
Supporting Primary School Children with Juvenile Idiopathic Arthritis: A Qualitative Investigation of Teaching Staff Experiences


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Recruitment
2.3. Data Collection
2.4. Data Analysis
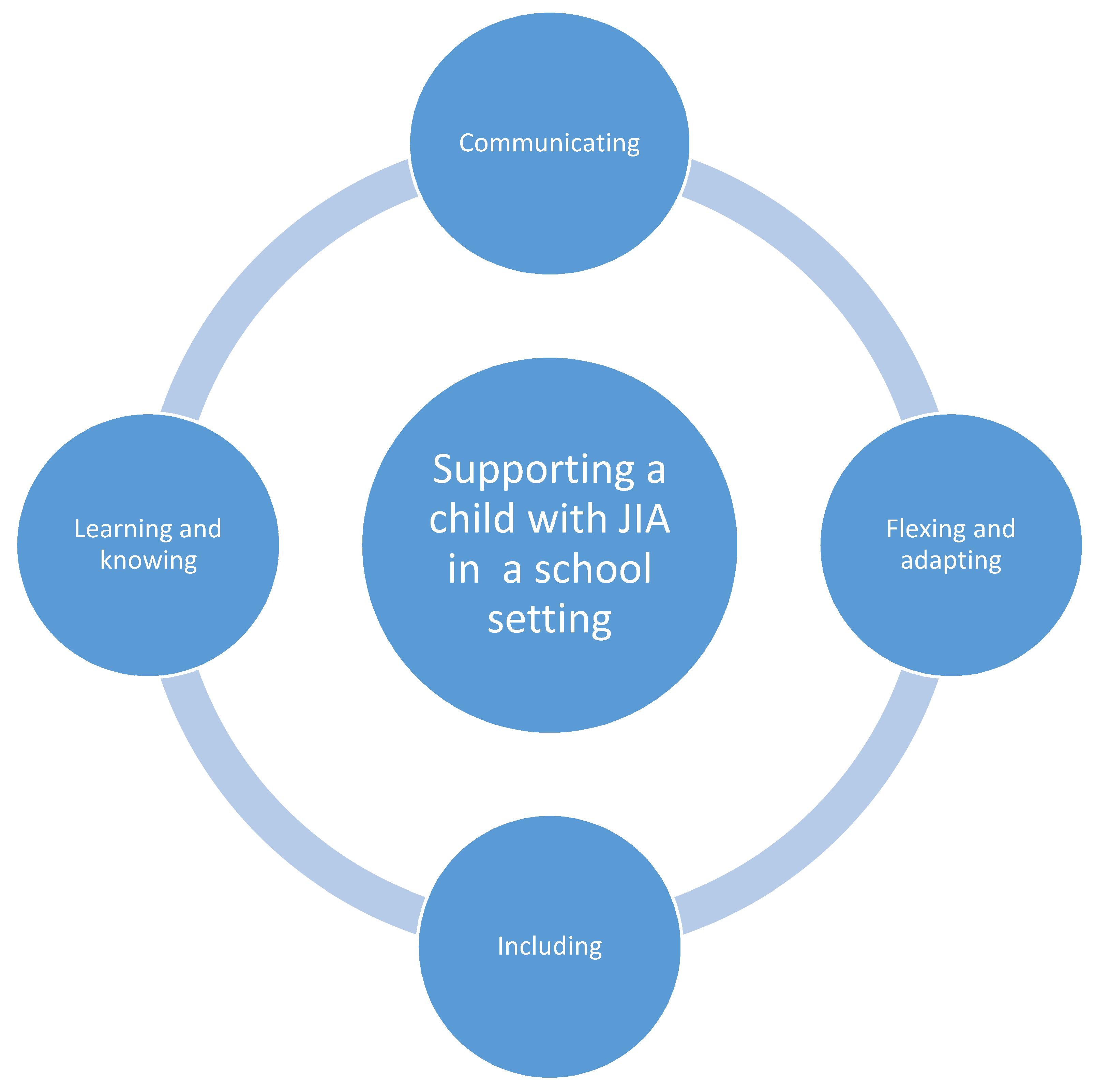
3. Results
3.1. Communicating
“All the support put in place has been through discussions with the parents and ideas that they have that can support her. We are in constant communication”.(P45—survey)
“The most important thing was to talk to the child and parents about the specific issues they faced. It seemed that each sufferer was very individual”.(P22—survey)
“Mum and myself communicated on a daily basis so I was always aware exactly how she [child with JIA] was feeling before commencing the school day”.(P06—survey)
“After diagnosis, I was able to research and was given some information from the paediatrician via parents”.(P09—survey)
“Initial communication with the previous teacher with regard to how and when to differentiate, the impact of his condition in the classroom and any strategies they may have previously used”.(P15—survey)
“With the traffic light system, red was sore, orange was okay, and green was really good. It was very simple for her to be able to say, ‘I’m green, I feel really okay today. I’m not too good, so it’s the orange. Red is, I’m feeling really sore”.(P07—interview)
“We also spoke to the pupils in the class about his arthritis so that they had an understanding and could consider it when they were working with him”.(P37—survey)
3.2. Flexing and Adapting
“He [child with JIA] wouldn’t put his full effort into certain activities, which wouldn’t be like him because he was always one for trying really hard. I would then have a wee conversation. ‘Are you feeling a bit tired today?’ ‘Yes.’ ‘That’s fine. Just do what you can and leave what you can’t do.’ It is having a little understanding and awareness”.(P18—interview)
“My TA [teaching assistant] or I can scribe if we are writing a larger piece of text—or they will type”.(P26—survey)
“Her mum always came on school trips for extra support and with her chair so she could use that when walking became too much”.(P06—survey)
3.3. Including
“If anything was wrong, there was an extra member of support staff there that predominantly was for her. However, we could share that support with the children that have got needs within the classroom, and that has certainly really worked. We didn’t want her to stand out”.(P07—interview)
“We took out netballs and everybody had a go so it wasn’t just you’re allowed to use this ball and everyone else is allowed to use this one. So, trying to think of ways of using different equipment but it being part of the lesson”.(P01—interview)
“She [child with JIA] could have friends go with her to different places so when she was allowed out early from a lesson, she could take a friend with her, so she wasn’t alone”.(P02—interview)
“I set up a reading group so that she had a social element that was inside, so she could still have a chance to talk to the girls”.(P01—interview)
