
Does Maternal Mental Health and Maternal Stress Affect Preschoolers’ Behavioral Symptoms?

Abstract
:1. Introduction
1.1. Depressive Symptomatology in Mothers and Its Impact on Children’s Socioemotional Development
1.2. Parental Stress in Mothers and Its Impact on the Child’s Socioemotional Development
1.3. Vulnerable Contexts, Children’s Socioemotional Development, and Maternal Mental Health
2. Methods
2.1. Participants and Procedures
2.2. Sociodemographic Data
2.3. Missing Cases
3. Results
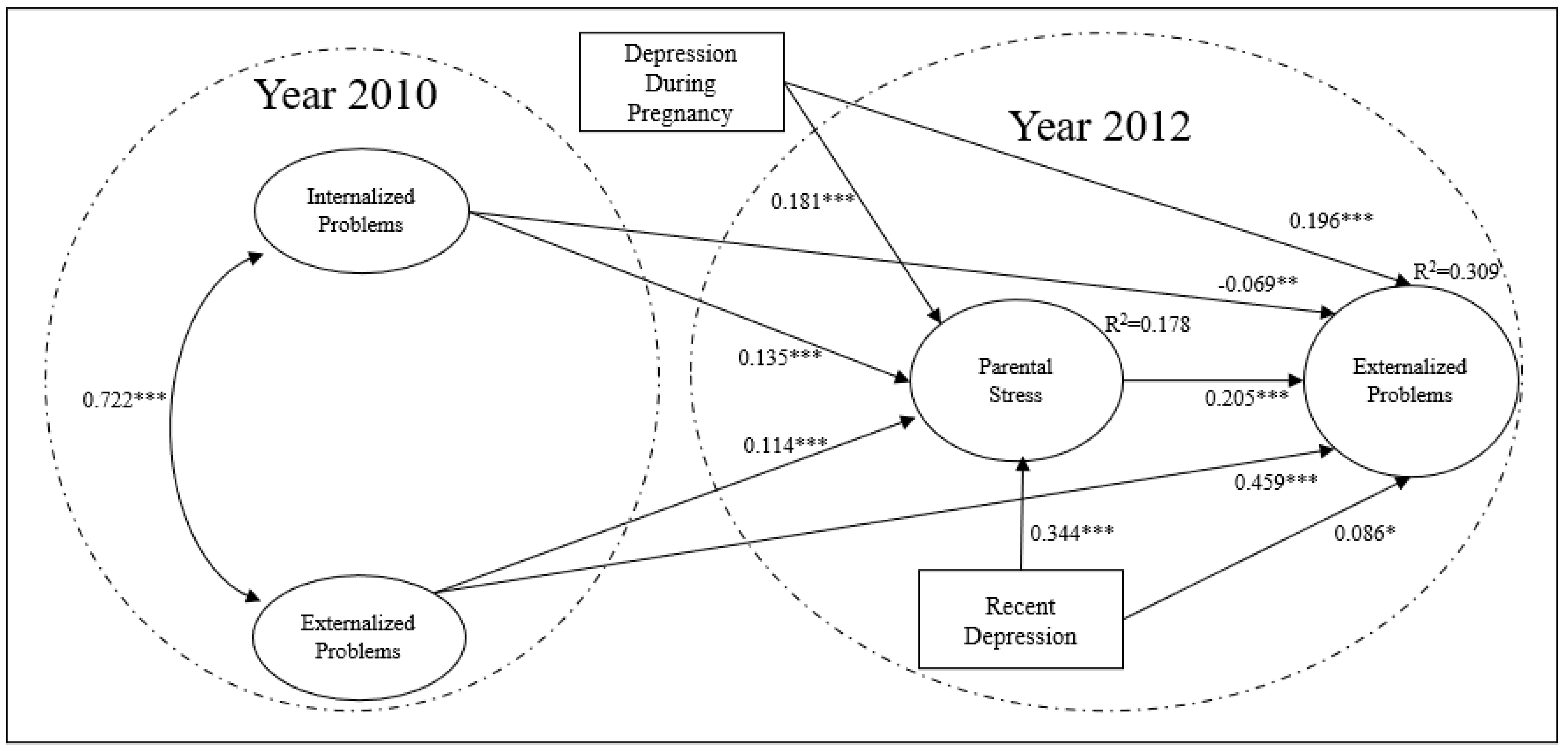
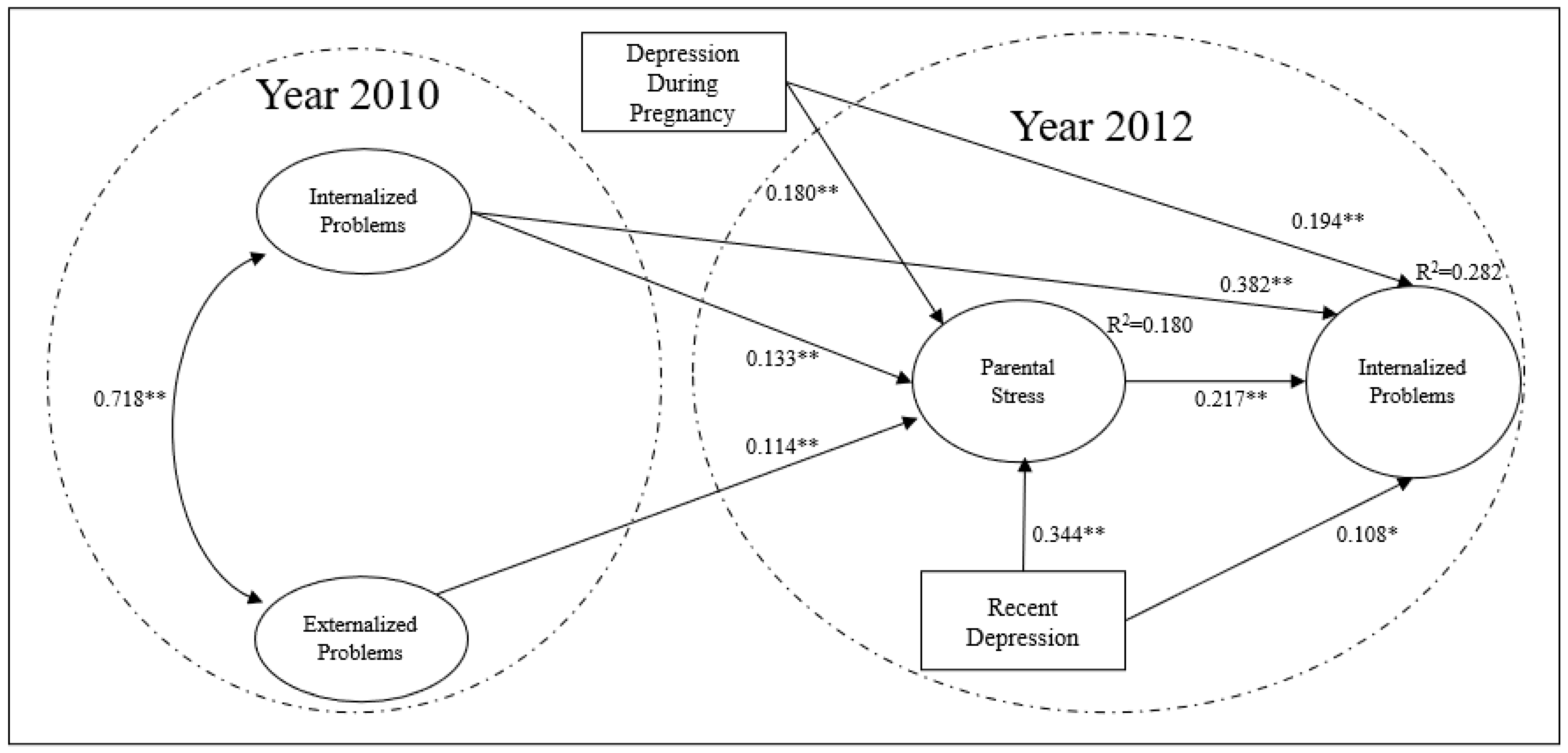
Analysis of the Hypothesized Model
4. Discussion
5. Key Messages
- Maternal mental health affects children’s socioemotional development and is related to internalizing and externalizing problems in early infancy.
