

Individualized Goal Setting for Pediatric Intensive Care Unit-Based Rehabilitation Using the Canadian Occupational Performance Measure

Abstract
:1. Introduction
2. Materials and Methods
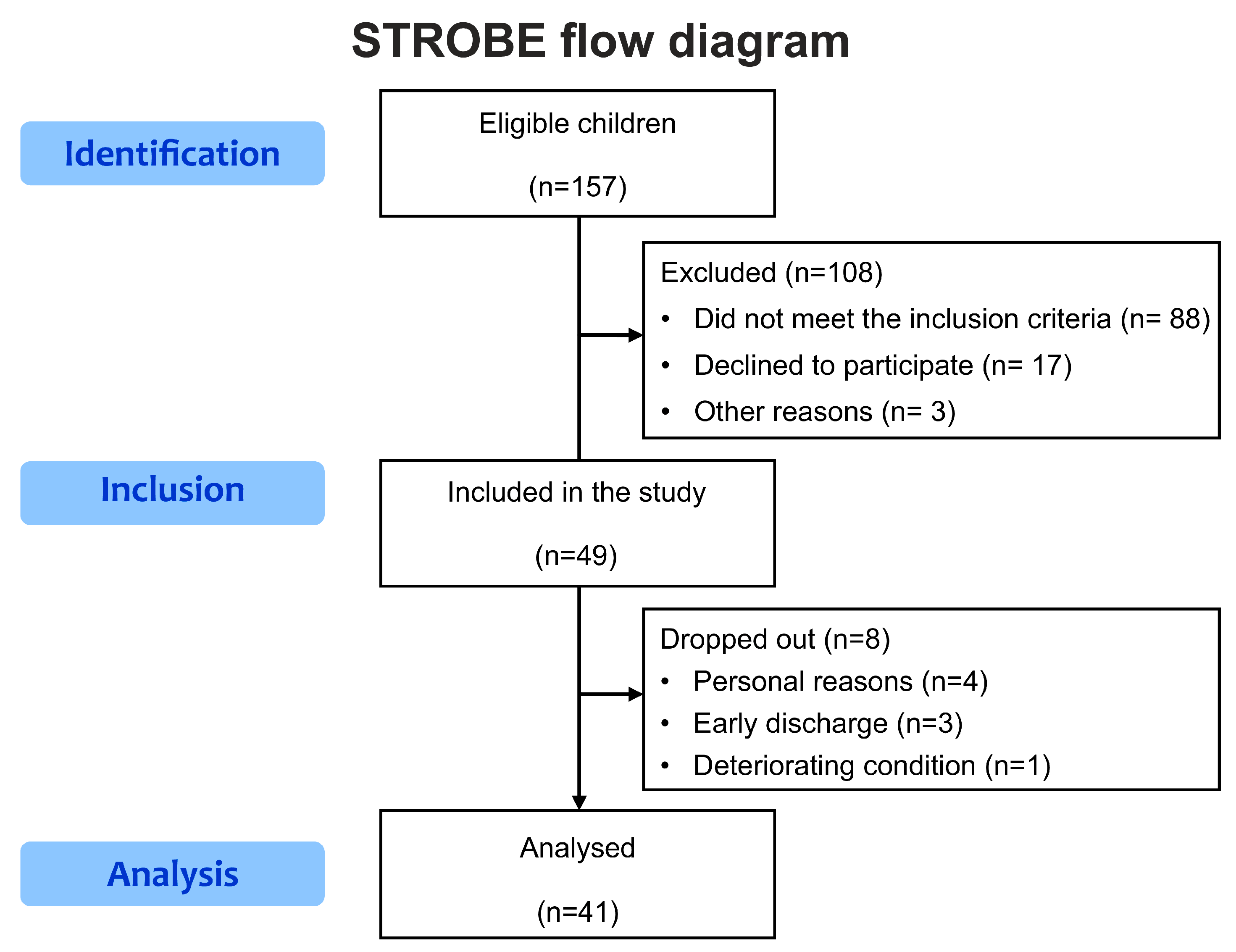
2.1. Study Design and Population
2.2. Caregivers’ Perspectives on Their Children’s Functional Goals
2.3. Feasibility Measurements
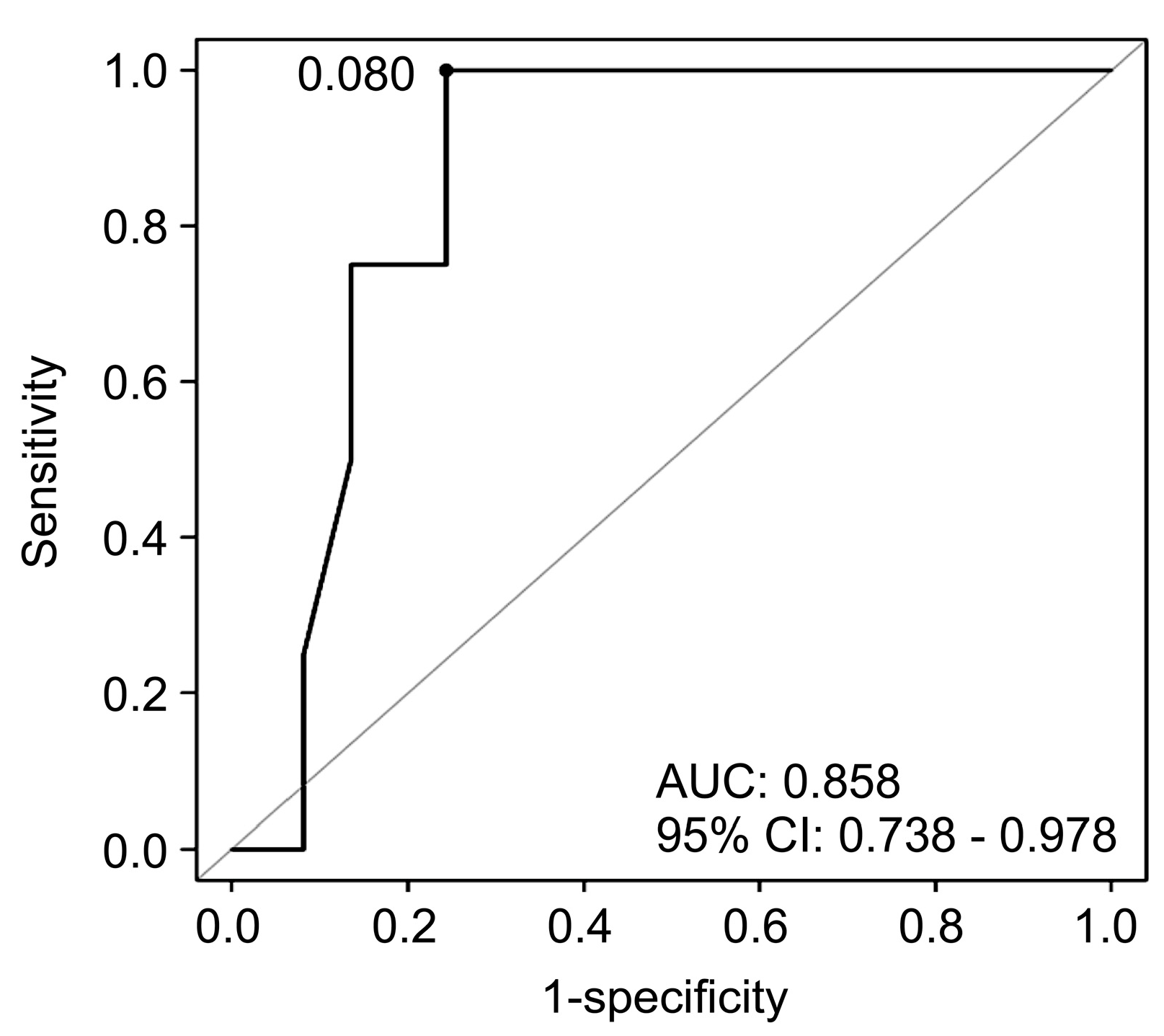
2.4. Clinical Indicators Predicting the Generation of Occupational Performance Goal List
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bloom, B.; Cohen, R.A.; Freeman, G. Summary health statistics for U.S. children: National Health Interview Survey, 2009. Vital Health Stat. 2010, 247, 1–82. [Google Scholar]
- Knoester, H.; Bronner, M.B.; Bos, A.P.; Grootenhuis, M.A. Quality of life in children three and nine months after discharge from a paediatric intensive care unit: A prospective cohort study. Health Qual Life Outcomes 2008, 6, 21. [Google Scholar] [CrossRef]
- Curran, A.L.; Sharples, P.M.; White, C.; Knapp, M. Time costs of caring for children with severe disabilities compared with caring for children without disabilities. Dev. Med. Child Neurol. 2001, 43, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Hogan, D.P.; Rogers, M.L.; Msall, M.E. Functional limitations and key indicators of well-being in children with disability. Arch. Pediatr. Adolesc. Med. 2000, 154, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Pollack, M.M.; Holubkov, R.; Funai, T.; Clark, A.; Berger, J.T.; Meert, K.; Newth, C.J.; Shanley, T.; Moler, F.; Carcillo, J.; et al. Pediatric intensive care outcomes: Development of new morbidities during pediatric critical care. Pediatr. Crit. Care Med. 2014, 15, 821–827. [Google Scholar] [CrossRef]
- Au, A.K.; Carcillo, J.A.; Clark, R.S.; Bell, M.J. Brain injuries and neurological system failure are the most common proximate causes of death in children admitted to a pediatric intensive care unit. Pediatr. Crit. Care Med. 2011, 12, 566–571. [Google Scholar] [CrossRef]
