
Elevated Urinary Hepcidin Level and Hypoferremia in Infants with Febrile Urinary Tract Infection: A Prospective Cohort Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
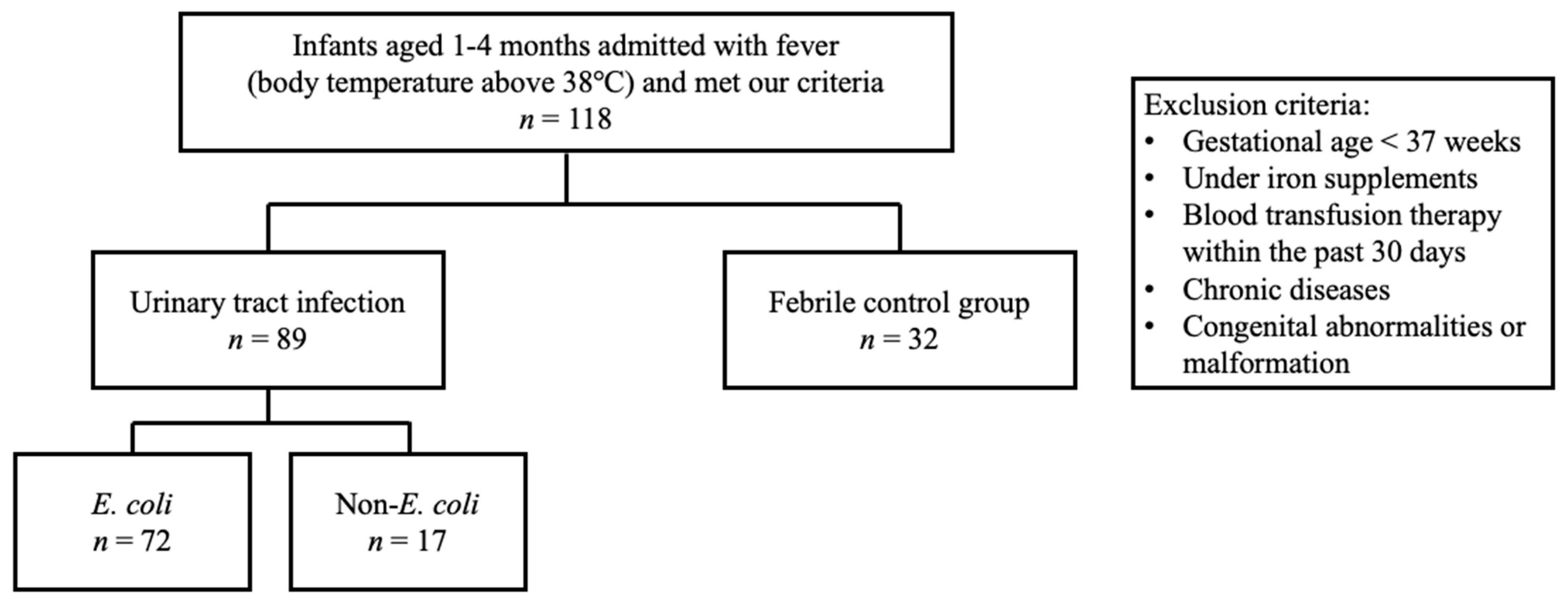
2.1. Patient Population
2.2. Laboratory Tests and Examinations
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Study Population
3.2. Analysis between the Febrile UTI and Febrile Control Groups
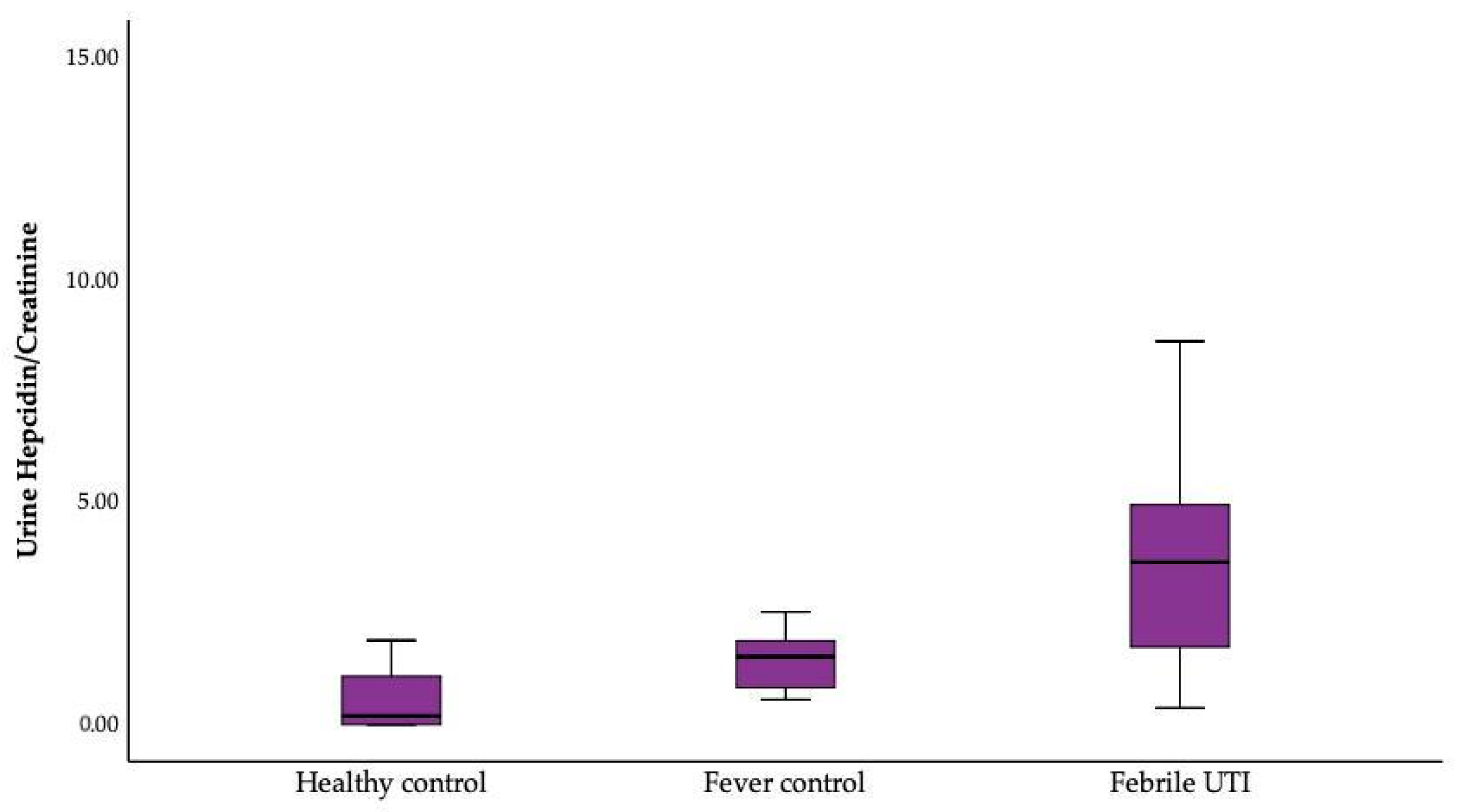
Analysis between the Healthy, Febrile Control, and Febrile UTI Groups
3.3. Analysis between the E. coli and Non-E. coli Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Park, C.H.; Valore, E.V.; Waring, A.J.; Ganz, T. Hepcidin, a urinary antimicrobial peptide synthesized in the liver. J. Biol. Chem. 2001, 276, 7806–7810. [Google Scholar] [CrossRef]
- Ganz, T.; Nemeth, E. Iron homeostasis in host defence and inflammation. Nat. Rev. Immunol. 2015, 15, 500–510. [Google Scholar] [CrossRef]
- Kossiva, L.; Soldatou, A.; Gourgiotis, D.I.; Stamati, L.; Tsentidis, C. Serum hepcidin: Indication of its role as an “acute phase” marker in febrile children. Ital. J. Pediatr. 2013, 39, 25. [Google Scholar] [CrossRef]
- Robinson, J.L.; Finlay, J.C.; Lang, M.E.; Bortolussi, R. Urinary tract infections in infants and children: Diagnosis and management. Paediatr. Child. Health 2014, 19, 315–325. [Google Scholar] [CrossRef]
- Mattoo, T.K.; Shaikh, N.; Nelson, C.P. Contemporary Management of Urinary Tract Infection in Children. Pediatrics 2021, 147, e2020012138. [Google Scholar] [CrossRef]
- National Collaborating Centre for Women’s and Children’s Health. Urinary Tract Infection in Children: Diagnosis, Treatment and Long-Term Management; National Collaborating Centre for Women’s and Children’s Health: London, UK; RCOG Press: London, UK, 2007. [Google Scholar]
- Williams, G.J.; Macaskill, P.; Chan, S.F.; Turner, R.M.; Hodson, E.; Craig, J.C. Absolute and relative accuracy of rapid urine tests for urinary tract infection in children: A meta-analysis. Lancet Infect. Dis. 2010, 10, 240–250. [Google Scholar] [CrossRef]