- It is fundamental to address maternal mental health in public health service during child medical assistance and in educational system.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Castro, P. Depresión Materna y desarrollo infantil. Rev. Inst. Chil. Ter. Fam. 2011, 20, 91–95. [Google Scholar]
- Lefkovics, E.; Baji, I.; Rigo, J. Impact of maternal depression on pregnancies and on early attachment. Infant Ment. Health J. 2014, 35, 354–365. [Google Scholar] [CrossRef]
- Ministerios de Salud. Guía Clínica AUGE, Depresión en Personas de 15 Años y Más; MINSAL: Santiago, Chile, 2013. [Google Scholar]
- Farkas, C.; Valdés, N. Maternal stress and perceptions of self-efficacy in socioeconomically disadvantaged mothers: An explicative model. Infant Behav. Dev. 2010, 33, 654–662. [Google Scholar] [CrossRef]
- Ménard, C.; Hodes, G.; Russo, S. Pathogenesis of depression: Insights from human and rodent studies. Neuroscience 2016, 321, 138–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, L.; Zhao, Y.; Wang, Y.; Liu, L.; Zhang, X.; Li, B.; Cui, R. The Effects of Psychological Stress on Depression. Curr. Neuropharmacol. 2015, 13, 494–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abidin, R. Parenting Stress Index; Psychological Assessment Resources: Odessa, Ukraine, 1995. [Google Scholar]
- Ôstberg, M.; Hagekull, B. A structural modeling approach to the understanding of parenting stress. J. Clin. Child Psychol. 2000, 29, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Webster-Stratton, C. Stress: A potential disruptor of parent perceptions and family interactions. J. Clin. Child Psychol. 1990, 19, 302–312. [Google Scholar] [CrossRef]
- Behrman, J. Investment in Education—Inputs and Incentives. In Handbook of Development Economics; Elsevier: Amsterdam, The Netherlands, 2010; Volume 5, pp. 4883–4975. [Google Scholar]
- American Psychiatric Association. DSM-5 task force. In Diagnostic and Statistical Manual of Mental Disorders: DSM-5™, 5th ed.; American Psychiatric Publishing Inc.: Arlington, VA, USA, 2013. [Google Scholar]
- Callender, K.; Olson, S.; Choe, D.; Sameroff, A. The effects of parental depressive symptoms, appraisals, and physical punishment on later child externalizing behavior. J. Abnorm. Child Psychol. 2012, 40, 471–483. [Google Scholar] [CrossRef] [Green Version]
- Cuervo, Á. Parenting styles and socioaffective development in childhood. Divers. Perspect. Psicol. 2010, 6, 111–121. [Google Scholar]
- Lindhorst, T.; Oxford, M. The long-term effects of intimate partner violence on adolescent mothers’ depressive symptoms. Soc. Sci. Med. 2008, 66, 1322–1333. [Google Scholar] [CrossRef] [Green Version]
- Fritsch, R.; Montt, M.; Solfs, J.; Pilowsky, D.; Rojas, C. ¿Cómo es la salud mental de los hijos de madres deprimidas consultantes a servicios de atención primaria? Rev. Médica Chile 2007, 135, 602–612. [Google Scholar] [CrossRef]
- Maughan, A.; Cicchetti, D.; Toth, S.; Rogosch, F. Early-occurring maternal depression and maternal negativity in predicting young children’s emotion regulation and socioemotional difficulties. J. Abnorm. Psychol. 2007, 35, 685–703. [Google Scholar] [CrossRef]
- Frick, P.; Morris, A. Temperament and developmental pathways to conduct problems. J. Clin. Child Adolesc. Psychol. 2004, 33, 54–68. [Google Scholar] [CrossRef]
- Chess, S.; Thomas, A. The New York Longitudinal Study (NYLS): The young adult period. Can. J. Psychiatry 1990, 35, 557–561. [Google Scholar] [CrossRef] [PubMed]
