
A Pilot Feasibility Study Assessing the Combined Effects of Early Behavioral Intervention and Propranolol on Autism Spectrum Disorder (ASD)

Abstract
:1. Background
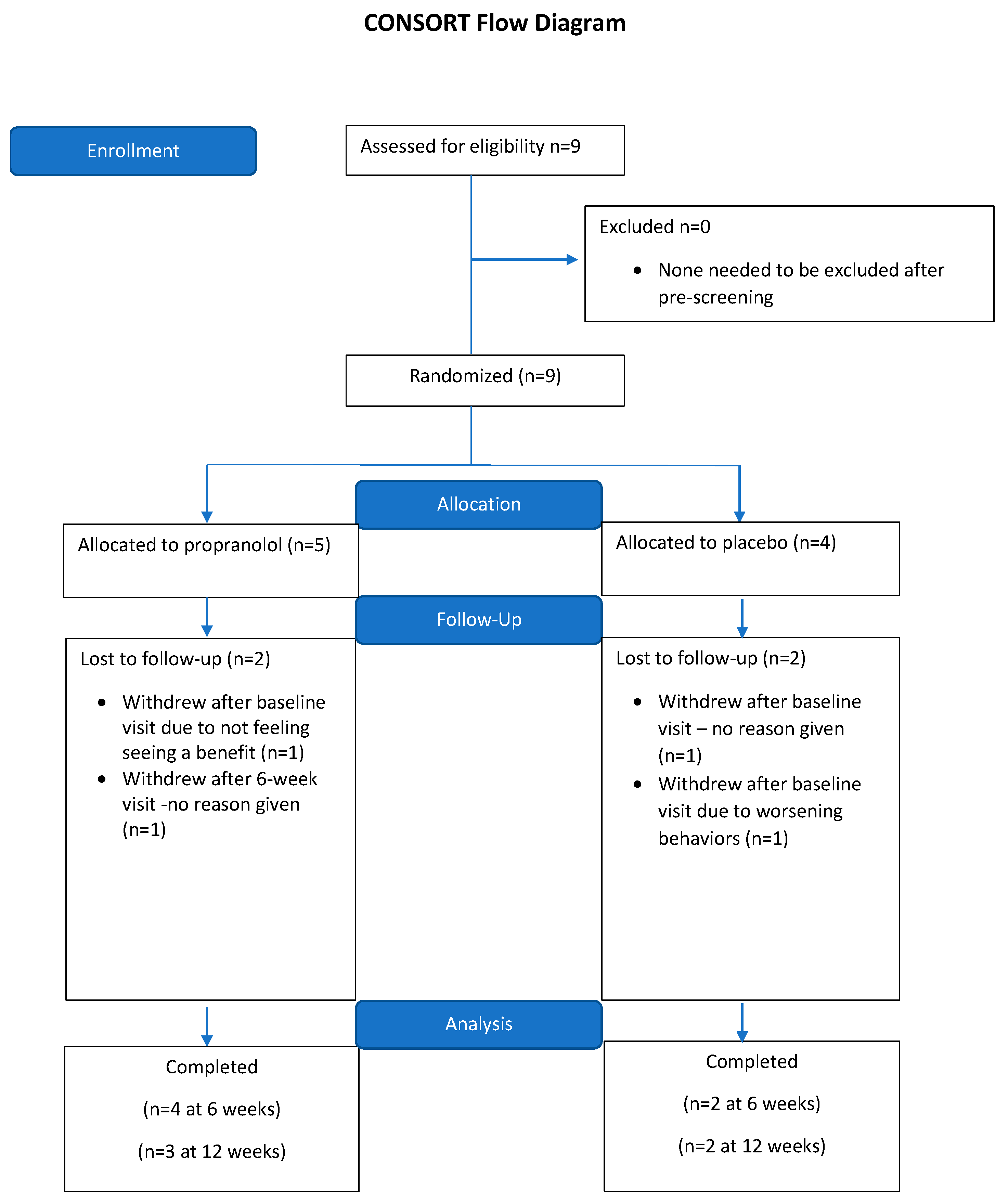
2. Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychological Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; (DSM-V); American Psychological Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Gaugler, T.; Klei, L.; Sanders, S.J.; Bodea, C.A.; Goldberg, A.P.; Lee, A.B.; Mahajan, M.; Manaa, D.; Pawitan, Y.; Reichert, J.; et al. Most genetic risk for autism resides with common variation. Nat. Genet. 2014, 46, 881–885. [Google Scholar] [CrossRef]
- Sandin, S.; Lichtenstein, P.; Kuja-Halkola, R.; Hultman, C.; Larsson, H.; Reichenberg, A. Heritability of autism spectrum disorder. J. Am. Med. Assoc. 2017, 318, 1182–1184. [Google Scholar] [CrossRef]
- Bai, D.; Yip, B.H.K.; Windham, G.C.; Sourander, A.; Francis, R.; Yoffe, R.; Glasson, E.; Mahjani, B.; Suominen, A.; Leonard, H.; et al. Association of genetic and environmental factors with autism in a 5-country cohort. JAMA Psychiatry 2019, 76, 1035–1043. [Google Scholar] [CrossRef]
- Hu, V.W.; Frank, B.C.; Heine, S.; Lee, N.H.; Quackenbush, J. Gene expression profiling of lymphoblastoid cell lines from monozygotic twins discordant in severity of autism reveals differential regulation of neurologically relevant genes. BMC Genom. 2006, 7, 118. [Google Scholar] [CrossRef]
- Nguyen, A.T.; Rauch, R.A.; Pfeifer, G.P.; Hu, V.W. Global methylation profiling of lymphoblastoid cell lines reveals epigenetic contributions to autism spectrum disorders and a novel autism candidate gene, RORA, whose protein product is reduced in autistic brain. FASEB J. 2010, 24, 3036–3051. [Google Scholar] [CrossRef]
- Geschwind, D.H. Advances in autism. Annu. Rev. Med. 2009, 60, 367–380. [Google Scholar] [CrossRef]
- Veenstra-VanderWeele, J.; Blakely, R.D. Networking in autism: Leveraging genetic, biomarker and model system findings in the search for new treatments. Neuropsychopharmacology 2012, 37, 196–212. [Google Scholar] [CrossRef]
- Myers, S.M.; Johnson, C.P. Management of children with autism spectrum disorders. Pediatrics 2007, 120, 1162–1182. [Google Scholar] [CrossRef]
- Landa, R.J. Diagnosis of autism spectrum disorders in the first 3 years of life. Nat. Clin. Pract. Neuro 2008, 4, 138–147. [Google Scholar] [CrossRef]
- Rogers, S.J.; Vismara, L.A. Evidence-based comprehensive treatments for early autism. J. Clin. Child Adolesc. Psychol. 2008, 37, 8–38. [Google Scholar] [CrossRef]
- Dawson, G. Early behavioral intervention, brain plasticity, and the prevention of autism spectrum disorder. Dev. Psychopathol. 2008, 20, 775–803. [Google Scholar] [CrossRef]
- Towbin, K.E. Strategies for pharmacologic treatment of high functioning autism and asperger syndrome. Child Adolesc. Psychiatr. Clin. N. Am. 2003, 12, 23–45. [Google Scholar] [CrossRef]
