Association between Dental Caries and Influenza Infection in Children: A Japanese Nationwide Population-Based Study


Abstract
:1. Introduction
2. Materials and Methods
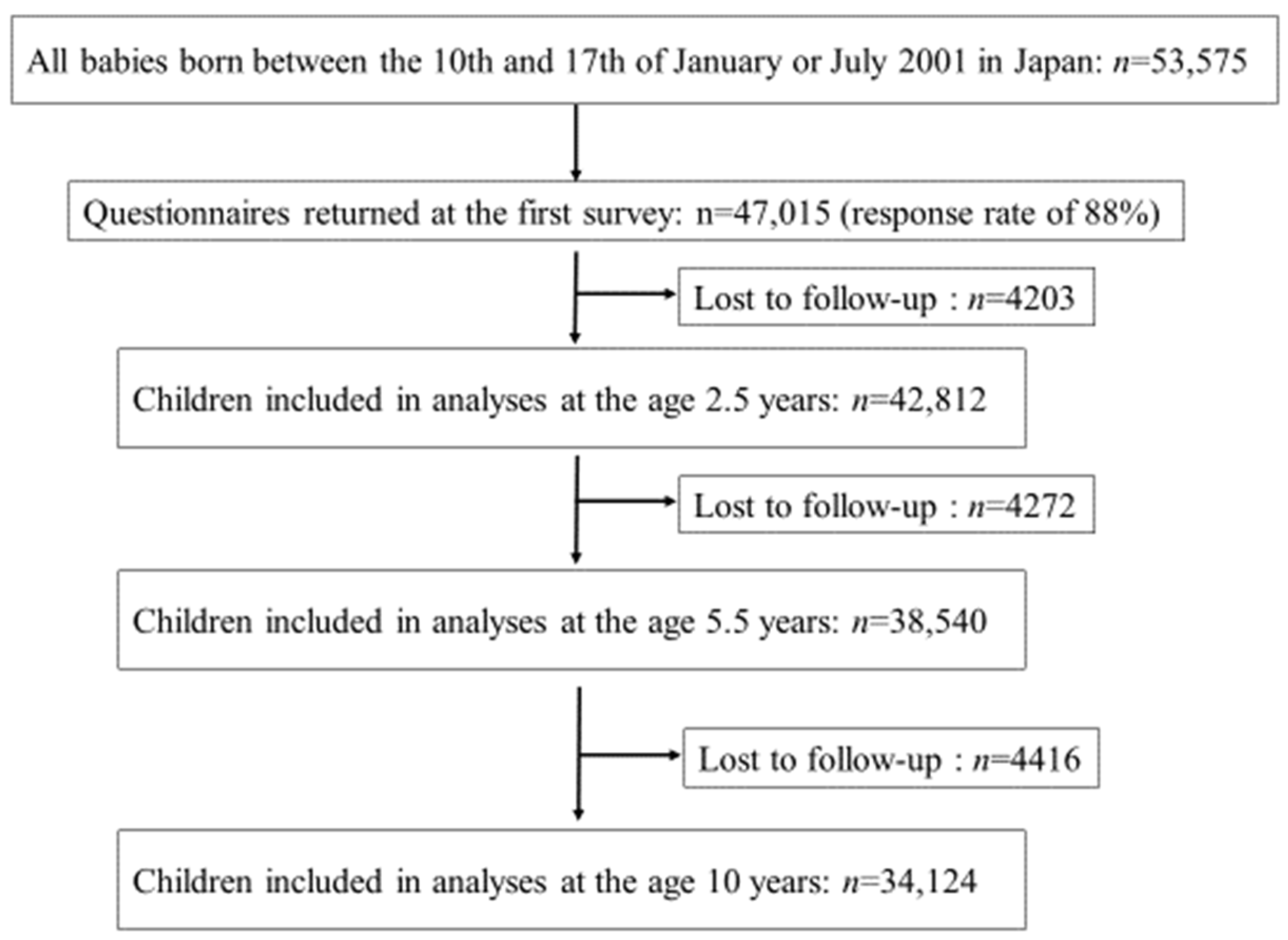
2.1. Participants
2.2. Dental Caries
2.3. Influenza
2.4. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Dental Caries and Influenza
3.3. Subgroup Analysis by Past Dental Caries Status
3.4. Sensitivity Analysis (Stratified by the Household Income Categories)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Oral Health Monitoring Group. Australia’s National Oral Health Plan 2015–2024. 2016. Available online: http://www.coaghealthcouncil.gov.au/Portals/0/Australia%27s%20National%20Oral%20Health%20Plan%202015-2024_uploaded%20170216.pdf (accessed on 2 April 2021).