- Shaikh, N.; Shope, T.R.; Hoberman, A.; Vigliotti, A.; Kurs-Lasky, M.; Martin, J.M. Association Between Uropathogen and Pyuria. Pediatrics 2016, 138, e20160087. [Google Scholar] [CrossRef]
- Chaudhari, P.P.; Monuteaux, M.C.; Bachur, R.G. Should the Absence of Urinary Nitrite Influence Empiric Antibiotics for Urinary Tract Infection in Young Children? Pediatr. Emerg. Care 2020, 36, 481–485. [Google Scholar] [CrossRef]
- Flo, T.H.; Smith, K.D.; Sato, S.; Rodriguez, D.J.; Holmes, M.A.; Strong, R.K.; Akira, S.; Aderem, A. Lipocalin 2 mediates an innate immune response to bacterial infection by sequestrating iron. Nature 2004, 432, 917–921. [Google Scholar] [CrossRef]
- Goetz, D.H.; Holmes, M.A.; Borregaard, N.; Bluhm, M.E.; Raymond, K.N.; Strong, R.K. The neutrophil lipocalin NGAL is a bacteriostatic agent that interferes with siderophore-mediated iron acquisition. Mol. Cell 2002, 10, 1033–1043. [Google Scholar] [CrossRef]
- Zasloff, M. Antimicrobial peptides, innate immunity, and the normally sterile urinary tract. J. Am. Soc. Nephrol. 2007, 18, 2810–2816. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.; Lucy, M.; Krokhin, O.; Hayglass, K.; Pascoe, E.; Darroch, G.; Rush, D.; Nickerson, P.; Rigatto, C.; Reslerova, M. Mass spectrometry-based proteomic analysis of urine in acute kidney injury following cardiopulmonary bypass: A nested case-control study. Am. J. Kidney Dis. 2009, 53, 584–595. [Google Scholar] [CrossRef]
- Ho, J.; Reslerova, M.; Gali, B.; Gao, A.; Bestland, J.; Rush, D.N.; Nickerson, P.W.; Rigatto, C. Urinary hepcidin-25 and risk of acute kidney injury following cardiopulmonary bypass. Clin. J. Am. Soc. Nephrol. 2011, 6, 2340–2346. [Google Scholar] [CrossRef] [PubMed]
- Edlin, R.S.; Shapiro, D.J.; Hersh, A.L.; Copp, H.L. Antibiotic resistance patterns of outpatient pediatric urinary tract infections. J. Urol. 2013, 190, 222–227. [Google Scholar] [CrossRef]
- Houamel, D.; Ducrot, N.; Lefebvre, T.; Daher, R.; Moulouel, B.; Sari, M.A.; Letteron, P.; Lyoumi, S.; Millot, S.; Tourret, J.; et al. Hepcidin as a Major Component of Renal Antibacterial Defenses against Uropathogenic Escherichia coli. J. Am. Soc. Nephrol. 2016, 27, 835–846. [Google Scholar] [CrossRef]