- Matson, J.; Dempsey, T. Autism spectrum disorders: Pharmacotherapy for challenging behaviors. J. Dev. Phys. Disabil. 2008, 20, 175–191. [Google Scholar] [CrossRef]
- Beversdorf, D. Therapeutic interventions in autism: A review for primary care physicians. Mo Med. 2008, 105, 390–395. [Google Scholar]
- Volkmar, F.R. Pharmacological interventions in autism: Theoretical and practical issues. J. Clin. Child Adolesc. Psychol. 2001, 30, 80–87. [Google Scholar] [CrossRef]
- Bartz, J.A.; Hollander, E. Oxytocin and experimental therapeutics in autism spectrum disorders. Prog. Brain Res. 2008, 170, 451–462. [Google Scholar]
- Hollander, E.; Bartz, J.; Chaplin, W.; Phillips, A.; Sumner, J.; Soorya, L.; Anagnostou, E.; Wasserman, S. Oxytocin increases retention of social cognition in autism. Biol. Psychiatry 2007, 61, 498–503. [Google Scholar] [CrossRef]
- Chez, M.G.; Burton, Q.; Dowling, T.; Chang, M.; Khanna, P.; Kramer, C. Memantine as adjunctive therapy in children diagnosed with autistic spectrum disorders: An observation of initial clinical response and maintenance tolerability. J. Child Neurol. 2007, 22, 574–579. [Google Scholar] [CrossRef]
- Erickson, C.; Posey, D.; Stigler, K.; Mullett, J.; Katschke, A.; McDougle, C. A retrospective study of memantine in children and adolescents with pervasive developmental disorders. Psychopharmacology 2007, 191, 141–147. [Google Scholar] [CrossRef]
- Erickson, C.; Veenstra-Vanderweele, J.; Melmed, R.; McCracken, J.; Ginsberg, L.; Sikich, L.; Scahill, L.; Cherubini, M.; Zarevics, P.; Walton-Bowen, K.; et al. Stx209 (arbaclofen) for autism spectrum disorders: An 8-week open-label study. J. Autism Dev. Disord. 2014, 44, 958–964. [Google Scholar] [CrossRef]
- Veenstra-VanderWeele, J.; Sikich, L.; Melmed, R.; von Hehn, J.S.; Walton-Brown, K.L.; Kuriyama, N.; Cherubini, M.; Zarevics, P.; Carpenter, R.L.; Bear, M.F.; et al. Randomized, Controlled, Phase 2 Trial of STX209 for social function in ASD. Int. Meet. Autism Res. 2013, 13, 102.001. [Google Scholar]
- Singh, K.; Connors, S.L.; Macklin, E.A.; Smith, K.D.; Fahey, J.W.; Talalay, P.; Zimmerman, A.W. Sulforaphane treatment of autism spectrum disorder (ASD). Proc. Natl. Acad. Sci. USA 2014, 111, 15550–15555. [Google Scholar] [CrossRef]
- Billeci, L.; Tonacci, A.; Narzisi, A.; Manigrasso, Z.; Varanini, M.; Fulceri, F.; Lattarulo, C.; Calderoni, S.; Muratori, F. Heart rate variability during a joint attention task in toddlers with autism spectrum disorders. Front. Physiol. 2019, 9, 467. [Google Scholar] [CrossRef] [PubMed]
- Corbett, B.A.; Muscatello, R.A.; Baldinger, C. Comparing stress arousal systems in response to different social context in children with, A.S.D. Biol. Psychol. 2019, 140, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Sheinkopf, S.J.; Levin, T.P.; McCormick, C.E.B.; Puggioni, G.; Conradt, E.; Lagasse, L.L.; Lester, B.M. Developmental trajectories of autonomic functioning in autism from birth to early childhood. Biol. Psychol. 2019, 142, 13–19. [Google Scholar] [CrossRef]
