
Outcomes of a Parent-Delivered Baby-mCIMT Model for Infants at High Risk of Unilateral Cerebral Palsy Using Remote Coaching in Telerehabilitation

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Intervention
2.3.1. Characteristics of Remote and In-Person Baby-mCIMT
2.3.2. Differences between Remote and In-Person Baby-mCIMT
2.3.3. Specific Characteristics of the Remote Baby-mCIMT Program
2.4. Procedure for Assessment
2.4.1. Assessments of Outcome
2.4.2. Baseline Measurement
2.5. Statistical Analysis
3. Result
3.1. Characteristics of the Study Population
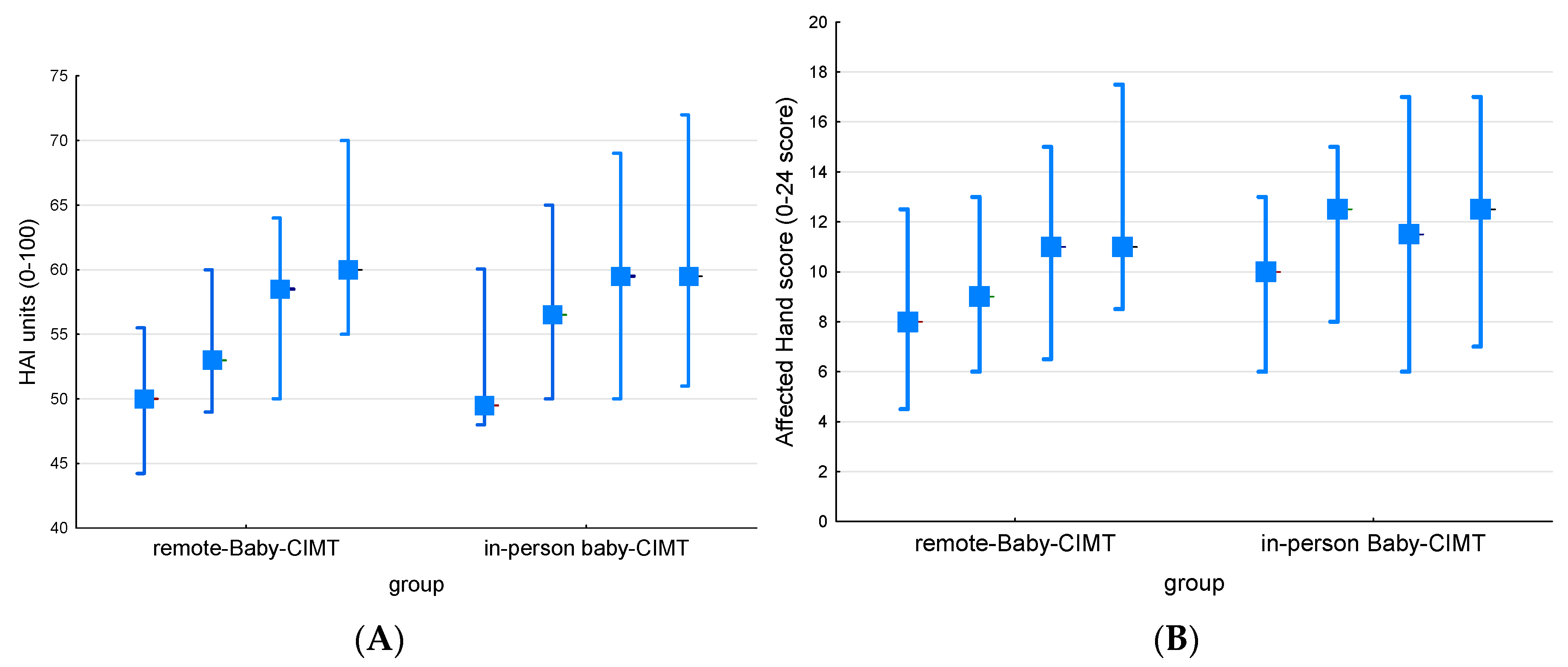
3.2. Outcome in HAI Units and Affected Hand Raw Score after Intervention
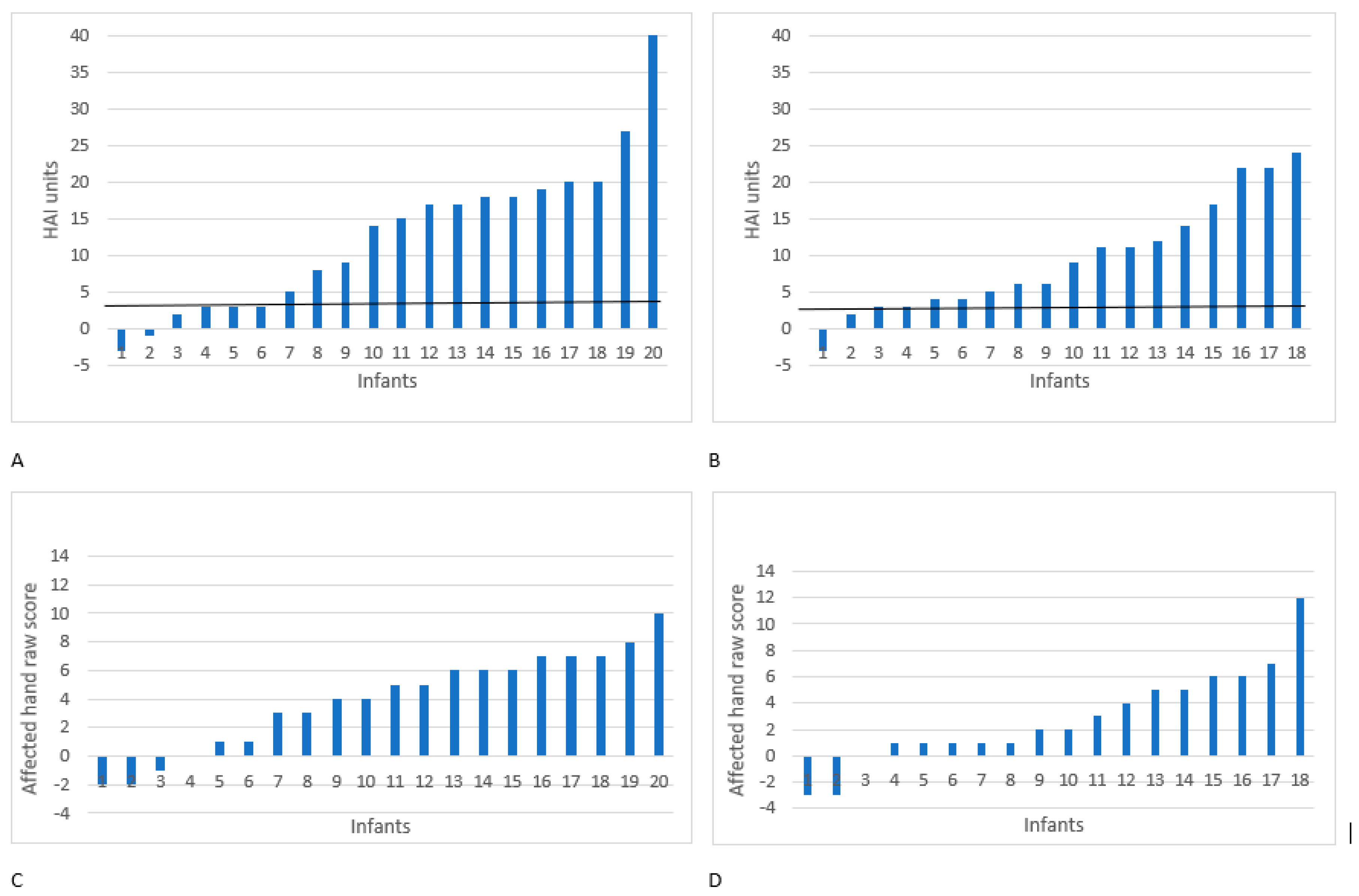
3.3. Individual Variation and Correlations
3.4. Outcome in HAI Units during Different Intervention Periods
3.5. Feasibility of the Intervention
4. Discussion
4.1. Digital Coaching versus In-Person Coaching
4.2. Feasibility of the Program
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morgan, C.; Fetters, L.; Adde, L.; Badawi, N.; Bancale, A.; Boyd, R.N.; Chorna, O.; Cioni, G.; Damiano, D.L.; Darrah, J.; et al. Early Intervention for Children Aged 0 to 2 Years with or at High Risk of Cerebral Palsy: International Clinical Practice Guideline Based on Systematic Reviews. JAMA Pediatr. 2021, 175, 846–858. [Google Scholar] [CrossRef]
- Hoare, B.J.; Wallen, M.A.; Thorley, M.N.; Jackman, M.L.; Carey, L.M.; Imms, C. Constraint-induced movement therapy in children with unilateral cerebral palsy. Cochrane Database Syst. Rev. 2019, 4, Cd004149. [Google Scholar] [CrossRef]
- Novak, I.; Morgan, C.; Fahey, M.; Finch-Edmondson, M.; Galea, C.; Hines, A.; Langdon, K.; Namara, M.M.; Paton, M.C.; Popat, H.; et al. State of the Evidence Traffic Lights 2019: Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy. Curr. Neurol. Neurosci. Rep. 2020, 20, 3. [Google Scholar] [CrossRef]
- Mailleux, L.; De Beukelaer, N.; Carbone, M.B.; Ortibus, E. Early interventions in infants with unilateral cerebral palsy: A systematic review and narrative synthesis. Res. Dev. Disabil. 2021, 117, 104058. [Google Scholar] [CrossRef]
- Eliasson, A.C.; Nordstrand, L.; Ek, L.; Lennartsson, F.; Sjostrand, L.; Tedroff, K.; Krumlinde-Sundholm, L. The effectiveness of Baby-CIMT in infants younger than 12 months with clinical signs of unilateral-cerebral palsy; an explorative study with randomized design. Res. Dev. Disabil. 2018, 72, 191–201. [Google Scholar] [CrossRef]