“In many ways they [strategies] worked as they allowed him to be included and ensured he wasn’t missing out on any key learning experiences. However, this pupil just wanted to be like everybody else. He didn’t want to be treated differently or do different things from the rest of the class. He never used the time out card, hated sitting on a chair when everyone else was on the floor and didn’t want to use different materials to other pupils…The resources and strategies were in place but more often than not he chose not to use it”.(P37—survey)
3.4. Learning and Knowing
“I’d never heard of it (JIA) until I taught the first child. My father suffers dreadfully from arthritis, so I often thought of him when working with the children”.(P36—survey)
“We also had a physiotherapist visit school and did daily exercises in school as recommended by the physiotherapist”.(P39—survey)
“Supporting parents when the child is reluctant to have routine injections and prepare the child for when we know they are due”.(P25—survey)
4. Discussion
4.1. Main Discussion Points
4.2. Limitations
4.3. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Survey Questionnaire
| Section A: Participant Demographic and Job-Related Information | |
| Question | Type of question (and options of answers where relevant) |
| (1) Which gender do you identify with? | Closed (1) Male (2) Female (3) Other (4) Prefer not to disclose |
| (2) What is your age? (age in years) | Open-ended |
| (3) What is your job title | Open-ended |
| (4) Can you please briefly describe your work role? (For example, leadership roles, curriculum areas of leadership, SENCO, etc.) | Open-ended |
| (5) How many years of experience do you have in the above-mentioned role? (Number in years) | Open-ended |
| (6) Which age groups have you taught/supported throughout your working experience? Please tick the boxes relevant to the age group of children you’ve taught/ supported, including the ones you are currently teaching/supporting. | Closed Primary school Teaching Please note that Scottish school years are placed in brackets (e.g., P5). (1) P1 (2) Y1 (P2) (3) Y2 (P3) (4) Y3 (P4) (5) Y4 (P5) (6) Y5 (P6) (7) Y6 (P7) Secondary school teaching Please note that Scottish school years are placed in brackets (e.g., P5). (1) Y7 (1ST) (2) Y8 (2ND) (3) Y9 (3RD) (4) Y10 (4TH) (5) Y11 (5TH) (6) 6TH (Scotland) Sixth form/College (1) Y12 (2) Y13 |
| (7) What year did you complete your teacher training? | Number indicating the year |
| (8) What type of training did you complete? Please choose all options that apply: | Closed 1. Postgraduate Certificate in Education 2. Postgraduate Teacher Training Course 3. Professional Graduate Diploma in Education 4. Undergraduate Teaching Degree 5. Future Teaching Scholars 6. Graduate Teaching Programme 7. Now Teach 8. Premier Pathways 9. Researchers in Schools (RiS) 10. Teach First 11. Transition to Teach 12. Other (please specify): |
| (9) Apart from your teacher training programme, can you briefly tell us about any other training you have completed with regards teaching primary school aged children? For example, have you received training in supporting children with additional needs? | Open-ended |
| Section B: Participants’ Experiences in Supporting a Child with JIA in School | |
| Question | Type of question (and options of answers where relevant) |