- Ratey, J.J.; Bemporad, J.; Sorgi, P.; Bick, P.; Polakoff, S.; O’Driscoll, G.; Mikkelsen, E. Brief report: Open trial effects of beta-blockers on speech and social behaviors in 8 autistic adults. J. Autism Devel. Disord. 1987, 17, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Faigel, H.C. The effect of beta blockade on stress-induced cognitive dysfunction in adolescents. Clin. Pediatr. 1991, 30, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Lader, M. Beta-adrenoceptor antagonists in neuropsychiatry: An update. J. Clin. Psychiatry 1988, 49, 213–223. [Google Scholar] [PubMed]
- Laverdure, B.; Boulenger, J.P. Beta-blocking drugs and anxiety. A proven therapeutic value. L’Encephale 1991, 17, 481–492. [Google Scholar]
- Keeshin, B.R.; Strawn, J.R. Treatment of children and adolescents with posttraumatic stress disorder (PTSD): A review of current evidence. Child Adolesc. Psychopharmacol. News 2012, 17, 5–10. [Google Scholar] [CrossRef]
- Searcy, C.P.; Bobadilla, L.; Gordon, W.A.; Jacques, S.; Elliott, L. Pharmacological prevention of combat-related PTSD: A literature review. Mil. Med. 2012, 177, 649–654. [Google Scholar] [CrossRef]
- Kampman, K.M.; Volpicelli, J.R.; Mulvaney, F.; Alterman, A.I.; Cornish, J.; Gariti, P.; Cnaan, A.; Poole, S.; Muller, E.; Acosta, T.; et al. Effectiveness of propranolol for cocaine dependence treatment may depend on cocaine withdrawal symptom severity. Drug Alcohol Depend. 2001, 63, 69–78. [Google Scholar] [CrossRef]
- Kelley, B.J.; Yeager, K.R.; Pepper, T.H.; Bornstein, R.A.; Beversdorf, D.Q. The effect of propranolol on cognitive flexibility and memory in acute cocaine withdrawal. Neurocase 2008, 13, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Beversdorf, D.Q.; Hughes, J.D.; Steinberg, B.A.; Lewis, L.D.; Heilman, K.M. Noradrenergic modulation of cognitive flexibility in problem solving. NeuroReport 1999, 10, 2763–2767. [Google Scholar] [CrossRef]
- Beversdorf, D.Q.; White, D.M.; Chever, D.C.; Hughes, J.D.; Bornstein, R.A. Central beta-adrenergic modulation of cognitive flexibility. NeuroReport 2002, 13, 2505–2507. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.K.; Hillier, A.; Smith, R.M.; Tivarus, M.E.; Beversdorf, D.Q. Beta-adrenergic modulation of cognitive flexibility during stress. J. Cogn. Neurosci. 2007, 19, 468–478. [Google Scholar] [CrossRef]
- Campbell, H.L.; Tivarus, M.E.; Hillier, A.; Beversdorf, D.Q. Increased task difficulty results in greater impact of noradrenergic modulation of cognitive flexibility. Pharmacol. Biochem. Behav. 2008, 88, 222–229. [Google Scholar] [CrossRef] [PubMed]
