
Behavior Rating Inventory of Executive Function in Preschool (BRIEF-P) and Attention-Deficit and Hyperactivity Disorders (ADHD): A Systematic Review and Meta-Analysis of Floor and Ceiling Effects



Abstract
:1. Introduction
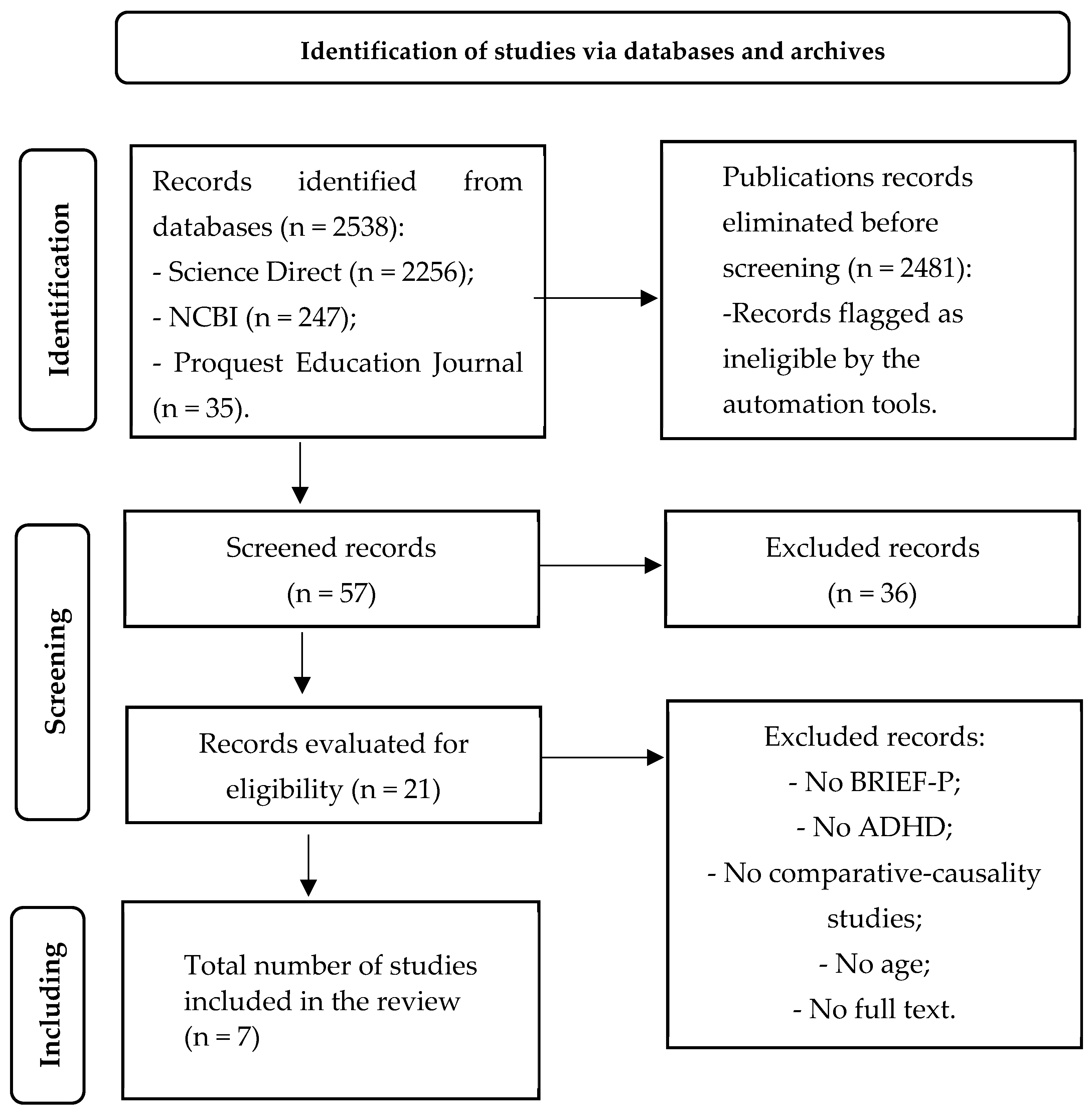
2. Method
Regarding the floor effect (minimum score), are there statistically significant differences in the executive profile of preschool children with ADHD versus typically developing children?
In terms of the ceiling effect (maximum score), are there significant differences in the executive profile of preschool children with ADHD versus typically developing children?
Search Strategy
- (i)
- Science Direct ◊
- -
- (Attention deficit hyperactivity disorder or ADHD) and (Behavior Rating Instrument of Executive Function-Preschool).
- -
- (Attention deficit hyperactivity disorder or ADHD) and (BRIEF-P).
- (ii)
- NCBI ◊ PubMed Central ◊ 247 results
- -
- (Attention deficit hyperactivity disorder + or + ADHD) and (BRIEF-P).
