
Structural and Intermediary Social Determinants of Health and the Emotional and Behavioral Health of US Children
 , , , ,
, , , ,
Abstract
:1. Introduction
1.1. Child Emotional and Behavioral Health (EBH)
1.2. Factors Associated with Child EBH Problems
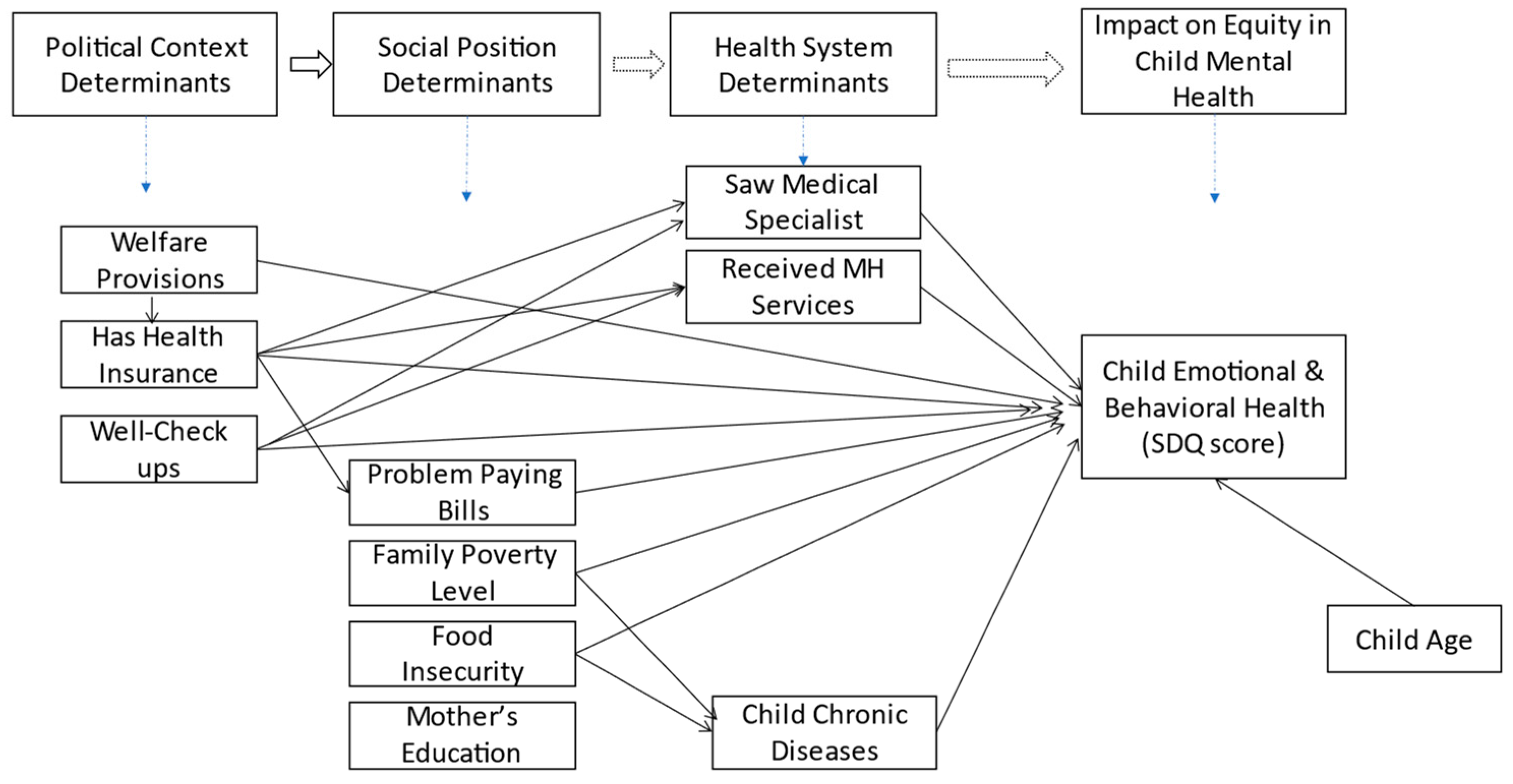
1.3. Social Determinants of Health (SDoH) Framework
1.4. Applying the SDoH to Child EBH
- How do structural social determinants of health from the macro context, such as availability of welfare services, health insurance, and use of child well-checkups, affect a child’s EBH problems?
