
Knee Flexion While Walking Exceeds Knee Flexion Contracture in Children with Spastic Cerebral Palsy

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Joint Contractures
2.3. Movement Analysis
2.4. Functional Mobility
2.5. Statistics
3. Results
3.1. Joint Contractures
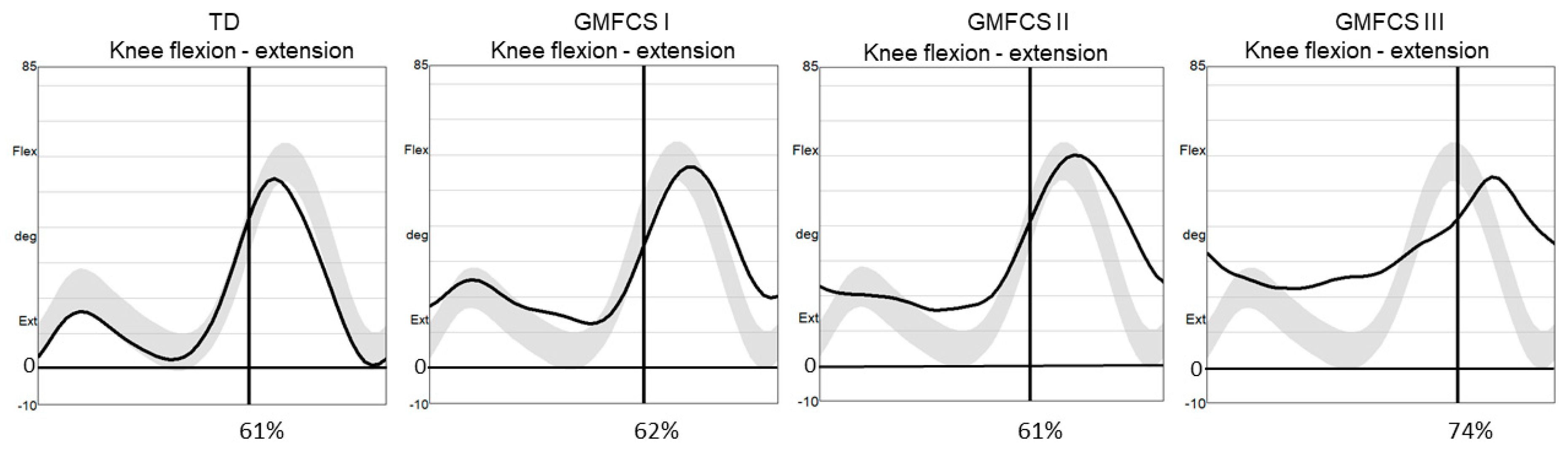
3.2. Knee Position at Initial Foot Contact (KneeAngleIC)
3.3. Minimum Knee Flexion in Stance (MinKneeFlexSt)
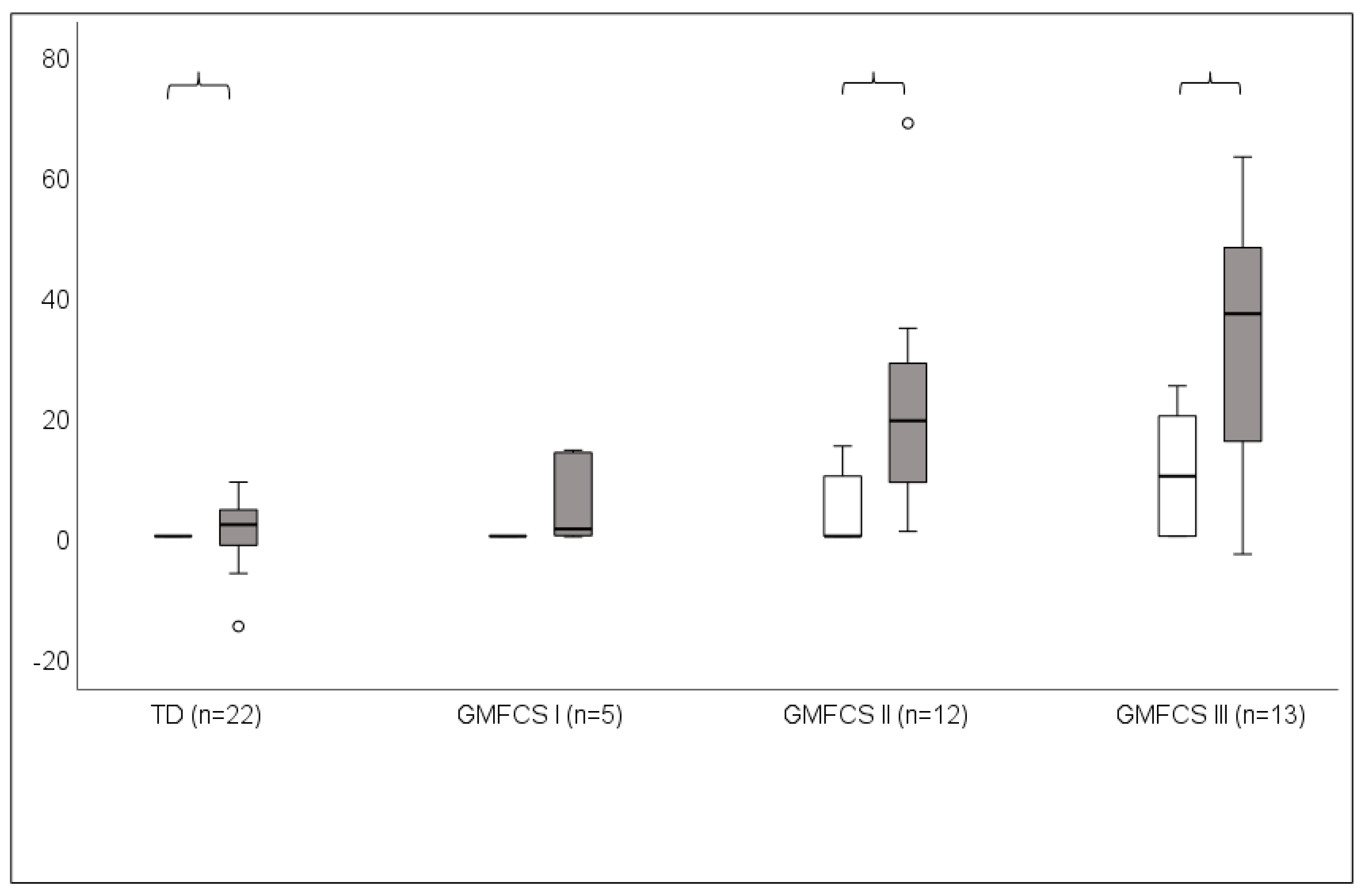
3.4. Knee Contractures versus Minimum Knee Flexion in Stance (MinKneeFlexSt)
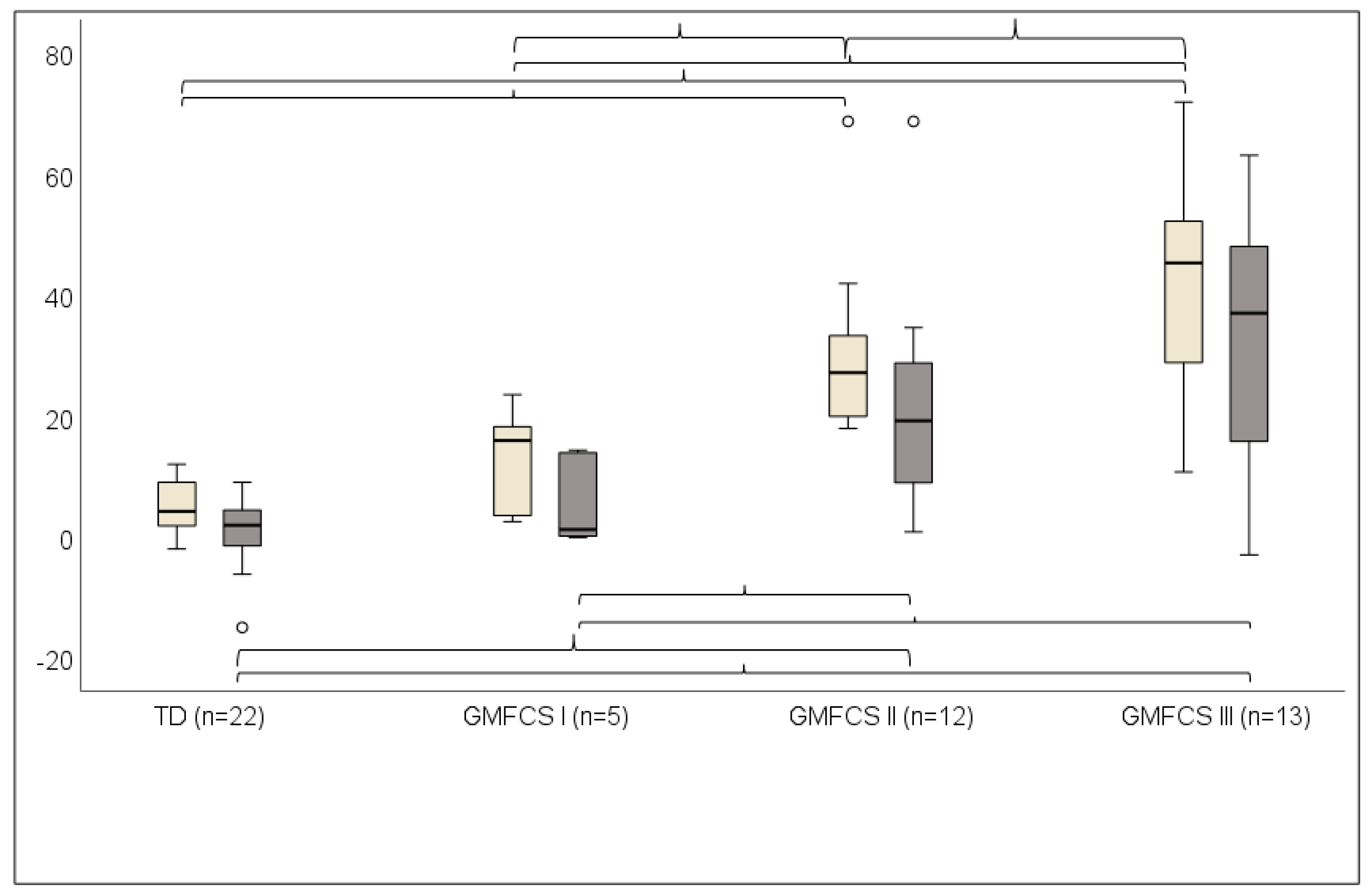
3.5. Knee Position at Initial Foot Contact (KneeAngleIC) versus Minimum Knee Flexion in Stance (MinKneeFlexSt)
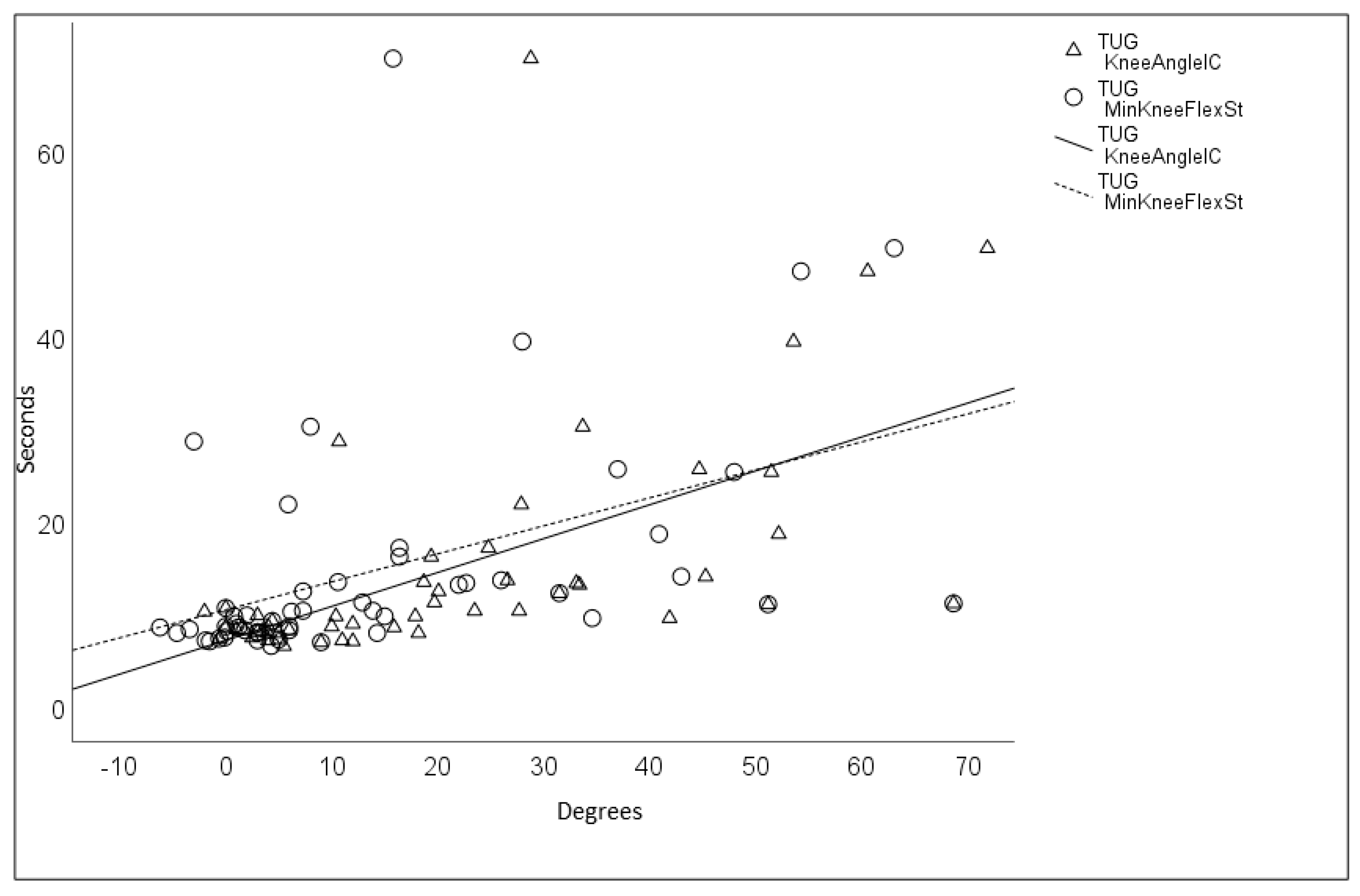
3.6. Timed up and Go Test (TUG)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M.; Damiano, D.; Jacobsson, B. A report: The definition and classification of cerebral palsy April 2006. Dev. Med. Child Neurol. 2007, 109, 8–14. [Google Scholar]
- Palisano, R.J.; Rosenbaum, P.; Bartlett, D.; Livingston, M.H. Content validity of the expanded and revised Gross Motor Function Classification System. Dev. Med. Child Neurol. 2008, 50, 744–750. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, S.; Goldsmith, S.; Webb, A.; Ehlinger, V.; Hollung, S.J.; McConnell, K.; Arnaud, C.; Smithers-Sheedy, H.; Oskoui, M.; Khandaker, G.; et al. Global prevalence of cerebral palsy: A systematic analysis. Dev. Med. Child Neurol. 2022, 64, 1494–1506. [Google Scholar] [CrossRef] [PubMed]