- Baker, A.; Niles, N.; Kysh, L.; Sargent, B. Effect of Motor Intervention for Infants and Toddlers With Cerebral Palsy: A Systematic Review and Meta-analysis. Pediatr. Phys. Ther. 2022, 34, 297–307. [Google Scholar] [CrossRef]
- Eliasson, A.C.; Krumlinde-Sundholm, L.; Gordon, A.M.; Feys, H.; Klingels, K.; Aarts, P.B.; Rameckers, E.; Autti-Ramo, I.; Hoare, B. European network for Health Technology Assessment: Guidelines for future research in constraint-induced movement therapy for children with unilateral cerebral palsy: An expert consensus. Dev. Med. Child Neurol. 2014, 56, 125–137. [Google Scholar] [CrossRef]
- Walker, C.; Shierk, A.; Roberts, H. Constraint Induced Movement Therapy in Infants and Toddlers with Hemiplegic Cerebral Palsy: A Scoping Review. Occup. Ther. Health Care 2022, 36, 29–45. [Google Scholar] [CrossRef]
- Reidy, T.G.; Carney, J.; Whiston, N.; Naber, E. Infant constraint induced movement therapy: Lessons learned from clinical implementation. J. Pediatr. Rehabil. Med. 2017, 10, 61–67. [Google Scholar] [CrossRef]
- DeLuca, S.C.; Trucks, M.R.; Wallace, D.A.; Ramey, S.L. Practice-based evidence from a clinical cohort that received pediatric constraint- induced movement therapy. J. Pediatr. Rehabil. Med. 2017, 10, 37–46. [Google Scholar] [CrossRef]
- Gelkop, N.; Burshtein, D.G.; Lahav, A.; Brezner, A.; Al-Oraibi, S.; Ferre, C.L.; Gordon, A.M. Efficacy of constraint-induced movement therapy and bimanual training in children with hemiplegic cerebral palsy in an educational setting. Phys. Occup. Ther. Pediatr. 2015, 35, 24–39. [Google Scholar] [CrossRef]
- Schlichting, T.; Martins da Silva, K.; Silva Moreira, R.; Marques de Moraes, M.V.; Cicuto Ferreira Rocha, N.A.; Boyd, R.N.; Neves Dos Santos, A. Telehealth Program for Infants at Risk of Cerebral Palsy during the Covid-19 Pandemic: A Pre-post Feasibility Experimental Study. Phys. Occup. Ther. Pediatr. 2022, 42, 490–509. [Google Scholar] [CrossRef]
- Cristinziano, M.; Assenza, C.; Antenore, C.; Pellicciari, L.; Foti, C.; Morelli, D. Telerehabilitation during COVID-19 lockdown and gross motor function in cerebral palsy: An observational study. Eur. J. Phys. Rehabil. Med. 2022, 58, 592–597. [Google Scholar] [CrossRef]
- da Silva, T.D.; da Silva, P.L.; Valenzuela, E.J.; Dias, E.D.; Simcsik, A.O.; de Carvalho, M.G.; Fontes, A.; Alberissi, C.A.O.; de Araújo, L.V.; Brandão, M.; et al. Serious Game Platform as a Possibility for Home-Based Telerehabilitation for Individuals With Cerebral Palsy During COVID-19 Quarantine—A Cross-Sectional Pilot Study. Front. Psychol. 2021, 12, 622678. [Google Scholar] [CrossRef]