- Sdogou, T.; Tsentidis, C.; Gourgiotis, D.; Marmarinos, A.; Gkourogianni, A.; Papassotiriou, I.; Anastasiou, T.; Kossiva, L. Immunoassay-based serum hepcidin reference range measurements in healthy children: Differences among age groups. J. Clin. Lab. Anal. 2015, 29, 10–14. [Google Scholar] [CrossRef]
- Aranda, N.; Bedmar, C.; Arija, V.; Jardí, C.; Jimenez-Feijoo, R.; Ferré, N.; Tous, M. Serum hepcidin levels, iron status, and HFE gene alterations during the first year of life in healthy Spanish infants. Ann. Hematol. 2018, 97, 1071–1080. [Google Scholar] [CrossRef]
- Bonadio, W.; Maida, G. Urinary tract infection in outpatient febrile infants younger than 30 days of age: A 10-year evaluation. Pediatr. Infect. Dis. J. 2014, 33, 342–344. [Google Scholar] [CrossRef]
- Goldman, M.; Lahat, E.; Strauss, S.; Reisler, G.; Livne, A.; Gordin, L.; Aladjem, M. Imaging after urinary tract infection in male neonates. Pediatrics 2000, 105, 1232–1235. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K.B. Urinary tract infection: Clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics 2011, 128, 595–610. [Google Scholar] [CrossRef] [PubMed]
- Ganz, T. Anemia of Inflammation. N. Engl. J. Med. 2019, 381, 1148–1157. [Google Scholar] [CrossRef] [PubMed]
- Nemeth, E.; Rivera, S.; Gabayan, V.; Keller, C.; Taudorf, S.; Pedersen, B.K.; Ganz, T. IL-6 mediates hypoferremia of inflammation by inducing the synthesis of the iron regulatory hormone hepcidin. J. Clin. Investig. 2004, 113, 1271–1276. [Google Scholar] [CrossRef] [PubMed]
- Kuruvilla, D.J.; Widness, J.A.; Nalbant, D.; Schmidt, R.L.; Mock, D.M.; An, G.; Veng-Pedersen, P. Estimation of adult and neonatal RBC lifespans in anemic neonates using RBCs labeled at several discrete biotin densities. Pediatr. Res. 2017, 81, 905–910. [Google Scholar] [CrossRef] [PubMed]
- Van Eijk, L.T.; Kroot, J.J.; Tromp, M.; van der Hoeven, J.G.; Swinkels, D.W.; Pickkers, P. Inflammation-induced hepcidin-25 is associated with the development of anemia in septic patients: An observational study. Crit. Care 2011, 15, R9. [Google Scholar] [CrossRef] [PubMed]
