
Maternal Wellbeing Five Years after a Very Preterm Delivery: Prevalence and Influencing Factors in a European Cohort

 , , ,
on behalf of the SHIPS Research Group
, , ,
on behalf of the SHIPS Research Group
Abstract
:1. Introduction
2. Materials and Methods
- (a)
- Perinatal and neonatal characteristics: GA at birth in completed weeks (analyzed in 4 groups: ≤25, 26–27, 28–29, 30–31), small for GA (SGA) (<3rd percentile, 3rd–9th percentile, ≥10th percentile based on intrauterine reference) [27], BPD (defined as supplemental oxygen at 36 weeks of postmenstrual age), any severe non-respiratory morbidity at discharge (defined as at least one of intraventricular haemorrhage grade III or IV, cystic periventricular leukomalacia, ROP stages III to V, or necrotizing enterocolitis requiring surgery or peritoneal drainage); maternal characteristics: parity (0; 1; ≥2), preterm premature rupture of membranes (PPROM) > 12 h, having one of preeclampsia, eclampsia or HELLP (haemolysis, elevated liver enzymes, and low platelets) syndrome, and type of pregnancy (singleton; multiples). In case of multiples, the most severe condition was retained (i.e., if one twin had BPD and the other did not, the mother was categorized as having a child with BPD).
- (b)
- Sociodemographic characteristics of the mother: maternal age at delivery (<25 years; 25–34 years; ≥35 years), maternal country of birth (native born; other European country; non-European country), maternal educational level based on the International Standard Classification of Education (ISCED) (low, ISCED 0–2; intermediate, ISCED 3–5; high, ISCED 6–8) [28,29], parental cohabiting status (single/other; married/couple/cohabiting) and household unemployment status (employed (part-/fulltime); at least one parent unemployed).
- (c)
- Child’s health and developmental characteristics at five years of age: sensory impairment (moderate to severe visual or hearing impairment), cerebral palsy, developmental delay, speech delay, attention deficit hyperactivity disorder (ADHD), autism, epilepsy (diagnoses as reported by the parents). For multiples, the same approach as for neonatal morbidities was applied with the most severe condition retained. For further analyses, the child’s health and developmental condition was categorized as follows: any severe health problems at five (defined as at least one of severe or moderate hearing or visual impairment, cerebral palsy, ADHD, autism, epilepsy) and any developmental delay at five (defined as at least one of developmental or speech delay).
3. Results
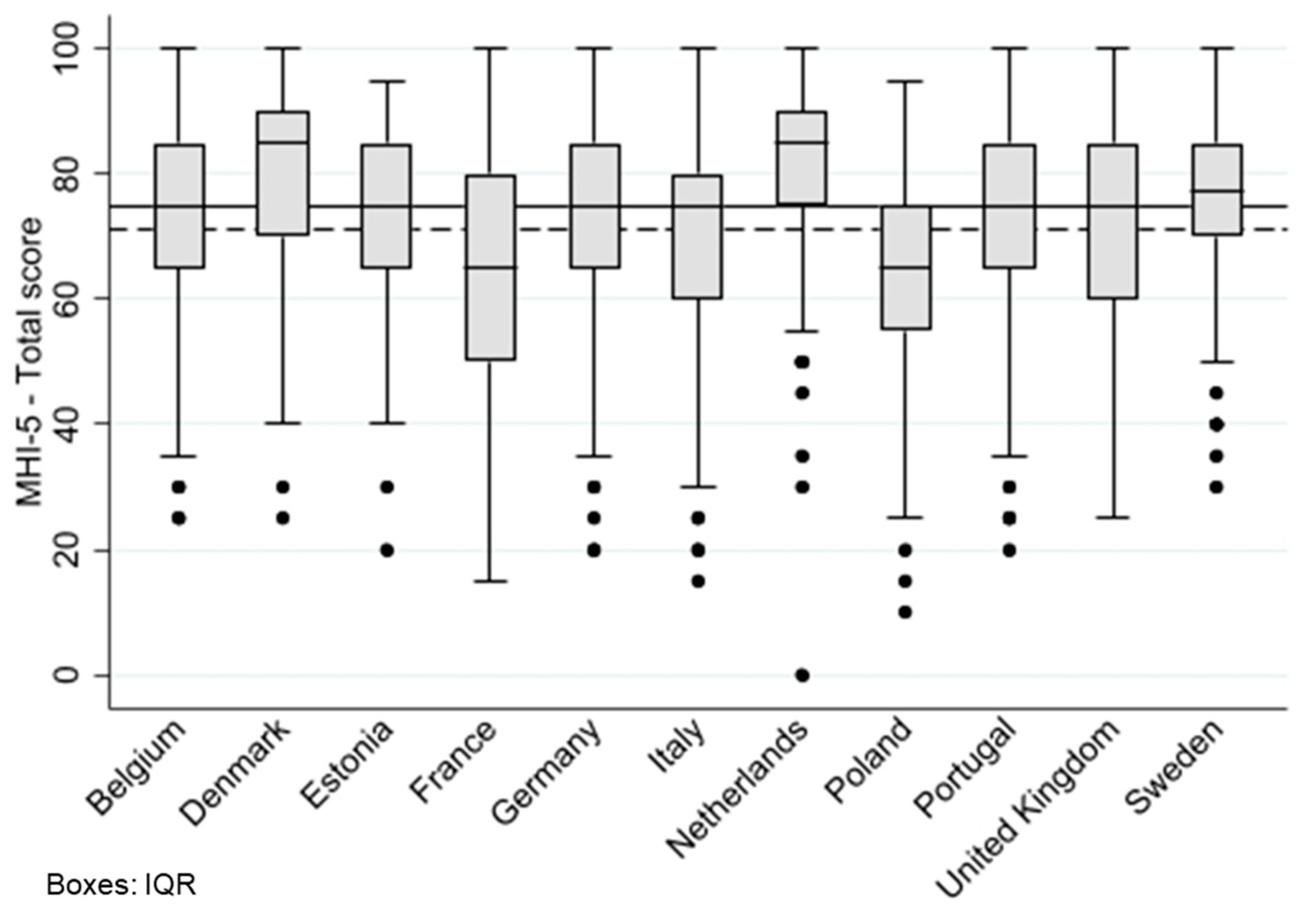
3.1. Variations in Maternal Emotional Wellbeing between EPICE-SHIPS Country Cohorts
3.2. Emotional Wellbeing of Mothers and Associated Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Widding, U.; Hägglöf, B.; Farooqi, A. Parents of preterm children narrate constructive aspects of their experiences. J. Clin. Nurs. 2019, 28, 4110–4118. [Google Scholar] [CrossRef] [PubMed]
- Provenzi, L.; Barello, S.; Fumagalli, M.; Graffigna, G.; Sirgiovanni, I.; Savarese, M.; Montirosso, R. A Comparison of Maternal and Paternal Experiences of Becoming Parents of a Very Preterm Infant. J. Obs. Gynecol. Neonatal Nurs. 2016, 45, 528–541. [Google Scholar] [CrossRef] [PubMed]