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Chaffee, B.W.; Rodrigues, P.H.; Kramer, P.F.; Vítolo, M.R.; Feldens, C.A. Oral health-related quality-of-life scores differ by socioeconomic status and caries experience. Community Dent. Oral Epidemiol. 2017, 45, 216–224. [Google Scholar] [CrossRef]
- Ozsin Ozler, C.; Cocco, P.; Cakir, B. Dental caries and quality of life among preschool children: A hospital-based nested case-control study. Br. Dent. J. 2020. [Google Scholar] [CrossRef]
- Casamassimo, P.S.; Flaitz, C.M.; Hammersmith, K.; Sangvai, S.; Kumar, A. Recognizing the Relationship between Disorders in the Oral Cavity and Systemic Disease. Pediatri. Clin. N. Am. 2018, 65, 1007–1032. [Google Scholar] [CrossRef]
- Carramolino-Cuéllar, E.; Tomás, I.; Jiménez-Soriano, Y. Relationship between the oral cavity and cardiovascular diseases and metabolic syndrome. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e289. [Google Scholar] [CrossRef]
- Azarpazhooh, A.; Leake, J.L. Systematic Review of the Association between Respiratory Diseases and Oral Health. J. Periodontol. 2006, 77, 1465–1482. [Google Scholar] [CrossRef] [Green Version]
- Manger, D.; Walshaw, M.; Fitzgerald, R.; Doughty, J.; Wanyonyi, K.; White, S.; Gallagher, J.E. Evidence summary: The relationship between oral health and pulmonary disease. Br. Dent. J. 2017, 222, 527–533. [Google Scholar] [CrossRef] [Green Version]
- Mehtonen, I.T.; Rantala, A.K.; Hugg, T.T.; Jaakkola, M.S.; Jaakkola, J.J.K. Dental caries is associated with lower respiratory tract infections: A population-based cohort study. Respir. Med. 2019, 158, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Fuse, K.; Nishi, N.; Ikeda, N. Cohort Profile: 2001 Cohort of the Longitudinal Survey of Newborns in the 21st Century. Int. J. Epidemiol. 2017, 46, 1398–1398f. [Google Scholar] [CrossRef]
- Kato, T.; Yorifuji, T.; Inoue, S.; Yamakawa, M.; Doi, H.; Kawachi, I. Associations of Preterm Births with Child Health and Development: Japanese Population-Based Study. J. Pediatr. 2013, 163, 1578–1584.e4. [Google Scholar] [CrossRef]
- Matsumoto, N.; Yorifuji, T.; Nakamura, K.; Ikeda, M.; Tsukahara, H.; Doi, H. Breastfeeding and risk of food allergy: A nationwide birth cohort in Japan. Allergol. Int. 2020, 69, 91–97. [Google Scholar] [CrossRef]
- Yamakawa, M.; Yorifuji, T.; Inoue, S.; Kato, T.; Doi, H. Breastfeeding and obesity among schoolchildren: A nationwide longitudinal survey in Japan. JAMA Pediatr. 2013, 167, 919–925. [Google Scholar] [CrossRef] [Green Version]
- Longitudinal Survey of Newborns in the 21st Century (2001 Cohort) | Ministry of Health, Labour and Welfare, Japan. Available online: https://www.mhlw.go.jp/toukei/list/27-9.html (accessed on 10 April 2021).