- (iii)
- ProQuest Education Journals
- -
- ((Attention deficit hyperactivity disorder or ADHD) AND (BRIEF-P)).AND stype.exact(“Scholarly Journals”) Education Database.
- -
- (Attention deficit hyperactivity disorder or ADHD) and (Behavior Rating Instrument of Executive Function-Preschool) Education Database.
3. Results
3.1. Risk of Bias
3.2. Floor Effect and Ceiling Effect
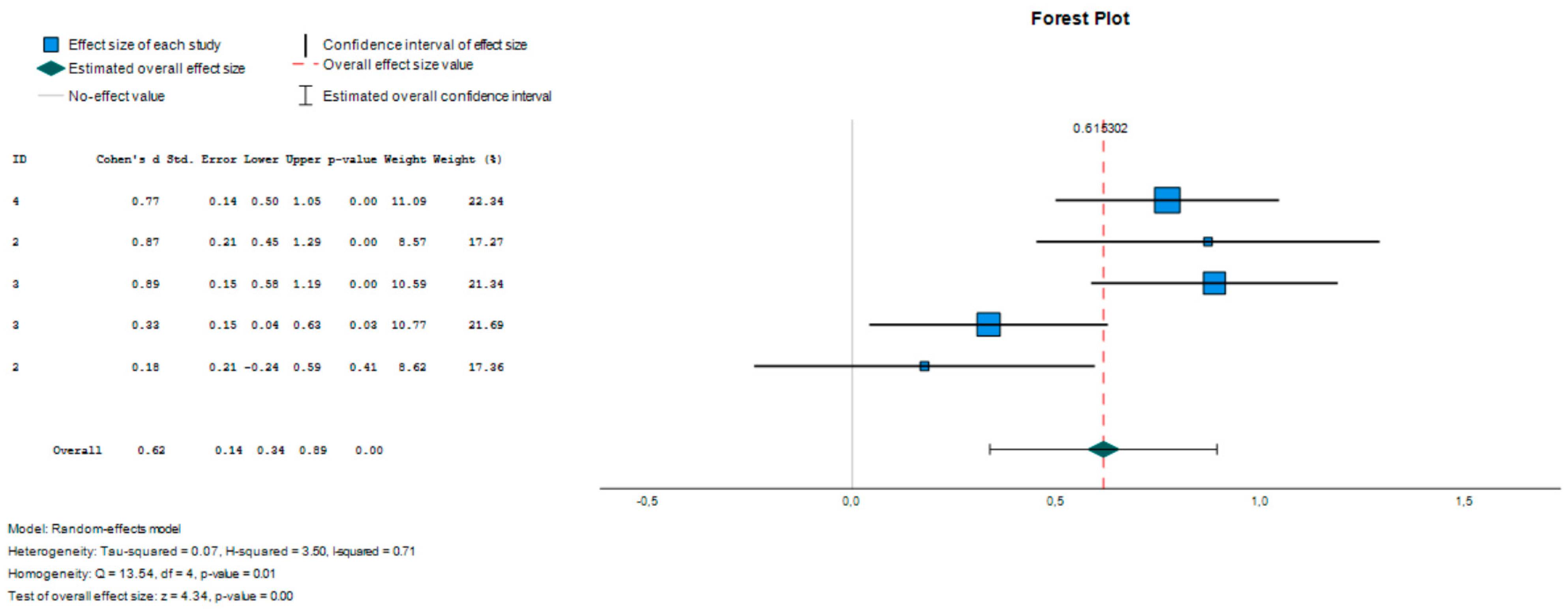
3.2.1. Floor Effect
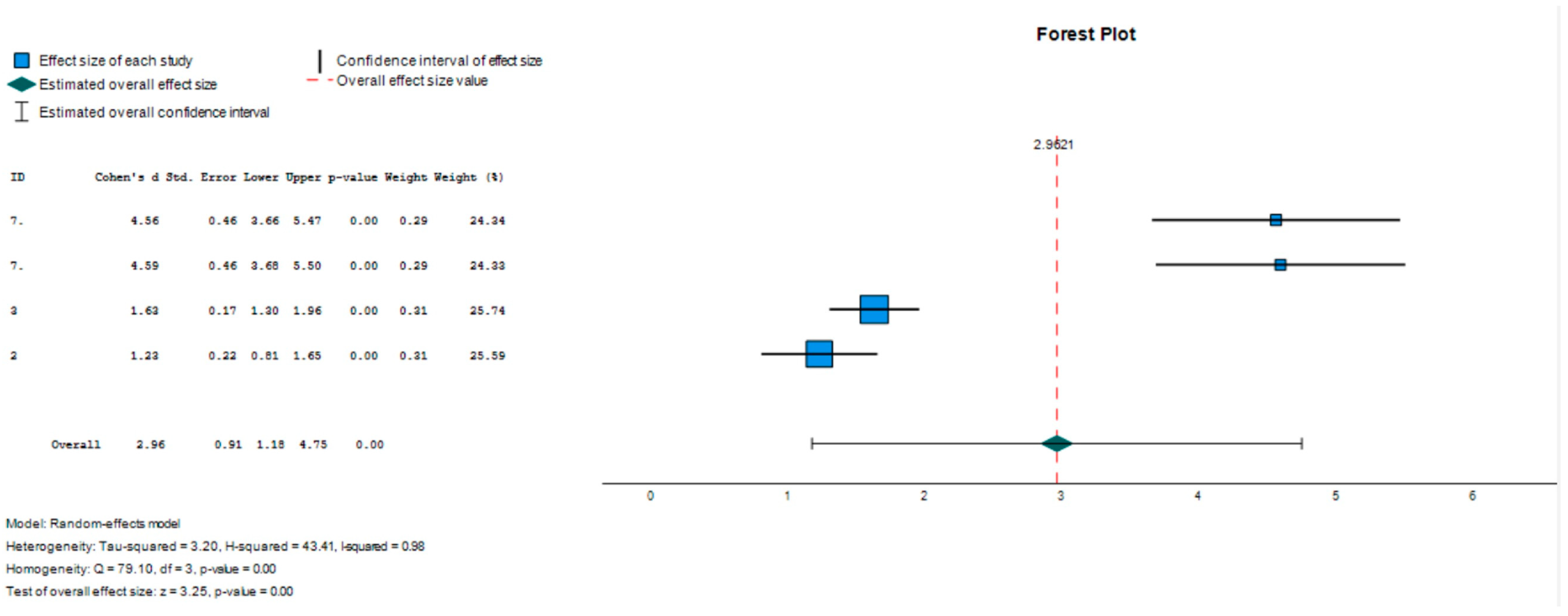
3.2.2. Ceiling Effect
4. Discussion and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sayal, K.; Prasad, V.; Daley, D.; Ford, T.; Coghill, D. ADHD in children and young people: Prevalence, care pathways, and service provision. Lancet Psychiatry 2018, 5, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Lange, K.; Reichl, S.; Lange, K.; Tucha, L.; Tucha, O. The history of attention deficit hyperactivity disorder. ASHD Atten. Deficit Hyperact. Disord. 2010, 2, 241–255. [Google Scholar] [CrossRef]
- American Psychiatric Association (APA). Diagnóstic and Statistical Manual of Mental Disorders; Text Revision (DSM-IV-TR); American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Becker, S.P.; Willcutt, E.G.; Leopold, D.R.; Fredrick, J.W.; Smith, Z.R.; Jacobson, L.A.; Burns, G.L.; Mayes, S.D.; Waschbusch, D.A.; Froehlich, T.E.; et al. Report of a Work Group on Sluggish Cognitive Tempo: Key Research Directions and a Consensus Change in Terminology to Cognitive Disengagement Syndrome. J. Am. Acad. Child Adolesc. Psychiatry 2023, 62, 629–645. [Google Scholar] [CrossRef]
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Publishing: Arlington, MA, USA, 2013. [Google Scholar]
- American Psychiatric Association (APA). Diagnóstic and Statistical Manual of Mental Disorders: DSM-5-TR, 5th ed.; American Psychiatric Association: Arlington, MA, USA, 2022. [Google Scholar]
- Koutsoklenis, A.; Honkasilta, J. ADHD in the DSM-5-TR: What has changed and what has not. Front. Psychiatry 2023, 13, 1064141. [Google Scholar] [CrossRef] [PubMed]
- Faraone, S.; Perlis, R.H.; Doyle, A.E.; Smoller, J.W.; Goralnick, J.; Holmgren, M.A.; Sklar, P. Molecular Genetics of Attention-Deficit/Hyperactivity Disorder. Biol. Psychiatry 2005, 57, 1313–1323. [Google Scholar] [CrossRef] [PubMed]
- Millichap, J. Etiologic Classification of Attention-Deficit/Hyperactivity Disorder. Pediatrics 2008, 121, e358–e365. [Google Scholar] [CrossRef]
- Conners, C.K.; Pitkanen, J.; Rzepa, S.R. Conners 3rd Edition (Conners 3; Conners 2008). In Encyclopedia of Clinical Neuropsychology; Springer: New York, NY, USA, 2011; pp. 675–678. [Google Scholar] [CrossRef]
- DuPaul, G.J.; Power, T.J.; Anastopoulos, A.D.; Reid, R. ADHD Rating Scale—5 for Children and Adolescents: Checklists, Norms, and Clinical Interpretation; Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Antshel, K.; Hier, B.O.; Barkley, R. Executive Functioning Theory and ADHD. In Handbook of Executive Funtioning; Springer: New York, NY, USA, 2014; pp. 107–120. [Google Scholar] [CrossRef]
- Barkley, R.A. Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment; The Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Doyle, A.E. Executive functions in attention-deficit/hyperactivity disorde. J. Clin. Psychiatry 2006, 67 (Suppl. S8), 21–26. [Google Scholar]