- How are intermediary social determinants of health, such as household socioeconomic position (poverty level) and problems paying medical bills, associated with a child’s EBH problems?
- What are the direct and indirect mediating effects of intermediary factors such as access to mental health services, food insecurity, and chronic disease on child EBH?
2. Materials and Methods
2.1. Data
2.2. Measures
2.3. Independent Variables
2.4. Statistical Analysis
3. Results
3.1. Demographics
3.2. EBH Outcomes across Child Characteristics

{kind=link}
{kind=link}
| Variables | Overall | SDQ Score (Difficulties) % | t or χ2 | ||
|---|---|---|---|---|---|
| N (%) | No | Minor | Severe | ||
| Gender | |||||
| Male | 4669 (51%) | 76.8 | 18.8 | 4.4 | 19.4 *** |
| Female | 4536 (49%) | 80.3 | 16.4 | 3.3 | |
| Age (yrs.) | |||||
| 4–5 years | 1269 (14%) | 82.6 | 15.1 | 2.4 | 34.18 *** |
| 6–11 years | 3726 (40%) | 80.0 | 16.4 | 3.6 | |
| 12–17 years | 4210 (46%) | 76.1 | 19.4 | 4.5 | |
| Food Insecurity (FI) | |||||
| Food secure | 7091 (77%) | 81.4 | 15.1 | 3.1 | 218.2 *** |
| Marginal FI | 630 (6.8%) | 70.3 | 25.4 | 4.3 | |
| High FI | 1484 (16%) | 66.2 | 26.3 | 7.5 | |
| Insurance Type | |||||
| Any Private | 5000 (54%) | 81.6 | 15.5 | 2.9 | 79.7 *** |
| Public only/Military | 3621 (39%) | 74.0 | 20.8 | 5.2 | |
| Uninsured | 584 (6%) | 80.8 | 16.0 | 3.2 | |
| Family Poverty Level | |||||
| 0–99% FPL | 1913 (21%) | 72.6 | 21.5 | 5.9 | 86.04 *** |
| 100–199% FPL | 2147 (23%) | 77.0 | 18.2 | 4.7 | |
| 200–399% FPL | 2624 (29%) | 80.2 | 16.9 | 2.9 | |
| 400% FPL or above | 2521 (27%) | 83.6 | 14.9 | 2.5 | |
| # Chronic Conditions | |||||
| None | 54% | 86.9 | 11.5 | 1.6 | 768.7 *** |
| 1 condition | 23% | 78.6 | 18.2 | 3.4 | |
| 2 or more conditions | 22% | 58.1 | 32.0 | 9.9 | |
| Overall Health Status | |||||