- Zaitsu, T.; Saito, T.; Kawaguchi, Y. The Oral Healthcare System in Japan. Healthcare 2018, 6, 79. [Google Scholar] [CrossRef] [Green Version]
- Tashiro, M.; McKimm-Breschkin, J.L.; Saito, T.; Klimov, A.; Macken, C.; Zambon, M.; Hayden, F.G.; Neuraminidase Inhibitor Susceptibility Network. Surveillance for neuraminidase-inhibitor-resistant influenza viruses in Japan, 1996–2007. Antivir. Ther. 2009, 14, 751–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaraket, H.; Saito, R. Japanese Surveillance Systems and Treatment for Influenza. Curr. Treat. Opt. Infect. Dis. 2016, 8, 311–328. [Google Scholar] [CrossRef] [Green Version]
- André Kramer, A.C.; Pivodic, A.; Hakeberg, M.; Östberg, A.L. Multilevel analysis of dental caries in swedish children and adolescents in relation to socioeconomic status. Caries Res. 2019, 53, 96–106. [Google Scholar] [CrossRef]
- Mamelund, S.-E.; Shelley-Egan, C.; Rogeberg, O. The association between socioeconomic status and pandemic influenza: Protocol for a systematic review and meta-analysis. Syst. Rev. 2019, 8, 5. [Google Scholar] [CrossRef]
- Zhou, Y.; Jiang, S.; Li, K.Y.; Lo, E.C.M.; Gao, X. Association between oral health and upper respiratory tract infection among children. Int. Dent. J. 2018, 68, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Dou, D.; Revol, R.; Östbye, H.; Wang, H.; Daniels, R. Influenza A virus cell entry, replication, virion assembly and movement. Front. Immunol. 2018, 9, 1581. [Google Scholar] [CrossRef] [PubMed]
- Gaymard, A.; Le Briand, N.; Frobert, E.; Lina, B.; Escuret, V. Functional balance between neuraminidase and haemagglutinin in influenza viruses. Clin. Microbiol. Infect. 2016, 22, 975–983. [Google Scholar] [CrossRef] [PubMed]
- Scheiblauer, H.; Reinacher, M.; Tashiro, M.; Rott, R. Interactions between Bacteria and Influenza A Virus in the Development of Influenza Pneumonia. J. Infect. Dis. 1992, 166, 783–791. [Google Scholar] [CrossRef]
- Tashiro, M.; Ciborowski, P.; Klenk, H.D.; Pulverer, G.; Rott, R. Role of Staphylococcus protease in the development of influenza pneumonia. Nature 1987, 325, 536–537. [Google Scholar] [CrossRef] [PubMed]
- Abe, S.; Ishihara, K.; Adachi, M.; Sasaki, H.; Tanaka, K.; Okuda, K. Professional oral care reduces influenza infection in elderly. Arch. Gerontol. Geriatr. 2006, 43, 157–164. [Google Scholar] [CrossRef] [Green Version]
- Adachi, M.; Ishihara, K.; Abe, S.; Okuda, K. Professional oral health care by dental hygienists reduced respiratory infections in elderly persons requiring nursing care. Int. J. Dent. Hyg. 2007, 5, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Bansal, M.; Khatri, M.; Taneja, V. Potential role of periodontal infection in respiratory diseases—A review. J. Med. life 2013, 6, 244–248. [Google Scholar] [PubMed]
- Department of Health and Human Services, U.S. Public Health Service. Oral Health in America: Surgeon General Summary. Available online: https://www.nidcr.nih.gov/sites/default/files/2017-10/hck1ocv.%40www.surgeon.fullrpt.pdf (accessed on 6 May 2021).