| (1) Can you please indicate the number and age group of children with JIA you’ve taught so far? Please include the count of the children you are currently associated with. | (1a) Number of children taught with JIA (1b) Age group of children with JIA taught, so far (please tick for current children too): Please note that Scottish school years are placed in brackets (e.g., P5). Q30 (1) P1 (Scotland) (2) Y1 (P2) (3) Y2 (P3) (4) Y3 (P4) (5) Y4 (P5) (6) Y5 (P6) (7) Y6 (P7) (8) Y7 (1ST) (9) Y8 (2ND) (10) Y9 (3RD) (11) Y10 (4TH) (12) Y11 (5TH) (13) Y12 (6TH) (14) Y13 |
| Please answer the questions below in relation to your knowledge of the child or children with JIA that you have supported in a school setting. We realise that this may not be current experience, it’s fine to tell us about previous experience you may have had in supporting a child with JIA in school. Please be careful not to mention any actual names, you can use initials if this makes things easier for you. (2) Can you describe how you came to know of the child’s/children’s diagnosis of JIA? | Open-ended |
| (3) In your opinion, does having JIA influence a child’s ability to attend, concentrate and engage with school-related activities, such as the following: 1. Academic performance, including the completion of homework? 2. Emotional wellbeing? 3. Playtime and socializing? 4. Movement around the school? 5. Taking part in PE or other sport-related activities? 6. Attending school trips and other activities? 7. Impact of time off due to medical appointments? 8. Other? If so, please specify. | Open-ended |
| (4) If any, which strategies did you put in place to support the child/children with JIA in your school? | Open-ended |
| (5) Can you share how useful you believe these support strategies were? | Open-ended |
| (6) Where there any challenges in providing these support strategies? If yes, please tell us about the challenges you encountered. | Open-ended |
| (7) Details on how you planned this support. Did you receive or consult any particular training or resources? If yes, where did you hear about these? | Open-ended |
| (8) Which training or resources did you consult or receive? | Open-ended |
| (9) To what extent was the information and training you received throughout your teacher training useful in supporting a child with JIA? | Open-ended |
| (10) How useful was the training or advice you received? | Open-ended |
| (11) Can you please tell us about any instances when, the training or information you received wasn’t of much use and you had to improvise on the training information or try something new of your own? | Open-ended |
| Section C: Teaching Staff’s Support and Training Needs in Relation to JIA | |
| Question | Type of question (and options of answers where relevant) |
| (1) On a scale of 0 (totally unconfident)—10 (very confident) how confident are you with supporting a child with JIA in school? | Closed 0 = totally unconfident 1 2 3 4 5 = neutral 6 7 8 9 10 = Very confident |
| (2) Which aspects of this support do you feel confident about? Please also tell us why you feel this way. | Open-ended |
| (3) Which aspects of this support do you not feel confident about? Please also tell us why you feel this way. | Open-ended |