| Excellent/Very good | 83% | 81.0 | 16.3 | 2.7 | 255.6 *** |
| Good | 15% | 68.2 | 23.2 | 8.5 | |
| Fair/Poor | 2% | 53.3 | 32.4 | 15.4 | |
| Received MH Care | |||||
| No care | 8.504 | 82.4 | 15.5 | 2.2 | 1.3 × 103 *** |
| Received Care | 731 | 34.1 | 42.8 | 23.1 | |
| Mother’s Education Level | |||||
| Some high school | 1527 | 77.8 | 18.1 | 4.1 | 61.7 *** |
| Some college | 3785 | 75.8 | 19.8 | 4.4 | |
| Associate Degree | 1179 | 77.5 | 17.4 | 5.1 | |
| Bachelor’s and more | 2744 | 83.2 | 14.5 | 2.3 | |
| Race/Ethnicity | |||||
| White/non-Hispanic | 4279 (46%) | ||||
| Black/non-Hispanic | 1243 (14%) | ||||
| Hispanic | 2672 (29%) | ||||
| Multiple/non-Hispanic | 1011 (11%) | ||||
3.3. Correlations
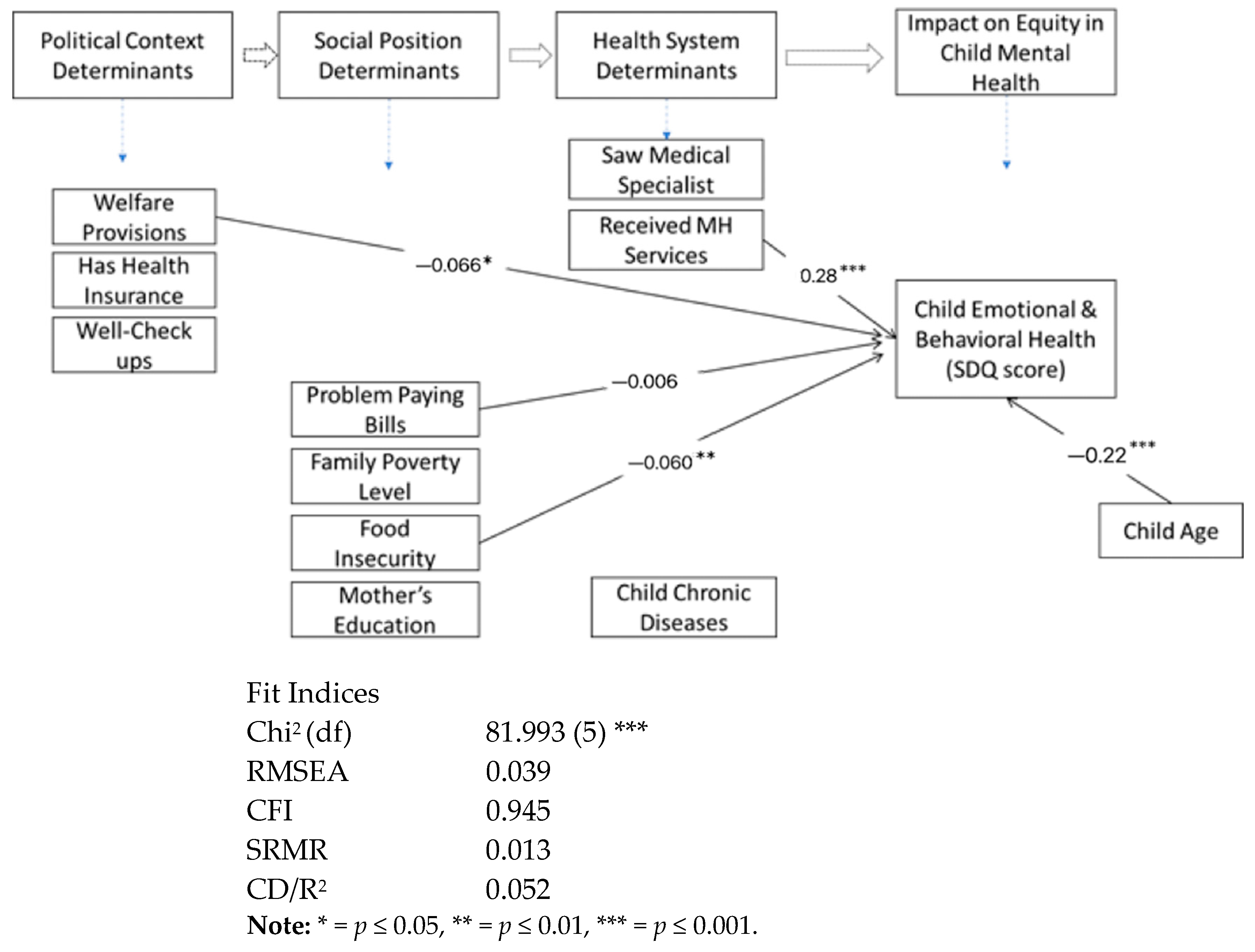
3.4. Path Coefficients
3.5. Total Effects

4. Discussion
5. Conclusions
5.1. Limitations
5.2. Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bernaras, E.; Jaureguizar, J.; Garaigordobil, M. Child and adolescent depression: A review of theories, evaluation instruments, prevention programs, and treatments. Front. Psychol. 2019, 10, 543. [Google Scholar] [CrossRef] [Green Version]
- Ogundele, M.O. Behavioural and emotional disorders in childhood: A brief overview for paediatricians. World J. Clin. Pediatr. 2018, 7, 9. [Google Scholar] [CrossRef] [PubMed]
- Braveman, P.; Egerter, S.; Williams, D.R. The social determinants of health: Coming of age. Annu. Rev. Public Health 2011, 32, 381–398. [Google Scholar] [CrossRef] [Green Version]
- Thompson, G. Meeting the needs of adolescent parents and their children. Paediatr. Child Health 2016, 21, 273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solar, O.; Irwin, A. A conceptual framework for action on the social determinants of health. In Social Determinants of Health Discussion Paper 2 (Policy and Practice); WHO Document Production Services: Geneva, Switzerland, 2010. [Google Scholar]
