
Stress and Anxiety among High School Adolescents: Correlations between Physiological and Psychological Indicators in a Longitudinal Follow-Up Study
 , , and
, , and
Abstract
:1. Introduction
Cortisol as a Biological Marker
- (1)
- How does the level of anxiety change during different periods of the school year (end of the year vs. beginning of the year)?
- (2)
- How do the results of psychological tests and biological sample collection relate to each other?
- (3)
- What are the differentiating factors underlying anxiety?
- (4)
- What is the correlation between anxiety and psychosomatic symptoms?
- (5)
- How does anxiety relate to performance expectations related to school tasks?
- (1)
- The level of anxiety decreases significantly after the summer vacation.
- (2)
- We can demonstrate a correlation between the level of anxiety measured by the psychological test and the cortisol level.
- (3)
- Certain characteristics, such as the gender of the respondent, the type of secondary school where he/she studies, the highest education level of the parents, and the family environment influence the level of anxiety.
- (4)
- A higher level of anxiety results in the appearance of psychosomatic symptoms.
2. Materials and Methods
2.1. Data Collection Methods
The Process of Generating the Scales Included in the Data Analysis
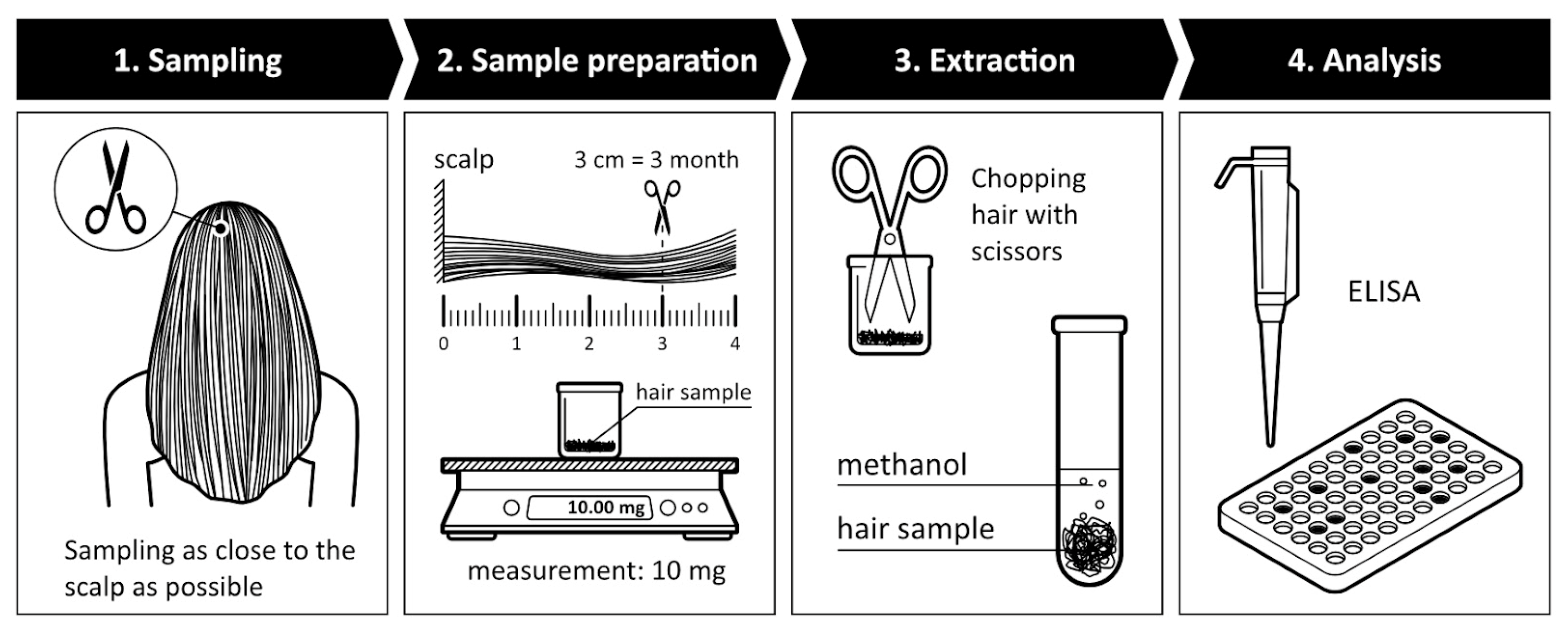
2.2. The Process of Biological Sample Collection
3. Results
3.1. The Main Characteristic of Sample
3.2. Results of the Study on Anxiety and Differentiating Factors of Anxiety
4. Discussion
4.1. Questionnaire Survey and Cortisol Level
4.2. Differences between School Types
4.3. Parental Expectations
4.4. Psychosomatic Symptoms
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chrousos, G.P. Stress and disorders of the stress system. Nat. Rev. Endocrinol. 2009, 5, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Kyrou, I.; Tsigos, C. Stress hormones: Physiological stress and regulation of metabolism. Curr. Opin. Pharmacol. 2009, 9, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Olinski, R.; Gackowski, D.; Foksinski, M.; Rozalski, R.; Roszkowski, K.; Jaruga, P. Oxidative DNA damage: Assessment of the role in carcinogenesis, atherosclerosis, and acquired immunodeficiency syndrome. Free Radic. Biol. Med. 2002, 33, 192. [Google Scholar] [CrossRef]
- Motta, E.; Motta, J.; Souza, L.N.; Vieira, B.B.; Delle, H.; Consolim-Colombo, F.M.; Egan, B.M.; Lopes, H.F. Acute physical and mental stress resulted in an increase in fatty acids, norepinephrine, and hemodynamic changes in normal individuals: A possible pathophysiological mechanism for hypertension-Pilot study. J. Clin. Hypertens. 2021, 23, 888–894. [Google Scholar] [CrossRef]