- Jackman, M.; Sakzewski, L.; Morgan, C.; Boyd, R.N.; Brennan, S.E.; Langdon, K.; Toovey, R.A.M.; Greaves, S.; Thorley, M.; Novak, I. Interventions to improve physical function for children and young people with cerebral palsy: International clinical practice guideline. Dev. Med. Child Neurol. 2022, 64, 536–549. [Google Scholar] [CrossRef] [PubMed]
- Miller, F. Crouch gait in Cerebral Palsy. In Cerebral Palsy; Miller, F., Bachrach, S., Lennon, N., O’Neil, M.E., Eds.; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Miller, F. Knee Flexion Deformity in Cerebral Palsy. In Cerebral Palsy; Miller, F., Bachrach, S., Lennon, N., O’Neil, M.E., Eds.; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Baird, G.; Chandler, S.; Shortland, A.; Will, E.; Simonoff, E.; Scrutton, D.; Fairhurst, C. Acquisition and loss of best walking skills in children and young people with bilateral cerebral palsy. Dev. Med. Child Neurol. 2022, 64, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Cloodt, E.; Lindgren, A.; Lauge-Pedersen, H.; Rodby-Bousquet, E. Sequence of flexion contracture development in the lower limb: A longitudinal analysis of 1,071 children with cerebral palsy. BMC Musculoskelet. Disord. 2022, 23, 629. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, D.H.; Cooper, D. The pathomechanics of progressive crouch gait in spastic diplegia. Orthop. Clin. N. Am. 1978, 1, 143–154. [Google Scholar] [CrossRef]
- Sutherland, D.H.; Davids, J.R. Common gait abnormalities of the knee in cerebral palsy. Clin. Orthop. Relat. Res. 1993, 288, 139–147. [Google Scholar]
- Rodda, J.; Graham, H.K. Classification of gait patterns in spastic hemiplegia and spastic diplegia: A basis for a management algorithm. Eur. J. Neurol. 2001, 8 (Suppl. S5), 98–108. [Google Scholar] [CrossRef]
