

Intermittent High-Dose Vitamin D3 Administration in Neonates with Multiple Comorbidities and Vitamin D Insufficiency
 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
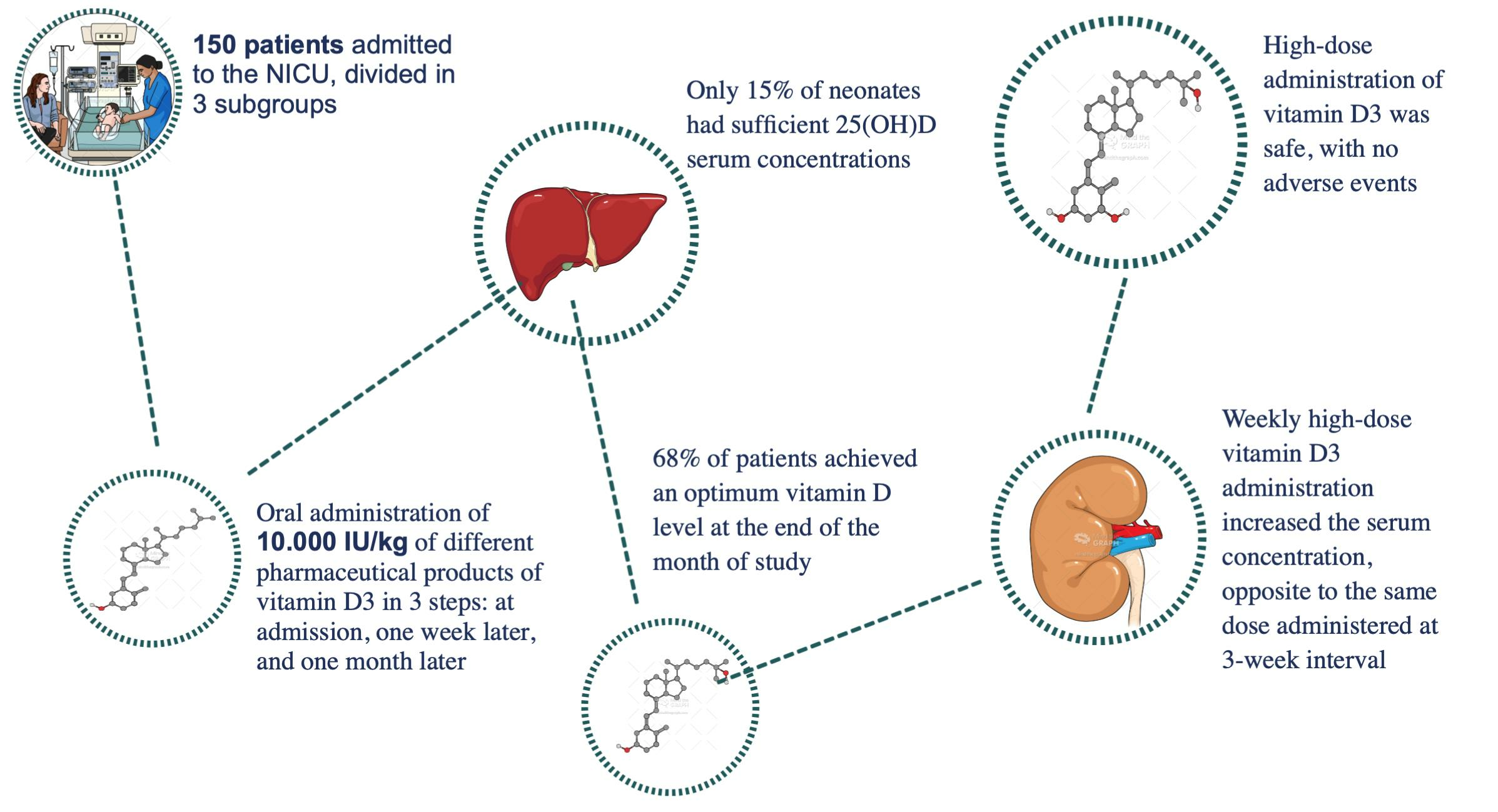
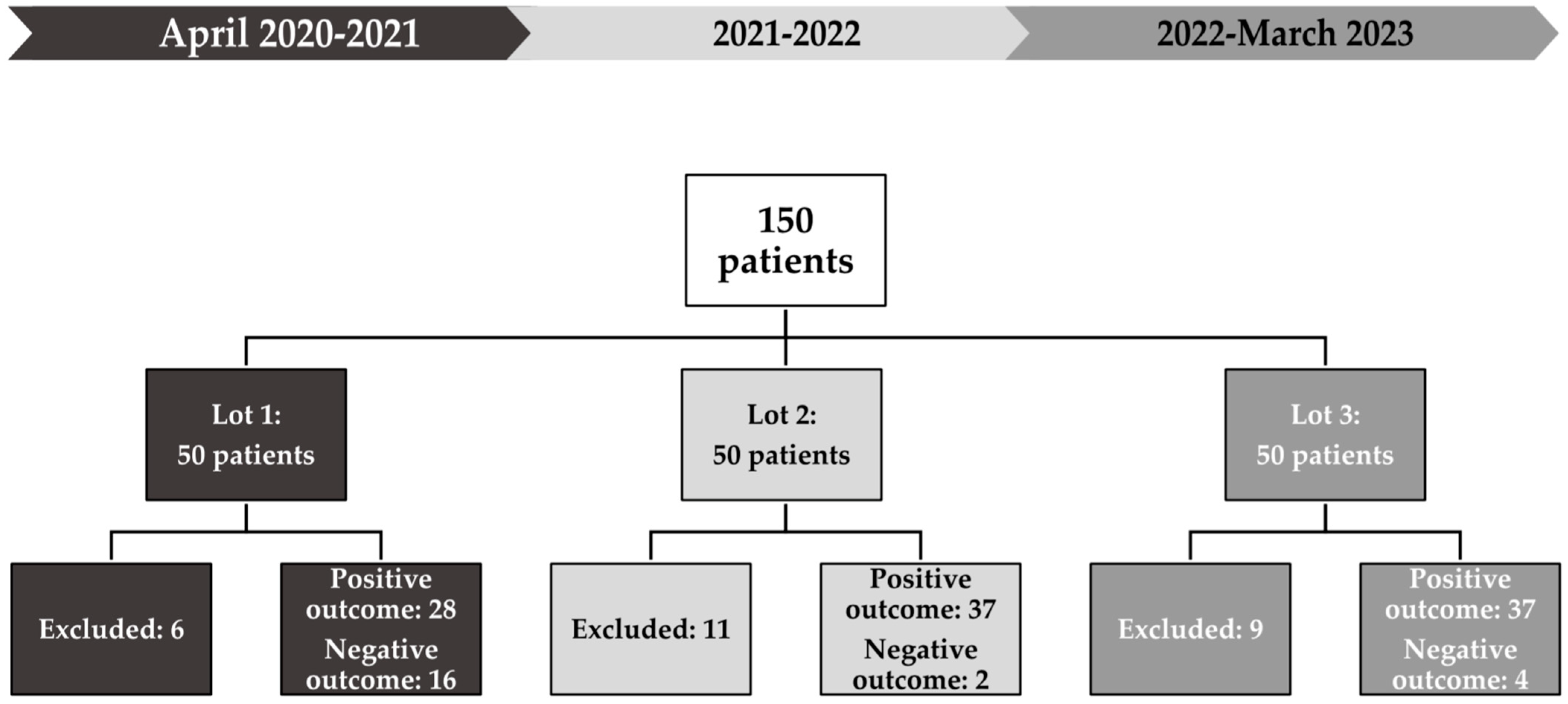
2.1. Study Design and Participants
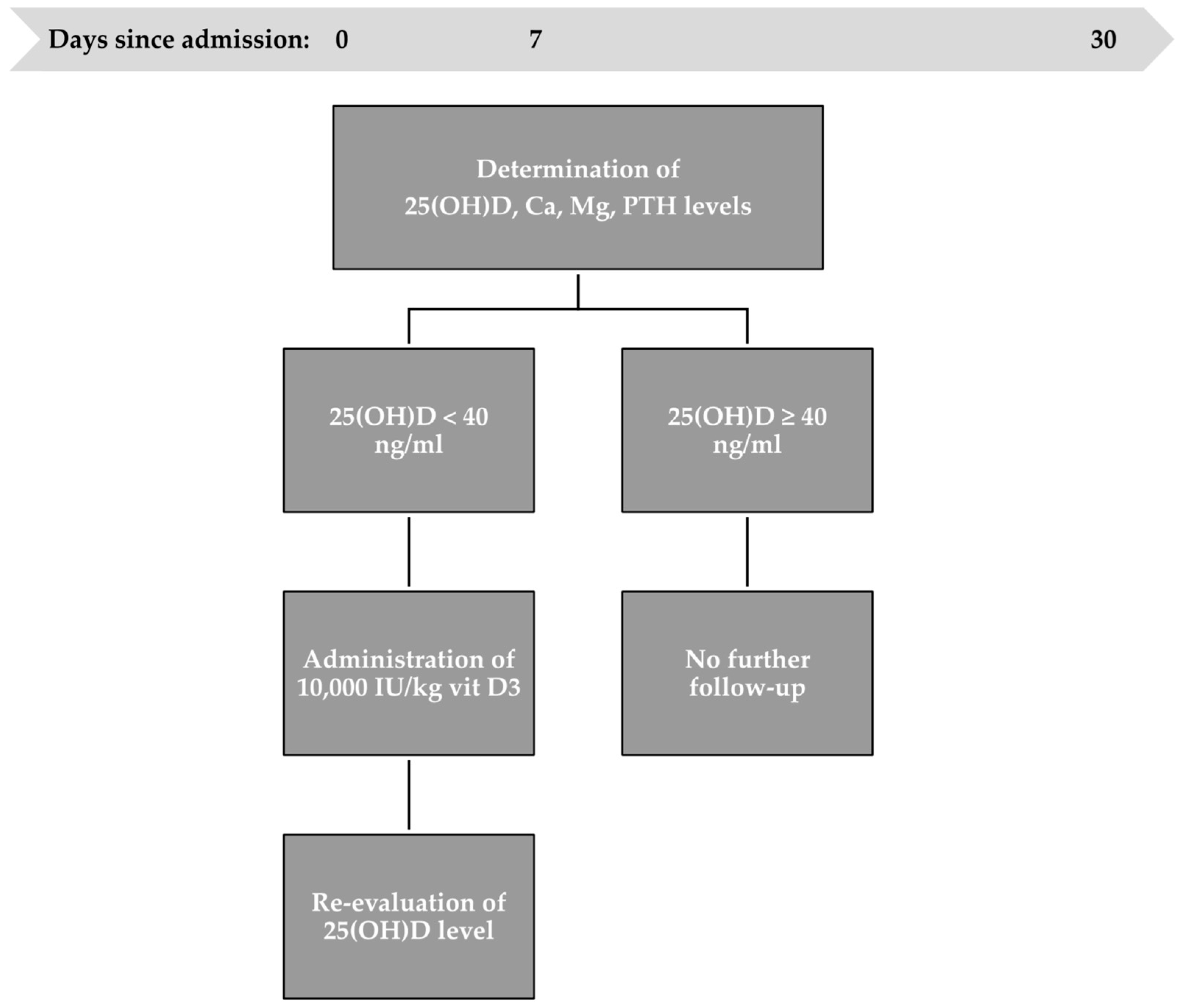
2.2. Vitamin D3 Administration Protocol
2.3. Statistical Analysis
2.4. Ethical Considerations
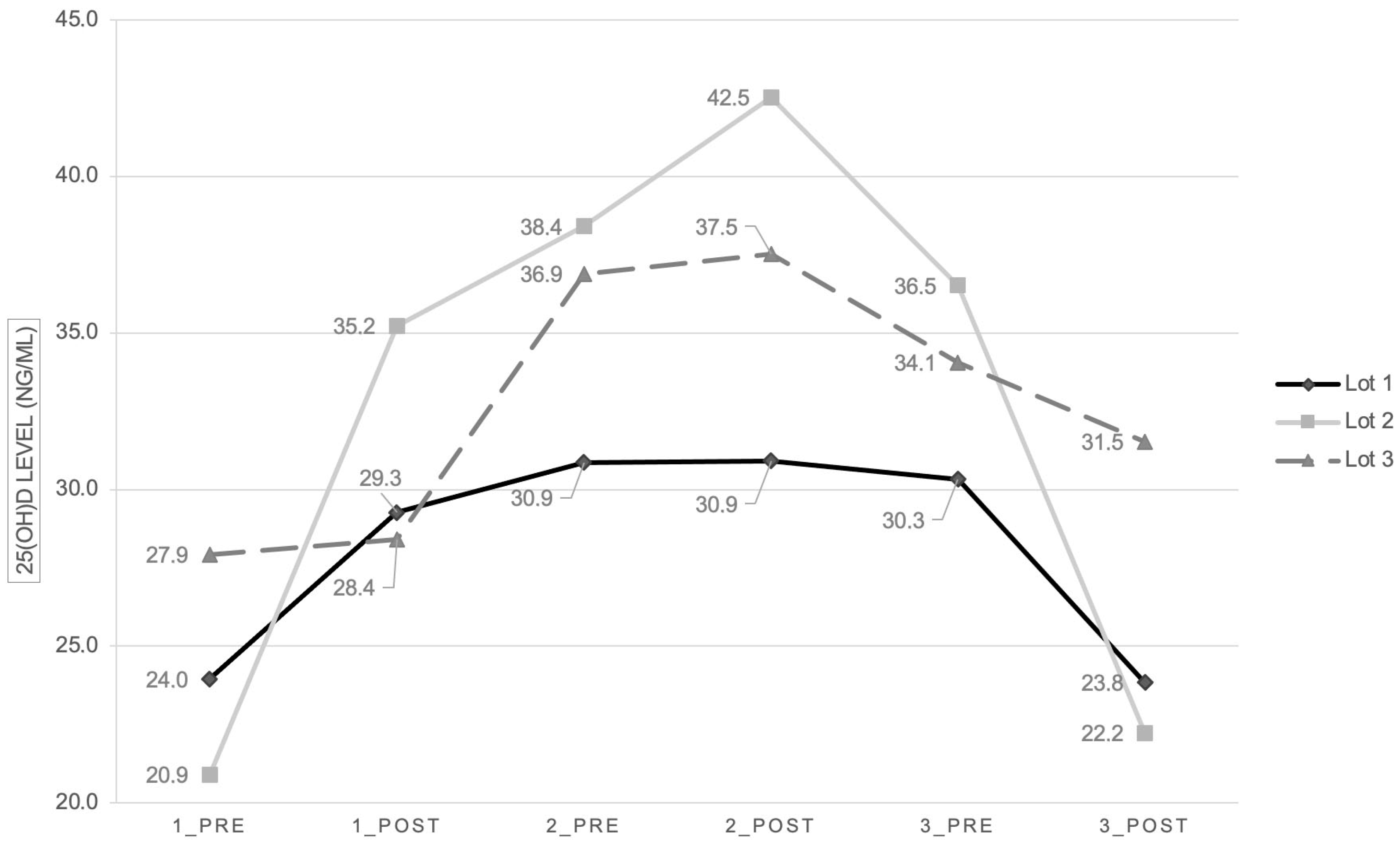
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aly, H.; Abdel-Hady, H. Vitamin D and the neonate: An update. J. Clin. Neonatol. 2015, 4, 1–7. [Google Scholar] [CrossRef]
- Clancy, N.; Onwuneme, C.; Carroll, A.; McCarthy, R.; McKenna, M.J.; Murphy, N.; Molloy, E.J. Vitamin D and neonatal immune function. J. Matern. Fetal Neonatal Med. 2013, 26, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.S.; Ren, S.; Liu, P.T.; Chun, R.F.; Lagishetty, V.; Gombart, A.F.; Borregaard, N.; Modlin, R.L.; Hewison, M. Vitamin D-directed rheostatic regulation of monocyte antibacterial responses. J. Immunol. 2009, 182, 4289–4295. [Google Scholar] [CrossRef]