- Huang, C.J.; Webb, H.E.; Zourdos, M.C.; Acevedo, E.O. Cardiovascular reactivity, stress, and physical activity. Front Physiol. 2013, 4, 314. [Google Scholar] [CrossRef]
- Dhabhar, F.S. Effects of stress on immune function: The good, the bad, and the beautiful. Immunol. Res. 2014, 58, 193–210. [Google Scholar] [CrossRef] [PubMed]
- Dávid, I.; Fülöp, M.; Pataky, N.; Rudas, J. Stressz, Megküzdés, Versengés, Konfliktusok; Magyar Tehetségsegítő Szervezetek Szövetsége: Budapest, Hungary, 2014; pp. 99–100. [Google Scholar]
- Lazarus, R.S. From psychological stress to the emotins: A History of Changing Outlooks. Annu. Rev. Psychol. 1993, 44, 1–21. [Google Scholar] [CrossRef]
- Klatzkin, R.R.; Baldassaro, A.; Hayden, E. The impact of chronic stress on the predictors of acute stress-induced eating in women. Appetite 2018, 123, 343–351. [Google Scholar] [CrossRef]
- Gketsios, I.; Tsiampalis, T.; Foscolou, A.; Kalafati, I.P.; Vassilakou, T.; Kanellopoulou, A.; Notara, V.; Antonogeorgos, G.; Rojas-Gil, A.P.; Androutsos, O.; et al. Association between Family and School Pressures, Consumption of Ultra-Processed Beverages, and Obesity in Preadolescents: A School-Based Epidemiological Study. Children 2023, 10, 500. [Google Scholar] [CrossRef]
- Watson, P. PTS Dasa public mental health priority. Curr. Psy. Rep. 2019, 21, 61. [Google Scholar] [CrossRef]
- Cooper, C.L.; Davidson, M. Sources of stress at work and their relation to stressors in non-working environments. In Psychological Factors at Work and Their Realatin to Health; Kalimo, R., El-Batawi, M.A.E., Cooper, C.L., Eds.; WHO: Geneva, Switzerland, 1987; pp. 99–123. [Google Scholar]
- Cooper, C.L.; Marshall, J. Occupational sources of stress: A review of the literature relating to coronary heart disease and mental ill health. J. Occup. Psychol. 1976, 49, 1128. [Google Scholar] [CrossRef]
- Ádám, S.; Salavecz, G. A sterssz elméleti háttere és mérése: A Selye János lelki egészségprogram tesztbattériájának bemutatása. Mentálhigiéné És Pszichoszom 2010, 11, 53–58. [Google Scholar] [CrossRef]
- McDougall, T. Mental health problems in childhood and adolescence. Nurs. Stand. 2011, 26, 48–56, quiz 58–60. Available online: https://www.proquest.com/scholarly-journals/mental-health-problems-childhood-adolescence/docview/911105618/se-2 (accessed on 12 June 2023). [CrossRef] [PubMed]
- Ab Ghaffar, S.F.; Mohd Sidik, S.; Ibrahim, N.; Awang, H.; Gyanchand Rampal, L.R. Effect of a School-Based Anxiety Prevention Program among Primary School Children. Int. J. Environ. Res. Public. Health 2019, 16, 4913. [Google Scholar] [CrossRef] [PubMed]
- Nakie, G.; Segon, T.; Melkam, M.; Desalegn, G.T.; Zeleke, T.A. Prevalence and associated factors of depression, anxiety, and stress among high school students in, Northwest Ethiopia, 2021. BMC Psychiatry 2022, 22, 739. [Google Scholar] [CrossRef]
