
Trends and Predictors of Pediatric Negative Appendectomy Rates: A Single-Centre Retrospective Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Outcomes of the Study
2.3. Data Collection and Study Design
2.4. Statistical Analysis
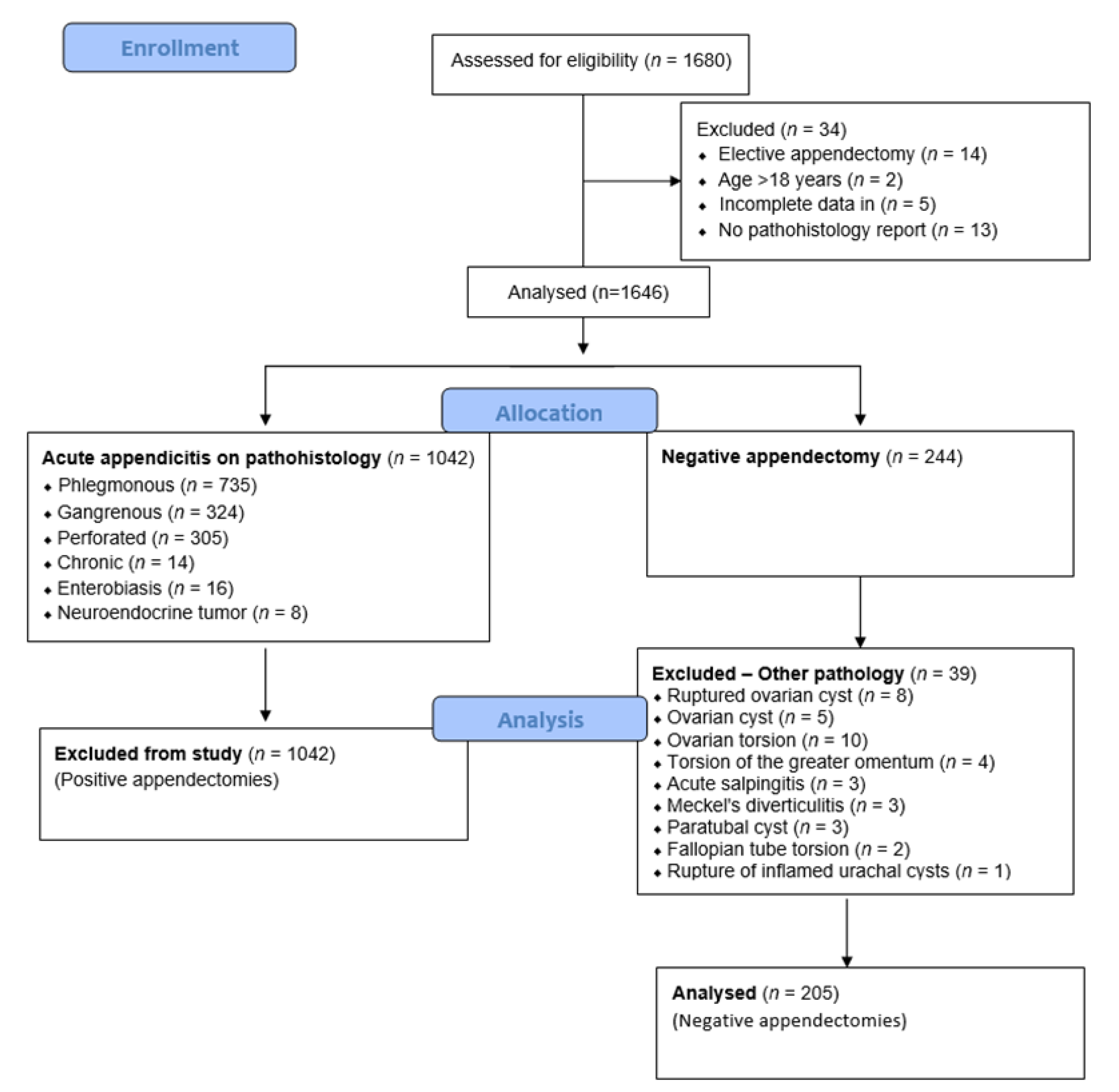
3. Results
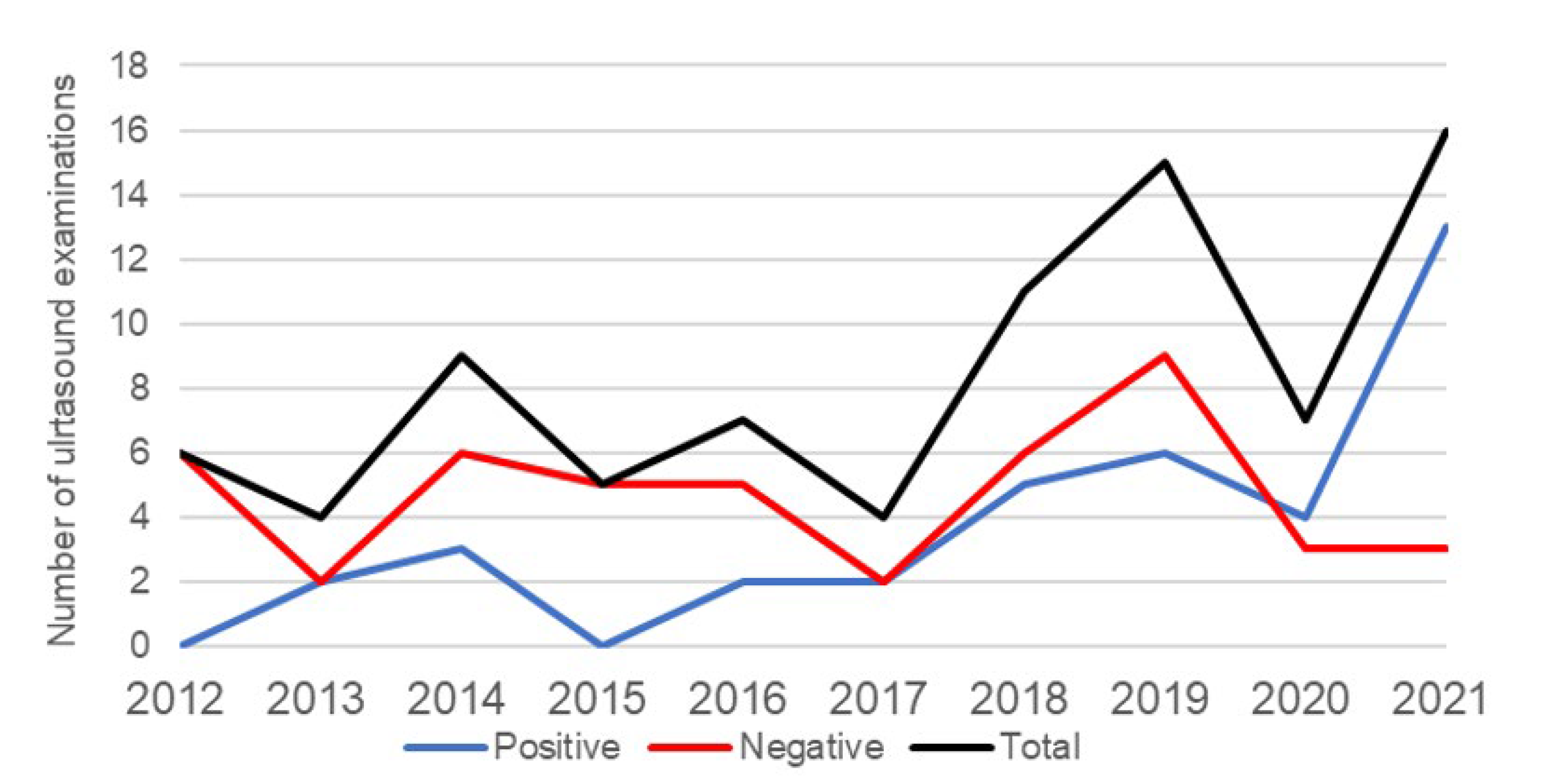
3.1. An Incidence of Negative Appendectomies
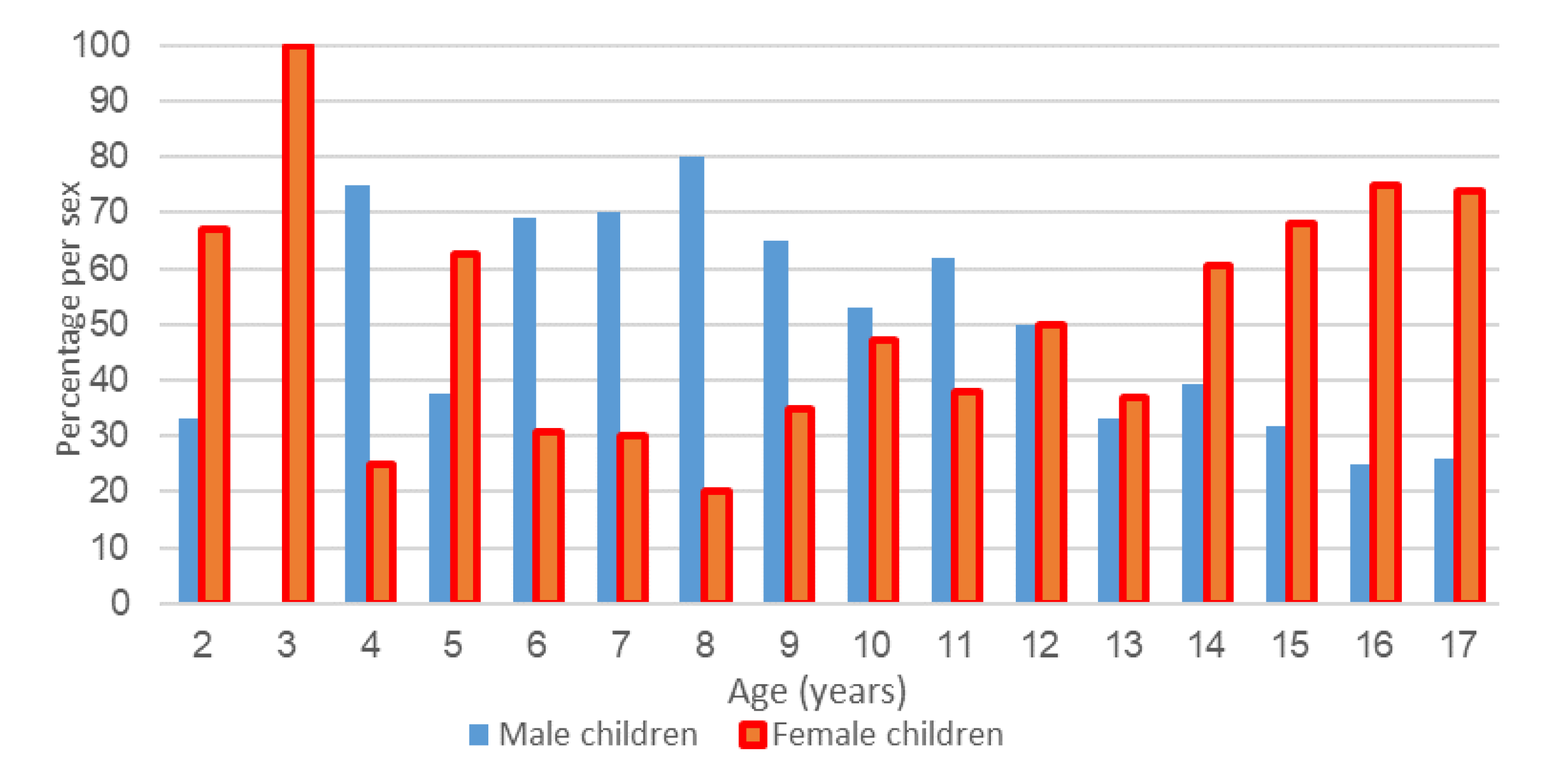
3.2. Analysis of Pathohistological Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pogorelić, Z.; Čohadžić, T. A bizarre cause of acute appendicitis in a pediatric patient: An ingested tooth. Children 2023, 10, 108. [Google Scholar] [CrossRef] [PubMed]
- Wickramasinghe, D.P.; Xavier, C.; Samarasekera, D.N. The world wide epidemiology of acute appendicitis: An analysis of the Global Health Data Exchange dataset. World J. Surg. 2021, 45, 1999–2008. [Google Scholar] [CrossRef] [PubMed]
- Hansen, G.L.; Kleif, J.; Jakobsen, C.; Paerregaard, A. Changes in Incidence and Management of Acute Appendicitis in Children—A Population-Based Study in the Period 2000–2015. Eur. J. Pediatr. Surg. 2021, 31, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Ferris, M.; Quan, S.; Kaplan, B.S.; Molodecky, N.; Ball, C.G.; Chernoff, G.W.; Bhala, N.; Ghosh, S.; Dixon, E.; Ng, S.; et al. The global incidence of appendicitis: A systematic review of population-based studies. Ann. Surg. 2017, 266, 237–241. [Google Scholar] [CrossRef]
- Feng, W.; Zhao, X.F.; Li, M.M.; Cui, H.L. A clinical prediction model for complicated appendicitis in children younger than five years of age. BMC Pediatr. 2020, 20, 401. [Google Scholar] [CrossRef]
- Jukić, M.; Tesch, A.; Todorić, J.; Šušnjar, T.; Milunović, K.P.; Barić, T.; Pogorelić, Z. Same-day discharge after laparoscopic appendectomy for simple appendicitis in pediatric patients-is it possible? Children 2022, 9, 1220. [Google Scholar] [CrossRef]
- Andersson, R.E. Meta-analysis of the clinical and laboratory diagnosis of appendicitis. Br. J. Surg. 2004, 91, 28–37. [Google Scholar] [CrossRef]