| (4) To what extent did you feel supported by members of your Senior Leadership Team, School Governing Body and Key Stage Leaders in your role? Did you ever require assistance with making decisions, reporting concerns or ensuring inclusion for the child? | Open-ended |
| (5) Did you ever need assistance from another member of staff with carrying out your job role? If so, how did they support you? | Open-ended |
| (6) Were you the only individually trained staff member or was there a supportive member of staff also trained? If so, what skills did you use to ensure you worked successfully and supportively together? | Open-ended |
| (7) Is there anything that would be helpful in further improving your confidence in supporting a child with JIA in your classroom? | Open-ended |
| (8) According to you, what type of training or resources do you think would benefit teachers who are looking for advice on how to support a child with JIA in their class? | Open-ended |
| (9) Lastly, if you were to conduct a seminar or a training programme for teachers to care for children with JIA, what topics would you include? | Open-ended |
Appendix B. Semistructured Interview Schedule
Appendix B.1. Experiences of Supporting Children with JIA
Appendix B.2. Educational Impact of the Physical Effects of JIA
- (a)
- Attendance?
- (b)
- Curriculum subjects that involve physical activity (PE, drama, music, arts)?
- (c)
- Core curriculum areas (numeracy, literacy, science)?
- (d)
- Extra-curricular activities?
- (e)
- School trips?
Appendix B.3. Children’s Social Wellbeing in School
- (a)
- Children’s seating plans with peers in lessons?
- (b)
- Seating arrangements for lunchtime?
- (c)
- Participation in group work?
Appendix B.4. Emotional Wellbeing in School
Appendix B.5. Children’s Engagement in Lessons and Learning
Appendix C. Support Strategies Employed by Teaching Staff to Support Primary-School-Aged Children with JIA in a School Setting
| Category of Support Strategy | Specific Support Strategy or Characteristic of Support Strategy |
| Strategies aiming to recognize and assess pain levels | Use of colored cards to notify teachers of pain |
| Use of “traffic light colors” or “faces” to assess and indicate the level of pain | |
| Use of aids by children as an indication of pain state | |
| Proximity in class assisted monitoring | |
| Adaptations and use of aids | Providing indoor space during breaks and lunchtime |
| Assisting handwriting (pencil grips; laptop to type work; touch-typing programs; dictation/scribe; occupational therapy hand exercises; encourage breaks) | |
| Assisting sitting (provide a chair, bench, or a cushion) | |
| Opportunities for rest & participation according to child’s capability | Regular breaks during activities and throughout school day |
| Reduced school day | |
| Participation led by child’s capability | |
| Qualities characterizing strategies | Discreet |
| Socially inclusive | |
| Flexible |
References
- Thierry, S.; Fautrel, B.; Lemelle, I.; Guillemin, F. Prevalence and incidence of juvenile idiopathic arthritis: A systematic review. Jt. Bone Spine 2014, 81, 112–117. [Google Scholar] [CrossRef] [PubMed]
- NRAS. A Focus on Juvenile Idiopathic Arthritis. Available online: https://nras.org.uk/resource/juvenile-idiopathic-arthritis-jia/?print-pdf=6864 (accessed on 21 January 2021).