- Saigal, S.; Doyle, L.W. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet 2008, 371, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.; Marlow, N. Early and long-term outcome of infants born extremely preterm. Arch. Dis. Child. 2017, 102, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Garel, M.; Dardennes, M.; Blondel, B. Mothers’ psychological distress 1 year after very preterm childbirth. Results of the EPIPAGE qualitative study. Child Care Health Dev. 2007, 33, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Pace, C.C.; Spittle, A.J.; Molesworth, C.M.; Lee, K.J.; Northam, E.A.; Cheong, J.L.; Davis, P.G.; Doyle, L.W.; Treyvaud, K.; Anderson, P.J. Evolution of Depression and Anxiety Symptoms in Parents of Very Preterm Infants During the Newborn Period. JAMA Pediatr. 2016, 170, 863–870. [Google Scholar] [CrossRef]
- Holditch-Davis, D.; Santos, H.; Levy, J.; White-Traut, R.; O’Shea, T.M.; Geraldo, V.; David, R. Patterns of psychological distress in mothers of preterm infants. Infant. Behav. Dev. 2015, 41, 154–163. [Google Scholar] [CrossRef]
- Ballantyne, M.; Orava, T.; Bernardo, S.; McPherson, A.C.; Church, P.; Fehlings, D. Parents’ early healthcare transition experiences with preterm and acutely ill infants: A scoping review. Child Care Health Dev. 2017, 43, 783–796. [Google Scholar] [CrossRef]
- Ionio, C.; Colombo, C.; Brazzoduro, V.; Mascheroni, E.; Confalonieri, E.; Castoldi, F.; Lista, G. Mothers and Fathers in NICU: The Impact of Preterm Birth on Parental Distress. Eur. J. Psychol. 2016, 12, 604–621. [Google Scholar] [CrossRef]
- Barthel, D.; Göbel, A.; Barkmann, C.; Helle, N.; Bindt, C. Does Birth-Related Trauma Last? Prevalence and Risk Factors for Posttraumatic Stress in Mothers and Fathers of VLBW Preterm and Term Born Children 5 Years After Birth. Front. Psychiatry 2020, 11, 575429. [Google Scholar] [CrossRef]
- Landsem, I.P.; Handegård, B.H.; Tunby, J.; Ulvund, S.E.; Rønning, J.A. Early intervention program reduces stress in parents of preterms during childhood, a randomized controlled trial. Trials 2014, 15, 387. [Google Scholar] [CrossRef] [PubMed]
- Farooqi, A.; Hagglof, B.; Sedin, G.; Gothefors, L.; Serenius, F. Chronic conditions, functional limitations, and special health care needs in 10- to 12-year-old children born at 23 to 25 weeks’ gestation in the 1990s: A Swedish national prospective follow-up study. Pediatrics 2006, 118, e1466–e1477. [Google Scholar] [CrossRef] [PubMed]
- Roque, A.T.F.; Lasiuk, G.C.; Radünz, V.; Hegadoren, K. Scoping Review of the Mental Health of Parents of Infants in the NICU. J. Obstet. Gynecol. Neonatal Nurs. 2017, 46, 576–587. [Google Scholar] [CrossRef] [PubMed]
- Cacciani, L.; Di Lallo, D.; Piga, S.; Corchia, C.; Carnielli, V.; Chiandotto, V.; Fertz, M.; Miniaci, S.; Rusconi, F.; Caravale, B.; et al. Interaction of child disability and stressful life events in predicting maternal psychological health. Results of an area-based study of very preterm infants at two years corrected age. Res. Dev. Disabil. 2013, 34, 3433–3441. [Google Scholar] [CrossRef] [PubMed]
- Schappin, R.; Wijnroks, L.; Uniken Venema, M.M.A.T.; Jongmans, M.J. Rethinking stress in parents of preterm infants: A meta-analysis. PLoS ONE 2013, 8, e54992. [Google Scholar] [CrossRef]
