
Measurement of Behavioral Emotion Regulation Strategies in Early Childhood: The Early Emotion Regulation Behavior Questionnaire (EERBQ)


Abstract
:1. Introduction
1.1. ER Behaviors in Early Childhood
1.2. The Regulation of Positive Emotion
1.3. Current Measures of ER in Early Childhood
1.3.1. Caregiver-Report Questionnaires
1.3.2. Laboratory Assessment
1.4. The Current Study
2. Methods
2.1. Participants
2.2. Procedures
2.2.1. Instrument Construction
2.2.2. Data Collection
2.3. Measures
2.4. Data Analysis
3. Results
3.1. Internal Consistency and Interrelations of EERBQ Behavioral Subscales
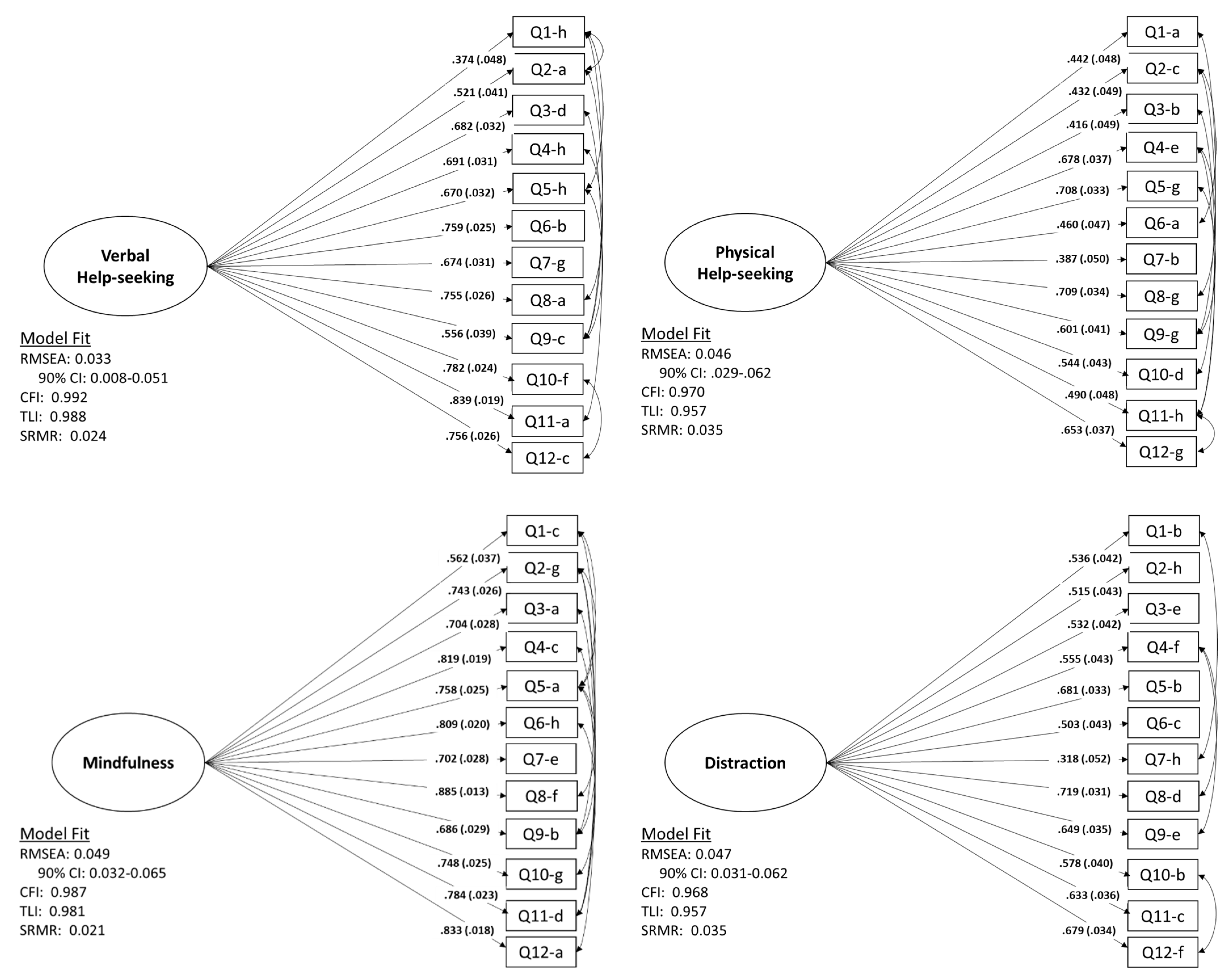
3.2. Factor Structure of EERBQ
3.3. Relation of EERBQ to Parent and Child Demographics
3.4. Comparison of EERBQ Subscales across Emotional Contexts
3.5. Relation of the EERBQ to Other Parent Indexes of Emotional Control
4. Discussion
Limitations and Future Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Calkins, S.D.; Perry, N.B. The development of emotion regulation: Implications for child adjustment. In Developmental Psychopathology: Maladaptation and Psychopathology, 3rd ed.; Cicchetti, D., Ed.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2019; Volume 3, pp. 187–242. [Google Scholar]
- Bailey, C.S.; Denham, S.A.; Curby, T.W.; Bassett, H.H. Emotional and organizational supports for preschoolers’ emotion regulation: Relations with school adjustment. Emotion 2016, 16, 263–279. [Google Scholar] [CrossRef]
- Zalewski, M.; Lengua, L.J.; Wilson, A.C.; Trancik, A.; Bazinet, A. Associations of coping and appraisal styles with emotion regulation during preadolescence. J. Exp. Child Psychol. 2011, 110, 141–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim-Spoon, J.; Cicchetti, D.; Rogosch, F.A. A longitudinal study of emotion regulation, emotion lability-negativity, and internalizing symptomology in maltreated and nonmaltreated children. Child Dev. 2013, 84, 512–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeman, J.; Shipman, K.; Suveg, C. Anger and sadness regulation: Predictions to internalizing and externalizing symptoms in children. J. Clin. Child Adolesc. Psychol. 2002, 31, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.L.; Degnan, K.A.; Calkins, S.D.; Keane, S.P. Profiles of externalizing behavior problems for boys and girls across preschool: The roles of emotion regulation and inattention. Dev. Psychol. 2006, 42, 913–928. [Google Scholar] [CrossRef] [Green Version]