- Sur, L.; Gaga, R.; Duca, E.; Sur, G.; Lupan, I.; Sur, D.; Samasca, G.; Lazea, C.; Lazar, C. Different chronic disorders that fall within the term juvenile idiopathic arthritis. Life 2021, 11, 398. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, M.G.; Whitham, J.N.; Roberton, D.M.; Taplin, J.E.; Varni, J.W.; Baghurst, P.A. The relationship between health-related quality of life, pain and coping strategies in juvenile idiopathic arthritis. Rheumatology 2003, 43, 325–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanns, L.; Cordingley, L.; Galloway, J.; Norton, S.; Carvalho, L.A.; Christie, D.; Sen, D.; Carrasco, R.; Rashid, A.; Foster, H.; et al. Depressive symptoms, pain and disability for adolescent patients with juvenile idiopathic arthritis: Results from the Childhood Arthritis Prospective Study. Rheumatol. Oxf. Engl. 2018, 57, 1381–1389. [Google Scholar] [CrossRef] [Green Version]
- Fowler, M.G.; Johnson, M.P.; Atkinson, S.S. School achievement and absence in children with chronic health conditions. J. Pediatr. 1985, 106, 683–687. [Google Scholar] [CrossRef]
- United Nations Children’s Fund UK. The United Nations Convention on the Rights of the Child. 1989. Available online: https://downloads.unicef.org.uk/wp-content/uloads/2010/05/UNCRC_PRESS200910web.pdf?_ga=2.78590034.795419542.1582474737-1972578648.1582474737 (accessed on 24 May 2021).
- Sato, A.F.; Hainsworth, K.R.; Khan, K.A.; Ladwig, R.J.; Weisman, S.J.; Davies, W.H. School absenteeism in pediatric chronic pain: Identifying lessons learned from the general school absenteeism literature. Child Healthcare 2007, 36, 355–372. [Google Scholar] [CrossRef]
- Nordal, E.; For the Nordic Study Group of Pediatric Rheumatology (NoSPeR); Rypdal, V.; Arnstad, E.D.; Aalto, K.; Berntson, L.; Ekelund, M.; Fasth, A.; Glerup, M.; Herlin, T.; et al. Participation in school and physical education in juvenile idiopathic arthritis in a Nordic long-term cohort study. Pediatr. Rheumatol. 2019, 17, 44. [Google Scholar] [CrossRef] [Green Version]
- Bouaddi, I.; Rostom, S.; El Badri, D.; Hassani, A.; Chkirate, B.; Amine, B.; Hajjaj-Hassouni, N. Impact of juvenile idiopathic arthritis on schooling. BMC Pediatr. 2013, 13. Available online: https://bmcpediatr.biomedcentral.com/articles/10.1186/1471-2431-13-2 (accessed on 1 March 2021). [CrossRef] [Green Version]
- Laila, K. Impact of juvenile idiopathic arthritis on school attendance and performance. Am. J. Clin. Exp. Med. 2016, 4, 185. [Google Scholar] [CrossRef]
- Agoston, A.; Gray, L.; Logan, D. Pain in school: Patterns of pain-related school impairment among adolescents with primary pain conditions, juvenile idiopathic arthritis pain, and pain-free peers. Children 2016, 30, 39. [Google Scholar] [CrossRef] [Green Version]
- Chomistek, K.; Johnson, N.; Stevenson, R.; Luca, N.; Miettunen, P.; Benseler, S.M.; Veeramreddy, D.; Schmeling, H. Patient-reported barriers at school for children with juvenile idiopathic arthritis. ACR Open Rheumatol. 2019, 1, 182–187. [Google Scholar] [CrossRef] [Green Version]
- Schlichtiger, J.; Haas, J.-P.; Barth, S.; Bisdorff, B.; Hager, L.; Michels, H.; Hügle, B.; Radon, K. Education and employment in patients with juvenile idiopathic arthritis—A standardized comparison to the German general population. Pediatr. Rheumatol. 2017, 15. Available online: http://ped-rheum.biomedcentral.com/articles/10.1186/s12969-017-0172-2 (accessed on 1 March 2021). [CrossRef] [Green Version]