- Alharbi, R.; Alsuhaibani, K.; Almarshad, A.; Alyahya, A. Depression and anxiety among high school student at Qassim Region. J. Family Med. Prim. Care. 2019, 8, 504–510. [Google Scholar] [CrossRef]
- Eslam, A.A.; Rabiei, L.; Afzali, S.M.; Hamidizadeh, S.; Masoudi, R. The effectiveness of assertiveness training on the levels of stress, anxiety, and depression of High School Students. Iran. Red. Crescent Med. J. 2016, 18, e21096. [Google Scholar] [CrossRef]
- Moustaka, E.; Bacopoulou, F.; Manousou, K.; Kanaka-Gantenbein, C.; Chrousos, G.P.; Darviri, C. Educational Stress among Greek Adolescents: Associations between Individual, Study and School-Related Factors. Int. J. Environ. Res. Public. Health 2023, 20, 4692. [Google Scholar] [CrossRef]
- Sakka, S.; Nikopoulou, V.; Bonti, E.; Tatsiopoulou, P.; Karamouzi, P.; Giazkoulidou, A.; Tsipropoulou, V.; Parlapani, E.; Holeva, V.; Diakogiannis, I. Assessing test anxiety and resilience among Greek adolescents during COVID-19 pandemic. J. Mind Med. Sci. 2020, 7, 173–178. [Google Scholar] [CrossRef]
- Hembree, R. Correlates, Causes, Effects, and Treatment of Test Anxiety. Rev. Educ. Res. 1988, 58, 47–77. [Google Scholar] [CrossRef]
- Hembree, R. The Nature, Effects, and Relief of Mathematics Anxiety. J. Res. Math. Educ. 1990, 21, 33–46. [Google Scholar] [CrossRef]
- Von der Embse, N.; Jester, D.; Roy, D.; Post, J. Test anxiety effects, predictors, and correlates: A 30-year meta-analytic review. J. Affect. Disord. 2018, 227, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhao, N.; Kong, Q.P. The Relationship Between Math Anxiety and Math Performance: A Meta-Analytic Investigation. Front. Psychol. 2019, 10, 1613. [Google Scholar] [CrossRef]
- Namkung, J.M.; Peng, P.; Lin, X. The Relation Between Mathematics Anxiety and Mathematics Performance Among School-Aged Students: A Meta-Analysis. Rev. Educ. Res. 2019, 89, 459–496. [Google Scholar] [CrossRef]
- Barroso, C.; Ganley, C.M.; McGraw, A.L.; Geer, E.A.; Hart, S.A.; Daucourt, M.C. A meta-analysis of the relation between math anxiety and math achievement. Psychol. Bull. 2021, 147, 134–168. [Google Scholar] [CrossRef] [PubMed]
- Caviola, S.; Toffalini, E.; Giofrè, D.; Ruiz, J.M.; Szűcs, D.; Mammarella, I.C. Math Performance and Academic Anxiety Forms, from Sociodemographic to Cognitive Aspects: A Meta-analysis on 906,311 Participants. Educ. Psychol. Rev. 2021, 34, 363–399. [Google Scholar] [CrossRef]
- Ahmed, W.; Minnaert, A.; Kuyper, H.; Van der Werf, M. Reciprocal relationships between math self-concept and math anxiety. Learn. Individ. Differ. 2012, 22, 385–389. [Google Scholar] [CrossRef]
- Brown, M.; Brown, P.; Bibby, T. “I would rather die”: Reasons given by 16-year-olds for not continuing their study of mathematics. Res. Math. Educ. 2008, 10, 3–18. [Google Scholar] [CrossRef]