- Gombart, A.F.; Pierre, A.; Maggini, S. A review of micronutrients and the immune system-working in harmony to reduce the risk of infection. Nutrients 2020, 12, 236. [Google Scholar] [CrossRef]
- Society, C.P. Preventing Symptomatic Vitamin D Deficiency and Rickets among Indigenous Infants and Children in Canada. Canadian Paediatric Society. Available online: https://cps.ca/en/documents/position/vitamin-d-deficiency-and-rickets-among-indigenous-infants-and-children (accessed on 20 March 2023).
- Braun, A.; Chang, D.; Mahadevappa, K.; Gibbons, F.K.; Liu, Y.; Giovannucci, E.; Christopher, K.B. Association of Low Serum 25-Hydroxyvitamin D Levels and Mortality in the Critically Ill. Crit. Care Med. 2011, 39, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.; Eisman, J.A.; Center, J.R. Vitamin D Deficiency in Critically Ill Patients. N. Engl. J. Med. 2009, 360, 1912–1914. [Google Scholar] [CrossRef]
- Moromizato, T.; Litonjua, A.A.; Braun, A.B.; Gibbons, F.K.; Giovannucci, E.; Christopher, K.B. Association of Low Serum 25-Hydroxyvitamin D Levels and Sepsis in the Critically Ill. Crit. Care Med. 2014, 42, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Madden, K.; Feldman, H.A.; Smith, E.M.; Gordon, C.M.; Keisling, S.M.; Sullivan, R.M.; Hollis, B.W.; Agan, A.A.; Randolph, A.G. Vitamin D deficiency in critically ill children. Pediatrics 2012, 130, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Nair, R.; Maseeh, A. Vitamin D: The “sunshine” vitamin. J. Pharmacol. Pharmacother. 2012, 3, 118–126. [Google Scholar]
- Rosen, C.J. Vitamin D Insufficiency. N. Engl. J. Med. 2011, 364, 248–254. [Google Scholar] [CrossRef]
- Ward, L.M.; Gaboury, I.; Ladhani, M.; Zlotkin, S. Vitamin D-deficiency rickets among children in Canada. CMAJ 2007, 177, 161–166. [Google Scholar] [CrossRef]
- Poel, Y.; Hummel, P.; Lips, P.; Stam, F.; van der Ploeg, T.; Simsek, S. Vitamin D and gestational diabetes: A systematic review and meta-analysis. Eur. J. Intern. Med. 2012, 23, 465–469. [Google Scholar] [CrossRef]
- Scholl, T.O.; Chen, X.; Stein, P. Maternal vitamin D status and delivery by caesarean. Nutrients 2012, 4, 319–330. [Google Scholar] [CrossRef]