- Logan, D.E.; Curran, J.A. Adolescent chronic pain problems in the school setting: Exploring the experiences and beliefs of selected school personnel through focus group methodology. J. Adolesc. Health 2005, 37, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Tarpey, S.; Caes, L.; Heary, C. Supporting children with chronic pain in school: Understanding teachers’ experiences of pain in the classroom. Eur. Health Psychol. 2018, 20, 419–424. [Google Scholar]
- Braun, V.; Clarke, V. Successful Qualitative Research: A Practical Guide for Beginners; SAGE: Los Angeles, CA, USA, 2013. [Google Scholar]
- Braun, V.; Clarke, V.; Boulton, E.; Davey, L.; McEvoy, C. The online survey as a qualitative research tool. Int. J. Soc. Res. Methodol. 2020, 1–14. [Google Scholar] [CrossRef]
- Qualtrics. Qualtrics: Provo, UT, USA, 2018. Available online: https://www.qualtrics.com/blog/citing-qualtrics/ (accessed on 1 March 2021).
- Drabble, L.; Trocki, K.F.; Salcedo, B.; Walker, P.C.; Korcha, R.A. Conducting qualitative interviews by telephone: Lessons learned from a study of alcohol use among sexual minority and heterosexual women. Qual. Soc. Work 2016, 15, 118–133. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study: Qualitative descriptive study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed]
- NVivo QSR International Pty Ltd. NVivo. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 21 January 2021).
- Patton, M.Q. Qualitative Evaluation and Research Methods, 2nd ed.; SAGE: Newbury Park, CA, USA, 1990. [Google Scholar]
- Elliott, R.; Fischer, C.T.; Rennie, D.L. Evolving guidelines for publication of qualitative research studies in psychology and related fields. Br. J. Clin. Psychol. 1999, 38, 215–229. [Google Scholar] [CrossRef] [Green Version]
- IBM Corp. IBM SPSS Statistics for Windows; Armonk, NY, USA, 2020. [Google Scholar]
- Department for Education and Department for Health. Special Educational Needs and Disability Code of Practice: 0 to 25 Years. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/398815/SEND_Code_of_Practice_January_2015.pdf (accessed on 21 May 2021).
- Rohde, G.; Westergren, T.; Haraldstad, K.; Johannessen, B.; Høie, M.; Helseth, S.; Fegran, L.; Slettebø, Å. Teachers’ experiences of adolescents’ pain in everyday life: A qualitative study. BMJ Open 2015, 5, e007989. [Google Scholar] [CrossRef]
- Bernard, H.R.; Killworth, P.; Kronenfeld, D.; Sailer, L. The problem of informant accuracy: The validity of retrospective data. Annu. Rev. Anthropol. 1984, 13, 495–517. [Google Scholar] [CrossRef]
- Majid, U.; Kim, C.; Cako, A.; Gagliardi, A.R. Engaging stakeholders in the co-development of programs or interventions using Intervention Mapping: A scoping review. PLoS ONE 2018, 13, e0209826. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, G.; O’Higgins, S.; Caes, L.; Saetes, S.; McGuire, B.E.; Stinson, J. Self-management needs of Irish adolescents with Juvenile Idiopathic Arthritis (JIA): How can a Canadian web-based programme meet these needs? Pediatr. Rheumatol. 2018, 8, 68. [Google Scholar] [CrossRef] [PubMed]
- Kohut, S.A.; Stinson, J.N.; Ruskin, D.; Forgeron, P.; Harris, L.; van Wyk, M.; Luca, S.; Campbell, F. iPeer2Peer program: A pilot feasibility study in adolescents with chronic pain. Pain 2016, 157, 1146–1155. [Google Scholar] [CrossRef]