- Campagna, C.G.; Curtis, G.J. So Worried I Don’t Know what to Be: Anxiety is Associated with Increased Career Indecision and Reduced Career Certainty. Aust. J. Guid. Couns. 2007, 17, 91–96. [Google Scholar] [CrossRef]
- Foley, A.E.; Herts, J.B.; Borgonovi, F.; Guerriero, S.; Levine, S.C.; Beilock, S.L. The Math Anxiety-Performance Link. Curr. Dir. Psychol. Sci. 2017, 26, 52–58. [Google Scholar] [CrossRef]
- Orbach, L.; Fritz, A. Patterns of Attention and Anxiety in Predicting Arithmetic Fluency among School-Aged Children. Brain Sci. 2022, 12, 376. [Google Scholar] [CrossRef] [PubMed]
- Costello, E.J.; Mustillo, S.; ErkanI, A.; Keeler, G.; Angold, A. Prevalence and Development of Psychiatric Disorders in childhood and adolescence. Arch. Gen. Psychiatry 2003, 60, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Langley, A.K.; Bergman, R.L.; McCracken, J.; Piacentini, J.C. Impairment in childhood anxiety disorders: Preliminary examination of the child anxiety impact scale–parent version. J. Child. Adolesc. Psychopharmacol. 2004, 14, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Kim-Cohen, J.; Caspi, A.; Moffitt, T.E.; Harrington, H.; Milne, B.J.; Poulton, R. Prior juvenile diagnoses in adults with mental disorder: Developmental follow-back of a prospective-longitudinal cohort. Arch. Gen. Psychiatry. 2003, 60, 709–717. [Google Scholar] [CrossRef]
- Bittner, A.; Egger, H.L.; Erkanli, A.; Costello, E.J.; Foley, D.L.; Angold, A. What do childhood anxiety disorders predict? J. Child. Psychol. Psychiatry 2007, 48, 1174–1183. [Google Scholar] [CrossRef]
- Woodward, L.J.; Fergusson, D.M. Life course outcomes of young people with anxiety disorders in adolescence. J. Am. Acad. Child. Adolesc. Psychiatry 2001, 40, 1086–1093. [Google Scholar] [CrossRef]
- Russell, E.; Koren, G.; Rieder, M.; Uum, S.V. Hair cortisol as a biological marker of chronic stress: Current status, future directions and unanswered questions. Psychoneuroendocrin 2012, 37, 589–601. [Google Scholar] [CrossRef]
- Chen, X.; Gelaye, B.; Velez, J.C.; Barbosa, C.; Pepper, M.; Andrade, A. Caregivers’ hair cortisol: A possible biomarker of chronic stress is associated with obesity measures among children with disabilities. BMC Pediatr. 2015, 15, 9. [Google Scholar] [CrossRef]
- McLachlan, K.; Rasmussen, C.; Oberlander, T.F.; Loock, C.; Pei, J.; Andrew, G.; Reynolds, J.; Weinberg, J. Dysregulation of the cortisol diurnal rhythm following prenatal alcohol exposure and early life adversity. Alcohol 2016, 53, 9–18. [Google Scholar] [CrossRef]
- Selye, J. Stressz Distressz Nélkül; Akadémiai Kiadó: Budapest, Hungary, 1976; ISBN 9630511061. [Google Scholar]