- Hopkins, R.O.; Choong, K.; Zebuhr, C.A.; Kudchadkar, S.R. Transforming PICU culture to facilitate early rehabilitation. J. Pediatr. Intensive Care 2015, 4, 204–211. [Google Scholar] [CrossRef]
- Wieczorek, B.; Burke, C.; Al-Harbi, A.; Kudchadkar, S.R. Early mobilization in the pediatric intensive care unit: A systematic review. J. Pediatr. Intensive Care 2015, 2015, 129–170. [Google Scholar] [CrossRef]
- Speyer, E.; Vuillemin, A.; Herbinet, A.; Chastagner, P.; Briançon, S. Effect of adapted physical activity on health-related quality of life among hospitalized children and adolescents (the ACTIV’HOP randomized controlled trial): Design and methods. Contemp. Clin. Trials 2010, 31, 165–171. [Google Scholar] [CrossRef]
- Baum, C.; Christiansen, C.; Bass, J. The person-environment-occupation-performance (PEOP) model. In Occupational Therapy: Performance, Participation and Well-Being, 4th ed.; Christiansen, C.H., Baum, C.M., Bass, J.D., Eds.; Slack Incorporated: West Deptford, NJ, USA, 2015; pp. 49–56. [Google Scholar]
- Costigan, F.A.; Duffett, M.; Harris, J.E.; Baptiste, S.; Kho, M.E. Occupational therapy in the ICU: A scoping review of 221 documents. Crit. Care Med. 2019, 47, e1014–e1021. [Google Scholar] [CrossRef]
- Law, M.C.; Baptiste, S.; Carswell, A.; McColl, M.A.; Polatajko, H.; Pollock, N. Canadian Occupational Performance Measure, 3rd ed.; CAOT Publications ACE: Ottawa, ON, Canada, 1998. [Google Scholar]
- Cusick, A.; Lannin, N.A.; Lowe, K. Adapting the Canadian Occupational Performance Measure for use in a paediatric clinical trial. Disabil. Rehabil. 2007, 29, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Lewin, S.A.; Skea, Z.C.; Entwistle, V.; Zwarenstein, M.; Dick, J. Interventions for providers to promote a patient-centred approach in clinical consultations. Cochrane Database Syst. Rev. 2001, CD003267. [Google Scholar] [CrossRef]