{kind=link}
| Total | Caries (−) between the Ages of 1.5 and 2.5 Years | Caries (+) between the Ages of 1.5 and 2.5 Years | |
|---|---|---|---|
| (N = 42,812) | (N = 39,776) | (N = 3036) | |
| Characteristics of children | |||
| Gender, n (%) * | |||
| Boys | 22,216 (51.89) | 20,594 (51.77) | 1622 (53.43) |
| Girls | 20,596 (48.11) | 19,182 (48.23) | 1414 (46.57) |
| Singleton or multiple birth, n (%) * | |||
| Singleton birth, n (%) | 41,955 (98.00) | 38,949 (97.92) | 3006 (99.01) |
| Multiple birth, n (%) | 857 (2.00) | 827 (2.08) | 30 (0.99) |
| Term or preterm birth, n (%) * | |||
| Term birth, n (%) | 40,698 (95.06) | 37,773 (94.96) | 2925 (96.34) |
| Preterm birth, n (%) | 2114 (4.94) | 2003 (5.04) | 111 (3.66) |
| Parity, n (%) * | |||
| 0 (no older siblings) | 20,926 (48.88) | 19,732 (49.61) | 1194 (39.33) |
| 1 | 15,630 (36.51) | 14,373 (36.13) | 1257 (41.40) |
| ≥2 | 6256 (14.61) | 5671 (14.26) | 585 (19.27) |
| Family numbers, n (%) * | |||
| 1 | 308 (0.72) | 290 (0.73) | 18 (0.59) |
| 2 | 11,564 (27.01) | 10,958 (27.55) | 606 (19.96) |
| 3~5 | 27,542 (64.33) | 25,486 (64.07) | 2056 (67.72) |
| ≥6 | 3396 (7.93) | 3040 (7.64) | 356 (11.73) |
| Infant feeding practice, n (%) † | |||
| Formula feeding without colostrum | 663 (1.56) | 623 (1.58) | 40 (1.33) |
| Partial breastfeeding | 32,644 (76.83) | 30,572 (77.42) | 2072 (69.11) |
| Exclusive breastfeeding to 6–7 months of age | 9181 (21.61) | 8295 (21.01) | 886 (29.55) |
| Daycare attendance, n (%) ‡ | |||
| No | 26,049 (77.20) | 17,577 (78.29) | 4811 (75.05) |
| Yes | 7595 (22.51) | 8472 (21.43) | 2784 (24.66) |
| Residential area, n (%) * | |||
| Wards | 9388 (21.93) | 8820 (22.17) | 568 (18.71) |
| Cities | 25,205 (58.87) | 23,410 (58.85) | 1795 (59.12) |
| Towns or villages | 8219 (19.20) | 7546 (18.97) | 673 (22.17) |
| Characteristics of parents | |||
| Mean maternal age at delivery, years (SD) * | 30.13 (4.42) | 30.13 (4.41) | 30.15 (4.64) |
| Mean paternal age at delivery, years (SD) * | 32.30 (5.53) | 32.29 (5.51) | 32.41 (5.84) |
| Maternal smoking status, n (%) † | |||
| Non-smoker | 35,882 (84.24) | 33,425 (84.44) | 2457 (81.60) |
| Smoker | 6711 (15.76) | 6157 (15.56) | 554 (18.40) |
| Maternal educational attainment, n (%) ‡ | |||
| University or higher | 5849 (14.12) | 5538 (14.38) | 311 (10.67) |
| Junior college | 17,305 (41.76) | 16,197 (42.05) | 1108 (38.01) |
| Less than or equal to high school | 18,284 (44.12) | 16,788 (43.58) | 1496 (51.32) |
| Paternal educational attainment, n (%) ‡ | |||
| University or higher | 15,134 (36.89) | 14,239 (37.33) | 895 (31.07) |
| Junior college | 6453 (15.73) | 6020 (15.78) | 433 (15.03) |
| Less than or equal to high school | 19,435 (47.38) | 17,882 (46.88) | 1553 (53.90) |