- Herman, J.P.; McKlveen, J.M.; Ghosal, S.; Kopp, B.; Wulsin, A.; Makinson, R.; Scheimann, J.; Myers, B. Regulation of the Hypothalamic-Pituitary-Adrenocortical Stress Response. Compr. Physiol. 2016, 6, 603–621. [Google Scholar] [CrossRef]
- Hinds, J.A.; Sanchez, E.R. The Role of the Hypothalamus–Pituitary–Adrenal (HPA) Axis in Test-Induced Anxiety: Assessments, Physiological Responses, and Molecular Details. Stresses 2022, 2, 146–155. [Google Scholar] [CrossRef]
- Sauve, B.; Koren, G.; Walsh, G. Measurement of cortisol in human hair as a biomarker of systemic exposure. Clin. Investig. Med. 2007, 30, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Wright, K.D.; Hickman, R.; Laudenslager, M.L. Hair Cortisol Analysis: A Promising Biomarker of HPA Activation in Older Adults. Gerontologist 2015, 55 (Suppl. S1), 140–145. [Google Scholar] [CrossRef]
- Gonzalez, D.; Jacobsen, D.; Ibar, C.; Pavan, C.; Monti, J.; Fernandez Machulsky, N.; Balbi, A.; Fritzler, A.; Jamardo, J.; Repetto, E.M.; et al. Hair Cortisol Measurement by an Automated Method. Sci. Rep. 2019, 9, 8213. [Google Scholar] [CrossRef] [PubMed]
- Vliegenthart, J.; Noppe, G.; van Rossum, E.F.C.; Koper, J.W.; Raat, H.; van den Akker, E.L.T. Socioeconomic status in children is associated with hair cortisol levels as a biological measure of chronic stress. Psychoneuroendocrin 2016, 65, 9–14. [Google Scholar] [CrossRef]
- Buse, J.; Rothe, J.; Uhlmann, A.; Bodmer, B.; Kirschbaum, C.; Hoekstra, P.J.; Dietrich, A.; Roessner, V. EMTICS collaborative group. Hair cortisol-a stress marker in children and adolescents with chronic tic disorders? A large European cross-sectional study. Eur. Child. Adolesc. Psychiatry 2022, 5, 771–779. [Google Scholar] [CrossRef]
- Rothe, J.; Buse, J.; Uhlmann, A.; Bodmer, B.; Kirschbaum, C.; Hoekstra, P.J.; Dietrich, A.; Roessner, V.; on behalf of the EMTICS Collaborative Group. Hair Cortisol and Perceived Stress—Predictors for the Onset of Tics? A European Longitudinal Study on High-Risk Children. Biomedicines 2023, 11, 1561. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Sipos, K.; Sipos, M.; Spielberger, C.D. A State-Trait Anxiety Inventory (STAI) magyar változata. In Mérei Ferenc, Szakács Ferenc. (szerk.): Pszichodiagnosztikai Vademecum I/2; Tankönyvkiadó: Budapest, Hungary, 1988; pp. 123–135. [Google Scholar]
- Lasky, P.; Buckwalter, K.; Whall, A.; Lederman, R.; Speer, J.; McLane, A.; King, J.; White, M. Developing an instrument for the assessment of family dynamics. Western J. Nurs. Res. 1985, 7, 40–57. [Google Scholar] [CrossRef]
- Inchley, J.; Currie, D.; Young, T.; Samdahl, O.; Torsheim, T.; Augustson, L.; Mathison, F.; Aleman-Diaz, A.; Molcho, M.; Weber, M. (Eds.) Growing up unequal: Gender and socioeconomic differences in young people’s health and well-being. In Health Behaviour in School Aged Children (HBSC) Study; WHO Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Personal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef]