- Rodda, J.; Graham, H.K.; Carson, L.; Galea, M.P.; Wolfe, R. Sagittal gait patterns in spastic diplegia. J. Bone Jt. Surg. Br. 2004, 86, 251–258. [Google Scholar] [CrossRef]
- Sangeux, M.; Rodda, J.; Graham, H.K. Sagittal gait patterns in cerebral palsy: The plantarflexor–knee extension couple index. Gait Posture 2015, 41, 586–591. [Google Scholar] [CrossRef] [PubMed]
- Armand, S.; Decoulon, G.; Bonnefoy-Mazure, A. Gait analysis in children with cerebral palsy. I. Open Rev. 2016, 1, 448–460. [Google Scholar] [CrossRef] [PubMed]
- Sees, J.P.; Truong, W.H.; Novacheck, T.F.; Miller, F.; Georgiadis, A.G. What’s New in the Orthopaedic Treatment of Ambulatory Children With Cerebral Palsy Using Gait Analysis. J. Child Orthop. 2020, 6, 498–509. [Google Scholar] [CrossRef]
- Dreher, T.; Vegvari, D.; Wolf, S.I.; Geisbüsch, A.; Gantz, S.; Wenz, W.; Braatz, F. Development of knee function after hamstring lengthening as a part of multilevel surgery in children with spastic diplegia: A long-term outcome study. J. Bone Surg. 2012, 94, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Galey, S.A.; Lerner, Z.F.; Bulea, T.C.; Zimbler, S.; Damiano, D.L. Effectiveness of surgical and non-surgical management of crouch gait in cerebral palsy: A systematic review. Gait Posture 2017, 54, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Shideler, B.L.; Bulea, T.C.; Chen, J.; Stanley, C.J.; Gravunder, A.J.; Damiano, D.L. Toward a hybrid exoskeleton for crouch gait in children with cerebral palsy: Neuromuscular electrical stimulation for improved knee extension. J. Neuroeng. Rehabil. 2020, 17, 121. [Google Scholar] [CrossRef] [PubMed]