| Crude | Model 1 | Model 2 | ||
|---|---|---|---|---|
| Ncase/N(%) | RR(95% CI) | † aRR(95% CI) | ‡ aRR(95% CI) | |
| Between the ages of 1.5 and 2.5 years | ||||
| caries (−) | 5433/39,776(13.66) | 1 (reference) | 1 (reference) | 1 (reference) |
| caries (+) | 488/3036(16.07) | 1.18(1.08–1.28) | 1.15 (1.06–1.25) | 1.15 (1.05–1.25) |
| Between the ages of 4.5 and 5.5 years | ||||
| caries (−) | 3683/24,497(15.03) | 1 (reference) | 1 (reference) | 1 (reference) |
| caries (+) | 2231/14,043(15.89) | 1.06(1.01–1.11) | 1.07 (1.02–1.12) | 1.06 (1.01–1.11) |
| Between the ages of 9 and 10 years | ||||
| caries (−) | 4035/22,715(17.76) | 1 (reference) | 1 (reference) | 1 (reference) |
| caries (+) | 2446/11,409(21.44) | 1.21(1.15–1.26) | 1.21(1.16–1.27) | 1.22 (1.17–1.28) |
| Ncase/N(%) | RR(95% CI) | † aRR(95% CI) | ‡ aRR(95% CI) | |
|---|---|---|---|---|
| Previous caries (−) | ||||
| caries (−) between the ages of 9 and 10 | 1495/8322(17.96) | 1 (reference) | 1 (reference) | 1 (reference) |
| caries (+) between the ages of 9 and 10 | 199/895(22.23) | 1.19(1.12–1.27) | 1.24(1.09–1.41) | 1.23(1.08–1.41) |
| Previous caries (+) | ||||
| caries (−) between the ages of 9 and 10 | 2343/13321(17.59) | 0.98(0.92–1.04) | 0.99(0.94–1.06) | 1.01(0.95–1.07) |
| caries (+) between the ages of 9 and 10 | 2222/10367(21.43) | 1.24(1.09–1.41) | 1.22(1.15–1.29) | 1.23(1.16–1.30) |
| House Income (yen) | ||||||
|---|---|---|---|---|---|---|
| Low Income | Middle Income | High Income | ||||
| Ncase/N(%) | aRR(95% CI) | Ncase/N(%) | aRR(95% CI) | Ncase/N(%) | aRR(95% CI) | |
| caries (−) between the ages of 9 and 10 | 376/2354 (15.97) | 1 (reference) | 2461/13,421 (18.34) | 1 (reference) | 489/2733 (17.89) | 1 (reference) |
| caries (+) between the ages of 9 and 10 | 542/2438 (22.23) | 1.34 (1.21–1.48) | 995/4609 (21.59) | 1.19 (1.11–1.27) | 462/2216 (20.85) | 1.16 (1.04–1.28) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumoto, N.; Kadowaki, T.; Tsukahara, H.; Yorifuji, T. Association between Dental Caries and Influenza Infection in Children: A Japanese Nationwide Population-Based Study. Children 2021, 8, 780. https://doi.org/10.3390/children8090780
Matsumoto N, Kadowaki T, Tsukahara H, Yorifuji T. Association between Dental Caries and Influenza Infection in Children: A Japanese Nationwide Population-Based Study. Children. 2021; 8(9):780. https://doi.org/10.3390/children8090780
Chicago/Turabian StyleMatsumoto, Naomi, Tomoka Kadowaki, Hirokazu Tsukahara, and Takashi Yorifuji. 2021. "Association between Dental Caries and Influenza Infection in Children: A Japanese Nationwide Population-Based Study" Children 8, no. 9: 780. https://doi.org/10.3390/children8090780