- Wennig, R. Potential problems with the interpretation of hair analysis results. Forensic Sci. Intl. 2000, 107, 5–12. [Google Scholar] [CrossRef]
- Gow, R.; Koren, G.; Rieder, M.; Van Uum, S. Hair cortisol content in patients with adrenal insufficiency on hydrocortisone replacement therapy. Clin. Endocrinol. 2011, 74, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Greff, M.J.E.; Levine, J.M.; Abuzgaia, A.M.; Elzagallaai, A.A.; Rieder, M.J.; van Uum, S.H.M. Hair cortisol analysis: An update on methodological considerations and clinical applications. Clin. Biochem. 2019, 63, 1–9. [Google Scholar] [CrossRef]
- Lu, Q.; Pan, F.; Ren, L.; Xiao, J.; Tao, F. Sex differences in the association between internalizing symptoms and hair cortisol level among 10–12 year-old adolescents in China. PLoS ONE 2018, 9, e0192901. [Google Scholar] [CrossRef]
- Mollenhauer, Klaus: Szocializáció és iskolai eredmény. In Meleg Csilla (szerk): Iskola és Társadalom, I. szöveggyűjtemény; JPTE TIPT: Pécs, Hungary, 1996; Available online: http://mek.oszk.hu/01900/01944/01944.pdf (accessed on 12 June 2023).
- Mazzone, L.; Ducci, F.; Scoto, M.C.; Passaniti, E.; D’Arrigo, V.G.; Vitiello, B. The role of anxiety symptoms in school performance in a community sample of children and adolescents. BMC Public. Health 2007, 7, 347. [Google Scholar] [CrossRef] [PubMed]
- Murberg, T.A.; Bru, E. School-Related Stress and Psychosomatic Symptoms among Norwegian Adolescents. Sch. Psychol. Int. 2004, 25, 317–332. [Google Scholar] [CrossRef]


{kind=link}
| Measuring Tool | Number of Items | Cronbach’s Alpha |
|---|---|---|
| 20 | 0.92 |
| 20 | 0.88 |
| 20 | 0.93 |
| 20 | 0.92 |
| 11 | 0.85 |
| 11 | 0.91 |
| Clear Communication Scale | 4 | 0.79 |
| Multiple Social Perceived Support Scale | 4 | 0.89 |
| Genders | STAI-S Standard Values | STAI-T Standard Values |
|---|---|---|
| Mean (Standard Deviation) | ||
| Male | 38.40 (10.66) | 40.96 (7.78) |
| Female | 42.64 (10.79) | 45.37 (7.97) |
| STAI-S 1. | STAI-S 2. | STAI-T 1. | STAI-T 2 | Cortisol 1 | Cortisol 2 | |
|---|---|---|---|---|---|---|
| Mean (Standard Deviation) | ||||||
| Genders | ||||||
| Male | 38.45 (9.46) | 38.45 (9.46) | 38.45 (9.46) | 38.45 (9.46) | 38.45 (9.46) | 38.45 (9.46) |
| Female | 46.04 (11.32) | 46.04 (11.32) | 46.04 (11.32) | 46.04 (11.32) | 46.04 (11.32) | 46.04 (11.32) |
| t = −4.00; p < 0.01 | t = −4.00; p < 0.01 | t = −4.00; p < 0.01 | t = −4.00; p < 0.01 | t = −4.00; p < 0.01 | t = −4.00; p < 0.01 | |
| School type | ||||||
| High school | 44.78 (11.17) | 43.10 (11.07) | 48. 51 (9.14) | 46.07 (8.29) | 1.06 (0.85) | 2.64 (3.15) |