- Bauermeister, J.; Shrout, P.; Ramírez, R.; Bravo, M.; Alegría, M.; Martínez-Taboas, A.; Chávez, L.; Rubio-Stipec, M.; García, P.R.J. ADHD correlates, comorbidity, and impairment in community and treated samples of children and adolescents. J. Abnorm. Child Psychol. 2007, 35, 883–898. [Google Scholar] [CrossRef]
- Gnanavel, S.; Sharma, P.; Kaushal, P.; Hussain, S. Attention deficit hyperactivity disorder and comorbidity: A review of literature. World J. Clin. Cases 2019, 7, 2420–2426. [Google Scholar] [CrossRef]
- Marqués-Cabezas, P.; Segura-Rodríguez, A.; García-Barriuso, P.; Gallardo-Borge, L.; Mateos-Sexmero, M.; Blanco, J.; Viuda, M.Q.D.L.D.L.; Perez-Carranza, M.; Aparicio-Parras, A.; Espina-Barrio, J.; et al. Comorbility symptoms in AHDH adult patients. Eur. Psychiatry 2022, 65, S466. [Google Scholar] [CrossRef]
- Brown, T.E. Executive Functions and Attention Deficit Hyperactivity Disorder: Implications of two conflicting views. Int. J. Disabil. Dev. Educ. 2006, 53, 35–46. [Google Scholar] [CrossRef]
- Castellanos, X.F.; Sonuga-Barke, E.J.S.; Milham, M.P.; Tannock, R. Characterizing cognition in ADHD: Beyond executive dysfunction. Trends Cogn. Sci. 2006, 10, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Lambek, R.; Tannock, R.; Dalsgaard, S.; Trillingsgaard, A.; Damm, D.; Thomsen, P. Validating neuropsychological subtypes of ADHD: How do children with and without an executive function deficit differ? J. Child Psychol. Psychiatry 2010, 51, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The Unity and Diversity of Executive Functions and Their Contributions to Complex “Frontal Lobe” Tasks: A Latent Variable Analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Shuai, L.; Zhang, J.; Wang, Y.; Lu, T.; Tan, X.; Pan, J.; Shen, L. Neuropsychological Profile Related with Executive Function of Chinese Preschoolers with Attention-Deficit/Hyperactivity Disorder: Neuropsychological Measures and Behavior Rating Scale of Executive Function-Preschool Version. Chin. Med. J. 2018, 131, 648–656. [Google Scholar] [CrossRef] [PubMed]
- Babb, K.A.; Levine, L.J.; Arseneault, J.M. Shifting gears: Coping flexibility in children with and without ADHD. Int. J. Behav. Dev. 2010, 34, 10–23. [Google Scholar] [CrossRef]
- Petersen, I.; Hoyniak, C.; McQuillan, M.; Bates, J.; Staples, A. Measuring the development of inhibitory control: The challenge of heterotypic continuity. Dev. Rev. 2016, 40, 25–71. [Google Scholar] [CrossRef]
- Bausela-Herreras, E. Development of Executive Function at the Preschool Age. In Handbook of Research on Neurocognitive Development of Excecutive Funtions and Implications for Intervention; IGI Glogal: Hershey, PA, USA, 2022; pp. 1–22. [Google Scholar]
- Zelazo, P.; Müller, U.; Frye, D.; Marcovitch, S.; Argitis, G.; Boseovski, J.; Chiang, J.; Hongwanishkul, D.; Schuster, B.; Sutherland, A. The development of executive function in early childhood. Monogr. Soc. Res. Child Dev. 2003, 68, vii-137. [Google Scholar] [CrossRef]
- Lensing, N.; Elsner, B. Development of hot and cool executive functions in middle childhood: Three-year growth curves of decision making and working memory updating. J. Exp. Child Psychol. 2018, 173, 187–204. [Google Scholar] [CrossRef]
- Zelazo, P.; Carlson, S. Hot and Cool Executive Function in Childhood and Adolescence: Development and Plasticity. Child Dev. Perspect. 2012, 6, 354–360. [Google Scholar] [CrossRef]