- Stewart, M. Towards a global definition of patient centred care. BMJ 2001, 322, 444–445. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Baptiste, S.; Mills, J. Client-centred practice: What does it mean and does it make a difference? Can. J. Occup. Ther. 1995, 62, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Haley, S.M.; Coster, W.J.; Dumas, H.M.; Fragala-Pinkham, M.A.; Kramer, J.; Ni, P.; Tian, F.; Kao, Y.C.; Moed, R.; Ludlow, L.H. Accuracy and precision of the Pediatric Evaluation of Disability Inventory computer-adaptive tests (PEDI-CAT). Dev. Med. Child. Neurol. 2011, 53, 1100–1106. [Google Scholar] [CrossRef]
- Haley, S.M.; Coster, W.J.; Dumas, H.M.; Fragala-Pinkham, M.A.; Moed, R.; Kramer, J.M.; Ludlow, L. PEDI-CAT, version 1.4.0; Development, Standardization and Administration Manual; Trustees of Boston University: Boston, MA, USA, 2015. [Google Scholar]
- Julian, L.J. Measures of anxiety: State–Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (HADS-A). Arthritis Care Res. 2011, 63 (Suppl. S11), S467–S472. [Google Scholar] [CrossRef]
- Kim, J. A study based on the standardization of the STAI for Korea. New Med. J. 1978, 21, 69–75. [Google Scholar]
- Pollack, M.M.; Patel, K.M.; Ruttimann, U.E. PRISM III: An updated Pediatric Risk of Mortality score. Crit. Care Med. 1996, 24, 743–752. [Google Scholar] [CrossRef]
- Pollack, M.M.; Holubkov, R.; Glass, P.; Dean, J.M.; Meert, K.L.; Zimmerman, J.; Anand, K.J.; Carcillo, J.; Newth, C.J.; Harrison, R.; et al. Functional Status Scale: New pediatric outcome measure. Pediatrics 2009, 124, e18–e28. [Google Scholar] [CrossRef]
- Turner-Stokes, L. Goal Attainment Scaling (GAS) in rehabilitation: A practical guide. Clin. Rehabil. 2009, 23, 362–370. [Google Scholar] [CrossRef]
- Reuben, D.B.; Tinetti, M.E. Goal-oriented patient care—An alternative health outcomes paradigm. N. Engl. J. Med. 2012, 366, 777–779. [Google Scholar] [CrossRef] [PubMed]
- Choong, K.; Fraser, D.; Al-Harbi, S.; Borham, A.; Cameron, J.; Cameron, S.; Cheng, J.; Clark, H.; Doherty, T.; Fayed, N.; et al. Functional recovery in critically ill children, the “WeeCover” multicenter study. Pediatr. Crit. Care Med. 2018, 19, 145–154. [Google Scholar] [CrossRef]
- Gaudry, S.; Messika, J.; Ricard, J.D.; Guillo, S.; Pasquet, B.; Dubief, E.; Boukertouta, T.; Dreyfuss, D.; Tubach, F. Patient-important outcomes in randomized controlled trials in critically ill patients: A systematic review. Ann. Intensive Care 2017, 7, 28. [Google Scholar] [CrossRef]