- Oztan, M.O.; Aksoy Gokmen, A.; Ozdemir, T.; Müderris, T.; Kaya, S.; Koyluoglu, G. Pentraxin-3: A strong novel biochemical marker for appendicitis in children. Am. J. Emerg. Med. 2019, 37, 1912–1916. [Google Scholar] [CrossRef]
- Arredondo Montero, J.; Antona, G.; Bardají Pascual, C.; Bronte Anaut, M.; Ros Briones, R.; Fernández-Celis, A.; Rivero Marcotegui, A.; López-Andrés, N.; Martín-Calvo, N. Serum neutrophil gelatinase-associated lipocalin (NGAL) as a diagnostic tool in pediatric acute appendicitis: A prospective validation study. Pediatr. Surg. Int. 2022, 38, 1569–1576. [Google Scholar] [CrossRef]
- Arredondo Montero, J.; Bardají Pascual, C.; Bronte Anaut, M.; López-Andrés, N.; Antona, G.; Martín-Calvo, N. Diagnostic performance of serum interleukin-6 in pediatric acute appendicitis: A systematic review. World J. Pediatr. 2022, 18, 91–99. [Google Scholar] [CrossRef]
- Wu, Z.; Zhao, L.; Feng, S.; Luo, J. Hyperfibrinogenemia and hyponatremia as predictors of perforated appendicitis in children: A retrospective cohort study. Int. J. Colorectal Dis. 2023, 38, 72. [Google Scholar] [CrossRef] [PubMed]
- Kakar, M.; Delorme, M.; Broks, R.; Asare, L.; Butnere, M.; Reinis, A.; Engelis, A.; Kroica, J.; Saxena, A.; Petersons, A. Deter-mining acute complicated and uncomplicated appendicitis using serum and urine biomarkers: Interleukin-6 and neutrophil gelatinase-associated lipocalin. Pediatr. Surg. Int. 2020, 36, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Tintor, G.; Jukić, M.; Šupe-Domić, D.; Jerončić, A.; Pogorelić, Z. Diagnostic utility of serum leucine-rich α-2-glycoprotein 1 for acute appendicitis in children. J. Clin. Med. 2023, 12, 2455. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Lukšić, A.M.; Mihanović, J.; Đikić, D.; Balta, V. Hyperbilirubinemia as an Indicator of Perforated Acute Appendicitis in Pediatric Population: A Prospective Study. Surg. Infect. 2021, 22, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.; Krishnan, N.; Birley, J.R.; Tintor, G.; Bajpai, M.; Pogorelić, Z. Hyponatremia-a new diagnostic marker for complicated acute appendicitis in children: A systematic review and meta-analysis. Children 2022, 9, 1070. [Google Scholar] [CrossRef]