- Guida, C.; Altamura, S.; Klein, F.A.; Galy, B.; Boutros, M.; Ulmer, A.J.; Hentze, M.W.; Muckenthaler, M.U. A novel inflammatory pathway mediating rapid hepcidin-independent hypoferremia. Blood 2015, 125, 2265–2275. [Google Scholar] [CrossRef]
- Kim, A.; Fung, E.; Parikh, S.G.; Valore, E.V.; Gabayan, V.; Nemeth, E.; Ganz, T. A mouse model of anemia of inflammation: Complex pathogenesis with partial dependence on hepcidin. Blood 2014, 123, 1129–1136. [Google Scholar] [CrossRef]
- Oppen, K.; Ueland, T.; Siljan, W.W.; Skadberg, Ø.; Brede, C.; Lauritzen, T.; Aukrust, P.; Steinsvik, T.; Husebye, E.; Michelsen, A.E.; et al. Hepcidin and Ferritin Predict Microbial Etiology in Community-Acquired Pneumonia. Open Forum Infect. Dis. 2021, 8, ofab082. [Google Scholar] [CrossRef]
- Kossiva, L.; Gourgiotis, D.I.; Tsentidis, C.; Anastasiou, T.; Marmarinos, A.; Vasilenko, H.; Sdogou, T.; Georgouli, H. Serum hepcidin and ferritin to iron ratio in evaluation of bacterial versus viral infections in children: A single-center study. Pediatr. Infect. Dis. J. 2012, 31, 795–798. [Google Scholar] [CrossRef]
- Yang, Y.L.; Kuo, H.C.; Chen, K.D.; Chu, C.H.; Kuo, K.C.; Guo, M.M.; Chang, L.S.; Huang, Y.H. Combination of Hemoglobin-for-Age Z-Score and Plasma Hepcidin Identified as a Novel Predictor for Kawasaki Disease. Children 2022, 9, 913. [Google Scholar] [CrossRef]
- Słomka, A.; Łęcka, M.; Styczyński, J. Hepcidin in Children and Adults with Acute Leukemia or Undergoing Hematopoietic Cell Transplantation: A Systematic Review. Cancers 2022, 14, 4936. [Google Scholar] [CrossRef]
- Gajewska, J.; Ambroszkiewicz, J.; Klemarczyk, W.; Głąb-Jabłońska, E.; Weker, H.; Chełchowska, M. Ferroportin-Hepcidin Axis in Prepubertal Obese Children with Sufficient Daily Iron Intake. Int. J. Environ. Res. Public Health 2018, 15, 2156. [Google Scholar] [CrossRef]
- Ferrucci, L.; Semba, R.D.; Guralnik, J.M.; Ershler, W.B.; Bandinelli, S.; Patel, K.V.; Sun, K.; Woodman, R.C.; Andrews, N.C.; Cotter, R.J.; et al. Proinflammatory state, hepcidin, and anemia in older persons. Blood 2010, 115, 3810–3816. [Google Scholar] [CrossRef]