- Child and Adolescent Health Measurement Initiative. 2014 National Health Interview Survey—Child. SPSS Codebook, Version 1, 2016. Data Resource Center for Child and Adolescent Health. 2016. Available online: http://www.childhealthdata.org (accessed on 15 March 2017).
- Bitsko, R.H.; Claussen, A.H.; Lichstein, J.; Black, L.I.; Jones, S.E.; Danielson, M.L.; Hoenig, J.M.; Jack, S.P.D.; Brody, D.J.; Gyawali, S.; et al. Mental health surveillance among children—United States, 2013–2019. MMWR Suppl. 2022, 71, 1. [Google Scholar] [CrossRef] [PubMed]
- Braveman, P.; Barclay, C. Health disparities beginning in childhood: A life-course perspective. Pediatrics 2009, 124, S163–S175. [Google Scholar] [CrossRef] [Green Version]
- Lebrun-Harris, L.A.; Ghandour, R.M.; Kogan, M.D.; Warren, M.D. Five-year trends in US children’s health and well-being, 2016–2020. JAMA Pediatr. 2022, 176, e220056. [Google Scholar] [CrossRef]
- Perou, R.; Bitsko, R.H.; Blumberg, S.J.; Pastor, P.; Ghandour, R.M.; Gfroerer, J.C.; Hedden, S.L.; Crosby, A.E.; Visser, S.N.; Schieve, L.A.; et al. Centers for Disease Control and Prevention (CDC) Mental health surveillance among children—United States, 2005–2011. MMWR Suppl. 2013, 62, 1–35. [Google Scholar]
- Cree, R.A.; Bitsko, R.H.; Robinson, L.R.; Holbrook, J.R.; Danielson, M.L.; Smith, C.; Kaminski, J.W.; Kenney, M.K.; Peacock, G. Health care, family, and community factors associated with mental, behavioral, and developmental disorders and poverty among children Aged 2–8 Years—United States, 2016. MMWR. Morb. Mortal. Wkly. Rep. 2018, 67, 1377–1383. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Data and Statistics on Children’s Mental Health. Children’s Mental Health 1–6. 2022. Available online: https://www.cdc.gov/childrensmentalhealth/data.html (accessed on 17 May 2022).