- Supplee, L.H.; Skuban, E.M.; Shaw, D.S.; Prout, J. Emotion regulation strategies and later externalizing behavior among European American and African American children. Dev. Psychopathol. 2009, 21, 393–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillion, M.; Shaw, D.S. Co-development of externalizing and internalizing problems in early childhood. Dev. Psychopathol. 2004, 16, 313–333. [Google Scholar] [CrossRef] [Green Version]
- Degnan, K.; Fox, N. Behavioral inhibition and anxiety disorders: Multiple levels of a resilience process. Dev. Psychopathol. 2007, 19, 729–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenberg, N.; Spinrad, T.; Eggum, N.D. Emotion-related self-regulation and its relation to children’s maladjustment. Annu. Rev. Clin. Psychol. 2010, 6, 495–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, P.M.; Martin, S.E.; Dennis, T.D. Emotion regulation as a scientific construct: Methodological challenges and directions for future research. Child Dev. 2004, 75, 317–333. [Google Scholar] [CrossRef] [Green Version]
- Eisenberg, N.; Hofer, C.; Vaughan, J. Effortful Control and Its Socioemotional Consequences. In Handbook of Emotion Regulation; Gross, J.J., Ed.; The Guilford Press: New York, NY, USA, 2007; pp. 287–306. [Google Scholar]
- Gross, J.J.; Thompson, R.A. Emotion Regulation: Conceptual Foundations. In Handbook of Emotion Regulation; Gross, J.J., Ed.; The Guilford Press: New York, NY, USA, 2007; pp. 3–24. [Google Scholar]
- Perry, N.B.; Calkins, S.D. A biopsychosocial perspective on the development of emotion regulation across childhood. In The Development of Emotion Regulation: A Matter of Time; Cole, P.M., Hollenstein, T., Eds.; Routledge: New York, NY, USA, 2018; pp. 3–30. [Google Scholar] [CrossRef]
- Kopp, C. Regulation of distress and negative emotions: A developmental view. Dev. Psychol. 1989, 25, 243–254. [Google Scholar] [CrossRef]
- Rydell, A.; Berlin, L.; Bohlin, G. Emotionality, emotion regulation, and adaptation among 5- to 8-year-old children. Emotion 2003, 3, 30–47. [Google Scholar] [CrossRef] [PubMed]
- Calkins, S.D.; Dedmon, S.A. Physiological and behavioral regulation in two-year-old children with aggressive/destructive behavior problems. J. Abnorm. Child Psychol. 2000, 28, 103–118. [Google Scholar] [CrossRef] [PubMed]
- Grolnick, W.S.; McMenamy, J.M.; Kurowski, C.O. Emotional self-regulation in infancy and toddlerhood. In Child Psychology: A Handbook of Contemporary Issues, 2nd ed.; Balter, L., Tamis-LeMonda, C.S., Eds.; Psychology Press: New York, NY, USA, 2006; pp. 3–25. [Google Scholar]