- Homer, B.D.; Plass, J.L.; Rose, M.C.; MacNamara, A.P.; Pawar, S.; Ober, T.M. Activating adolescents’ “hot” executive functions in a digital game to train cognitive skills: The effects of age and prior abilities. Cogn. Dev. 2019, 49, 20–32. [Google Scholar] [CrossRef]
- Prencipe, A.; Kesek, A.; Cohen, J.; Lamm, C.; Lewis, M.; Zelazo, P. Development of hot and cool executive function during the transition to adolescence. J. Exp. Child Psychol. 2011, 108, 621–631. [Google Scholar] [CrossRef] [PubMed]
- Rastikerdar, N.; Nejati, V.; Sammaknejad, N.; Fathabadi, J. Developmental trajectory of hot and cold executive functions in children with and without attention deficit-hyperactivity disorder (ADHD). Res. Dev. Disabil. 2023, 137, 104514. [Google Scholar] [CrossRef] [PubMed]
- Shakehnia, F.; Amiri, S.; Ghamarani, A. The comparison of cool and hot executive functions profiles in children with ADHD symptoms and normal children. Asian J. Psychiatry 2021, 55, 102483. [Google Scholar] [CrossRef] [PubMed]
- Berger, I.; Slobodin, O.; Aboud, M.; Melamed, J.; Cassuto, H. Maturational delay in ADHD: Evidence from CPT. Front. Hum. Neurosci. 2013, 7, 691. [Google Scholar] [CrossRef]
- Schoemaker, K.; Bunte, T.; Wiebe, S.; Espy, K.; Deković, M.; Matthys, W. Executive function deficits in preschool children with ADHD and DBD. J. Child Psychol. Psychiatry 2012, 53, 111–119. [Google Scholar] [CrossRef]
- Yáñez-Téllez, G.; Romero-Romero, H.; Rivera-García, L.; Prieto-Corona, B.; Bernal-Hernández, J.; Marosi-Holczberger, E.; Guerrero-Juárez, V.; Rodríguez-Camacho, M.; Silva-Pereyra, J.F. Cognitive and executive functions in ADHD. Actas Españolas Psiquiatr. 2012, 40, 293–298. [Google Scholar]
- Roshani, F.; Piri, R.; Malek, A.; Michel, T.M.; Vafaee, M.S. Comparison of cognitive flexibility, appropriate risk-taking and reaction time in individuals with and without adult ADHD. Psychiatry Res. 2020, 284, 112494. [Google Scholar] [CrossRef]
- Karalunas, S.L.; Huang-Pollock, C.L. Examining relationships between executive functioning and delay aversion in attention deficit hyperactivity disorder. J. Clin. Child Adolesc. Psychol. 2011, 40, 837–847. [Google Scholar] [CrossRef]
- Varrasi, S.; Boccaccio, F.M.; Guerrera, C.S.; Platania, G.A.; Pirrone, C.; Castellano, S. Schooling and Occupational Outcomes in Adults with ADHD: Predictors of Success and Support Strategies for Effective Learning. Educ. Sci. 2023, 13, 37. [Google Scholar] [CrossRef]
- Vergara-Maragues, E.; González-Saiz, F.; Lozano-Rojas, Ó.; Billbao-Acedos, I.; Fernández-Calderón, F.; Betanzos-Espinosa, P.; Verdejo García, A.; Pérez-García, M. Diagnosing adult attention-deficit/hyperactivity disorder in patients with cocaine dependence: Usefulness of new Barkley executive function symptoms. Trastor. Adict. 2010, 12, 72–78. [Google Scholar] [CrossRef]
- Zhang, S.-Y.; Qiu, S.-W.; Pan, M.-R.; Zhao, M.-J.; Zhao, R.-J.; Liu, L.; Li, H.-M.; Wang, Y.-F.; Qian, Q.-J. Adult ADHD, executive function, depressive/anxiety symptoms, and quality of life: A serial two-mediator model. J. Affect. Disord. 2021, 293, 97–108. [Google Scholar] [CrossRef] [PubMed]
- Barkley, R. Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychol. Bull. 1997, 121, 65–94. [Google Scholar] [CrossRef] [PubMed]
- Hobson, C.; Scott, S.; Rubia, K. Investigation of cool and hot executive function in ODD/CD independently of ADHD. J. Child Psychol. Psychiatry 2011, 52, 1035–1043. [Google Scholar] [CrossRef] [PubMed]