- Ong, C.; Lee, J.H.; Leow, M.K.; Puthucheary, Z.A. Functional outcomes and physical impairments in pediatric critical care survivors: A scoping review. Pediatr. Crit. Care Med. 2016, 17, e247–e259. [Google Scholar] [CrossRef]
- Boyer, G.; Hachey, R.; Mercier, C. Perceptions of occupational performance and subjective quality of life in persons with severe mental illness. Occup. Ther. Ment. Health 2000, 15, 1–15. [Google Scholar] [CrossRef]
- American Occupational Therapy Association. Occupational Therapy Practice Framework: Domain and Process (3rd Edition). Am. J. Occup. Ther. 2014, 68, S1–S48. [Google Scholar] [CrossRef]
- Estes, J.; Pierce, D.E. Pediatric therapists’ perspectives on occupation-based practice. Scand J. Occup. Ther. 2012, 19, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rey, R.; Alonso-Tapia, J. Development of a screening measure of stress for parents of children hospitalised in a Paediatric Intensive Care Unit. Aust. Crit. Care. 2016, 29, 151–157. [Google Scholar] [CrossRef]
- Burns, J.P.; Mello, M.M.; Studdert, D.M.; Puopolo, A.L.; Truog, R.D.; Brennan, T.A. Results of a clinical trial on care improvement for the critically ill. Crit. Care Med. 2003, 31, 2107–2117. [Google Scholar] [CrossRef]
- Curtis, J.R.; Engelberg, R.A.; Wenrich, M.D.; Shannon, S.E.; Treece, P.D.; Rubenfeld, G.D. Missed opportunities during family conferences about end-of-life care in the intensive care unit. Am. J. Respir. Crit. Care Med. 2005, 171, 844–849. [Google Scholar] [CrossRef]
- Tulsky, J.A. Interventions to enhance communication among patients, providers, and families. J. Palliat. Med. 2005, 8 (Suppl. S1), S95–S102. [Google Scholar] [CrossRef] [PubMed]
- Hays, R.M.; Valentine, J.; Haynes, G.; Geyer, J.R.; Villareale, N.; McKinstry, B.; Varni, J.W.; Churchill, S.S. The Seattle Pediatric Palliative Care Project: Effects on family satisfaction and health-related quality of life. J. Palliat. Med. 2006, 9, 716–728. [Google Scholar] [CrossRef] [PubMed]