- Kessler, R.C.; Amminger, G.P.; Aguilar-Gaxiola, S.; Alonso, J.; Lee, S.; Üstün, T.B. Age of onset of mental disorders: A review of recent literature. Curr. Opin. Psychiatry 2007, 20, 359–364. [Google Scholar] [CrossRef]
- Kessler, R.C.; Angermeyer, M.; Anthony, J.C.; De Graaf, R.; Demyttenaere, K.; Gasquet, I.; De Girolamo, G.; Gluzman, S.; Gureje, O.; Haro, M.; et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry 2007, 6, 168–176. [Google Scholar] [PubMed]
- Suryavanshi, M.S.; Yang, Y. Clinical and economic burden of mental disorders among children with chronic physical conditions, United States, 2008–2013. Prev. Chronic Dis. 2016, 13, 150535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Achilles, G.M.; McLaughlin, M.J.; Croninger, R.G. Sociocultural correlates of disciplinary exclusion among students with emotional, behavioral, and learning disabilities in the SEELS national dataset. J. Emot. Behav. Disord. 2007, 15, 33–45. [Google Scholar] [CrossRef]
- Kim, Y.; Lee, H.; Park, A. Patterns of adverse childhood experiences and depressive symptoms: Self-esteem as a mediating mechanism. Soc. Psychiatry Psychiatr. Epidemiol. 2022, 57, 331–341. [Google Scholar] [CrossRef]
- Sonu, S.; Post, S.; Feinglass, J. Adverse childhood experiences and the onset of chronic disease in young adulthood. Prev. Med. 2019, 123, 163–170. [Google Scholar] [CrossRef]
- Leis, J.A.; Heron, J.; Stuart, E.A.; Mendelson, T. Associations between maternal mental health and child emotional and behavioral problems: Does prenatal mental health matter? J. Abnorm. Child Psychol. 2014, 42, 161–171. [Google Scholar] [CrossRef]
- Monk, C.; Georgieff, M.K.; Osterholm, E.A. Maternal prenatal distress and poor nutrition-mutually influencing risk factors affecting infant neurocognitive development. J. Child Psychol. Psychiatry 2013, 54, 115–130. [Google Scholar] [CrossRef]
- Molenaar, D.; Middeldorp, C.; van Beijsterveldt, T.; Boomsma, D.I. Analysis of behavioral and emotional problems in children highlights the role of genotype X environment interaction. Child Dev. 2015, 86, 1999–2016. [Google Scholar] [CrossRef]
- Goodman, S.; Gotlib, I.H. Risk for psychopathology in the children of depressed mothers: A developmental model for understanding mechanisms of transmission. Psychol. Rev. 1999, 106, 458–490. [Google Scholar] [CrossRef]
- Zandi, P.P.; Wilcox, H.C.; Dong, L.; Chon, S.; Maher, B. Genes as a source of risk for mental disorders. In Public Mental Health; Eaton, W.W., Ed.; Oxford University Press: New York, NY, USA, 2012; pp. 201–244. [Google Scholar]
- Rijlaarsdam, J.; Stevens, G.W.J.M.; van der Ende, J.; Hofman, A.; Jaddoe, V.W.; Mackenbach, J.P.; Verhulst, F.C.; Tiemeier, H. Economic disadvantage and young children’s emotional and behavioral problems: Mechanisms of risk. J. Abnorm. Child Psychol. 2013, 41, 125–137. [Google Scholar] [CrossRef] [Green Version]
- Leung, B.M.; Wandler, C.; Pringsheim, T.; Santana, M.J. Working with parents of children with complex mental health issues to improve care: A qualitative inquiry. J. Child Health Care 2021, 26, 548–567. [Google Scholar] [CrossRef]
- Brassett-Harknett, A.; Butler, N. Attention-deficit/hyperactivity disorder: An overview of the etiology and a review of the literature relating to the correlates and life course outcomes for men and women. Clin. Psychol. Rev. 2007, 27, 188–210. [Google Scholar] [CrossRef]
- Food Research & Action Center. The Impact of Poverty, Food Insecurity, and Poor Nutrition on Health and Well-Being. 2017. Available online: http://www.frac.org (accessed on 28 April 2019).