- Nejati, V. Reading mind from the eyes in individuals with attention deficit-hyperactivity disorder (ADHD): A meta-analysis. Expert Rev. Neurother. 2022, 22, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Nigg, J. Is ADHD a disinhibitory disorder? Psychol. Bull. 2001, 127, 571–598. [Google Scholar] [CrossRef]
- Barkley, R. Advances in the diagnosis and subtyping of attention deficit hyperactivity disorder: What may lie ahead for DSM-V. Rev. Neurol. 2009, 48 (Suppl. S2), S101–S106. [Google Scholar]
- Servera, M. Modelo de autorregulación de Barkley aplicado al trastorno por déficit de atención con hiperactividad: Una revisión. Rev. Neurol. 2005, 40, 358–368. [Google Scholar] [CrossRef]
- Kofler, M.; Singh, L.; Soto, E.; Chan, E.; Miller, C.; Harmon, S.; Spiegel, J. Working memory and short-term memory deficits in ADHD: A bifactor modeling approach. Neuropsychology 2020, 34, 686–698. [Google Scholar] [CrossRef]
- Kasper, L.; Alderson, R.; Hudec, K. Moderators of working memory deficits in children with attention-deficit/hyperactivity disorder (ADHD): A meta-analytic review. Clin. Psychol. Rev. 2012, 32, 605–617. [Google Scholar] [CrossRef]
- Nejati, V.; Derakhshan, Z.; Mohtasham, A. The effect of comprehensive working memory training on executive functions and behavioral symptoms in children with attention deficit-hyperactivity disorder (ADHD). Asian J. Psychiatry 2023, 81, 103469. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Chan, R.; Gracia, N.; Cao, X.; Zou, X.; Jing, J.; Mai, J.; Li, J.; Shum, D. Cool and hot executive functions in medication-naive attention deficit hyperactivity disorder children. Psychol. Med. 2011, 41, 2593–2602. [Google Scholar] [CrossRef] [PubMed]
- Cañas, J.; Quesada, J.; Antolí, A.; Fajardo, I. Cognitive flexibility and adaptability to environmental changes in dynamic complex problem-solving tasks. Ergonomics 2003, 46, 482–501. [Google Scholar] [CrossRef] [PubMed]
- Schoemaker, M.; Hijlkema, M.; Kalverboer, A. Physiotherapy for clumsy children: An evaluation study. Dev. Med. Child Neurol. 1994, 36, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Wixted, E.; Sue, I.; Dube, S.; Potter, A. Cognitive Flexibility and Academic Performance in College Students with ADHD: An fMRI Study. Bachelor’s Thesis, University of Vermont, Burlington, VT, USA, 2016. Available online: https://scholarworks.uvm.edu/cgi/viewcontent.cgi?article=1144&context=hcoltheses (accessed on 19 October 2023).
- Chan, R.C.; Shum, D.; Toulopoulou, T.; Chen, E.Y. Assessment of executive functions: Review of instruments and identification of critical issues. Arch. Clin. Neuropsychol. 2008, 23, 201–216. [Google Scholar] [CrossRef] [PubMed]
- Donders, J. The Behavior Rating Inventory of Executive Function: Introduction. Child Neuropsychol. 2002, 8, 229–230. [Google Scholar] [CrossRef]
- Gioia, G.; Kenworthy, L.; Isquith, P. Executive Function in the Real World: BRIEF lessons from Mark Ylvisaker. J. Head Trauma Rehabil. 2010, 25, 433–439. [Google Scholar] [CrossRef]
- Henry, L.A.; Bettenay, C. The assessment of executive functioning in children. Child Adolesc. Ment. Health 2010, 15, 110–119. [Google Scholar] [CrossRef]