- Richmond, T.; Peterson, C.; Cason, J.; Billings, M.; Terrell, E.A.; Lee, A.C.W.; Towey, M.; Parmanto, B.; Saptono, A.; Cohn, E.R.; et al. American Telemedicine Association’s Principles for Delivering Telerehabilitation Services. Int. J. Telerehabil. 2017, 9, 63–68. [Google Scholar] [CrossRef]
- WHO Global Observatory for eHealth. Telemedicine: Opportunities and Developments in Member States: Report on the Second Global Survey on eHealth. World Health Organization. Available online: https://apps.who.int/iris/handle/10665/44497 (accessed on 1 December 2023).
- Pagaki-Skaliora, M.; Morrow, E.; Theologis, T. Telehealth and Remote Interventions for Children with Cerebral Palsy: Scoping Review. JMIR Rehabil. Assist. Technol. 2022, 9, e36842. [Google Scholar] [CrossRef]
- Hung Kn, G.; Fong, K.N. Effects of telerehabilitation in occupational therapy practice: A systematic review. Hong Kong J. Occup Ther. 2019, 32, 3–21. [Google Scholar] [CrossRef]
- Camden, C.; Pratte, G.; Fallon, F.; Couture, M.; Berbari, J.; Tousignant, M. Diversity of practices in telerehabilitation for children with disabilities and effective intervention characteristics: Results from a systematic review. Disabil. Rehabil. 2020, 42, 3424–3436. [Google Scholar] [CrossRef]
- Graham, F.; Rodger, S.; Ziviani, J. Enabling occupational performance of children through coaching parents: Three case reports. Phys. Occup. Ther. Pediatr. 2010, 30, 4–15. [Google Scholar] [CrossRef]
- Seruya, F.M.; Feit, E.; Tirado, A.; Ottomanelli, D.; Celio, M. Caregiver Coaching in Early Intervention: A Scoping Review. Am. J. Occup. Therapy. 2022, 76, 7604205070. [Google Scholar] [CrossRef]
- Basu, A.P.; Pearse, J.; Watson, R.; Dulson, P.; Baggaley, J.; Wright, B.; Howel, D.; Vale, L.; Mitra, D.; Embleton, N.; et al. Feasibility trial of an early therapy in perinatal stroke (eTIPS). BMC Neurol. 2018, 18, 102. [Google Scholar] [CrossRef]
- Morgan, C.; Novak, I.; Dale, R.C.; Guzzetta, A.; Badawi, N. Single blind randomised controlled trial of GAME (Goals—Activity - Motor Enrichmentin infants at high risk of cerebral palsy. Res. Dev. Disabil. 2016, 55, 256–267. [Google Scholar] [CrossRef] [PubMed]
- Eliasson, A.C.; Sjostrand, L.; Ek, L.; Krumlinde-Sundholm, L.; Tedroff, K. Efficacy of baby-CIMT: Study protocol for a randomised controlled trial on infants below age 12 months, with clinical signs of unilateral CP. BMC Pediatr. 2014, 14, 141. [Google Scholar] [CrossRef] [PubMed]
- Santarossa, S.; Kane, D.; Senn, C.Y.; Woodruff, S.J. Exploring the Role of In-Person Components for Online Health Behavior Change Interventions: Can a Digital Person-to-Person Component Suffice? J. Med. Internet Res. 2018, 20, e144. [Google Scholar] [CrossRef] [PubMed]