- Burris, H.H.; Rifas-Shiman, S.L.; Camargo, C.A.; Litonjua, A.A.; Huh, S.Y.; Rich-Edwards, J.W.; Gillman, M.W. Plasma 25-hydroxyvitamin D during pregnancy and small-for-gestational age in black and white infants. Ann. Epidemiol. 2012, 22, 581–586. [Google Scholar] [CrossRef]
- Whitehouse, A.J.O.; Holt, B.J.; Serralha, M.; Holt, P.G.; Kusel, M.M.H.; Hart, P.H. Maternal serum vitamin D levels during pregnancy and offspring neurocognitive development. Pediatrics 2012, 129, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Javaid, M.; Crozier, S.; Harvey, N.; Gale, C.; Dennison, E.; Boucher, B.; Arden, N.; Godfrey, K.; Cooper, C.; Princess Anne Hospital Study Group. Maternal vitamin D status during pregnancy and childhood bone mass at age 9 years: A longitudinal study. Lancet 2006, 367, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Sai, A.J.; Walters, R.W.; Fang, X.; Gallagher, J.C. Relationship between vitamin D, parathyroid hormone, and bone health. J. Clin. Endocrinol. Metab. 2011, 96, E436–E446. [Google Scholar] [CrossRef]
- Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes for Calcium and Vitamin D; National Academy Press: Washington, DC, USA, 2010. [Google Scholar]