- Skreden, M.; Skari, H.; Björk, M.D.; Malt, U.F.; Veenstra, M.; Faugli, A.; Avitsland, T.L.; Emblem, R. Psychological distress in mothers and fathers of preschool children: A 5-year follow-up study after birth. BJOG Int. J. Obstet. Gynaecol. 2008, 115, 462–471. [Google Scholar] [CrossRef]
- Yaari, M.; Treyvaud, K.; Lee, K.J.; Doyle, L.W.; Anderson, P.J. Preterm Birth and Maternal Mental Health: Longitudinal Trajectories and Predictors. J. Pediatr. Psychol. 2019, 44, 736–747. [Google Scholar] [CrossRef]
- Zeitlin, J.; Maier, R.F.; Cuttini, M.; Aden, U.; Boerch, K.; Gadzinowski, J.; Jarreau, P.H.; Lebeer, J.; Norman, M.; Pedersen, P.; et al. Cohort profile: Effective Perinatal Intensive Care in Europe (EPICE) very preterm birth cohort. Int. J. Epidemiol. 2020, 49, 372–386. [Google Scholar] [CrossRef]
- Ancel, P.Y.; Goffinet, F. EPIPAGE 2: A preterm birth cohort in France in 2011. BMC Pediatr. 2014, 14, 97. [Google Scholar] [CrossRef]
- Rumpf, H.J.; Meyer, C.; Hapke, U.; John, U. Screening for mental health: Validity of the MHI-5 using DSM-IV Axis I psychiatric disorders as gold standard. Psychiatry Res. 2001, 105, 243–253. [Google Scholar] [CrossRef]
- Kelly, M.J.; Dunstan, F.D.; Lloyd, K.; Fone, D.L. Evaluating cutpoints for the MHI-5 and MCS using the GHQ-12: A comparison of five different methods. BMC Psychiatry 2008, 8, 10. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- van den Beukel, T.O.; Siegert, C.E.H.; van Dijk, S.; Ter Wee, P.M.; Dekker, F.W.; Honig, A. Comparison of the SF-36 Five-item Mental Health Inventory and Beck Depression Inventory for the screening of depressive symptoms in chronic dialysis patients. Nephrol. Dial. Transplant. 2012, 27, 4453–4457. [Google Scholar] [CrossRef] [PubMed]
- Robine, J.M.; Jagger, C. Creating a coherent set of indicators to monitor health across Europe: The Euro-REVES 2 project. Eur. J. Public. Health 2003, 13, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr. SF-36 health survey update. Spine 2000, 25, 3130–3139. [Google Scholar] [CrossRef] [PubMed]
- McHorney, C.A.; Ware, J.E., Jr.; Lu, J.F.; Sherbourne, C.D. The MOS 36-item Short-Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med. Care 1994, 32, 40–66. [Google Scholar] [CrossRef] [PubMed]
- Zeitlin, J.; Bonamy, A.E.; Piedvache, A.; Cuttini, M.; Barros, H.; Van Reempts, P.; Mazela, J.; Jarreau, P.H.; Gortner, L.; Draper, E.S.; et al. Variation in term birthweight across European countries affects the prevalence of small for gestational age among very preterm infants. Acta Paediatr. 2017, 106, 1447–1455. [Google Scholar] [CrossRef]
- Sentenac, M.; Johnson, S.; Charkaluk, M.-L.; Sëppanen, A.-V.; Aden, U.; Cuttini, M.; Maier, R.; Mannamaa, M.; Zeitlin, J.; EPICE Group. Maternal education and language development at 2 years corrected age in children born very preterm: Results from a European population-based cohort study. J. Epidemiol. Community Health 2020, 74, 346–353. [Google Scholar] [CrossRef]
- UNESCO Institute for Statistics. International Standard Classification of Education ISCED 2011. Available online: http://uis.unesco.org/sites/default/files/documents/international-standard-classification-of-education-isced-2011-en.pdf (accessed on 26 December 2023).