- Lezak, M.; Howieson, D.; Bigler, E.; Tranel, D. Neuropsychological Assessment; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Miyake, A.; Emerson, M.J.; Friedman, N.P. Assessment of executive functions in clinical settings: Problemas and recomendations. Semin. Speech Lang. 2000, 21, 169–183. [Google Scholar] [CrossRef]
- Toplak, M.; Bucciarelli, S.; Jain, U.; Tannock, R. Executive functions: Performance-based measures and the behavior rating inventory of executive function (BRIEF) in adolescents with attention deficit/hyperactivity disorder (ADHD). Child Neuropsychol. 2009, 15, 53–72. [Google Scholar] [CrossRef]
- Verdejo-García, A.; Bechara, A. Neuropsychology of the executive Funtions. Psicothema 2010, 22, 227–235. [Google Scholar] [PubMed]
- Wild, K.; Musser, E.D. The Cambridge Neuropsychological Test Automated Battery in the Assessment of Executive Functioning. In Handbook of Executive Funtioning; Springer: New York, NY, USA, 2014; pp. 171–190. [Google Scholar] [CrossRef]
- Kramer, J.; Mungas, D.; Possin, K.; Rankin, K.; Boxer, A.; Rosen, H.; Bostrom, A.; Sinha, L.; Berhel, A.; Widmeyer, M. NIH EXAMINER: Conceptualization and development of an executive function battery. J. Int. Neuropsychol. Soc. 2014, 20, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Naglieri, J.; Das, J. Cognitive Assessment System; Riverside Publishing Company: Itasca, IL, USA, 1997. [Google Scholar]
- Naglieri, J.; Das, J.; Goldstein, S. Cognitive Assessment System2; ProEd: Austin, TX, USA, 2013. [Google Scholar]
- Delis, D.; Kaplan, E.; Kramer, J. Delis Kaplan (D-KEFS) Technical Manual; NCS Pearson Inc.: San Antonio, TX, USA, 2001. [Google Scholar]
- Naglieri, J.A.; Goldstein, S. Comprenhensive Executive Functioning Index; Multi Health Systems: Toronto, ON, Canada, 2013. [Google Scholar]
- Gioia, G.; Isquith, P.; Guy, S.; Kenworthy, L. BRIEF: Behavior Rating Inventory of Executive Function Professional Manual; Psychological Assessment Resources: Lutz, FL, USA, 2000. [Google Scholar]
- Guy, S.C.; Isquith, P.K.; Gioia, G.A. Behavior Rating Inventory of Executive Function—Self Report Version; Psychological Assessment Resources: Lutz, FL, USA, 2004. [Google Scholar]
- Roth, R.M.; Isquith, P.K.; Gioia, G.A. Behavior Rating Inventory of Executive Function. Adult Version (BRIEF-A); Psychological Assessment Resources: Lutz, FL, USA, 2005. [Google Scholar]
- Çak, H.T.; Çengel, S.E.; Gökler, B.; Öktem, F.; Taşkıran, C. The Behavior Rating Inventory of Executive Function and Continuous Performance Test in Preschoolers with Attention Deficit Hyperactivity Disorder. Psychiatry Investig. 2017, 14, 260–270. [Google Scholar] [CrossRef] [PubMed]
- Gioia, G.A.; Espy, K.A.; Isquith, P.K. Behavior Rating Inventory of Executive Function Preschool Version (BRIEF-P); Psychological Assessment Resources: Lutz, FL, USA, 2003. [Google Scholar]
- García-Fernández, T.; González-Pienda, J.A.; Rodríguez-Pérez, C.; Álvarez-García, D. Psychometric characteristics of the BRIEF scale for the assessment of executive functions in Spanish clinical population. Psicothema 2014, 26, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Skogan, A.H.; Egeland, J.; Zeiner, P.; Øvergaard, K.R.; Oerbeck, B.; Reichborn-Kjennerud, T.; Aase, H. Factor structure of the Behavior Rating Inventory of Executive Functions (BRIEF-P) at age three years. Child Neuropsychol. 2016, 22, 472–492. [Google Scholar] [CrossRef]
- Mahone, E.M.; Hoffman, J. Behavior Ratings of Executive Function among Preschoolers with ADHD. Clin. Neuropsychol. 2007, 21, 569–586. [Google Scholar] [CrossRef]