- Massion, J. Postural control system. Curr. Opin. Neurol. 1994, 4, 877–887. [Google Scholar] [CrossRef]
- Dan, B. Cerebral palsy is a sensorimotor disorder. Dev. Med. Child Neurol. 2020, 62, 768. [Google Scholar] [CrossRef]
- Alboresi, S.; Belmonti, V.; Ferrari, A.l.; Ferrari, A. Dysperceptive forms. In The Spastic Forms of Cerebral Palsy. A Guide to the Assessment of Adaptive Functions; Ferrari, A., Cioni, G., Eds.; Springer: Milan, Italy, 2010; pp. 273–291. [Google Scholar]
- Ferrari, A.; Bergamini, L.; Giorgio Guerzoni, G.; Calderara, S.; Bicocchi, N.; Vitetta, G.; Borghi, C.; Neviani, R.; Ferrari, A. Gait-Based Diplegia Classification Using LSMT Networks. J. Healthc. Eng. 2019, 2109, 3796898. [Google Scholar] [CrossRef]
- Lidbeck, C.; Bartonek, Å.; Yadav, P.; Tedroff, K.; Åstrand, P.; Hellgren, K.; Gutierrez-Farewik, E.M. The role of visual stimuli on standing posture in children with bilateral cerebral palsy. BMC Neurol. 2016, 16, 151. [Google Scholar] [CrossRef]
- Bartonek, A.; Lidbeck, C.; Hellgren, K.; Gutierrez-Farewik, E. Head and Trunk Movements During Turning Gait in Children with Cerebral Palsy. J. Mot. Behav. 2019, 51, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Lidbeck, C.; Bartonek, Å. Motor function at increasing postural demands in children with bilateral cerebral palsy. Eur. J. Phys. Rehabil. Med. 2021, 57, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Hislop, H.J.; Montgomery, J. Daniels and Worthingham’s Muscle Testing, Techniques of Manual Examination, 8th ed.; Saunders Company: Philadelphia, PA, USA, 2007. [Google Scholar]