- Munns, C.F.; Shaw, N.; Kiely, M.; Specker, B.L.; Thacher, T.D.; Ozono, K.; Michigami, T.; Tiosano, D.; Mughal, M.Z.; Mäkitie, O.; et al. Global Consensus Recommendations on Prevention and Management of Nutritional Rickets. J. Clin. Endocrinol. Metab. 2016, 101, 394–415. [Google Scholar] [CrossRef] [PubMed]
- Rostami, M.; Tehrani, F.R.; Simbar, M.; Bidhendi Yarandi, R.; Minooee, S.; Hollis, B.W.; Hosseinpanah, F. Effectiveness of Prenatal Vitamin D Deficiency Screening and Treatment Program: A Stratified Randomized Field Trial. J. Clin. Endocrinol. Metab. 2018, 103, 2936–2948. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US). Committee to Review Dietary Reference Intakes for Vitamin D and Calcium; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; Dietary reference intakes for vitamin D and calcium; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Larqué, E.; Morales, E.; Leis, R.; Blanco-Carnero, J.E. Maternal and Foetal Health Implications of Vitamin D Status during Pregnancy. Ann. Nutr. Metab. 2018, 72, 179–192. [Google Scholar] [CrossRef]
- Mehrotra, P.; Marwaha, R.K.; Aneja, S.; Seth, A.; Singla, B.M.; Ashraf, G.; Sharma, B.; Sastry, A.; Tandon, N. Hypovitaminosis D and hypocalcemic seizures in infancy. Indian Pediatr. 2009, 47, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Reeve, L.E.; Chesney, R.W.; DeLuca, H.F. Vitamin D of human milk: Identification of biologically active forms. Am. J. Clin. Nutr. 1982, 36, 122–126. [Google Scholar] [CrossRef]
- Novakovic, B.; Galati, J.C.; Chen, A.; Morley, R.; Craig, J.M.; Saffery, R. Maternal vitamin D predominates over genetic factors in determining neonatal circulating vitamin D concentrations. Am. J. Clin. Nutr. 2012, 96, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Braegger, C.; Bronsky, J.; Cai, W.; Campoy, C.; Carnielli, V.; Darmaun, D.; Decsi, T.; Domellöf, M.; Embleton, N.; Fewtrell, M.; et al. ESPGHAN/ESPEN/ESPR/CSPEN guidelines on pediatric parenteral nutrition: Vitamins. Clin. Nutr. 2018, 37, 2366–2378. [Google Scholar] [CrossRef]
- NIH Office of Dietary Supplements. Dietary Supplement Fact Sheet: Vitamin D. Available online: http://ods.od.nih.gov/factsheets/vitamind.asp (accessed on 24 December 2023).