- Tintor, G.; Jukić, M.; Šupe-Domić, D.; Jerončić, A.; Pogorelić, Z. Diagnostic accuracy of leucine-rich α-2-glycoprotein 1 as a non-invasive salivary biomarker in pediatric appendicitis. Int. J. Mol. Sci. 2023, 24, 6043. [Google Scholar] [CrossRef]
- Gorter, R.R.; Eker, H.H.; Gorter-Stam, M.A.; Abis, G.S.; Acharya, A.; Ankersmit, M.; Antoniou, S.A.; Arolfo, S.; Babic, B.; Boni, L.; et al. Diagnosis and management of acute appendicitis. EAES consensus development conference 2015. Surg. Endosc. 2016, 30, 4668–4690. [Google Scholar] [CrossRef]
- Kaselas, C.; Florou, M.; Demiri, C.; Tsopozidi, M.; Anastasiadis, K.; Spyridakis, I. Classification systems of acute appendicitis as an indicator for paediatric surgical consultation of children with acute abdominal pain. J. Paediatr. Child. Health 2023, 59, 360–364. [Google Scholar] [CrossRef]
- Andersson, R.E. The appendicitis inflammatory response score: A tool for the diagnosis of acute appendicitis that outperforms the Alvarado score. World J. Surg. 2008, 32, 1843–1849. [Google Scholar] [CrossRef]
- Sartelli, M.; Baiocchi, G.L.; Di Saverio, S.; Ferrara, F.; Labricciosa, F.M.; Ansaloni, L.; Coccolini, F.; Vijayan, D.; Abbas, A.; Abongwa, H.K.; et al. Prospective Observational Study on acute Appendicitis Worldwide (POSAW). World J. Emerg. Surg. 2018, 13, 19. [Google Scholar] [CrossRef]
- Gudjonsdottir, J.; Marklund, E.; Hagander, L.; Salö, M. Clinical prediction scores for pediatric appendicitis. Eur. J. Pediatr. Surg. 2021, 31, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Kharbanda, A.B.; Vazquez-Benitez, G.; Ballard, D.W.; Vinson, D.R.; Chettipally, U.K.; Kene, M.V.; Dehmer, S.P.; Bachur, R.G.; Dayan, P.S.; Kuppermann, N.; et al. Development and validation of a novel pediatric appendicitis risk calculator (pARC). Pediatrics 2018, 141, e20172699. [Google Scholar] [CrossRef] [PubMed]
- Pogorelić, Z.; Mihanović, J.; Ninčević, S.; Lukšić, B.; Elezović Baloević, S.; Polašek, O. Validity of appendicitis inflammatory response score in distinguishing perforated from non-perforated appendicitis in children. Children 2021, 19, 309. [Google Scholar] [CrossRef]