- Beversdorf, D.Q.; Carpenter, A.L.; Miller, R.F.; Cios, J.S.; Hillier, A. Effect of propranolol on verbal problem solving in autism spectrum disorder. Neurocase 2008, 14, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Beversdorf, D.Q.; Saklayen, S.; Higgins, K.F.; Bodner, K.E.; Kanne, S.M.; Christ, S.E. Effect of propranolol on word fluency in autism. Cogn. Behav. Neurol. 2011, 24, 11–17. [Google Scholar] [CrossRef]
- Bodner, K.E.; Beversdorf, D.Q.; Saklayen, S.S.; Christ, S.E. Noradrenergic moderation of working memory impairments in adults with autism spectrum disorder. J. Int. Neuropsychol. Soc. 2012, 18, 556–564. [Google Scholar] [CrossRef]
- Zamzow, R.M.; Christ, S.E.; Saklayen, S.S.; Moffitt, A.J.; Bodner, K.E.; Higgins, K.F.; Beversdorf, D.Q. Effect of propranolol on facial scanning in autism spectrum disorder: A preliminary investigation. J. Clin. Exp. Neuropsychol. 2014, 36, 431–445. [Google Scholar] [CrossRef] [PubMed]
- Zamzow, R.M.; Ferguson, B.J.; Stichter, J.P.; Porges, E.C.; Ragsdale, A.S.; Lewis, M.L.; Beversdorf, D.Q. Effects of propranolol on conversational reciprocity in autism spectrum disroder: A pilot, double-blind, single-dose psychopharmacological challenge study. Psychopharmacology 2016, 233, 1171–1178. [Google Scholar] [CrossRef]
- Sagar-Ouriaghli, I.; Lievesley, K.; Santosh, P.J. Propranolol for treating emotional, behavioral, autonomic dysregulation in children and adolescents with autism spectrum disorder. J. Psychopharmacol. 2018, 32, 641–653. [Google Scholar] [CrossRef] [PubMed]
- London, E.B.; Yoo, J.H.; Fethke, E.D.; Zimmerman-Bier, B. The Safety and Effectiveness of High-Dose Propranolol as a Treatment for Challenging Behaviors in Individuals with Autism Spectrum Disorders. J. Clin. Psychopharmacol. 2020, 40, 122–129. [Google Scholar] [CrossRef]
- Beversdorf, D.Q.; Ferguson, B.; Hunter, S.; Hirst, K.; Lolli, B.; Bellesheim, K.R.; Barton, A.U.; Muckerman, J.; Takahashi, N.; Selders, K. Randomized controlled trial of propranolol on social communication and anxiety in children and young adults with autism spectrum disorder. Psychopharmacology, 2013; in press. [Google Scholar]
- Lovaas, O.I.; Ackerman, A.; Alexander, D.; Firestone, P.; Perkins, J.; Young, D. Teaching Developmentally Disabled Children: The Me Book; University Park Press: Austin, TX, USA, 1981. [Google Scholar]
- Eldevik, S.; Hastings, R.P.; Hughes, J.C.; Jahr, E.; Eikeseth, S.; Cross, S. Meta-analysis of early intensive behavioral intervention for children with autism. J. Clin. Child Adolesc. Psychol. 2009, 38, 439–450. [Google Scholar] [CrossRef]
- Lovaas, O.I. Behavioral treatment and normal educational and intellectual functioning in young autistic children. J. Consult. Clin. Psychol. 1987, 55, 3–9. [Google Scholar] [CrossRef]
- McEachin, J.J.; Smith, T.; Lovaas, O.I. Long-term outcome for children with autism who received early intensive behavioral treatment. Am. J. Ment. Retard. 1993, 97, 359–372. [Google Scholar]