- Krumlinde-Sundholm, L.; Ek, L.; Sicola, E.; Sjöstrand, L.; Guzzetta, A.; Sgandurra, G.; Cioni, G.; Eliasson, A.C. Development of the Hand Assessment for Infants: Evidence of internal scale validity. Dev. Med. Child Neurol. 2017, 59, 1276–1283. [Google Scholar] [CrossRef]
- Romeo, D.M.; Ricci, D.; Brogna, C.; Mercuri, E. Use of the Hammersmith Infant Neurological Examination in infants with cerebral palsy: A critical review of the literature. Dev. Med. Child Neurol. 2016, 58, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Taub, E.; Ramey, S.L.; DeLuca, S.; Echols, K. Efficacy of constraint-induced movement therapy for children with cerebral palsy with asymmetric motor impairment. Pediatrics 2004, 113, 305–312. [Google Scholar] [CrossRef]
- Ullenhag, A.; Ek, L.; Eliasson, A.C.; Krumlinde-Sundholm, L. Interrater and test-retest reliability of the Hand Assessment for Infants. Dev. Med. Child Neurol. 2021, 63, 1456–1461. [Google Scholar] [CrossRef]
- Darrah, J.; Piper, M.; Watt, M.J. Assessment of gross motor skills of at-risk infants: Predictive validity of the Alberta Infant Motor Scale. Dev. Med. Child Neurol. 1998, 40, 485–491. [Google Scholar] [CrossRef]
- Ashwal, S.; Russman, B.S.; Blasco, P.A.; Miller, G.; Sandler, A.; Shevell, M.; Stevenson, R. Practice parameter: Diagnostic assessment of the child with cerebral palsy: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 2004, 62, 851–863. [Google Scholar] [CrossRef]
- Chamudot, R.; Parush, S.; Rigbi, A.; Horovitz, R.; Gross-Tsur, V. Effectiveness of Modified Constraint-Induced Movement Therapy Compared with Bimanual Therapy Home Programs for Infants with Hemiplegia: A Randomized Controlled Trial. Am. J. Occup. Therapy. Off. Publ. Am. Occup. Ther. Assoc. 2018, 72, 7206205010p1–7206205010p9. [Google Scholar] [CrossRef]
- Holmstrom, L.; Eliasson, A.C.; Almeida, R.; Furmark, C.; Weiland, A.L.; Tedroff, K.; Lowing, K. Efficacy of the Small Step Program in a Randomized Controlled Trial for Infants under 12 Months Old at Risk of Cerebral Palsy (CP) and Other Neurological Disorders. J. Clin. Med. 2019, 8, 1016. [Google Scholar] [CrossRef] [PubMed]
- van Balen, L.C.; Dijkstra, L.J.; Dirks, T.; Bos, A.F.; Hadders-Algra, M. Early Intervention and Postural Adjustments During Reaching in Infants at Risk of Cerebral Palsy. Pediatr. Phys. Ther. 2019, 31, 175–183. [Google Scholar] [CrossRef]
