B.; Rushton, A.B.; Martin, P.; Barr, M.; Soundy, A.; Heneghan, N.R. The experiences and perceived health benefits of individuals with a disability participating in sport: A systematic review and narrative synthesis. Disabil. Health J. 2021, 101164. [Google Scholar] [CrossRef] [PubMed]
- Bjørnarå, H.B.; Westergren, T.; Sejersted, E.; Torstveit, M.K.; Hansen, B.H.; Berntsen, S.; Bere, E. Does organized sports participation in childhood and adolescence positively influence health? A review of reviews. Prev. Med. Rep. 2021, 23, 101425. [Google Scholar] [CrossRef] [PubMed]
- Carter, T.; Pascoe, M.; Bastounis, A.; Morres, I.D.; Callaghan, P.; Parker, A.G. The effect of physical activity on anxiety in children and young people: A systematic review and meta-analysis. J. Affect. Disord. 2021, 285, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Isaksson, J.; Selinus, E.N.; Åslund, C.; Nilsson, K.W. Physical activity in early adolescence predicts depressive symptoms 3 years later: A community-based study. J. Affect. Disord. 2020, 277, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Matta, P.N.; Baul, T.D.; Loubeau, K.; Sikov, J.; Plasencia, N.; Sun, Y.; Spencer, A.E. Low sports participation is associated with withdrawn and depressed symptoms in urban, school-age children. J. Affect. Disord. 2021, 280, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Pirnes, K.P.; Kallio, J.; Kankaanpää, A.; Häkkinen, A.; Tammelin, T. Associations of neck and shoulder pain with objectively measured physical activity and sedentary time among school-aged children. Scand. J. Pain 2020, 20, 821–827. [Google Scholar] [CrossRef] [PubMed]
- van den Heuvel, M.M.; Jansen, P.W.; Bindels, P.J.E.; Bierma-Zeinstra, S.M.A.; van Middelkoop, M. Musculoskeletal pain in 6-year-old children: The Generation R Study. Pain 2020, 161, 1278–1285. [Google Scholar] [CrossRef]
- Vierola, A.; Suominen, A.L.; Lindi, V.; Viitasalo, A.; Ikävalko, T.; Lintu, N.; Väistö, J.; Kellokoski, J.; Närhi, M.; Lakka, T.A. Associations of Sedentary Behavior, Physical Activity, Cardiorespiratory Fitness, and Body Fat Content With Pain Conditions in Children: The Physical Activity and Nutrition in Children Study. J. Pain 2016, 17, 845–853. [Google Scholar] [CrossRef]
- Ohmichi, Y.; Ohmichi, M.; Tashima, R.; Osuka, K.; Fukushige, K.; Kanikowska, D.; Fukazawa, Y.; Yawo, H.; Tsuda, M.; Naito, M.; et al. Physical disuse contributes to widespread chronic mechanical hyperalgesia, tactile allodynia, and cold allodynia through neurogenic inflammation and spino-parabrachio-amygdaloid pathway activation. Pain 2020, 161, 1808–1823. [Google Scholar] [CrossRef]
- Haverkamp, B.F.; Wiersma, R.; Vertessen, K.; van Ewijk, H.; Oosterlaan, J.; Hartman, E. Effects of physical activity interventions on cognitive outcomes and academic performance in adolescents and young adults: A meta-analysis. J. Sports Sci. 2020, 38, 2637–2660. [Google Scholar] [CrossRef]
- Dolezal, B.A.; Neufeld, E.V.; Boland, D.M.; Martin, J.L.; Cooper, C.B. Interrelationship between Sleep and Exercise: A Systematic Review. Adv. Prev. Med. 2017, 2017, 1364387. [Google Scholar] [CrossRef] [PubMed]
- Kredlow, M.A.; Capozzoli, M.C.; Hearon, B.A.; Calkins, A.W.; Otto, M.W. The effects of physical activity on sleep: A meta-analytic review. J. Behav. Med. 2015, 38, 427–449. [Google Scholar] [CrossRef]
- Hulst, R.Y.; Gorter, J.W.; Voorman, J.M.; Kolk, E.; Van Der Vossen, S.; Visser-Meily, J.M.A.; Ketelaar, M.; Pillen, S.; Verschuren, O. Sleep problems in children with cerebral palsy and their parents. Dev. Med. Child Neurol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Verschuren, O.; Hulst, R.Y.; Voorman, J.; Pillen, S.; Luitwieler, N.; Dudink, J.; Gorter, J.W. 24-hour activity for children with cerebral palsy: A clinical practice guide. Dev. Med. Child Neurol. 2021, 63, 54–59. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child. Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Boe, A.J.; Koch, L.L.M.; O’Brien, M.K.; Shawen, N.; Rogers, J.A.; Lieber, R.L.; Reid, K.J.; Zee, P.C.; Jayaraman, A. Automating sleep stage classification using wireless, wearable sensors. NPJ Digit. Med. 2019, 2, 131. [Google Scholar] [CrossRef] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neyroud, M.C.; Newman, C.J. Parents’ Perspectives on Adaptive Sports in Children with Profound Intellectual and Multiple Disabilities. Children 2021, 8, 815. https://doi.org/10.3390/children8090815
Neyroud MC, Newman CJ. Parents’ Perspectives on Adaptive Sports in Children with Profound Intellectual and Multiple Disabilities. Children. 2021; 8(9):815. https://doi.org/10.3390/children8090815
Chicago/Turabian StyleNeyroud, Marion C., and Christopher J. Newman. 2021. "Parents’ Perspectives on Adaptive Sports in Children with Profound Intellectual and Multiple Disabilities" Children 8, no. 9: 815. https://doi.org/10.3390/children8090815