- Substance Abuse and Mental Health Services Administration. Improving Life Outcomes for Children with History of Mental Health Challenges and Trauma. SAMHSA—Substance Abuse and Mental Health Services Administration. 2018. Available online: https://www.samhsa.gov/newsroom/press-announcements/201805090400 (accessed on 28 April 2019).
- Bharmal, N.; Derose, K.P.; Felician, M.; Weden, M.M. Understanding the Upstream Social Determinants of Health; RAND: Santa Monica, CA, USA, 2015. [Google Scholar]
- Mikkonen, J.; Raphael, D. Social Determinants of Health: The Canadian Facts; York University School of Health Policy and Management: Toronto, ON, Canada, 2010. [Google Scholar]
- Robert Wood Johnson Foundation. A New Way to Talk about the Social Determinants of Health. 2014. Available online: https://societyforhealthpsychology.org/wp-content/uploads/2016/08/rwjf63023.pdf (accessed on 15 August 2016).
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the social determinants of health. Adolescent Health 2. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef]
- Goodman, R. The strengths and difficulties questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Goodman, A.; Goodman, R. Strengths and difficulties questionnaire as a dimensional measure of child mental health. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 400–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theunissen, M.H.; Vogels, A.G.C.; de Wolff, M.S.; Reijneveld, S.M.D. Characteristics of the strengths and difficulties questionnaire in preschool children. Pediatrics 2013, 131, e446–e454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez, D.; Sribney, W.M.; Rodríguez, M.A. Perceived discrimination and self-reported quality of care among Latinos in the United States. J. Gen. Intern. Med. 2009, 24, 548–554. [Google Scholar] [CrossRef] [Green Version]
- StataCorp. Stata Structural Equation Modeling Reference Manual: Release 15; StataCorp: College Station, TX, USA, 2017. [Google Scholar]
- Boomsma, A. Reporting analyses of covariance structures. Struct. Equ. Model. A Multidiscip. J. 2009, 7, 461–483. [Google Scholar] [CrossRef]
- Kline, R.B. Mean structures and latent growth models. In Principles and Practice of Structural Equation Modeling; The Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Durlak, J.A. How to select, calculate, and interpret effect sizes. J. Pediatr. Psychol. 2009, 34, 917–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention (CDC). Youth Risk Behavior Survey: Data Summary & Trends Report 2011–2021; Centers for Disease Control and Prevention (CDC): Atlanta, GA, USA, 2022. [Google Scholar]
- Liverpool, S.; Edbrooke-Childs, J. Associations between child mental health, carer worry and help-seeking. J. Child Health Care 2021, 26, 355–366. [Google Scholar] [CrossRef]