- Bartonek, Å.; Eriksson, M.; Ericson, A.; Reimeringer, M.; Lidbeck, C. Evaluation of Knee Position Sense in Children with Motor Disabilities and Children with Typical Development: A Cross-Sectional Study. Children 2023, 10, 1056. [Google Scholar] [CrossRef] [PubMed]
- Mudge, A.; Bau, K.V.; Purcell, L.N.; Wu, J.C.; Axt, M.W.; Selber, P.; Burns, J. Normative reference values for lower limb joint range, bone torsion, and alignment in children aged 4–16 years. J. Pediatr. Orthop. B 2014, 23, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Barouk, P.; Barouk, L.S. Clinical diagnosis of gastrocnemius tightness. Foot Ankle Clin. 2014, 19, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, M.D.; Wolf, L.S.; Shurtleff, D.B.; Staheli, L.T. Hip flexion contractures: A comparison of measurement methods. Arch. Phys. Med. Rehabil. 1985, 66, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.; Õunpuu, S.; Tyburski, D.; Gage, J.R. A gait analysis data collection and reduction technique. Hum. Mov. Sci. 1991, 10, 575–587. [Google Scholar] [CrossRef]
- Williams, E.N.; Carroll, S.G.; Reddihough, D.S.; Phillips, B.A.; Galea, M.P. Investigation of the timed ‘up & go’ test in children. Dev. Med. Child Neurol. 2005, 47, 518–524. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Borelli, G.; Neviani, R.; Sghedoni, A.; Ovi, A.; Ferrari, A. La Fisioterapia Nella Paralisi Cerebrale Infantile. La Funzione Cammino; Springer: Milano, Italy, 2014; p. 50. (In Italian) [Google Scholar]