- Plomin, R.; DeFries, J.; Knopik, V.; Neiderhiser, J. Top 10 Replicated Findings from Behavioral Genetics. Perspect. Psychol. Sci. 2016, 11, 3–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Díaz-Herrero, A.; Brito de la Nuez, A.; López, J.; Pérez-López, J.; Martínez-Fuentes, M. Estructura factorial y consistencia interna de la versión española del Parenting Stress Index-Short Form. Psicothema 2010, 22, 1033–1038. [Google Scholar]
- Oliva, L.; Montero, J.; Gutiérrez, M. Relación entre el estrés parental y la del niño preescolar. Psicol. Salud 2006, 16, 171–178. [Google Scholar]
- Olhaberry, M.; Farkas, C. Estrés materno y configuración familiar: Estudio comparativo en familias chilenas monoparentales y nucleares de bajos ingresos. Univ. Psychol. 2012, 11, 1317–1326. [Google Scholar] [CrossRef]
- Crnic, K.; Gaze, C.; Hoffman, C. Cumulative parenting stress across the preschool period: Relations to maternal parenting and child behaviour at age 5. Infant Child Development. Int. J. Res. Pract. 2005, 14, 117–132. [Google Scholar]
- Deater-Deckard, K. Parenting Stress and Child Adjustment: Some Old Hypotheses and New Questions. Clin. Psychol. Sci. Pract. 1998, 5, 314–332. [Google Scholar] [CrossRef]
- Pérez, J.; Menéndez, S. Un análisis tipológico del estrés parental en familias en riesgo psicosocial. Salud Ment. 2014, 37, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Del Barrio, V.; Carrasco, M. Adaptación del CDI, Inventario de Depresión Infantil de Maria Kovacs; TEA: Madrid, Spain, 2004. [Google Scholar]
- Elias, M.; Arnold, H.; Hussey, C. (Eds.) EQ + IQ = Best Leadership Practices for Caring and Successful Schools; Corwin Press: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Long, C.; Gurka, M.; Blackman, J. Family Stress and Children’s Language and Behavior Problems: Results from the National Survey of Children’s Health. Top. Early Child. Spec. Educ. 2008, 28, 148–157. [Google Scholar] [CrossRef]
- Aláez, M.; Martínez-Arias, R.; Rodríguez-Sutil, C. Prevalencia de trastornos psicológicos en niños y adolescentes, su relación con la edad y género. Psicothema 2000, 12, 525–532. [Google Scholar]
- Andrade, P.; Betancourt, O. Factores individuales, familiares y sociales y conductas de riesgo en adolescentes. In Investigaciones Psicosociales en Adolescentes; En Andrade, P.P., Cañas, M.J.L., Betancourt, O.D., Eds.; Unicach: Tuxtla Gutierrez, Mexico, 2008; pp. 181–213. [Google Scholar]
- Bragado, C.; Carrasco, I.; Sánchez-Bernardos, M.; Bersabé, R.; Loriga, A.; Monsalve, T. Prevalencia de los trastornos psicopatológicos en niños y adolescentes: Resultados preliminares. Clínica Salud 1995, 6, 67–82. [Google Scholar]
- Khawaja, M.; Barazi, R.; Linos, N. Maternal cultural participation and child health status in a Middle Eastern context: Evidence from an urban health study. Child Care Health Dev. 2007, 33, 117–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OECD Annual Report. 2009. Available online: https://www.oecd.org/newsroom/43125523.pdf (accessed on 20 July 2021).
- Rodriguez, C.; Muñoz, J. Rezago en el desarrollo infantil: La importancia de la calidad educativa del ambiente familiar. Rev. Int. Investig. Cienc. Soc. 2017, 13, 253–270. [Google Scholar] [CrossRef]
- Ministerio de Salud. Informe Encuesta Nacional de Salud, ENS 2009–2011; MINSAL: Santiago, Chile, 2011. [Google Scholar]
- Ulloa, N.; Cova, F.; Bustos, C. Nivel Socioeconómico y conductas externalizadas en preescolares: El rol del mediador parental. Rev. Chil. Pediatría 2016, 88, 340–347. [Google Scholar] [CrossRef] [Green Version]
- Encuesta Longitudinal de Primera Infancia (ELPI) (2010, 2012). Available online: http://observatorio.ministeriodesarrollosocial.gob.cl/elpi-primera-ronda (accessed on 20 July 2021).