- Bhangu, A.; Søreide, K.; Di Saverio, S.; Assarsson, J.H.; Drake, F.T. Acute appendicitis: Modern understanding of pathogenesis, diagnosis, and management. Lancet 2015, 386, 1278–1287. [Google Scholar] [CrossRef] [PubMed]
- Carr, N.J. The pathology of acute appendicitis. Ann. Diagn. Pathol. 2000, 4, 46–58. [Google Scholar] [CrossRef]
- Maloney, C.; Edelman, M.C.; Bolognese, A.C.; Lipskar, A.M.; Rich, B.S. The impact of pathological criteria on pediatric negative appendectomy rate. J. Pediatr. Surg. 2019, 54, 1794–1799. [Google Scholar] [CrossRef]
- Oyetunji, T.A.; Ong’uti, S.K.; Bolorunduro, O.B.; Cornwell, E.E., 3rd; Nwomeh, B.C. Pediatric negative appendectomy rate: Trend, predictors, and differentials. J. Surg. Res. 2012, 173, 16–20. [Google Scholar] [CrossRef]
- Charfi, S.; Sellami, A.; Affes, A.; Yaïch, K.; Mzali, R.; Boudawara, T.S. Histopathological findings in appendectomy specimens: A study of 24,697 cases. Int. J. Colorectal Dis. 2014, 29, 1009–1012. [Google Scholar] [CrossRef]
- Tiboni, S.; Bhangu, A.; Hall, N.J. Paediatric Surgery Trainees Research Network and the National Surgical Research Collaborative. Outcome of appendicectomy in children performed in paediatric surgery units compared with general surgery units. Br. J. Surg. 2014, 101, 707–714. [Google Scholar] [CrossRef]
- Mariadason, J.G.; Wang, W.N.; Wallack, M.K.; Belmonte, A.; Matari, H. Negative appendicectomy rate as a quality metric in the management of appendicitis: Impact of computed tomography, Alvarado score and the definition of negative appendicectomy. Ann. R. Coll. Surg. Engl. 2012, 94, 395–401. [Google Scholar] [CrossRef]
- Augustin, G.; Čižmešija, Z.; Žedelj, J.; Petrović, I.; Ivković, V.; Antabak, A.; Mijatović, D.; Škegro, M. Laparoscopic appendectomy does not increase the rate of negative appendectomy along with a lower rate of perforated appendicitis—Results in 1899 patients at Zagreb UHC. Acta Clin. Croat. 