- DeLambo, D.; Chung, W.; Huang, W. Stress and age: A comparison of Asian American and non-Asian American parents of children with developmental disabilities. J. Dev. Phys. Disabil. 2011, 23, 129–141. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | n (%) | |
|---|---|---|
| Age, mean (SD), y | 8.31 (5.87) | |
| Sex, n (%) | Boys | 22 (53.66) |
| Girls | 19 (46.34) | |
| STAI-X-1, mean (SD) | 57.93 (10.02) | |
| FSS, mean (SD) | 11.51 (6.43) | |
| PEDI-CAT, mean (SD) | Daily activities | 54.93 (11.12) |
| Mobility | 60.54 (12.06) | |
| Cognitive/social | 61.39 (12.47) | |
| Responsibility | 44.56 (14.50) | |
| PRISM III, mean (SD) | 8.66 (7.55) | |
| Ventilator use, n (%) | Yes | 24 (58.54) |
| No | 17 (41.46) | |
| Previous PICU admission, n (%) | Yes | 13 (31.71) |
| No | 28 (68.29) | |
| Reasons for admission, n (%) | Cardiovascular | 6 (14.63) |
| Hematology and oncology | 7 (17.07) | |
| Neurologic | 8 (19.51) | |
| Respiratory | 16 (39.02) | |
| Sepsis | 4 (9.76) | |
| COPM, mean (SD) | Administration time (min) | 15.12 (3.68) |
| Difficulty | 4.49 (2.55) | |
| Goal Domains | n/Total (%) | Importance, Mean (SD) |
|---|---|---|
| Occupational performance goal lists | ||
| Functional mobility | 55/190 (28.9) | 6.76 (1.24) |
| Actively repositioning in bed | 26/55 (47.4) | 7.23 (1.19) |
| Ambulation | 11/55 (20.0) | 6.54 (1.40) |
| Sitting whilst leaning back | 7/55 (12.7) | 6.29 (1.18) |
| Sitting on the edge of the bed | 7/55 (12.7) | 6.00 (1.14) |
| Transfer | 2/55 (3.6) | 7.00 (0) |
| Reaching | 2/55 (3.6) | 6.00 (0) |
| Personal care | 29/190 (15.2) | 6.24 (1.42) |
| Communication | 15/29 (51.7) | 6.20 (1.52) |
| Dressing | 8/29 (27.6) | 6.00 (1.43) |
| Personal hygiene | 6/29 (20.7) | 6.33 (1.00) |
| Quiet recreation | 3/190 (1.6) | 3.67 (0.44) |
| Using electronic devices | 3/3 (100.0) | 3.67 (0.44) |
| Additional concerns (Personal factors) | ||
| Physiological factors | 68/190 (35.8) | 7.01 (1.52) |
| Respiratory function | 18/68 (26.6) | 8.56 (1.11) |
| Consciousness | 17/68 (25.0) | 7.06 (1.25) |
| Intubation, IV nutrition | 17/68 (25.0) | 6.11 (1.79) |