- Eliasson, A.C.; Krumlinde-sundholm, L.; Shaw, K.; Wang, C. Effects of constraint-induced movement therapy in young children with hemiplegic cerebral palsy: An adapted model. Dev. Med. Child Neurol. 2005, 47, 266–275. [Google Scholar] [CrossRef]
- Miller, W.; Rollnick, S. Motivational Interviewing: Preparing People for Change, 2nd ed.; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Baldwin, P.; King, G.; Evans, J.; McDougall, S.; Tucker, M.A.; Servais, M. Solution-focused coaching in pediatric rehabilitation: An integrated model for practice. Phys. Occup. Ther. Pediatr. 2013, 33, 467–483. [Google Scholar] [CrossRef] [PubMed]
- Hurd, C.L.; Barnes, M.; Diot, C.M.; Condliffe, E.G.; Alazem, H.; Pritchard, L.; Zwicker, J.D.; McCormick, A.; Watt, M.J.; Andersen, J.; et al. Parent-therapist partnership to ELEVATE gross motor function in children with perinatal stroke: Protocol for a mixed methods randomized controlled trial. BMC Pediatr. 2022, 22, 480. [Google Scholar] [CrossRef] [PubMed]
- Hutchon, B.; Gibbs, D.; Harniess, P.; Jary, S.; Crossley, S.L.; Moffat, J.V.; Basu, N.; Basu, A.P. Early intervention programmes for infants at high risk of atypical neurodevelopmental outcome. Dev. Med. Child Neurol. 2019, 61, 1362–1367. [Google Scholar] [CrossRef]
- King, G.; Chiarello, L. Family-centered care for children with cerebral palsy: Conceptual and practical considerations to advance care and practice. J. Child Neurol. 2014, 29, 1046–1054. [Google Scholar] [CrossRef]
- Roberts, C.A.; Smith, K.C.; Sherman, A.K. Comparison of Online and Face-to-Face Parent Education for Children with Autism and Sleep Problems. J. Autism Dev. Disord. 2019, 49, 1410–1422. [Google Scholar] [CrossRef]
- Grafft, N.; Aftosmes-Tobio, A.; Gago, C.; Lansburg, K.; Beckerman-Hsu, J.; Trefry, B.; Kumanyika, S.; Davison, K. Adaptation and implementation outcomes of a parenting program for low-income, ethnically diverse families delivered virtually versus in-person. Transl. Behav. Med. 2022, 12, 1065–1075. [Google Scholar] [CrossRef]
- Thabane, L.; Ma, J.; Chu, R.; Cheng, J.; Ismaila, A.; Rios, L.P.; Robson, R.; Thabane, M.; Giangregorio, L.; Goldsmith, C.H. A tutorial on pilot studies: The what, why and how. BMC Med. Res. Methodol. 2010, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Beani, E.; Menici, V.; Cecchi, A.; Cioni, M.L.; Giampietri, M.; Rizzi, R.; Sgandurra, G.; Cioni, G. Feasibility Analysis of CareToy-Revised Early Intervention in Infants at High Risk for Cerebral Palsy. Front. Neurol. 2020, 11, 601137. [Google Scholar] [CrossRef] [PubMed]