- Cohen, H.; Amerine-Dickens, M.; Smith, T. Early intensive behavioral treatment: Replication of the UCLA model in a community setting. J. Dev. Behav. Pediatr. 2006, 27, S145–S155. [Google Scholar] [CrossRef]
- Eikeseth, S.; Smith, T.; Jahr, E.; Eldevik, S. Intensive behavioral treatment at school for 4- to 7-year-old children with autism: A 1-year comparison controlled study. Behav. Modif. 2002, 26, 49–68. [Google Scholar] [CrossRef]
- Eikeseth, S.; Smith, T.; Jahr, E.; Eldevik, S. Outcome for children with autism who began intensive behavioral treatment between ages 4 and 7: A comparison controlled study. Behav. Modif. 2007, 31, 264–278. [Google Scholar] [CrossRef] [PubMed]
- Eldevik, S.; Eikeseth, S.; Jahr, E.; Smith, T. Effects of low-intensity behavioral treatment for children with autism and mental retardation. J. Autism Dev. Disord. 2006, 36, 211–224. [Google Scholar] [CrossRef] [PubMed]
- Howard, J.S.; Sparkman, C.R.; Cohen, H.G.; Green, G.; Stanislaw, H. A comparison of intensive behavior analytic and eclectic treatments for young children with autism. Res. Dev. Disabil. 2005, 26, 359–383. [Google Scholar] [CrossRef]
- Remington, B.; Hastings, R.P.; Kovshoff, H.; degli Espinosa, F.; Jahr, E.; Brown, T.; Alsford, P.; Lemaic, M.; Ward, N.; MacLean, J.W.E. Early intensive behavioral intervention: Outcomes for children with autism and their parents after two years. Am. J. Ment. Retard. 2007, 112, 418–438. [Google Scholar] [CrossRef] [PubMed]
- Sallows, G.O.; Graupner, T.D.; MacLean, W.E., Jr. Intensive behavioral treatment for children with autism: Four-year outcome and predictors. Am. J. Ment. Retard. 2005, 110, 417–438. [Google Scholar] [CrossRef] [PubMed]
- Sheinkopf, S.; Siegel, B. Home-based behavioral treatment of young children with autism. J. Autism Dev. Disord. 1998, 28, 15–23. [Google Scholar] [CrossRef]
- Smith, T.; Eikeseth, S.; Klevstrand, M.; Lovaas, O.I. Intensive behavioral treatment for preschoolers with severe mental retardation and pervasive developmental disorder. Am. J. Ment. Retard. 1997, 102, 238–249. [Google Scholar] [CrossRef]
- Smith, T.; Groen, A.D.; Wynn, J.W. Randomized trial of intensive early intervention for children with pervasive developmental disorder. Am. J. Ment. Retard. 2000, 105, 269–285. [Google Scholar] [CrossRef]
- Howlin, P.; Magiati, I.; Charman, T.; MacLean, J.W.E. Systematic review of early intensive behavioral interventions for children with autism. Am. J. Intellect. Dev. Disabil. 2009, 114, 23–41. [Google Scholar] [CrossRef]
- Ashrafi, M.R.; Shabanian, R.; Zamani, G.R.; Mahfelati, F. Sodium valproate versus propranolol in paediatric migraine prophylaxis. Eur. J. Paediatr. Neurol. 2005, 9, 333–338. [Google Scholar] [CrossRef]
- Bidabadi, E.; Mashouf, M. A randomized trial of propranolol versus sodium valproate for the prophylaxis of migraine in pediatric patients. Pediatr. Drugs 2010, 12, 269–275. [Google Scholar] [CrossRef]