- Linsell, L.; Johnson, S.; Wolke, D.; Morris, J.; Kurinczuk, J.J.; Marlow, N. Trajectories of behavior, attention, social and emotional problems from childhood to early adulthood following extremely preterm birth: A prospective cohort study. Eur. Child Adolesc. Psychiatry 2019, 28, 531–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gelaye, B.; Rondon, M.; Araya, R.; Williams, M.A.; Author, C. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries HHS Public Access. Lancet Psychiatry 2016, 3, 973–982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerman, A.; Garman, E.; Avendano-Pabon, M.; Araya, R.; Evans-Lacko, S.; McDaid, D.; Park, A.L.; Hessel, P.; Diaz, Y.; Matijasevich, A.; et al. The impact of cash transfers on mental health in children and young people in low-income and middle-income countries: A systematic review and meta-analysis. BMJ Glob. Health 2021, 6, e004661. [Google Scholar] [CrossRef] [PubMed]
- Zaneva, M.; Guzman-Holst, C.; Reeves, A.; Bowes, L. The Impact of Monetary Poverty Alleviation Programs on Children’s and Adolescents’ Mental Health: A Systematic Review and Meta-Analysis Across Low-, Middle-, and High-Income Countries. J. Adolesc. Health 2022, 71, 147–156. [Google Scholar] [CrossRef]
- Alegría, M.; NeMoyer, A.; Falgàs Bagué, I.; Wang, Y.; Alvarez, K. Social determinants of mental health: Where we are and where we need to go. Curr. Psychiatry Rep. 2018, 20, 95. [Google Scholar] [CrossRef]
- Chen, K.L.; Miake-Lye, I.M.; Begashaw, M.M.; Zimmerman, F.J.; Larkin, J.; McGrath, E.L.; Shekelle, P.G. Association of promoting housing affordability and stability with improved health outcomes: A systematic review. JAMA Netw. Open 2022, 5, E2239860. [Google Scholar] [CrossRef]
- Branas, C.C.; South, E.; Kondo, M.C.; Hohl, B.C.; Bourgois, P.; Wiebe, D.J.; MacDonald, J.M. Citywide cluster randomized trial to restore blighted vacant land and its effects on violence, crimse, and fear. Proc. Natl. Acad. Sci. USA 2018, 115, 2946–2951. [Google Scholar] [CrossRef] [Green Version]
- Fagan, A.A.; Fagan, A.A.; Hawkins, J.D.; Catalano, R.F.; Farrington, D.P. The future of CTC and community-based prevention. In Communities That Care: Building Community Engagement and Capacity to Prevent Youth Behavior Problems; Oxford University Press: Oxford, UK, 2018. [Google Scholar] [CrossRef]
- Hodgkinson, S.; Godoy, L.; Beers, L.S.; Lewin, A. Improving mental health access for low-income children and families in the primary care setting. Pediatrics 2017, 139, e20151175. [Google Scholar] [CrossRef] [Green Version]

| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Macro/Policy factors | |||||||||||||
| 1. Well Visits | 1 | ||||||||||||
| 2. Insurance type | 0.11 c | 1 | |||||||||||
| 3. Use of welfare | −0.03 b | 0.34 c | 1 | ||||||||||
| Family SES factors | |||||||||||||
| 4. Mom education | 0.11 c | 0.43 c | 0.30 c | 1 | |||||||||
| 5. Problem med. bills | 0.03 b | 0.17 c | 0.13 c | 0.13 c | 1 | ||||||||
| 6. Family Poverty | −0.76 c | −0.56 c | −0.52 c | −0.55 c | −0.20 c | 1 | |||||||
| 7. Food Insecurity | 0.03 b | 0.27 c | 0.29 c | 0.26 c | 0.27 c | −0.39 c | 1 | ||||||
| Health System Factors | |||||||||||||
| 8. Rcvd Mental care | −0.04 c | 0.0 | 0.07 c | −0.03 a | 0.07 c | −0.02 | 0.07 c | 1 | |||||
| 9. Rcvd Specialized care | −0.07 c | −0.05 c | −0.02 | −0.07 c | 0.04 c | 0.06 | 0.01 | 0.14 c | 1 | ||||
| Child Health Factors | |||||||||||||
| 10. Overall Health | 0.03 a | 0.16 c | 0.13 c | 0.18 c | 0.08 c | −0.21 c | 0.17 c | 0.12 c | 0.11 c | 1 | |||