| Urinary catheterization | 10/68 (14.8) | 6.20 (1.40) |
| Sensory | 3/68 (4.4) | 5.67 (0.44) |
| Body temperature | 1/68 (1.4) | 7.00 (0) |
| Cough | 1/68 (1.4) | 6.00 (0) |
| Swelling | 1/68 (1.4) | 7.00 (0) |
| Physical factors | 35/190 (18.4) | 7.43 (1.45) |
| Muscle strength | 22/35 (62.8) | 7.50 (1.59) |
| Stiffness | 8/35 (22.9) | 7.00 (0.50) |
| Range of motion | 5/35 (14.3) | 7.80 (0.64) |
| Characteristics | nOP ≥ 4 (0, 1, 2, and 3 vs. 4 and 5) | ||
|---|---|---|---|
| Crude OR | 95% CI | p-Value | |
| Age | 1.011 | 0.995–1.027 | 0.195 |
| Sex (females) | 0.352 | 0.033–3.701 | 0.384 |
| STAI-X-1 | 0.867 | 0.756–0.994 | 0.041 * |
| PEDI-CAT Daily Activities | 1.063 | 0.970–1.165 | 0.193 |
| PEDI-CAT Mobility | 1.075 | 0.953–1.213 | 0.239 |
| PEDI-CAT Cognitive/Social | 1.063 | 0.949–1.189 | 0.291 |
| PEDI-CAT Responsibility | 1.063 | 0.970–1.165 | 0.193 |
| PRISM III | 0.920 | 0.772–1.096 | 0.350 |
| FSS | 0.944 | 0.775–1.149 | 0.566 |
| Ventilator use, yes | 1.467 | 0.186–11.587 | 0.716 |
| Previous PICU admission, yes | N/A | ||
| Cardiovascular, yes | 8.251 | 0.898–75.791 | 0.062 |
| Hematology and oncology, yes | N/A | ||
| Neurologic, yes | N/A | ||
| Sepsis, yes | N/A | ||
| Respiratory, yes | 1.643 | 0.207–13.013 | 0.638 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, Y.; Kwon, J.-Y.; Cho, J.; Choi, J. Individualized Goal Setting for Pediatric Intensive Care Unit-Based Rehabilitation Using the Canadian Occupational Performance Measure. Children 2023, 10, 985. https://doi.org/10.3390/children10060985
Hwang Y, Kwon J-Y, Cho J, Choi J. Individualized Goal Setting for Pediatric Intensive Care Unit-Based Rehabilitation Using the Canadian Occupational Performance Measure. Children. 2023; 10(6):985. https://doi.org/10.3390/children10060985
Chicago/Turabian StyleHwang, Youngsub, Jeong-Yi Kwon, Joongbum Cho, and Jaeyoung Choi. 2023. "Individualized Goal Setting for Pediatric Intensive Care Unit-Based Rehabilitation Using the Canadian Occupational Performance Measure" Children 10, no. 6: 985. https://doi.org/10.3390/children10060985