- Page, M.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Rev. Española Cardiol. 2021, 74, 790–799. [Google Scholar] [CrossRef]
- Dettori, J.; Norvell, D.; Chapman, J. Fixed-Effect vs. Random-Effects Models for Meta-Analysis: 3 Points to Consider. Glob. Spine J. 2022, 12, 1624–1626. [Google Scholar] [CrossRef]
- Lacerda, B.; Martínez, S.; Franz, A.; Moreira-Maia, C.; Silveira, R.; Procianoy, R.; Wagner, F. Does ADHD worsen inhibitory control in preschool children born very premature and/or with very low birth weight? Trends Psychiatry Psychother. 2020, 42, 340–347. [Google Scholar] [CrossRef]
- Ezpeleta, L.; Granero, R. Executive functions in preschoolers with ADHD, ODD, and comorbid ADHD-ODD: Evidence from ecological and performance-based measures. J. Neuropsychol. 2015, 9, 258–270. [Google Scholar] [CrossRef]
- Skogan, A.H.; Zeiner, P.; Egeland, J.; Urnes, A.-G.; Reichborn-Kjennerud, T.; Aase, H. Parent ratings of executive function in young preschool children with symptoms of attention-deficit/-hyperactivity disorder. Behav. Brain Funct. 2015, 11, 16. [Google Scholar] [CrossRef] [PubMed]
- Schneider, H.; Ryan, M.; Mahone, E. Parent versus teacher ratings on the BRIEF-preschool version in children with and without ADHD. Child Neuropsychol. 2020, 26, 113–128. [Google Scholar] [CrossRef] [PubMed]
- Perrin, H.; Heller, N.; Loe, I. School Readiness in Preschoolers With Symptoms of Attention-Deficit/Hyperactivity Disorder. Am. Acad. Pediatr. 2019, 144, e20190038. [Google Scholar] [CrossRef] [PubMed]
- Wiebe, S.; Sheffield, T.; Nelson, J.; Clark, C.; Chevalier, N.; Espy, K. The structure of executive function in 3-year-olds. J. Exp. Child Psychol. 2011, 108, 436–452. [Google Scholar] [CrossRef] [PubMed]
- Takacs, Z.; Kassai, R. The efficacy of different interventions to foster children’s executive function skills: A series of meta-analyses. Psychol. Bull. 2019, 145, 653–697. [Google Scholar] [CrossRef] [PubMed]
- Shaw, P.; Stringaris, A.; Nigg, J.; Leibenluft, E. Emotion dysregulation in attention deficit hyperactivity disorder. Am. J. Psychiatry 2014, 171, 276–293. [Google Scholar] [CrossRef] [PubMed]
- Slaats-Willemse, D.; Swaab-Barneveld, H.; de Sonneville, L.; van der Meulen, E.; Buitelaar, J. Deficient response inhibition as a cognitive endophenotype of ADHD. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 1242–1248. [Google Scholar] [CrossRef] [PubMed]
- Barkley, R.A. Response inhibition in attention-deficit hyperactivity disorder. Ment. Retard. Dev. Disabil. Res. Rev. 1999, 5, 177–187. [Google Scholar] [CrossRef]
- Mukherjee, P.; Hartanto, T.; Iosif, A.M.; Dixon, J.F.; Hinshaw, S.P.; Pakyurek, M.; van den Bos, W.; Guyer, A.E.; McClure, S.M.; Schweitzer, J.B.; et al. Neural basis of working memory in ADHD: Load versus complexity. NeuroImage Clin. 2021, 30, 102662. [Google Scholar] [CrossRef]
- Van De Voorde, S.; Roeyers, H.; Verté, S.W.J. Working memory, response inhibition, and within-subject variability in children with attention-deficit/hyperactivity disorder or reading disorder. J. Clin. Exp. Neuropsychol. 2010, 32, 366–379. [Google Scholar] [CrossRef]
- Salehinejad, M.; Ghanavati, E.; Rashid, M.; Nitsche, M.A. Hot and cold executive functions in the brain: A prefrontal-cingular network. Brain Neurosci. Adv. 2021, 23, 5. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| (a) Participants: persons with symptoms compatible with ADHD obtained from the application of standardized tests; | (a) Participants: not diagnosed with ADHD; |