- Delrue, C.; Speeckaert, R.; Delanghe, J.R.; Speeckaert, M.M. Vitamin D Deficiency: An Underestimated Factor in Sepsis? Int. J. Mol. Sci. 2023, 24, 2924. [Google Scholar] [CrossRef] [PubMed]
- McKenna, M.J.; Lyons, O.C.; Flynn, M.A.; Crowley, R.K.; Twomey, P.J.; Kilbane, M.T. COVID-19 pandemic and vitamin D: Rising trends in status and in daily amounts of vitamin D provided by supplements. BMJ Open 2022, 12, e059477. [Google Scholar] [CrossRef]
- Burris, H.H.; Van Marter, L.J.; McElrath, T.F.; Tabatabai, P.; Litonjua, A.A.; Weiss, S.T.; Christou, H. Vitamin D status among preterm and full-term infants at birth. Pediatr. Res. 2014, 75, 75–80. [Google Scholar] [CrossRef]
- Yu, S.B.; Lee, Y.; Oh, A.; Yoo, H.W.; Choi, J.H. Efficacy and safety of parenteral vitamin D therapy in infants and children with vitamin D deficiency caused by intestinal malabsorption. Ann. Pediatr. Endocrinol. Metab. 2020, 25, 112–117. [Google Scholar] [CrossRef]
- Mansur, J.L.; Oliveri, B.; Giacoia, E.; Fusaro, D.; Costanzo, P.R. Vitamin D: Before, during and after Pregnancy: Effect on Neonates and Children. Nutrients 2022, 14, 1900. [Google Scholar] [CrossRef]
- Mosayebi, Z.; Sagheb, S.; Mirzendedel, M.; Movahedian, A.H. E Serum Vitamin D Deficiency in NICU Hospitalized Neonates and Its Association With Neonatal Outcomes. J. Fam. Reprod. Health 2021, 15, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Arnson, Y.; Grinzauz, I.; Itzhaky, D.; Amital, H. Vitamin D deficiency is associated with poor outcomes and increased mortality in severely ill patients. QJM 2012, 105, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Rippel, C.; South, M.; Butt, W.W.; Shekerdemian, L.S. Vitamin D status in critically ill children. Intensive Care Med. 2012, 38, 2055–2062. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Farruggia, M.; Veronese, N.; Barbagallo, M. Vitamin D Sources, Metabolism, and Deficiency: Available Compounds and Guidelines for Its Treatment. Metabolites 2021, 11, 255. [Google Scholar] [CrossRef] [PubMed]
- Perrine, C.G.; Sharma, A.J.; Jefferds, M.E.D.; Serdula, M.K.; Scanlon, K.S. Adherence to vitamin D recommendations among US infants. Pediatrics 2010, 125, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Gallo, S.; Comeau, K.; Vanstone, C.; Agellon, S.; Sharma, A.; Jones, G.; L’abbé, M.; Khamessan, A.; Rodd, C.; Weiler, H. Effect of different dosages of oral vitamin D supplementation on vitamin D status in healthy, breastfed infants: A randomized trial. JAMA 2013, 309, 1785–1792. [Google Scholar] [CrossRef]
- McNally, J.D.; Iliriani, K.; Pojsupap, S.; Sampson, M.; O’hearn, K.; McIntyre, L.; Fergusson, D.; Menon, K. Rapid normalization of vitamin D levels: A meta-analysis. Pediatrics 2015, 135, e152–e166. [Google Scholar] [CrossRef]
- McNally, J.D.; Menon, K. Vitamin D deficiency in surgical congenital heart disease: Prevalence and relevance. Transl. Pediatr. 2013, 2, 99–111. [Google Scholar] [CrossRef]