2018, 57, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Newman, K.; Ponsky, T.; Kittle, K.; Dyk, L.; Throop, C.; Gieseker, K.; Sills, M.; Gilbert, J. Appendicitis 2000: Variability in practice, outcomes, and resource utilization at thirty pediatric hospitals. J. Pediatr. Surg. 2003, 38, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Ponsky, T.A.; Huang, Z.J.; Kittle, K.; Eichelberger, M.R.; Gilbert, J.C.; Brody, F.; Newman, K.D. Hospital- and patient-level characteristics and the risk of appendiceal rupture and negative appendectomy in children. JAMA 2004, 292, 1977–1982. [Google Scholar] [CrossRef] [PubMed]
- Bachur, R.G.; Hennelly, K.; Callahan, M.J.; Chen, C.; Monuteaux, M.C. Diagnostic imaging and negative appendectomy rates in children: Effects of age and gender. Pediatrics 2012, 129, 877–884. [Google Scholar] [CrossRef]
- Bijnen, C.L.; Van Den Broek, W.T.; Bijnen, A.B.; De Ruiter, P.; Gouma, D.J. Implications of removing a normal appendix. Dig. Surg. 2003, 20, 115–121. [Google Scholar] [CrossRef]
- O’sullivan, D.; Abd Elwahab, S.; Sharkey, C.; Kavanagh, E.; Browne, L.; Lowery, A.; Merrigan, A.; Tormey, S. Negative paediatric appendicectomy rates. Ir. Med. J. 2020, 113, 177. [Google Scholar]
- Jeon, B.G. Predictive factors and outcomes of negative appendectomy. Am. J. Surg. 2017, 213, 731–738. [Google Scholar] [CrossRef]
- Bates, M.F.; Khander, A.; Steigman, S.A.; Tracy TFJr Luks, F.I. Use of white blood cell count and negative appendectomy rate. Pediatrics 2014, 133, e39–e44. [Google Scholar] [CrossRef]
- Chiang, J.J.; Angus, M.I.; Nah, S.A.; Jacobsen, A.S.; Low, Y.; Choo, C.S.; Yap, T.L.; Chen, Y. Time course response of inflammatory markers in pediatric appendicitis. Pediatr. Surg. Int. 2020, 36, 493–500. [Google Scholar] [CrossRef]
- Kaiser, S.; Mesas-Burgos, C.; Söderman, E.; Frenckner, B. Appendicitis in children—Impact of US and CT on the negative appendectomy rate. Eur. J. Pediatr. Surg. 2004, 14, 260–264. [Google Scholar] [CrossRef]