- Aldao, A.; Nolen-Hoeksema, S.; Schweizer, S. Emotion-regulation strategies across psychopathology: A meta-analytic review. Clin. Psychol. Rev. 2010, 30, 217–237. [Google Scholar] [CrossRef]
- Calkins, S.D.; Bell, M.A. Child development at the intersection of emotion and cognition. In Human Brain Development; American Psychological Association: Washington, DC, USA, 2010. [Google Scholar]
- Stifter, C.; Dollar, J. Temperament and developmental psychopathology. In Developmental Psychopathology: Risk, Resilience, and Intervention; Cicchetti, D., Ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2012; pp. 546–607. [Google Scholar] [CrossRef]
- Rothbart, M.K. Measurement of temperament in infancy. Child Dev. 1981, 52, 569–578. [Google Scholar] [CrossRef]
- Hageskull, B. The baby and toddler behavior questionnaires: Empirical studies and conceptual consideration. Scand. J. Psychol. 1985, 26, 110–122. [Google Scholar] [CrossRef]
- Putnam, S.P.; Rothbart, M.K. Development of short and very short forms of the Children’s Behavior Questionnaire. J. Personal. Assess. 2006, 87, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Achenbach, T.M. Integrative Guide for the 1991 CBCL/4-18, YSR, and TRF Profiles; Department of Psychiatry, University of Vermont: Burlington, NJ, USA, 1991. [Google Scholar]
- Shields, A.; Cicchetti, D. Emotion regulation among school-age children: The development and validation of a new criterion Q-sort scale. Dev. Psychol. 1997, 33, 906–916. [Google Scholar] [CrossRef] [PubMed]
- Graziano, P.; Calkins, S.D.; Keane, S.P. Maternal behavior and children’s early emotion regulation skills differentially predict development of children’s reactive control and later effortful control. Infant Child Dev. 2010, 19, 333–352. [Google Scholar] [CrossRef]
- Perry, N.B.; Calkins, S.D.; Nelson, J.A.; Leerkes, E.M.; Marcovitch, S. Mothers’ responses to children’s negative emotions and child emotion regulation: The moderating role of vagal suppression. Dev. Psychobiol. 2012, 54, 503–513. [Google Scholar] [CrossRef] [Green Version]
- Rothbart, M.K.; Derryberry, D. Development of individual differences in temperament. In Advances in Developmental Psychology; Lamb, M.E., Brown, A.L., Eds.; Erlbaum: Hillsdale, NJ, USA, 1981; Volume 1, pp. 37–86. [Google Scholar]
- Rothbart, M.; Ziaie, H.; O’Boyle, C. Self-regulation and emotion in infancy. In Emotion and Its Regulation in Early Development. New Directions for Child Development; Eisenberg, N., Fabes, R., Eds.; Jossey-Bass/Pfeiffer: San Francisco, CA, USA, 1992; pp. 7–23. [Google Scholar]