- Harniess, P.A.; Gibbs, D.; Bezemer, J.; Purna Basu, A. Parental engagement in early intervention for infants with cerebral palsy-A realist synthesis. Child Care Health Dev. 2022, 48, 359–377. [Google Scholar] [CrossRef] [PubMed]
- Provenzi, L.; Grumi, S.; Gardani, A.; Aramini, V.; Dargenio, E.; Naboni, C.; Vacchini, V.; Borgatti, R. Italian parents welcomed a telehealth family-centred rehabilitation programme for children with disability during COVID-19 lockdown. Acta Paediatr. 2021, 110, 194–196. [Google Scholar] [CrossRef]
- Sakzewski, L.; Sicola, E.; Verhage, C.H.; Sgandurra, G.; Eliasson, A.C. Development of hand function during the first year of life in children with unilateral cerebral palsy. Dev. Med. Child Neurol. 2019, 61, 563–569. [Google Scholar] [CrossRef]
- McCormack, J.; Baker, E.; Masso, S.; Crowe, K.; McLeod, S.; Wren, Y.; Roulstone, S. Implementation fidelity of a computer-assisted intervention for children with speech sound disorders. Int. J. Speech-Lang. Pathol. 2017, 19, 265–276. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Children at High Risk of UCP | |||
|---|---|---|---|
| Remote Coaching Baby-mCIMT (n = 20) | In-Person Coaching Baby-mCIMT (n = 18) | Statistics | |
| Gestational age, weeks, mean (SD) (min–max) | 38 (3.2) (31–41) | 34 (6.5) (23–41) | p < 0.001 |
| Age (CA) at baseline, months, mean (SD) (min–max) | 7 (2.8) (3–13) | 6 (1.7) (4–9) | p = 0.227 |
| Gender, male/female | 12/8 | 8/10 | p = 0.300 |
| Preterm/term | 4/16 | 8/10 | p = 0.106 |
| HAI units at start (0–100), mean (SD) (min–max) | 51 (8) (39–65) | 52 (8) (42–69) | p = 0.599 |
| Affected hand, left/right n (%) | 11 (55%)/9 (45%) | 7 (39%)/11 (61%) | p = 0.481 |
| Weeks of inclusion, mean (SD) (min–max) | 25.5 (5.3) (19–36) | 22.7 (3.4) (17–29) | p = 0.026 |
| AIMS at baseline | Missing, n = 8 | Missing, n = 3 | |
| <5 | 8 | 3 | |
| 5–10 | 2 | 3 | |
| 10–25 | 1 | 6 | |
| >25 | 1 | 3 | |
| Diagnosis CP,1 year of age | |||
| Unilateral CP | 17 | 18 | |
| Bilateral CP | 1 | 0 | |
| No diagnosis | 2 * | 0 | |
| Neuroimaging ** | Missing, n = 3 | Missing, n = 3 | |
| No sign of lesion | 0 | 0 | |
| Focal infarct | 8 | 4 | |
| WMDI | 7 | 7 | |
| Miscellaneous | 2 | 3 | |
| Malformation | 0 | 1 | |
| Outcome | Baseline | After Period 1 | Before Period 2 | After Period 2 | Difference within Groups: Baseline–after Period 2 a | Difference between Groups: Baseline–after Period 2 b |
|---|---|---|---|---|---|---|
| HAI units (0–100) | ||||||
| Remote coaching Baby-mCIMT | 50 (44:57) | 53 * (50:59) | 59 (49:64) | 60 (55:70) | p ≤ 0.001 | p = 0.803 |
| In-person coaching Baby-mCIMT | 50 (48:60) | 57 (50:65) | 60 (50:69) | 60 (51:72) | p = 0.001 | |