- Arredondo Montero, J.; Bardají Pascual, C.; Bronte Anaut, M.; Antona, G.; López-Andrés, N.; Martín-Calvo, N. Coagulation Profile: Alterations and Diagnostic Yield in Pediatric Acute Appendicitis: A Prospective Validation Study. Surg. Infect. 2023, 24, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Addiss, D.G.; Shaffer, N.; Fowler, B.S.; Tauxe, R.V. The epidemiology of appendicitis and appendectomy in the United States. Am. J. Epidemiol. 1990, 132, 910–925. [Google Scholar] [CrossRef] [PubMed]
- Pogorelić, Z.; Anand, S.; Žuvela, T.; Singh, A.; Križanac, Z.; Krishnan, N. Incidence of complicated appendicitis during the COVID-19 pandemic versus the pre-pandemic period: A systematic review and meta-analysis of 2782 pediatric appendectomies. Diagnostics 2022, 12, 127. [Google Scholar] [CrossRef] [PubMed]
- Azadbakht, M.; Azadbakht, S.; Daniali, S.; Dehghani, M. Comparison of the prevalence of perforated appendicitis during and before COVID19 pandemic. Ann. Med. Surg. 2022, 82, 104785. [Google Scholar] [CrossRef] [PubMed]
- Kariya, A.; Krutsri, C.; Singhatas, P.; Sumritpradit, P.; Thampongsa, T.; Lertsitthichai, P.; Phoprom, N. Incidence of complicated appendicitis during the COVID-19 pandemic: A systematic review and meta-analysis. Int. J. Surg. Open 2022, 45, 100512. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Year | Appendectomies | p * | |
|---|---|---|---|
| Total (n = 1646) | Negative (n = 205) | ||
| 2012 | 178 | 26 (12.7) | 0.455 |
| 2013 | 174 | 19 (9.3) | |
| 2014 | 181 | 27 (13.2) | |
| 2015 | 176 | 14 (6.8) | |
| 2016 | 149 | 27 (13.2) | |
| 2017 | 165 | 21 (10.2) | |
| 2018 | 164 | 22 (10.7) | |
| 2019 | 172 | 16 (7.8) | |
| 2020 | 143 | 15 (7.3) | |
| 2021 | 144 | 18 (8.8) | |
| Parameter | Value |
|---|---|
| Demographic characteristics | |
| Age (years) | 12 (9, 15) |
| Gender | |
| Male | 97 (47.3) |
| Female | 108 (52.7) |
| BMI percentile range | 75.4 (41.8, 95.6) |
| Laboratory parameters | |
| Leukocytes (×109/L) | 10.4 (7.9, 14) |
| Neutrophils (%) | 75.9 (65.5, 83) |
| CRP (mg/L) | 11 (1.7, 44.8) |
| Diagnostic scores | |
| Alvarado score | 6 (4, 7.5) |
| AIR score | 5 (4, 7) |
| Abdominal ultrasound | |
| Positive (n = 84) | 37 (44) |
| Negative (n = 84) | 47 (56) |