- Stinson, J.; Kohut, S.A.; Forgeron, P.; Amaria, K.; Bell, M.; Kaufman, M.; Luca, N.; Luca, S.; Harris, L.; Victor, C.; et al. The iPeer2Peer Program: A pilot randomized controlled trial in adolescents with Juvenile Idiopathic Arthritis. Pediatr. Rheumatol. 2016, 14. Available online: http://ped-rheum.biomedcentral.com/articles/10.1186/s12969-016-0108-2 (accessed on 1 March 2021). [CrossRef] [Green Version]
- Suldo, S.M.; Friedrich, A.A.; White, T.; Farmer, J.; Minch, D.; Michalowski, J. Teacher support and adolescents’ subjective well-being: A mixed-methods investigation. Sch. Psychol. Rev. 2009, 38, 67–85. [Google Scholar] [CrossRef]
- Vervoort, T.; Logan, D.E.; Goubert, L.; De Clercq, B.; Hublet, A. Severity of pediatric pain in relation to school-related functioning and teacher support: An epidemiological study among school-aged children and adolescents. Pain 2014, 155, 1118–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Gender | Women | 43 (84.3%) |
|---|---|---|
| Men | 8 (15.7%) | |
| Age (in years) | Mean (SD) = 41.6 (10.3) | |
| Min = 22; Max = 60 | ||
| Current job title | (a) Teacher (various levels/seniorities) | 36 (70.5%) |
| (b) Special Educational Needs Coordinator SENCO | 5 (9.8%) | |
| (c) Teaching assistant positions (various levels/seniorities) | 7 (13.7%) | |
| (d) Primary physical education (PE] specialist | 1 (1.9%) | |
| (e) Other roles (e.g., administration manager) | 2 (3.9%) | |
| Years of experience in the current work role | Mean (SD) = 11.5 (8.1) Min = 1; Max = 34 | |
| Level of confidence with supporting a child with JIA (1 = totally unconfident; 10 = very confident) | Mean (SD) = 6.9 (1.8) | |
| Knowledge Gap Domain | Specific Identified Training Need |
|---|---|
| Medical and physical | Presentation of JIA and how this differs to other types of arthritis |
| How to support the child to manage pain flares | |
| Short and long-term effects of JIA on the child | |
| Co-occurrence of JIA with other conditions | |
| Pain management (how to administer, side effects of medications, effectiveness of non-pharmacological methods of pain management) | |
| How to support children to use aids in a school setting (e.g., handwriting aids) | |
| Emotional | Potential effects of JIA on a child’s self-esteem and self-image |
| How JIA may impact a child’s mental health | |
| Strategies to support familial management of JIA | |
| Peer relationships | Supporting children’s friendships during breaktimes/lunchtimes |
| Educating the child’s peers about JIA | |
| How to create an inclusive environment among the child’s classmates | |
| Academic | Impact of JIA on children’s attention and concentration |
| Supporting school attendance | |
| How to support a child academically while absent from school |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jordan, A.; Vasileiou, K.; Brown, C.; Caes, L. Supporting Primary School Children with Juvenile Idiopathic Arthritis: A Qualitative Investigation of Teaching Staff Experiences. Children 2021, 8, 555. https://doi.org/10.3390/children8070555
Jordan A, Vasileiou K, Brown C, Caes L. Supporting Primary School Children with Juvenile Idiopathic Arthritis: A Qualitative Investigation of Teaching Staff Experiences. Children. 2021; 8(7):555. https://doi.org/10.3390/children8070555
Chicago/Turabian StyleJordan, Abbie, Konstantina Vasileiou, Ceri Brown, and Line Caes. 2021. "Supporting Primary School Children with Juvenile Idiopathic Arthritis: A Qualitative Investigation of Teaching Staff Experiences" Children 8, no. 7: 555. https://doi.org/10.3390/children8070555