- Ferrari, A. Perceptive Defects. In The Spastic Forms of Cerebral Palsy; Ferrari, A., Cioni, G., Eds.; Springer: Milan, Italy, 2010; pp. 73–98. [Google Scholar]
- Ferrari, A.; Sghedoni, A.; Alboresi, S.; Pedroni, E.; Lombardi, F. New definitions of 6 clinical signs of perceptual disorder in children with cerebral palsy: An observational study through reliability measures. Eur. J. Phys. Rehabil. Med. 2014, 50, 709–716. [Google Scholar]
- Alboresi, S.; Sghedoni, A.; Borelli, G.; Costi, S.; Beccani, L.; Neviani, R.; Ferrari, A. Are perceptual disorder signs in diplegic cerebral palsied children stable over time? A retrospective cohort analysis. Minerva Pediatr. 2020, 72, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Noten, S.; Pettersson, K.; Czuba, T.; Cloodt, E.; Casey, J.; Rodby-Bousquet, E. Probability of independent walking and wheeled mobility in individuals with cerebral palsy. Dev. Med. Child Neurol. 2023, 1–7. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TD (n = 22) | GMFCS I (n = 5) | GMFCS II (n = 12) | GMFCS III (n = 13) | p Value | |
|---|---|---|---|---|---|
| Age median (min, max), years | 8.9 (6.5, 16.9) | 10.3 (8.6, 15.9) | 11.8 (8.2, 15.8) | 10.6 (7.6, 17.1) | 0.635 |
| Weight median (min, max), kg | 33.3 (22.3, 81.8) | 46.3 (31.6, 52.7) | 40.2 (26.4, 99.7) | 29.4 (18.5, 56.2) | 0.601 |
| Height median (min, max), cm | 140 (121, 181) | 145 (132, 164) | 153 (130, 166) | 137 (110, 170) | 0.385 |
| Joint contracture < neutral position in support limb expressed as “0”, median (min–max) degrees | |||||