| Parameter | 2012–2016 (n = 107) | 2017–2022 (n = 98) | p |
|---|---|---|---|
| Age (years) | 13 (9, 15) | 11 (8.3, 14) | 0.144 † |
| Male | 56 (52.3) | 41 (41.8) | 0.729 * |
| BMI percentile range | 78.1 (45.8, 97.3) | 71.7 (37, 94) | 0.120 † |
| Leukocytes (×109/L) | 10.6 (7.6, 14) | 10.1 (8.2, 14.2) | 0.830 † |
| Neutrophils (%) | 76 (63.6, 84) | 75.6 (66.9, 82.6) | 0.733 † |
| CRP (mg/L) | 13.2 (1.7, 46.6) | 8.7 (1.2, 35) | 0.495 † |
| Alvarado score | 6 (4, 7) | 6 (4, 8) | 0.733 † |
| AIR score | 5 (4, 7) | 5 (4, 6) | 0.411 † |
| Positive abdominal US | 7 (22.6) | 30 (56.6) | <0.0001 * |
| Parameter | Male Children | Female Children | p † |
|---|---|---|---|
| Age (years) | 10.5 (8, 13.5) | 14 (10, 15.8) | <0.0001 |
| BMI percentile range | 86.8 (45.4, 98.0) | 64.7 (31.1, 89.4) | 0.0004 |
| Leukocytes (×109/L) | 11.4 (8.6, 14.5) | 9.9 (7.5, 13.2) | 0.118 |
| Neutrophils (%) | 79 (71.3, 86.9) | 73.2 (62.7, 89.5) | 0.062 |
| CRP (mg/L) | 17.1 (5.2, 55.3) | 6.2 (1.2, 33.2) | 0.138 |
| Alvarado score | 7 (4, 8) | 6 (4, 7) | 0.108 |
| AIR score | 5 (4, 7) | 5 (3, 6) | 0.038 |
| Season | Pathohistological Finding | p * | |
|---|---|---|---|
| Positive (n = 1402) | Negative (n = 244) | ||
| Winter | 310 (22.1) | 67 (27.4) | 0.042 |
| Spring | 322 (22.9) | 50 (20.5) | |
| Summer | 439 (31.3) | 59 (24.2) | |
| Autumn | 331 (23.7) | 68 (27.9) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jukić, M.; Nizeteo, P.; Matas, J.; Pogorelić, Z. Trends and Predictors of Pediatric Negative Appendectomy Rates: A Single-Centre Retrospective Study. Children 2023, 10, 887. https://doi.org/10.3390/children10050887
Jukić M, Nizeteo P, Matas J, Pogorelić Z. Trends and Predictors of Pediatric Negative Appendectomy Rates: A Single-Centre Retrospective Study. Children. 2023; 10(5):887. https://doi.org/10.3390/children10050887
Chicago/Turabian StyleJukić, Miro, Petra Nizeteo, Jakov Matas, and Zenon Pogorelić. 2023. "Trends and Predictors of Pediatric Negative Appendectomy Rates: A Single-Centre Retrospective Study" Children 10, no. 5: 887. https://doi.org/10.3390/children10050887