- Eiland, L.S.; Jenkins, L.S.; Durham, S.H. Pediatric migraine: Pharmacologic agents for prophylaxis. Ann. Pharmacother. 2007, 41, 1181–1190. [Google Scholar] [CrossRef]
- Sans, V.; de la Roque, E.D.; Berge, J.; Grenier, N.; Boralevi, F.; Mazereeuw-Hautier, J.; Lipsker, D.; Dupuis, E.; Ezzedine, K.; Vergnes, P.; et al. Propranolol for severe infantile hemangiomas: Follow-up report. Pediatrics 2009, 124, e423–e431. [Google Scholar] [CrossRef]
- Lord, C.M.; Rutter, P.C.; DiLavore, S.; Risi, K.; Gotham, S. Bishop. In Autism Diagnostic Observation Schedule: ADOS-2; Western Psychological Services: Los Angeles, CA, USA, 2012. [Google Scholar]
- Sparrow, S.; Cicchetti, D.; Balla, D. The Vineland—II Adaptive Behavior Scales; American Guidance Service: Circle Pines, MN, USA, 2014. [Google Scholar]
- Aman, M.G.; Singh, N.N.; Stewart, A.W.; Field, C.J. The aberrant behavior checklist: A behavior rating scale for the assessment of treatment effects. Am. J. Ment. Defic. 1985, 89, 485–491. [Google Scholar]
- Stichter, J.P.; Herzog, M.J.; O’Connor, K.V.; Schmidt, C. A preliminary examination of a general social outcome measure. Assess. Eff. Interv. 2012, 38, 40–52. [Google Scholar] [CrossRef]
- Constantino, J.; Davis, S.; Todd, R.; Schindler, M.; Gross, M.; Brophy, S.; Metzger, L.; Shoushtari, C.; Splinter, R.; Reich, W. Validation of a brief quantitative measure of autistic traits: Comparison of the social responsiveness scale with the autism diagnostic interview-revised. J. Autism Dev. Disord. 2003, 33, 427–433. [Google Scholar] [CrossRef]
- Frazier, T.W.; Ratliff, K.R.; Gruber, C.; Zhang, Y.; Law, P.A.; Constantino, J.N. Confirmatory factor analytic structure and measurement invariance of quantitative autistic traits measured by the social responsiveness scale-2. Autism 2013, 18, 31–44. [Google Scholar] [CrossRef]
- Zimmerman, I.L.; Steiner, V.G.; Pond, R.E. Preschool Language Scales; Pearson: San Antonio, TX, USA, 2011. [Google Scholar]
- Spence, S.H.; Rapee, R.; McDonald, C.; Ingram, M. The structure of anxiety symptoms among preschoolers. Behav. Res. Ther. 2001, 39, 1293–1316. [Google Scholar] [CrossRef]
- Kanne, S.; Mazurek, M.; Sikora, D.; Bellando, J.; Branum-Martin, L.; Handen, B.; Katz, T.; Freedman, B.; Powell, M.; Warren, Z. The autism impact measure (AIM): Initial development of a new tool for treatment outcome measurement. J. Autism Dev. Disord. 2014, 44, 168–179. [Google Scholar] [CrossRef]
- Baranek, G.T.; David, F.J.; Poe, M.D.; Stone, W.L.; Watson, L.R. Sensory experiences questionnaire: Discriminating sensory features in young children with autism, developmental delays, and typical development. J. Child Psychol. Psychiatry 2006, 47, 591–601. [Google Scholar] [CrossRef]
- Du, L.; Shan, L.; Wang, B.; Li, H.; Xu, Z.; Staal, W.G.; Jia, F. A pilot study on the combination of applied behavior analysis and bumetanide treatment for children with autism. J. Child Adolesc. Psychopharmacol. 2015, 25, 585–588. [Google Scholar] [CrossRef] [PubMed]