| Ankle plantarflexion | 0 | 0 | 0 (0, 5) | 0 (0, 5) | 0.530 |
| Knee flexion | 0 | 0 | 0 (0, 15) | 0 (0, 25) | <0.001 * |
| Hip flexion | 0 | 0 | 0 (0, 15) | 0 (0, 15) | 0.167 |
| Orthopedic surgery performed (number of children) | - | 1 | 7 | 2 | 0.065 |
| Strayer (number of surgeries in both limbs) | - | 1 | 3 | 0 | 0.175 |
| Achilles tendon lengthening (number of surgeries in both limbs) | 1 | 5 | 2 | 0.323 | |
| Medial hamstrings (number of surgeries in both limbs) | 0 | 1 | 0 | 0.472 |
| TD n = 22 | GMFCS I n = 5 | GMFCS II n = 12 | GMFCS III n = 13 | p Value | |
|---|---|---|---|---|---|
| KneeAngleIC (°) median (min, max) | 4.2 (−2.0, 12.0) | 15.9 (2.5, 23.5) | 27.1 (17.9, 68.7) | 45.3 (10.7, 71.9) | <0.001 * |
| MinKneeFlexSt (°) median (min, max) | 2.5 (−6.2, 9.0) | 1.2 (−0.1, 14.3) | 19.2 (0.8, 68.7) | 37 (−3, 63.1) | <0.001 * |
| TUG (s) median (min, max) | 8.2 (6.5, 10.6) | 8.1 (7.4, 10.3) | 12.3 (9.5, 17.1) | 25.6 (11, 70) | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartonek, Å.; Lidbeck, C. Knee Flexion While Walking Exceeds Knee Flexion Contracture in Children with Spastic Cerebral Palsy. Children 2023, 10, 1867. https://doi.org/10.3390/children10121867
Bartonek Å, Lidbeck C. Knee Flexion While Walking Exceeds Knee Flexion Contracture in Children with Spastic Cerebral Palsy. Children. 2023; 10(12):1867. https://doi.org/10.3390/children10121867
Chicago/Turabian StyleBartonek, Åsa, and Cecilia Lidbeck. 2023. "Knee Flexion While Walking Exceeds Knee Flexion Contracture in Children with Spastic Cerebral Palsy" Children 10, no. 12: 1867. https://doi.org/10.3390/children10121867