| Affected-hand raw score (0–24) | ||||||
| Remote coaching Baby-mCIMT | 8 (5:13) | 9 * (6:13) | 11 (7:15) | 11 (9:18) | p ≤ 0.001 | p = 0.942 |
| In-person coaching Baby-mCIMT | 10 (6:13) | 13 (8:15) | 12 (6:17) | 13 (7:17) | p = 0.005 | |
| Questions | % | % | % | % |
|---|---|---|---|---|
| How did the training go? | Very easy | Easy | Difficult | Very difficult |
| Remote coaching Baby-mCIMT | 6 | 73 | 13 | 7 |
| In-person coaching Baby-mCIMT | 6 | 59 | 36 | 0 |
| How significant was the support provided by the occupational therapist via the video meeting/home visits? | Of great significance | Of some significance | Of less significance | It would have probably gone well anyway |
| Remote coaching Baby-mCIMT | 93 | 0 | 7 | 0 |
| In-person coaching Baby-mCIMT | 75 | 25 | 0 | 0 |
| How did you perceive that the training affected your child’s hand function? | Good effect | Some effect | Minor effect | No effect |
| Remote coaching Baby-mCIMT | 73 | 20 | 0 | 7 |
| In-person coaching Baby-mCIMT | 59 | 41 | 0 | 0 |
| Would you recommend the training to other parents in similar situations? | Absolutely | Sure, it is ok | With some doubt | No |
| Remote coaching Baby-mCIMT *** | 93 | 0 | 7 | 0 |
| In-person coaching Baby-mCIMT | 75 | 25 | 0 | 0 |
| How laborious/difficult did you find it to complete the training? | Very difficult | Quite difficult | Pretty easy | Usually easy |
| Remote Baby-mCIMT * | 8 | 46 | 38 | 8 |
| What did you think about the material that was on the web? | Very informative and inspiring | Fairly relevant to my family | Not helpful | Can’t remember reading it |
| Remote coaching Baby-mCIMT ** | 36 | 64 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Svensson, K.; Sundelin, H.; Eliasson, A.-C. Outcomes of a Parent-Delivered Baby-mCIMT Model for Infants at High Risk of Unilateral Cerebral Palsy Using Remote Coaching in Telerehabilitation. Children 2024, 11, 101. https://doi.org/10.3390/children11010101
Svensson K, Sundelin H, Eliasson A-C. Outcomes of a Parent-Delivered Baby-mCIMT Model for Infants at High Risk of Unilateral Cerebral Palsy Using Remote Coaching in Telerehabilitation. Children. 2024; 11(1):101. https://doi.org/10.3390/children11010101
Chicago/Turabian StyleSvensson, Katarina, Heléne Sundelin, and Ann-Christin Eliasson. 2024. "Outcomes of a Parent-Delivered Baby-mCIMT Model for Infants at High Risk of Unilateral Cerebral Palsy Using Remote Coaching in Telerehabilitation" Children 11, no. 1: 101. https://doi.org/10.3390/children11010101