- Beversdorf, D.Q. The role of the noradrenergic system in autism spectrum disorders, implications for treatment. Semin. Pediatr. Neurol. 2020, 35, 100834. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Bodyweight (kg) | Dose (mg) |
|---|---|
| >30 | 4 |
| 22.5–30 | 3 |
| 15–22.5 | 2 |
| <15 | N/A |
| Number of Patients Propranolol Group | Number of Patients Placebo Group | |
|---|---|---|
| Gender | ||
| Male | 5 | 4 |
| Female | 0 | 0 |
| Age (years) | ||
| 3–6 | 4 | 2 |
| 7–10 | 1 | 2 |
| Body weight (kg)-adjusted doses (mg) | ||
| >30 kg, 4 mg | 2 | 2 |
| 22.5–30 kg, 3 mg | 1 | 1 |
| 15–22.4 kg, 2 mg | 2 | 1 |
| Task | Propranolol: Baseline | Propranolol: 12 wk | Placebo: Baseline | Placebo: 12 wk |
|---|---|---|---|---|
| GSOM total | 31.7 (±16.9 SD) | 48.3 (±14.0 SD) | 20.5 (±6.4 SD) | 20.0 (±15.6 SD) |
| SRS | 76.0 (±12.0 SD) | 79.3 (±17.0 SD) | 75.0 (±1.4 SD) | 72.0 (±2.8 SD) |
| PAS | 78.0 (±24.3 SD) | 87.7 (±32.9 SD) | 64.0 (±19.8 SD) | 71.5 (±30.4 SD) |
| SEQ | 91.0 (±26.0 SD) | 102.3 (±30.7 SD) | 116.0 (±29.7 SD) | 102.0 (±35.4 SD) |
| Vineland: communication | 81.7 (±12.1 SD) | 76.0 (±26.2 SD) | 75.0 (±22.6 SD) | 74.5 (±29.0 SD) |
| Vineland: daily living | 81.3 (±6.4 SD) | 69.7 (±20.4 SD) | 76.5 (±14.8 SD) | 77.0 (±22.6 SD) |
| Vineland: social | 70.3 (±8.5 SD) | 70.7 (±10.2 SD) | 66.0 (±26.9 SD) | 66.5 (±23.3 SD) |
| AIM: peer interaction Subdomain impact raw score | 31.3 (±5.0 SD) | 23.7 (±8.7 SD) | 26.5 (±9.2 SD) | 24.5 (±6.4 SD) |
| AIM: social reciprocity Subdomain impact raw score | 30.7 (±1.5 SD) | 31.3 (±3.1 SD) | 37.5 (±9.2 SD) | 32.0 (±9.9 SD) |
| AIM: atypical behavior Subdomain impact raw score | 31.3 (±11.0 SD) | 36.7 (±15.3 SD) | 26.0 (±5.7 SD) | 25.0 (±1.4 SD) |
| AIM: communication Subdomain impact raw score | 39.0 (±6.0 SD) | 36.0 (±11.8 SD) | 45.0 (±8.5 SD) | 41.0 (±8.5 SD) |
| AIM: repetitive behavior Subdomain impact raw score | 38.7 (±16.2 SD) | 41.7 (±19.7 SD) | 49.5 (±7.8 SD) | 45.0 (±15.6 SD) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hirst, K.; Zamzow, R.M.; Stichter, J.P.; Beversdorf, D.Q. A Pilot Feasibility Study Assessing the Combined Effects of Early Behavioral Intervention and Propranolol on Autism Spectrum Disorder (ASD). Children 2023, 10, 1639. https://doi.org/10.3390/children10101639
Hirst K, Zamzow RM, Stichter JP, Beversdorf DQ. A Pilot Feasibility Study Assessing the Combined Effects of Early Behavioral Intervention and Propranolol on Autism Spectrum Disorder (ASD). Children. 2023; 10(10):1639. https://doi.org/10.3390/children10101639
Chicago/Turabian StyleHirst, Kathy, Rachel M. Zamzow, Janine P. Stichter, and David Q. Beversdorf. 2023. "A Pilot Feasibility Study Assessing the Combined Effects of Early Behavioral Intervention and Propranolol on Autism Spectrum Disorder (ASD)" Children 10, no. 10: 1639. https://doi.org/10.3390/children10101639