- Fabes, R.A.; Poulin, R.E.; Eisenberg, N.; Madden-Derdich, D.A. The coping with children’s negative emotions scale (CCNES): Psychometric properties and relations with children’s competence. Marriage Fam. Rev. 2002, 34, 285–310. [Google Scholar] [CrossRef]
- Goodman, R. The strengths and difficulties questionnaire. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Muthén, L.K.; Muthén, B.O. Mplus Users Guide (2012–2017), 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Dollar, J.M.; Stifter, C.A. Temperamental surgency and emotion regulation as predictors of childhood social competence. J. Exp. Child Psychol. 2012, 112, 178–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Root, A.K.; Denham, S.A. The role of gender in the socialization of emotion: Key concepts and critical issues. In Focus on Gender: Parent and Child Contributions to the Socialization of Emotional Competence; Root, A.K., Denham, S.A., Eds.; Jossey-Bass: San Francisco, CA, USA, 2010; Volume 128, pp. 1–9. [Google Scholar]
- Brody, L.R.; Hall, J.A. Gender and emotion in context. In Handbook of Emotions, 3rd ed.; Lewis, M., Haviland-Jones, J.M., Barrett, L.F., Eds.; The Guilford Press: New York, NY, USA, 2008. [Google Scholar]
- Barrett, L.F.; Adolphs, R.; Marsella, S.; Martinez, A.M.; Pollak, S.D. Emotional Expressions Reconsidered: Challenges to Inferring Emotion from Human Facial Movements. Psychol. Sci. Public Interest 2019, 20, 1–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Measure | Mean | SD | Range | α |
|---|---|---|---|---|
| EERBQ | ||||
| Distraction | 3.32 | 1.08 | 1.00–6.67 | 0.85 |
| Mindfulness | 4.69 | 1.48 | 1.00–7.00 | 0.94 |
| Physical Help-Seeking | 4.63 | 1.04 | 1.08–7.00 | 0.84 |
| Verbal Help-Seeking | 4.48 | 1.34 | 1.00–6.92 | 0.91 |
| Avoidance | 2.42 | 0.88 | 1.00–5.00 | 0.77 |
| Physical Venting | 2.62 | 0.86 | 1.00–5.75 | 0.84 |
| Verbal Venting | 2.83 | 1.12 | 1.00–5.92 | 0.85 |
| Self-Soothing | 1.80 | 1.19 | 1.00–6.50 | 0.95 |
| Emotional Reactivity | 3.60 | 0.96 | 1.33–6.67 | 0.75 |
| ERC | ||||
| Emotion Regulation | 3.40 | 0.31 | 2.25–4.00 | 0.59 |
| Lability/Negativity | 1.92 | 0.35 | 1.00–3.27 | 0.83 |
| SDQ | ||||
| Emotional Problems | 0.33 | 0.32 | 0.00–1.60 | 0.62 |
| Conduct Problems | 0.31 | 0.28 | 0.00–1.40 | 0.57 |
| Hyperactivity | 0.83 | 0.49 | 0.00–2.00 | 0.79 |
| Peer Problems | 0.27 | 0.29 | 0.00–1.40 | 0.53 |
| Prosocial Scale | 1.58 | 0.33 | 0.60–2.00 | 0.65 |
| Total Difficulties | 0.44 | 0.22 | 0.00–1.10 | 0.73 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Distraction | -- | ||||||||||||||||