- Kolenikov, S.; Angeles, G. Socioeconomic status measurement with discrete proxy variables: Is principal component analysis a reliable answer? Rev. Income Wealth 2009, 55, 128–165. [Google Scholar] [CrossRef] [Green Version]
- Lecannelier, F.; Ewert, J.; Groissman, S.; Gallardo, D.; Bardet, A.; Bascuñan, A.; Rodríguez, J. Validación del Inventario de Conductas Infantiles para niños de entre 1½-5 años (CBCL 1½-5) en la Ciudad de Santiago de Chile. Univ. Psychol. 2014, 13, 491–500. [Google Scholar] [CrossRef] [Green Version]
- Mesman, J.; Bongers, I.; Koot, H. Preschool developmental pathways to preadolescent internalizing and externalizing problems. J. Child Psychol. Psychiatry Allied Discip. 2001, 42, 679–689. [Google Scholar] [CrossRef]
- Luo, J.; Wang, M.C.; Gao, Y.; Zeng, H.; Yang, W.; Chen, W.; Zhao, S.; Qi, S. Refining the Parenting Stress Index—Short Form (PSI-SF) in Chinese Parents. Assessment 2019, 28, 551–566. [Google Scholar] [CrossRef] [PubMed]
- Whiteside-Mansell, L.; Ayoub, C.; McKelvey, L.; Faldowski, R.A.; Hart, A.; Shears, J. Parenting stress of low-income parents of toddlers and preschoolers: Psychometric properties of a short form of the Parenting Stress Index. Parenting 2007, 7, 26–56. [Google Scholar] [CrossRef]
- Mills, R.S.L.; Hastings, P.D.; Helm, J.; Serbin, L.A.; Etezadi, J.; Stack, D.M.; Schwartzman, A.E.; Li, H.H. Temperamental, parental, and contextual contributors to early-emerging internalizing problems: A new integrative analysis approach. Soc. Dev. 2012, 21, 229–253. [Google Scholar] [CrossRef]
- Rosseel, Y. Lavaan: An R Package for Structural Equation. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Rhemtulla, M.; Brosseau-Liard, P.; Savalei, V.; Appelbaum, M.I.; Maxwell, S.E. When Can Categorical Variables Be Treated as Continuous? A Comparison of Robust Continuous and Categorical SEM Estimation Methods under Suboptimal Conditions. Psychol. Methods 2012, 17, 354–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sobel, M.E. Asymptotic confidence intervals for indirect effects in structural equation models. Sociol. Methodol. 1982, 13, 290–312. [Google Scholar] [CrossRef]
- Shrout, P.; Bolger, N. Mediation in Experimental and Nonexperimental Studies: New Procedures and Recommendations. Psychol. Methods 2002, 7, 422–445. [Google Scholar] [CrossRef]
- Psychogiou, L.; Parry, E. Why do depressed individuals have difficulties in their parenting role? Psychol. Med. 2014, 44, 1345–1347. [Google Scholar] [CrossRef] [Green Version]
- Field, T. Prenatal Depression Risk Factors, Developmental Effects and Interventions: A Review. J. Pregnancy Child Health 2017, 4, 301. [Google Scholar] [CrossRef] [PubMed]
- Hallers-Haalboom, E.; Mesman, J.; Groeneveld, M.; Endendijk, J.; van Berkel, S.; van der Pol, L.; Bakermans-Kranenburg, M. Mothers, fathers, sons and daughters: Parental sensitivity in families with two children. J. Fam. Psychol. 2014, 28, 138. [Google Scholar] [CrossRef] [Green Version]
- Olhaberry, M. Early interactions and child gender in Chilean single mother families. Rev. Latinoam. Psicol. 2012, 44, 76–86. [Google Scholar]