| 11. Chronic Conditions | −0.05 c | 0.01 | 0.09 c | −0.03 b | 0.14 | −0.02 | 0.19 c | 0.26 c | 0.22 c | 0.18 c | 1 | ||
| Child Demographics | |||||||||||||
| 12. Age | −0.10 c | 0.06 c | 0.11 c | 0.01 | 0.02 a | −0.08 c | −0.01 | −0.07 c | −0.02 a | −0.03 b | −0.05 c | 1 | |
| 13. Ethnicity | 0.02 a | 0.23 c | 0.12 c | 0.23 c | 0.13 | −0.25 c | 0.12 c | −0.05 c | −0.07 c | 0.10 c | −0.07 c | 0.03 b | 1 |
| 14. Gender | 0.02 | 0.02 | 0.01 | 0.01 | 0.00 | −0.01 | 0.01 | −0.04 c | −0.01 | −0.03 b | −0.07 c | 0.01 | 0.02 |
| SDQ Score (Child EBH Symptoms) | (On Figure 2) | |||
|---|---|---|---|---|
| Variables | Coeff. (S.E.) | Standardized Coeff. (S.E.) | Indirect Effects | Total Effects |
| Macro/Policy factors | ||||
| 1. Well Visits | 0.20 (0.039) *** | 0.05 (0.009) *** | - | - |
| 2. Insurance type | −0.01 (0.031) | −0.00 (0.011) | - | - |
| 3. Use of welfare | −0.07 (0.033) * | −0.027 (0.011) * | −0.024 (−0.005) * | −0.066 (−0.024) * |
| Family SES factors | ||||
| 4. Mom education | 0.05 (0.18) ** | 0.03 (0.011) ** | - | - |
| 5. Problem medical bills | 0.14 (0.025) *** | 0.06 (0.010) *** | −0.006 (0.002) | −0.006 (0.002) |
| 6. Family Poverty Level | −0.01 (0.021) | −0.01 (0.01) | −0.002 (−0.001) | −0.004 (−0.003) |
| 7. Food Insecurity | 0.06 (0.020) *** | 0.033 (0.010) *** | −0.003 (−0.001) | 0.060 (0.032) ** |
| Health System Factors | ||||
| 8. Rcvd Mental care | 0.30 (0.05) *** | 0.059 (0.009) *** | −0.024 (−0.005) | 0.28 (0.05) *** |
| 9. Rcvd Specialized care | 0.05 (0.047) | 0.01 (0.010) *** | - | - |
| Child Health Factors | ||||
| 10. Overall Health | 0.31 (0.038) *** | 0.08 (0.010) *** | - | - |
| 11. Chronic Conditions | −0.033 (0.021) *** | −0.019 (0.010) *** | - | −0.031 (−0.019) |
| Child Demographics | ||||
| 12. Age | 0.22 (0.020) *** | 0.11 (0.009) ** | −0.001 (−0.001) | −0.22 (0.11) *** |
| 13. Ethnicity | −0.08 (0.015) *** | −0.05 (0.009) *** | - | - |
| 14. Gender | −0.10 (0.031) *** | −0.03 (0.009) ** | - | - |
| Error terms | ||||
| e.sdq score | 1.98 (0.027) | 0.98 (0.002) | ||
| e.chronic diseases | 0.60 (0.008) | 0.90 (0.005) | ||
| e.mental health care | 0.08 (0.001) | 0.99 (0.002) | ||
| Fit Indices | ||||
| Chi2 (df) | 81.993 (5) *** | |||
| RMSEA | 0.039 | |||
| CFI | 0.945 | |||
| SRMR | 0.013 | |||
| CD/R2 | 0.052 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Enelamah, N.V.; Lombe, M.; Yu, M.; Villodas, M.L.; Foell, A.; Newransky, C.; Smith, L.C.; Nebbitt, V. Structural and Intermediary Social Determinants of Health and the Emotional and Behavioral Health of US Children. Children 2023, 10, 1100. https://doi.org/10.3390/children10071100
Enelamah NV, Lombe M, Yu M, Villodas ML, Foell A, Newransky C, Smith LC, Nebbitt V. Structural and Intermediary Social Determinants of Health and the Emotional and Behavioral Health of US Children. Children. 2023; 10(7):1100. https://doi.org/10.3390/children10071100
Chicago/Turabian StyleEnelamah, Ngozi V., Margaret Lombe, Mansoo Yu, Melissa L. Villodas, Andrew Foell, Chrisann Newransky, Lisa C. Smith, and Von Nebbitt. 2023. "Structural and Intermediary Social Determinants of Health and the Emotional and Behavioral Health of US Children" Children 10, no. 7: 1100. https://doi.org/10.3390/children10071100