| Vocational high school | 41.93 (11.13) | 37.84 (12.01) | 44.30 (9.43) | 41.21 (11.49) | 2.03 (2.59) | 4.60 (3.72) |
| Vocational school | 37.79 (9.15) | 30.42 (6.05) | 39.00 (8.11) | 33.14 (4.77) | 3.50 (2.14) | 3.27 (1.85) |
| F = 3.44; p < 0.001 | F = 8.63; p < 0.001 | F = 8.60; p < 0.001 | F = 11.76; p < 0.001 | χ2 = 26.17; p < 0.001 | χ2 = 11.02; p = 0.004 | |
| Mother’s education level | ||||||
| Under degree | 39.70 (10.78) | 33.75 (10.85) | 41.36 (9.74) | 38.30 (9.07) | 3.54 (4.07) | 3.12 (3.12) |
| High school degree | 41.14 (11.54) | 39.42 (11.65) | 43.61 (9.69) | 41.57 (10.92) | 1.99 (0.91) | 3.65 (3.5) |
| University degree | 44.65 (10.31) | 39.66 (11.06) | 47.21 (8.53) | 42.29 (10.09) | 1.61 (0.80) | 3.75 (2.99) |
| F = 1.72; p = 0.18 | F = 1.96; p = 0.14 | F = 3.10; p = 0.49 | F = 0.96; p = 0.38 | χ2 = 7.18; p = 0.02 | χ2 = 1.14; p = 0.56 | |
| Complete sample | 41.43 (10.84) | 37.74 (11.47) | 43.75 (9.57) | 40.82 (10.35) | 2.35 (2.31) | 3.56 (3.30) |
| STAI-S II. Data Collection | STAI-T II. Data Collection | Cortisol 2. Measurement | |
|---|---|---|---|
| STAI-S I. data collection | t = 3.51; p = 0.001 | ||
| STAI-T I. data collection | t = 3.75; p < 0.001 | ||
| Cortisol 1. measurement | Z = −2.58; p = 0.01 |
| STAI-S 1. | STAI-S 2. | STAI-T 1. | STAI-T 2. | Cortisol 1 | Cortisol 2 | |
|---|---|---|---|---|---|---|
| Mean (Standard Deviation) | ||||||
| They are not distressing | 35.37 (8.10) | 29.56 (6.17) | 38.18 (9.67) | 33.87 (9.50) | 2.51 (1.74) | 7.83 (6.10) |
| They are a bit distressing | 39.10 (8.87) | 36.82 (11.70) | 42.36 (9.13) | 40.25 (10.61) | 2.62 (2.90) | 2.32 (1.90) |
| Quite distressing | 44.43 (10.90) | 41.80 (10.07) | 45.97 (8.25) | 43.11 (7.46) | 1.93 (1.79) | 2.92 (2.61) |
| Very distressing | 54.22 (13.77) | 48.00 (12.94) | 53.44 (9.13) | 53.16 (8.99) | 2.13 (0.87) | 2.68 (1.64) |
| F = 9.31; p < 0.001 | F = 6.54; p = 0.006 | F = 6.81; p < 0.001 | F = 6.88; p < 0.001 | χ2 = 4.72; p = 0.19 | χ2 = 8.93; p = 0.03 | |
| STAI-S 1. | STAI-S 2. | STAI-T 1. | STAI-T 2. | Cortisol 1 | Cortisol 2 | |
|---|---|---|---|---|---|---|
| Mean (Standard Deviation) | ||||||
| Almost daily | 52.86 (10.47) | 48.50 (.6.45) | 52.20 (6.42) | 54.50 (7.72) | 2.03 (0.76) | 1.39 (0.78) |
| Several times a week | 46.33 (9.99) | 46.50 (10.43) | 49.82 (8.10) | 51.71 (9.26) | 1.55 (0.59) | 4.57 (3.19) |
| Weekly | 39.48 (8.03) | 38.17 (7.47) | 41.92 (9.00) | 41.70 (8.98) | 2.39 (2.02) | 3.91 (4.74) |
| Per month | 35.40 (7.19) | 38.81 (12.76) | 38.06 (5.79) | 40.14 (6.66) | 2.61 (1.84) | 3.16 (3.53) |
| Rarely or never | 31.60 (8.99) | 29.68 (7.78) | 33.10 (5.19) | 32.68 (7.58) | 5.17 (6.19) | 2.14 (1.47) |