{kind=link}
{kind=link}
| N = 6335 | |
|---|---|
| Sex of the child | |
| Boy | 3172 (50.1%) |
| Girl | 3163 (49.9%) |
| Occupational status | |
| Inactive | 2879 (45.4%) |
| Unemployed | 318 (5.0%) |
| In employment | 3138 (49.5%) |
| Educational level | |
| Incomplete schooling | 1079 (17.1%) |
| Full schooling | 3987 (63.1%) |
| Incomplete higher education | 552 (8.7%) |
| Full higher education | 701 (11.1%) |
| SES | |
| Quintile I | 1199 (18.9%) |
| Quintile II | 1265 (20.0%) |
| Quintile III | 1265 (20.0%) |
| Quintile IV | 1359 (21.5%) |
| Quintile V | 1247 (19.7%) |
| Cases with Complete Data | Cases with Missing Data | % of Missing Data | |
|---|---|---|---|
| Parental stress | 5655 | 680 | 10.73% |
| Internalized problems, 2012 | 6073 | 262 | 4.13% |
| Externalized problems, 2012 | 6077 | 258 | 4.07% |
| Postpartum depression | 6254 | 81 | 1.27% |
| Internalized problems, 2010 | 6316 | 19 | 0.29% |
| Externalized problems, 2010 | 6316 | 19 | 0.29% |
| Recent depression | 6317 | 18 | 0.27% |
| Scholarship | 6319 | 16 | 0.25% |
| Initial Sample (N = 6335) | Sample with Complete Data (N = 5302) | p Value | |
|---|---|---|---|
| Sex of the child | 0.948 | ||
| Boy | 3172 (50.1%) | 2658 (50.1%) | |
| Girl | 3163 (49.9%) | 2644 (49.9%) | |
| Occupational status | 0.623 | ||
| Inactive | 2879 (45.4%) | 2390 (45.1%) | |
| Unemployed | 318 (5.0%) | 258 (4.9%) | |
| In employment | 3138 (49.5%) | 2654 (50.1%) | |
| Educational level | 0.061 | ||
| Incomplete schooling | 1079 (17.1%) | 824 (15.5%) | |
| Full schooling | 3987 (63.1%) | 3375 (63.7%) | |
| Incomplete higher education | 552 (8.7%) | 495 (9.3%) | |
| Full higher education | 701 (11.1%) | 608 (11.5%) | |
| Socioeconomic status | 0.516 | ||
| Quintile I | 1199 (18.9%) | 948 (17.9%) | |
| Quintile II | 1265 (20.0%) | 1044 (19.7%) | |
| Quintile III | 1265 (20.0%) | 1054 (19.9%) | |
| Quintile IV | 1359 (21.5%) | 1170 (22.1%) | |
| Quintile V | 1247 (19.7%) | 1086 (20.5%) | |
| Depression during pregnancy | 0.676 | ||
| No | 5474 (87.5%) | 4627 (87.3%) | |
| Yes | 780 (12.5%) | 675 (12.7%) | |
| Postpartum depression | 0.727 | ||
| No | 5605 (88.5%) | 4702 (88.7%) | |
| Yes | 730 (11.5%) | 600 (11.3%) | |
| Recent depression | 0.871 | ||
| No | 5559 (88.0%) | 4671 (88.1%) | |
| Yes | 758 (12.0%) | 631 (11.9%) |
| Parental Stress | se | p-Value | β |
|---|---|---|---|
| Mother’s age | 0.002 | 0.476 | 0.001 |
| Child’s age (months) | 0.002 | 0.497 | −0.001 |
| Child’s sex 1 | 0.030 | 0.074 | −0.048 |
| Internalized problems, 2010 | 0.026 | 0.000 | 0.133 |
| Externalized problems, 2010 | 0.025 | 0.000 | 0.114 |
| Depression during pregnancy 2 | 0.048 | 0.000 | 0.180 |
| Recent depression 2 | 0.046 | 0.000 | 0.344 |
| Postpartum depression 2 | 0.047 | 0.089 | 0.073 |
| Unemployed 3 | 0.074 | 0.262 | −0.075 |
| In employment 3 | 0.033 | 0.000 | −0.172 |
| Quintile 2 4 | 0.048 | 0.001 | −0.145 |
| Quintile 3 4 | 0.049 | 0.000 | −0.157 |
| Quintile 4 4 | 0.050 | 0.000 | −0.249 |
| Quintile 5 4 | 0.055 | 0.000 | −0.505 |
| Secondary education 5 | 0.042 | 0.000 | −0.327 |
| Incomplete higher education 5 | 0.067 | 0.000 | −0.564 |