| (b) Cognitive age that allows the application of BRIEF-P; | (b) Cognitive age: does not allow application of BRIEF-P; |
| (c) Cognitive competence (obtained through the application of standardized tests); | (c) Cognitive competence: not available; |
| (d) Executive dimensions: single construct or basic dimensions (flexibility, inhibition and working memory); | (d) Assessment instruments: non-standardized; |
| (e) Assessment instruments: standardized for assessing executive functions: hetero- and/or self-report; | (e) Type of studies: case study and review; |
| (f) Type of studies: empirical; | (f) Type of design: non-comparative-causal; |
| (g) Type of design: non-experimental, comparative-causal (group with ADHD-compatible symptoms versus group with typical development); | (g) Type of design: non-comparative-causal; |
| (h) Language: English and Spanish; | (h) Language: other; |
| (i) Other characteristics: full text. | (i) Other characteristics: abstract, full text not available. |
| Study | Author/Year/Country | ADHD | CONTROL | ODD | ODD + ADHD |
|---|---|---|---|---|---|
| 1 | (Lacerda et al. 2020) Brazil [78]; | 24 | 55 | ||
| 2 | (Ezpeleta and Granero, 2015) Sapin [79]; | 23 | 538 | 51 | 10 |
| 3 | (Zhang et al. 2018) China [22]; | 163 | 63 | ||
| 4 | (Skogan et al. 2015) Norway [80]; | 1134 | |||
| 5 | (Schneider, Ryan & Mahone, 2020) USA [81]; | 49 | 35 | ||
| 6 | (Perrin, Heller & Loe, 2019) USA [82]; | 45 | 48 | ||
| 7 | (Çak, Çengel, Gökler, Öktem & Taşkıran, 2017) Turkey [71]. | 21 | 52 | ||
| SUBTOTAL | 1459 | 791 | 51 | 10 | |
| TOTAL | 2311 | ||||
| Effect Size | Standard Error | Z | Sig. (Bilateral) | Confidence Interval 95% | Prediction Interval 95% a | |||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | Lower | Upper | |||||
| Global | 0.615 | 0.1419 | 4.335 | <0.001 | 0.337 | 0.893 | −0.343 | 1.574 |
| Effect Size | Standard Error | Z | Sig. (Bilateral) | Confidence Interval 95% | Prediction Interval 95% a | |||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | Lower | Upper | |||||
| Global | 2.962 | 0.9117 | 3.249 | 0.001 | 1.175 | 4.749 | −5.679 | 11.603 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bausela-Herreras, E.; Alonso-Esteban, Y.; Alcantud-Marín, F. Behavior Rating Inventory of Executive Function in Preschool (BRIEF-P) and Attention-Deficit and Hyperactivity Disorders (ADHD): A Systematic Review and Meta-Analysis of Floor and Ceiling Effects. Children 2024, 11, 58. https://doi.org/10.3390/children11010058
Bausela-Herreras E, Alonso-Esteban Y, Alcantud-Marín F. Behavior Rating Inventory of Executive Function in Preschool (BRIEF-P) and Attention-Deficit and Hyperactivity Disorders (ADHD): A Systematic Review and Meta-Analysis of Floor and Ceiling Effects. Children. 2024; 11(1):58. https://doi.org/10.3390/children11010058
Chicago/Turabian StyleBausela-Herreras, Esperanza, Yurena Alonso-Esteban, and Francisco Alcantud-Marín. 2024. "Behavior Rating Inventory of Executive Function in Preschool (BRIEF-P) and Attention-Deficit and Hyperactivity Disorders (ADHD): A Systematic Review and Meta-Analysis of Floor and Ceiling Effects" Children 11, no. 1: 58. https://doi.org/10.3390/children11010058