- Wechsler, D. Wechsler Preschool and Primary Scale of Intelligence, 4th ed.; Pearson: London, UK, 1989; Volume 2002, p. 2012. [Google Scholar]
- Petermann, F.; Ricken, G.; Schuck, K.; Preuß, U. Wechsler Preschool and Primary Scale of Intelligence-III (WPPSI-III)—Deutsche Version, 3., Überarbeitete und Erweiterte Auflage, Manual, 3rd ed.; Pearson: London, UK, 2014. [Google Scholar]
- Henderson, S.E. Movement Assessment Battery for Children, 3rd ed.; Pearson: London, UK, 2007. [Google Scholar]
- Bonnet, C.; Blondel, B.; Piedvache, A.; Wilson, E.; Bonamy, A.E.; Gortner, L.; Rodrigues, C.; van Heijst, A.; Draper, E.S.; Cuttini, M.; et al. Low breastfeeding continuation to 6 months for very preterm infants: A European multiregional cohort study. Matern. Child. Nutr. 2018, 15, e12657. [Google Scholar] [CrossRef]
- Seppänen, A.V.; Sauvegrain, P.; Draper, E.S.; Toome, L.; El Rafei, R.; Petrou, S.; Barros, H.; Zimmermann, L.J.I.; Cuttini, M.; Zeitlin, J. Parents’ ratings of post-discharge healthcare for their children born very preterm and their suggestions for improvement: A European cohort study. Pediatr. Res. 2020, 89, 1004–1012. [Google Scholar] [CrossRef]
- Piedvache, A.; van Buuren, S.; Barros, H.; Ribeiro, A.I.; Draper, E.; Zeitlin, J. Strategies for assessing the impact of loss to follow-up on estimates of neurodevelopmental impairment in a very preterm cohort at 2 years of age. BMC Med. Res. Methodol. 2021, 21, 118. [Google Scholar] [CrossRef] [PubMed]
- Aubert, A.M.; Costa, R.; Ådén, U.; Cuttini, M.; Männamaa, M.; Pierrat, V.; Sarrechia, I.; van Heijst, A.F.; Zemlin, M.; Johnson, S.; et al. Movement Difficulties at Age Five Among Extremely Preterm Infants. Pediatrics 2022, 149, e2021054920. [Google Scholar] [CrossRef] [PubMed]
- Cole, S.R.; Hernán, M.A. Constructing inverse probability weights for marginal structural models. Am. J. Epidemiol. 2008, 168, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Seaman, S.R.; White, I.R. Review of inverse probability weighting for dealing with missing data. Stat. Methods Med. Res. 2013, 22, 278–295. [Google Scholar] [CrossRef] [PubMed]
- Royston, P.; White, I.R. Multiple Imputation by Chained Equations (MICE): Implementation in Stata. J. Stat. Softw. 2011, 45, 1–20. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Kosinski, M.; Gandek, B.; Aaronson, N.K.; Apolone, G.; Bech, P.; Brazier, J.; Bullinger, M.; Kaasa, S.; Leplège, A.; et al. The factor structure of the SF-36 Health Survey in 10 countries: Results from the IQOLA Project. International Quality of Life Assessment. J. Clin. Epidemiol. 1998, 51, 1159–1165. [Google Scholar] [CrossRef] [PubMed]
- Nordheim, T.; Rustøen, T.; Solevåg, A.L.; Småstuen, M.C.; Nakstad, B. Hope in Parents of Very-Low Birth Weight Infants and its Association with Parenting Stress and Quality of Life. J. Pediatr. Nurs. 2018, 38, e53–e58. [Google Scholar] [CrossRef]
- Spittle, A.J.; Barton, S.; Treyvaud, K.; Molloy, C.S.; Doyle, L.W.; Anderson, P.J. School-Age Outcomes of Early Intervention for Preterm Infants and Their Parents: A Randomized Trial. Pediatrics 2016, 138, e20161363. [Google Scholar] [CrossRef]