| Full higher education 5 | 0.067 | 0.000 | −0.594 |
| R2 | 0.178 |
| Externalized Problems 2012 | se | p-Value | β |
|---|---|---|---|
| Parental stress | 0.016 | 0.000 | 0.205 |
| Internalized problems | 0.028 | 0.003 | −0.069 |
| Externalized problems | 0.028 | 0.000 | 0.459 |
| Mother’s age | 0.002 | 0.000 | −0.017 |
| Child’s sex 1 | 0.032 | 0.000 | −0.177 |
| Child’s age (months) | 0.002 | 0.000 | −0.010 |
| Recent depression 2 | 0.051 | 0.043 | 0.086 |
| Depression during pregnancy 2 | 0.055 | 0.000 | 0.196 |
| Postpartum depression 2 | 0.051 | 0.470 | 0.031 |
| Quintile 2 3 | 0.054 | 0.704 | −0.017 |
| Quintile 3 3 | 0.054 | 0.365 | −0.041 |
| Quintile 4 3 | 0.055 | 0.270 | −0.050 |
| Quintile 5 3 | 0.060 | 0.011 | −0.127 |
| Secondary education 4 | 0.048 | 0.009 | −0.104 |
| Incomplete higher education 4 | 0.073 | 0.026 | −0.135 |
| Full higher education 4 | 0.071 | 0.001 | −0.192 |
| R2 | 0.309 |
| se | p-Value | β | |
|---|---|---|---|
| Internalized problems | 0.006 | <0.001 | 0.028 |
| Externalized problems | 0.006 | <0.001 | 0.023 |
| Depression during pregnancy | 0.012 | <0.001 | 0.037 |
| Recent depression | 0.011 | <0.001 | 0.070 |
| Internalized Problems 2012 | se | p-Value | β |
|---|---|---|---|
| Parental stress | 0.017 | 0.000 | 0.217 |
| Internalized problems | 0.033 | 0.000 | 0.382 |
| Externalized problems | 0.028 | 0.430 | −0.019 |
| Mother’s age | 0.003 | 0.000 | −0.009 |
| Child’s sex 1 | 0.034 | 0.711 | 0.011 |
| Child’s age (months) | 0.002 | 0.676 | −0.001 |
| Recent depression 2 | 0.051 | 0.013 | 0.108 |
| Depression during pregnancy 2 | 0.056 | 0.000 | 0.194 |
| Postpartum depression 2 | 0.051 | 0.221 | 0.053 |
| Quintile 2 3 | 0.055 | 0.594 | −0.025 |
| Quintile 3 3 | 0.056 | 0.013 | −0.118 |
| Quintile 4 3 | 0.056 | 0.007 | −0.130 |
| Quintile 5 3 | 0.063 | 0.000 | −0.233 |
| Secondary education 4 | 0.018 | 0.000 | −0.186 |
| Incomplete higher education 4 | 0.028 | 0.000 | −0.310 |
| Full higher education 4 | 0.027 | 0.000 | −0.356 |
| R2 | 0.282 |
| se | p-Value | Std. lv | |
|---|---|---|---|
| Internalized problems | 0.006 | <0.001 | 0.029 |
| Externalized problems | 0.006 | <0.001 | 0.025 |
| Depression during pregnancy | 0.004 | <0.001 | 0.039 |
| Recent depression | 0.005 | <0.001 | 0.075 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santelices, M.P.; Irarrázaval, M.; Jervis, P.; Brotfeld, C.; Cisterna, C.; Gallardo, A.M. Does Maternal Mental Health and Maternal Stress Affect Preschoolers’ Behavioral Symptoms? Children 2021, 8, 816. https://doi.org/10.3390/children8090816
Santelices MP, Irarrázaval M, Jervis P, Brotfeld C, Cisterna C, Gallardo AM. Does Maternal Mental Health and Maternal Stress Affect Preschoolers’ Behavioral Symptoms? Children. 2021; 8(9):816. https://doi.org/10.3390/children8090816
Chicago/Turabian StyleSantelices, María Pía, Matías Irarrázaval, Pamela Jervis, Cristian Brotfeld, Carla Cisterna, and Ana María Gallardo. 2021. "Does Maternal Mental Health and Maternal Stress Affect Preschoolers’ Behavioral Symptoms?" Children 8, no. 9: 816. https://doi.org/10.3390/children8090816