- Huynh, J.; Lu, T.; Liew, D.; Doery, J.C.; Tudball, R.; Jona, M.; Bhamjee, R.; Rodda, C.P. Vitamin D in newborns. A randomised controlled trial comparing daily and single oral bolus vitamin D in infants. J. Paediatr. Child Health 2017, 53, 163–169. [Google Scholar] [CrossRef]
- Dalle Carbonare, L.; Valenti, M.T.; Del Forno, F.; Caneva, E.; Pietrobelli, A. Vitamin D: Daily vs. Monthly Use in Children and Elderly-What Is Going On? Nutrients 2017, 9, 652. [Google Scholar] [CrossRef]
- Di Marco, N.; Kaufman, J.; Rodda, C.P. Shedding Light on Vitamin D Status and Its Complexities during Pregnancy, Infancy and Childhood: An Australian Perspective. Int. J. Environ. Res. Public Health 2019, 16, 538. [Google Scholar] [CrossRef] [PubMed]
- Schlingmann, K.P.; Kaufmann, M.; Weber, S.; Irwin, A.; Goos, C.; John, U.; Misselwitz, J.; Klaus, G.; Kuwertz-Bröking, E.; Fehrenbach, H.; et al. Mutations in CYP24A1 and idiopathic infantile hypercalcemia. N. Engl. J. Med. 2011, 365, 410–421. [Google Scholar] [CrossRef] [PubMed]
- Vogiatzi, M.G.; Jacobson-Dickman, E.; DeBoer, M.D. DeBoer, for the Drugs, and Therapeutics Committee of The Pediatric Endocrine Society, Vitamin D Supplementation and Risk of Toxicity in Pediatrics: A Review of Current Literature. J. Clin. Endocrinol. Metab. 2014, 99, 1132–1141. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LOT 1 | LOT 2 | LOT 3 | Overall Patients | ||
|---|---|---|---|---|---|
| Gender | Female | 28 (56%) | 18 (36%) | 21 (42%) | 67 (44.6%) |
| Male | 22 (44%) | 32 (64%) | 29 (58%) | 83 (55.3%) | |
| Gestational age | Term | 34 (68%) | 36 (72%) | 37 (74%) | 107 (71.3%) |
| Pre-term | 16 (32%) | 14 (28%) | 13 (26%) | 43 (28.6%) | |
| Associated comorbidities | Cardiac malformation | 21 (42%) | 25 (50%) | 20 (40%) | 66 (44%) |
| Respiratory Disease | 42 (84%) | 39 (78%) | 46 (92%) | 127 (84.6%) | |
| Gastrointestinal malformation | 11 (22%) | 12 (24%) | 17 (34%) | 40 (26.6%) | |
| Necrotizing enterocolitis | 2 (4%) | 3 (6%) | 2 (4%) | 7 (4.6%) | |
| Tumor | 3 (6%) | 2 (4%) | 3 (6%) | 8 (5.3%) | |
| Neurologic disorder | 12 (24%) | 18 (36%) | 13 (26%) | 43 (28.6%) | |
| Renal Disease | 7 (14%) | 8 (16%) | 8 (16%) | 23 (15.3%) | |
| Surgical condition | 29 (58%) | 17 (34%) | 33 (66%) | 79 (52.6%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cirstoveanu, C.; Ionita, I.; Georgescu, C.; Heriseanu, C.; Vasile, C.M.; Bizubac, M. Intermittent High-Dose Vitamin D3 Administration in Neonates with Multiple Comorbidities and Vitamin D Insufficiency. Children 2024, 11, 328. https://doi.org/10.3390/children11030328
Cirstoveanu C, Ionita I, Georgescu C, Heriseanu C, Vasile CM, Bizubac M. Intermittent High-Dose Vitamin D3 Administration in Neonates with Multiple Comorbidities and Vitamin D Insufficiency. Children. 2024; 11(3):328. https://doi.org/10.3390/children11030328
Chicago/Turabian StyleCirstoveanu, Catalin, Iulia Ionita, Carmina Georgescu, Carmen Heriseanu, Corina Maria Vasile, and Mihaela Bizubac. 2024. "Intermittent High-Dose Vitamin D3 Administration in Neonates with Multiple Comorbidities and Vitamin D Insufficiency" Children 11, no. 3: 328. https://doi.org/10.3390/children11030328