- Winter, L.; Colditz, P.B.; Sanders, M.R.; Boyd, R.N.; Pritchard, M.; Gray, P.H.; Whittingham, K.; Forrest, K.; Leeks, R.; Webb, L.; et al. Depression, posttraumatic stress and relationship distress in parents of very preterm infants. Arch. Womens Ment. Health 2018, 21, 445–451. [Google Scholar] [CrossRef]
- Sullivan, M.; Karlsson, J. The Swedish SF-36 Health Survey III. Evaluation of criterion-based validity: Results from normative population. J. Clin. Epidemiol. 1998, 51, 1105–1113. [Google Scholar] [CrossRef]
- Miles, M.S.; Holditch-Davis, D.; Schwartz, T.A.; Scher, M. Depressive symptoms in mothers of prematurely born infants. J. Dev. Behav. Pediatr. 2007, 28, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.R.; Bora, S.; Austin, N.C.; Woodward, L.J. Mental health, neurodevelopmental, and family psychosocial profiles of children born very preterm at risk of an early-onset anxiety disorder. Dev. Med. Child. Neurol. 2021, 63, 954–962. [Google Scholar] [CrossRef] [PubMed]
- Huhtala, M.; Korja, R.; Lehtonen, L.; Haataja, L.; Lapinleimu, H.; Rautava, P.; Group, P.S. Associations between parental psychological well-being and socio-emotional development in 5-year-old preterm children. Early Hum. Dev. 2014, 90, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Seppänen, A.V.; Draper, E.S.; Petrou, S.; Barros, H.; Aubert, A.M.; Andronis, L.; Kim, S.W.; Maier, R.F.; Pedersen, P.; Gadzinowski, J.; et al. High Healthcare Use at Age 5 Years in a European Cohort of Children Born Very Preterm. J. Pediatr. 2022, 243, 69–77.e9. [Google Scholar] [CrossRef] [PubMed]
- Shaw, R.J.; Sweester, C.J.; St John, N.; Lilo, E.; Corcoran, J.B.; Jo, B.; Howell, S.H.K.; Benitz, W.E.; Feinstein, N.; Melnyk, B.; et al. Prevention of postpartum traumatic stress in mothers with preterm infants: Manual development and evaluation. Issues Ment. Health Nurs. 2013, 34, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Gelaye, B.; Sanchez, S.E.; Andrade, A.; Gómez, O.; Coker, A.L.; Dole, N.; Rondon, M.B.; Williams, M.A. Association of antepartum depression, generalized anxiety, and posttraumatic stress disorder with infant birth weight and gestational age at delivery. J. Affect. Disord. 2020, 262, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Mahrer, N.E.; Guardino, C.M.; Hobel, C.; Dunkel Schetter, C. Maternal Stress Before Conception Is Associated with Shorter Gestation. Ann. Behav. Med. 2021, 55, 242–252. [Google Scholar] [CrossRef]
- Treyvaud, K.; Aldana, A.C.; Scratch, S.E.; Ure, A.M.; Pace, C.C.; Doyle, L.W.; Anderson, P.J. The influence of multiple birth and bereavement on maternal and family outcomes 2 and 7years after very preterm birth. Early Hum. Dev. 2016, 100, 1–5. [Google Scholar] [CrossRef]
- Singer, L.T.; Fulton, S.; Kirchner, H.L.; Eisengart, S.; Lewis, B.; Short, E.; Min, M.O.; Kercsmar, C.; Baley, J.E. Parenting very low birth weight children at school age: Maternal stress and coping. J. Pediatr. 2007, 151, 463–469. [Google Scholar] [CrossRef]
- Seppänen, A.V.; Barros, H.; Draper, E.S.; Petrou, S.; Andronis, L.; Kim, S.; Maier, R.F.; Pedersen, P.; Gadzinowski, J.; Pierrat, V.; et al. Variation in follow-up for children born very preterm in Europe. Eur. J. Public Health 2023, ckad192. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sociodemographic Characteristics | MHI-5 Scores | |||
|---|---|---|---|---|
| n | Mean | SD | p-Value | |