| 2. Mindfulness | 0.29 * | -- | |||||||||||||||
| 3. Physical Help-Seeking | 0.31 * | 0.39 * | -- | ||||||||||||||
| 4. Verbal Help-Seeking | 0.45 * | 0.74 * | 0.38 * | -- | |||||||||||||
| 5. Avoidance | 0.01 | 0.08 | 0.11 * | 0.02 | -- | ||||||||||||
| 6. Physical Venting | −0.09 | −0.09 | −0.08 | −0.18 * | 0.31 * | -- | |||||||||||
| 7. Verbal Venting | −0.15 * | −0.05 | −0.08 | −0.22 * | 0.27 * | 0.75 * | -- | ||||||||||
| 8. Self-Soothing | −0.05 | −0.04 | 0.18 * | −0.04 | 0.34 * | 0.18 * | 0.14 * | -- | |||||||||
| 9. Emotional Reactivity | −0.29 * | −0.10 | −0.26 * | −0.19 * | 0.21 * | 0.47 * | 0.51 * | 0.05 | -- | ||||||||
| 10. Emotion Regulation (ERC) | 0.19 * | 0.48 * | 0.31 * | 0.43 * | −0.18 * | −0.26 * | −0.24 * | −0.10 | −0.30 * | -- | |||||||
| 11. Negativity/Lability (ERC) | −0.28 * | −0.05 | −0.24 * | −0.17 * | 0.18 * | 0.52 * | 0.55 * | 0.08 | 0.67 * | −0.30 * | -- | ||||||
| 12. Emotional Problems (SDQ) | −0.11 * | 0.18 * | 0.09 | 0.13 * | 0.31 * | 0.11 * | 0.14 * | 0.16 * | 0.31 * | −0.10 | 0.22 * | -- | |||||
| 13. Conduct Problems (SDQ) | −0.26 * | −0.06 | −0.28 * | −0.15 * | 0.19 * | 0.40 * | 0.41 * | 0.11 * | 0.59 * | −0.31 * | 0.71 * | 0.18 * | -- | ||||
| 14. Hyperactivity (SDQ) | −0.10 | 0.01 | −0.09 | −0.10 * | 0.08 | 0.28 * | 0.32 * | 0.05 | 0.38 * | −0.14 * | 0.59 * | 0.11 * | 0.47 * | -- | |||
| 15. Peer Problems (SDQ) | −0.06 | −0.19 * | −0.14 * | −0.19 * | −0.01 | 0.12 * | 0.12 * | 0.03 | 0.11 * | −0.33 * | 0.18 * | 0.14 * | 0.11 * | 0.08 | -- | ||
| 16. Prosocial Scale (SDQ) | 0.29 * | 0.33 * | 0.32 * | 0.34 * | −0.02 | −0.33 * | −0.33 * | −0.06 | −0.37 * | 0.50 * | −0.43 * | −0.034 | −0.47 * | −0.25 * | −0.29 * | -- | |
| 17. Total Problems (SDQ) | −0.20 * | −0.01 | −0.16 * | −0.12 * | 0.22 * | 0.36 * | 0.40 * | 0.13 * | 0.55 * | −0.33 * | 0.70 * | 0.54 * | 0.69 * | 0.77 * | 0.47 * | −0.40 * | -- |
| Measure | Age 2 α (N = 85) | Mean (SD) | Age 3 α (N = 84) | Mean (SD) | Age 4 α (N = 77) | Mean (SD) | Age 5 α (N = 73) | Mean (SD) | Age 6 α (N = 43) | Mean (SD) |
|---|---|---|---|---|---|---|---|---|---|---|
| EERBQ | ||||||||||
| Distraction | 0.85 | 3.23 (1.07) | 0.88 | 3.16 (1.14) | 0.84 | 3.48 (1.04) | 0.79 | 3.58 (0.93) | 0.87 | 3.62 (1.21) |
| Mindfulness | 0.94 | 3.51 (1.52) | 0.94 | 4.85 (1.38) | 0.92 | 5.20 (1.25) | 0.89 | 5.14 (1.10) | 0.93 | 5.25 (1.30) |
| Physical Help Seeking | 0.82 | 4.42 (0.99) | 0.84 | 4.77 (1.02) | 0.87 | 4.85 (1.10) | 0.81 | 4.42 (0.98) | 0.85 | 4.77 (1.05) |
| Verbal Help-Seeking | 0.93 | 3.38 (1.48) | 0.89 | 4.53 (1.20) | 0.86 | 4.96 (1.03) | 0.84 | 4.88 (0.94) | 0.89 | 5.08 (1.10) |