| F = 16.15; p < 0.001 | F = 8.06; p < 0.001 | F = 21.15; p < 0.001 | F = 16.37; p < 0.001 | χ2 = 12.71; p = 0.01 | χ2 = 5.41; p = 0.24 | |
| STAI-S 1. | STAI-S 2. | STAI-T 1. | STAI-T 2. | |
|---|---|---|---|---|
| Mean (Standard Deviation) | ||||
| Almost daily | 45.30 (12.15) | 51.50 (15.60) | 48.50 (9.65) | 56.50 (7.04) |
| Several times a week | 46.16 (11.41) | 41.76 (8.43) | 48.54 (9.54) | 45.05 (11.81) |
| Weekly | 41.13 (8.88) | 39.07 (10.75) | 42.89 (8.06) | 43.21 (8.83) |
| Per month | 34.40 (8.58) | 40.60 (11.82) | 39.31 (8.08) | 42.44 (7.32) |
| Rarely or never | 38.35 (9.28) | 29.85 (7.96) | 38.15 (8.00) | 33.11 (7.57) |
| F = 5.63; p < 0.001 | F = 7.19; p < 0.001 | F = 7.25; p < 0.001 | F = 10.09; p < 0.001 | |
| STAI-S 1. | STAI-S 2. | STAI-T 1. | STAI-T 2. | |
|---|---|---|---|---|
| Mean (Standard Deviation) | ||||
| Almost daily | 45.42 (12.08) | 41.11 (10.92) | 48.46 (8.45) | 45.38 (10.47) |
| Several times a week | 43.72 (10.26) | 43.26 (11.81) | 45.84 (9.25) | 46.40 (9.17) |
| Weekly | 40.96 (7.62) | 42.41 (10.70) | 42.28 (8.74) | 43.58 (10.01) |
| Per month | 31.31 (5.53) | 37.36 (14.10) | 34.37 (5.51) | 38.81 (9.17) |
| Rarely or never | 31.80 (12.07) | 29.34 (5.07) | 35.40 (7.47) | 33.50 (7.25) |
| F = 7.30; p < 0.001 | F = 6.95; p < 0.001 | F = 9.44; p < 0.001 | F = 7.26; p < 0.001 | |
| STAI-S 1. | STAI-S 2. | STAI-T 1. | STAI-T 2. | |
|---|---|---|---|---|
| Psychosomatic symptoms (aggregate variable) | r = 0.70 p < 0.001 | r = 0.55 p < 0.001 | r = 0.74 p < 0.001 | r = 0.66 p < 0.001 |
| STAI-S 1. | STAI-T 1. | Psychosomatic Symptoms (Aggregate Variable) | |
|---|---|---|---|
| Clear Communication Scale | r = −0.29; p = 0.001 | r = −0.22; p = 0.01 | r = −0.29; p = 0.001 |
| Multiple Social Perceived Support Scale | r = −0.32; p < 0.001 | r = −0.29; p = 0.001 | r = −0.32; p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stromájer, G.P.; Csima, M.; Iváncsik, R.; Varga, B.; Takács, K.; Stromájer-Rácz, T. Stress and Anxiety among High School Adolescents: Correlations between Physiological and Psychological Indicators in a Longitudinal Follow-Up Study. Children 2023, 10, 1548. https://doi.org/10.3390/children10091548
Stromájer GP, Csima M, Iváncsik R, Varga B, Takács K, Stromájer-Rácz T. Stress and Anxiety among High School Adolescents: Correlations between Physiological and Psychological Indicators in a Longitudinal Follow-Up Study. Children. 2023; 10(9):1548. https://doi.org/10.3390/children10091548
Chicago/Turabian StyleStromájer, Gábor Pál, Melinda Csima, Réka Iváncsik, Bernadett Varga, Krisztina Takács, and Tímea Stromájer-Rácz. 2023. "Stress and Anxiety among High School Adolescents: Correlations between Physiological and Psychological Indicators in a Longitudinal Follow-Up Study" Children 10, no. 9: 1548. https://doi.org/10.3390/children10091548