| Maternal age at childbirth | 0.03 | |||
| <25 years | 313 | 70.3 | 16.8 | |
| 25–34 years | 1499 | 72.0 | 16.6 | |
| ≥35 years | 785 | 70.2 | 16.8 | |
| Maternal country of birth | <0.01 | |||
| Native born | 2129 | 71.7 | 16.4 | |
| Other European country | 164 | 71.6 | 16.4 | |
| Non-European country | 306 | 68.2 | 18.7 | |
| Maternal educational level | <0.01 | |||
| Low (ISCED 0–2) | 431 | 68.9 | 18.4 | |
| Intermediate (ISCED 3–5) | 1092 | 71.3 | 16.7 | |
| High (ISCED 6–8) | 1072 | 72.2 | 15.9 | |
| Parental cohabiting status | <0.001 | |||
| Single/Other | 318 | 66.6 | 19.8 | |
| Married/Couple/Cohabiting | 2282 | 71.9 | 16.1 | |
| Household unemployment situation | <0.001 | |||
| Employed (part-/fulltime) * | 2304 | 71.8 | 16.4 | |
| At least one parent unemployed | 294 | 67.3 | 18.7 | |
| Perinatal and neonatal characteristics | MHI-5 scores | |||
| n | Mean | SD | p-Value | |
| Parity | <0.001 | |||
| Zero | 1548 | 72.6 | 15.9 | |
| One | 660 | 70.3 | 16.7 | |
| Two or more | 368 | 67.5 | 19.2 | |
| Antepartum haemorrhage after week 20 | 0.26 | |||
| No | 2040 | 71.5 | 16.4 | |
| Yes | 502 | 70.6 | 17.8 | |
| Admission for preterm labour or contractions after week 20 | 0.18 | |||
| No | 1430 | 71.0 | 16.6 | |
| Yes | 1118 | 71.9 | 16.7 | |
| Preterm premature rupture of membranes | 0.02 | |||
| No | 1903 | 71.7 | 16.5 | |
| Yes | 665 | 69.9 | 17.2 | |
| Mother has one of preeclampsia, eclampsia or HELLP syndrome | 0.31 | |||
| No | 2069 | 71.1 | 16.6 | |
| Yes | 499 | 71.9 | 17.0 | |
| Multiples | 0.34 | |||
| Singleton | 2070 | 71.3 | 16.8 | |
| Multiple no death | 446 | 70.7 | 16.5 | |
| Multiple with at least one child death | 89 | 73.5 | 15.0 | |
| Sex of the baby | 0.29 | |||
| Male | 1402 | 71.0 | 16.5 | |
| Female | 1203 | 71.6 | 17.0 | |
| Gestational age | 0.48 | |||
| ≤25 weeks | 235 | 71.1 | 16.1 | |
| 26–27 weeks | 489 | 70.2 | 17.8 | |
| 28–29 weeks | 670 | 71.6 | 16.3 | |
| 30–31 weeks | 1211 | 71.5 | 16.6 | |
| Small for gestational age | 0.84 | |||
| <3rd percentile | 568 | 71.6 | 16.4 | |
| 3rd–9th percentile | 298 | 71.1 | 16.8 | |
| ≥10th percentile | 1739 | 71.2 | 16.8 | |
| Mothers with at least one child who died before 2 years of age | 0.32 | |||
| No | 2523 | 71.2 | 16.8 | |
| Yes | 82 | 73.1 | 14.9 | |
| Excluding the 89 mothers with at least one child who died before 2 years of age (n = 2516) | ||||
| At least one child had a BPD ** | 0.46 | |||
| No | 2157 | 71.3 | 16.8 | |
| Yes | 359 | 70.6 | 16.5 | |
| At least one child had a congenital anomaly | 0.06 | |||
| No | 2364 | 71.5 | 16.7 | |
| Yes | 241 | 69.3 | 16.8 | |
| At least one child had a severe non-respiratory morbidity at discharge *** | 0.0012 | |||
| No | 2232 | 71.6 | 16.6 | |
| Yes | 284 | 68.2 | 17.7 | |
| Child’s Health and Developmental Characteristics at Five Years | MHI-5 Scores | |||
|---|---|---|---|---|
| n | Mean | SD | p-Value | |
| Sensory impairment | <0.001 | |||
| None/mild | 2492 | 71.6 | 16.6 | |
| Moderate/severe | 113 | 63.3 | 18.2 | |
| Cerebral palsy | <0.001 | |||
| No | 2444 | 71.7 | 16.4 | |
| Yes | 161 | 65.1 | 19.6 | |
| Developmental delay * | <0.001 | |||
| No | 1781 | 73.9 | 15.3 | |
| Yes | 310 | 65.9 | 18.3 | |
| Speech delay * | <0.001 | |||
| No | 1734 | 73.6 | 15.5 | |