| Avoidance | 0.76 | 2.34 (0.79) | 0.80 | 2.44 (0.92) | 0.77 | 2.32 (0.86) | 0.77 | 2.56 (0.89) | 0.80 | 2.49 (0.95) |
| Physical Venting | 0.84 | 2.86 (0.95) | 0.80 | 2.68 (0.78) | 0.85 | 2.56 (0.82) | 0.85 | 2.64 (0.89) | 0.77 | 2.24 (0.95) |
| Verbal Venting | 0.85 | 3.20 (1.16) | 0.84 | 3.01 (1.09) | 0.87 | 2.69 (1.13) | 0.84 | 2.66 (1.04) | 0.82 | 2.28 (0.96) |
| Self-Soothing | 0.95 | 1.93 (1.27) | 0.95 | 1.91 (1.32) | 0.94 | 1.73 (1.11) | 0.94 | 1.78 (1.11) | 0.96 | 1.54 (1.02) |
| Emotional Reactivity | 0.69 | 3.54 (0.85) | 0.70 | 3.64 (0.85) | 0.71 | 3.50 (0.95) | 0.84 | 3.86 (1.16) | 0.76 | 3.42 (1.02) |
| Paired Samples | Mean (SD) | r | Mean Change (SD) | t (df = 361) |
|---|---|---|---|---|
| Mindfulness in Positive | 4.95 (1.60) | 0.80 ** | 0.35 (1.00) | 6.74 ** |
| Mindfulness in Negative | 4.60 (1.52) | |||
| Avoidance in Positive | 1.29 (0.56) | 0.38 ** | −1.49 (1.02) | −27.94 ** |
| Avoidance in Negative | 2.79 (1.09) | . | ||
| Distraction in Positive | 3.58 (1.26) | 0.65 ** | 0.35 (1.01) | 6.49 ** |
| Distraction in Negative | 3.23 (1.13) | |||
| Verbal Help-Seeking Positive | 5.03 (1.61) | 0.79 ** | 0.73 (0.99) | 14.08 ** |
| Verbal Help-Seeking Negative | 4.30 (1.33) | |||
| Physical Help-Seeking Positive | 4.26 (1.28) | 0.55 ** | −0.49 (1.15) | −8.10 ** |
| Physical Help-Seeking Negative | 4.76 (1.10) | |||
| Self-Soothing Positive | 1.38 (0.83) | 0.79 ** | −0.57 (0.88) | −12.38 ** |
| Self-Soothing Negative | 1.95 (1.36) | |||
| Verbal Venting Positive | 2.79 (1.54) | 0.52 ** | −0.05 (1.37) | −0.757 ** |
| Verbal Venting Negative | 2.84 (1.17) | |||
| Physical Venting Positive | 4.72 (1.09) | 0.36 ** | 2.80 (1.17) | 45.61 ** |
| Physical Venting Negative | 1.91 (0.96) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perry, N.B.; Dollar, J.M. Measurement of Behavioral Emotion Regulation Strategies in Early Childhood: The Early Emotion Regulation Behavior Questionnaire (EERBQ). Children 2021, 8, 779. https://doi.org/10.3390/children8090779
Perry NB, Dollar JM. Measurement of Behavioral Emotion Regulation Strategies in Early Childhood: The Early Emotion Regulation Behavior Questionnaire (EERBQ). Children. 2021; 8(9):779. https://doi.org/10.3390/children8090779
Chicago/Turabian StylePerry, Nicole B., and Jessica M. Dollar. 2021. "Measurement of Behavioral Emotion Regulation Strategies in Early Childhood: The Early Emotion Regulation Behavior Questionnaire (EERBQ)" Children 8, no. 9: 779. https://doi.org/10.3390/children8090779