| Yes | 357 | 68.4 | 17.8 | |
| ADHD * | <0.001 | |||
| No | 2044 | 72.9 | 15.9 | |
| Yes | 47 | 64.0 | 19.1 | |
| Autism | <0.001 | |||
| No | 2545 | 71.5 | 16.6 | |
| Yes | 60 | 62.8 | 18.3 | |
| Epilepsy | <0.03 | |||
| No | 2554 | 71.4 | 16.7 | |
| Yes | 51 | 66.0 | 18.8 | |
| At least one severe diagnose or severe vision/hearing impairment | <0.001 | |||
| No | 1825 | 73.8 | 15.4 | |
| Yes | 266 | 65.6 | 18.1 | |
| At least one of developmental or speech delay | <0.001 | |||
| No | 1610 | 74.2 | 15.1 | |
| Yes | 481 | 67.7 | 17.8 | |
| only for EPT (n = 724) ** | ||||
| Motor impairment (MABC-2 ≤5th percentile) | 0.0087 | |||
| No | 492 | 71.7 | 16.7 | |
| Yes | 232 | 68.1 | 18.3 | |
| Cognitive impairment (IQ <70) | <0.001 | |||
| None/mild | 646 | 71.4 | 16.8 | |
| Moderate/severe | 78 | 63.0 | 19.7 | |
| Multilevel Multivariate Linear Regression * | (a) Perinatal, Neonatal and Sociodemographic Characteristics | (b) Perinatal, Neonatal, Sociodemographic and Child’s Health and Developmental Characteristics at Five Years ** | (c) Model b Excluding the Variables Developmental Delay, Speech Delay and ADHD (Not Available in France) *** | |||
|---|---|---|---|---|---|---|
| Coef. | [95% CI] | Coef. | [95% CI] | Coef. | [95% CI] | |
| Perinatal and neonatal characteristics | ||||||
| Parity | ||||||
| Zero | Ref. | Ref. | Ref. | |||
| One | −2.3 | [−3.8; −0.8] | −2.5 | [−4.0; −1.0] | −2.3 | [−3.7; −0.9] |
| Two or more | −5.0 | [−7.8; −2.2] | −5.2 | [−8.4; −2.0] | −4.9 | [−7.7; −2.0] |
| Antepartum haemorrhage after week 20 | ||||||
| No | Ref. | Ref. | Ref. | |||
| Yes | 0.1 | [−2.0; 2.1] | 0.2 | [−2.4; 2.7] | 0.3 | [−1.8; 2.4] |
| Admission for preterm labor or contractions after week 20 | ||||||
| No | Ref. | Ref. | Ref. | |||
| Yes | 1.2 | [−0.4; 2.7] | 1.1 | [−0.7; 2.8] | 1.1 | [−0.5; 2.7] |
| Mother has one of preeclampsia, eclampsia or HELLP syndrome | ||||||
| No | Ref. | Ref. | Ref. | |||
| Yes | 0.9 | [−1.1; 3.0] | 1.4 | [−0.7; 3.5] | 0.7 | [−1.3; 2.8] |
| Preterm premature rupture of membranes | ||||||
| No | Ref. | Ref. | Ref. | |||
| Yes | −0.6 | [−2.1; 0.9] | −0.5 | [−2.6; 1.6] | −0.7 | [−2.4; 1.0] |
| Multiples | ||||||
| Singleton | Ref. | Ref. | Ref. | |||
| Multiples no death | −1.6 | [−3.3; 0.1] | −1.7 | [−3.5; 0.2] | −1.4 | [−3.2; 0.4] |
| Sex of the baby | ||||||
| Male | Ref. | Ref. | Ref. | |||
| Female | 0.4 | [−0.9; 1.7] | −0.1 | [−1.4; 1.3] | 0.3 | [−1.0; 1.6] |
| Gestational age | ||||||
| ≤25 weeks | 1.1 | [−1.7; 4.0] | 2.0 | [−1.4; 5.3] | 1.4 | [−1.5; 4.3] |
| 26–27 weeks | −0.3 | [−2.5; 1.9] | 0.4 | [−1.7; 2.4] | −0.3 | [−2.4; 1.8] |
| 28–29 weeks | 1.0 | [−0.3; 2.4] | 1.5 | [0.2; 2.4] | 1.0 | [−0.3; 2.4] |
| 30–31 weeks | Ref. | Ref. | Ref. | |||
| Small for gestational age | ||||||
| <3rd percentile | 0.1 | [−2.8; 3.1] | −0.4 | [−3.5; 2.8] | −0.0 | [−3.0; 3.0] |
| 3rd–9th percentile | Ref. | Ref. | Ref. | |||
| ≥10th percentile | −0.4 | [−2.6; 1.7] | −0.8 | [−3.3; 1.7] | −0.6 | [−2.9; 1.7] |
| At least one child had a BPD | ||||||
| No | Ref. | Ref. | Ref. | |||
| Yes | −0.5 | [−2.3; 1.4] | 0.7 | [−0.1; 2.4] | −0.2 | [−1.8; 1.5] |
| At least one child had a congenital anomaly | ||||||
| No | Ref. | Ref. | Ref. | |||
| Yes | 0.2 | [−2.5; 3.0] | 2.3 | [0.4; 4.2] | 0.7 | [−2.0; 3.4] |
| At least one child had any severe non-respiratory morbidity at discharge **** | ||||||
| No | Ref. | Ref. | Ref. | |||
| Yes | −3.8 | [−6.6; −1.0] | −3.1 | [−5.9; −0.4] | −2.5 | [−5.7; 0.6] |
| Sociodemographic characteristics | ||||||
| Maternal age at childbirth | ||||||
| <25 years | −1.0 | [−2.6; 0.6] | −1.1 | [−2.7; 0.5] | −0.9 | [−2.4; 0.5] |
| 25–34 years | Ref. | Ref. | Ref. | |||
| ≥35 years | −1.2 | [−3.0; 0.6] | −1.0 | [−2.8; 0.9] | −1.3 | [−3.0; 0.4] |
| Maternal country of birth | ||||||
| Native born | Ref. | Ref. | Ref. | |||
| Other European country | −0.4 | [−3.3; 2.5] | −0.1 | [−2.9; 2.7] | −0.7 | [−3.6; 2.1] |
| Non-European country | −1.2 | [−3.6; 1.6] | −0.4 | [−3.7; 2.8] | −1.3 | [−3.9; 1.4] |
| Maternal educational level | ||||||
| Low (ISCED 0–2) | −1.2 | [−3.4; 1.0] | −1.9 | [−4.4; 0.6] | −1.3 | [−3.5; 0.9] |
| Intermediate (ISCED 3–5) | Ref. | Ref. | Ref. | |||
| High (ISCED 6–8) | 0.0 | [−1.2; 1.3] | −0.5 | [−2.0; 0.9] | −0.1 | [−1.3; 1.2] |
| Parental cohabiting status | ||||||
| Single/Other | −6.0 | [−8.8; −3.1] | −5.8 | [−8.8; −2.9] | −5.8 | [−8.4; −3.2] |
| Married/Couple/Cohabiting | Ref. | Ref. | Ref. | |||
| Household unemployment situation | ||||||
| Employed (part-/fulltime) ***** | Ref. | Ref. | Ref. | |||
| At least one parent unemployed | −1.6 | [−2.7; −0.4] | −1.1 | [−2.8; −0.0] | −1.6 | [−2.8; −0.5] |
| Child’s health and developmental characteristics at five years | ||||||
| Sensory impairment | ||||||
| None/mild | Ref. | Ref. | ||||
| Moderate/severe | −4.0 | [−7.3; −0.7] | −6.1 | [−9.2; −3.1] | ||
| Cerebral palsy | ||||||
| No | Ref. | Ref. | ||||
| Yes | 1.3 | [−0.9; 3.5] | −1.0 | [−3.4; 1.3] | ||
| Autism | ||||||
| No | Ref. | Ref. | ||||
| Yes | −5.0 | [−10.8; 0.7] | −6.4 | [−11.0; −1.8] | ||
| Epilepsy | ||||||
| No | Ref. | Ref. | ||||
| Yes | −2.1 | [−5.3; 1.2] | −3.7 | [−7.2; −0.2] | ||
| Developmental delay | ||||||
| No | Ref. | |||||
| Yes | −3.7 | [−8.0; −0.5] | ||||
| Speech delay | ||||||
| No | Ref. | |||||
| Yes | −0.8 | [−5.8; 4.1] | ||||
| ADHD | ||||||
| No | Ref. | |||||
| Yes | −5.1 | [−9.1; −1.1] | ||||
| At least one of developmental or speech delay | ||||||
| No | Ref. | |||||
| Yes | −0.8 | [−6.2; 5.0] | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wohlers, L.; Maier, R.F.; Cuttini, M.; Wilson, E.; Benhammou, V.; Lebeer, J.; Laroche, S.; Sarrechia, I.; Petrou, S.; Thiele, N.; et al. Maternal Wellbeing Five Years after a Very Preterm Delivery: Prevalence and Influencing Factors in a European Cohort. Children 2024, 11, 61. https://doi.org/10.3390/children11010061
Wohlers L, Maier RF, Cuttini M, Wilson E, Benhammou V, Lebeer J, Laroche S, Sarrechia I, Petrou S, Thiele N, et al. Maternal Wellbeing Five Years after a Very Preterm Delivery: Prevalence and Influencing Factors in a European Cohort. Children. 2024; 11(1):61. https://doi.org/10.3390/children11010061
Chicago/Turabian StyleWohlers, Lena, Rolf F. Maier, Marina Cuttini, Emilija Wilson, Valérie Benhammou, Jo Lebeer, Sabine Laroche, Iemke Sarrechia, Stavros Petrou, Nicole Thiele, and et al. 2024. "Maternal Wellbeing Five Years after a Very Preterm Delivery: Prevalence and Influencing Factors in a European Cohort" Children 11, no. 1: 61. https://doi.org/10.3390/children11010061