- Semrin, G.; Fishman, D.S.; Bousvaros, A.; Zholudev, A.; Saunders, A.C.; Correia, C.E.; Nemeth, E.; Grand, R.J.; Weinstein, D.A. Impaired intestinal iron absorption in Crohn’s disease correlates with disease activity and markers of inflammation. Inflamm. Bowel Dis. 2006, 12, 1101–1106. [Google Scholar] [CrossRef] [PubMed]
- Ayoya, M.A.; Spiekermann-Brouwer, G.M.; Stoltzfus, R.J.; Nemeth, E.; Habicht, J.P.; Ganz, T.; Rawat, R.; Traoré, A.K.; Garza, C. Alpha 1-acid glycoprotein, hepcidin, C-reactive protein, and serum ferritin are correlated in anemic schoolchildren with Schistosoma haematobium. Am. J. Clin. Nutr. 2010, 91, 1784–1790. [Google Scholar] [CrossRef] [PubMed]
- Swinkels, D.W.; Girelli, D.; Laarakkers, C.; Kroot, J.; Campostrini, N.; Kemna, E.H.; Tjalsma, H. Advances in quantitative hepcidin measurements by time-of-flight mass spectrometry. PLoS ONE 2008, 3, e2706. [Google Scholar] [CrossRef]
- Kulaksiz, H.; Theilig, F.; Bachmann, S.; Gehrke, S.G.; Rost, D.; Janetzko, A.; Cetin, Y.; Stremmel, W. The iron-regulatory peptide hormone hepcidin: Expression and cellular localization in the mammalian kidney. J. Endocrinol. 2005, 184, 361–370. [Google Scholar] [CrossRef]
- Verga Falzacappa, M.V.; Muckenthaler, M.U. Hepcidin: Iron-hormone and anti-microbial peptide. Gene 2005, 364, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Maisetta, G.; Petruzzelli, R.; Brancatisano, F.L.; Esin, S.; Vitali, A.; Campa, M.; Batoni, G. Antimicrobial activity of human hepcidin 20 and 25 against clinically relevant bacterial strains: Effect of copper and acidic pH. Peptides 2010, 31, 1995–2002. [Google Scholar] [CrossRef]
- Jiang, X.F.; Liu, Z.F.; Lin, A.F.; Xiang, L.X.; Shao, J.Z. Coordination of Bactericidal and Iron Regulatory Functions of Hepcidin in Innate Antimicrobial Immunity in a Zeb.brafish Model. Sci. Rep. 2017, 7, 4265. [Google Scholar] [CrossRef]
- Polnay, L.; Fraser, A.M.; Lewis, J.M. Complication of suprapubic bladder aspiration. Arch. Dis. Child. 1975, 50, 80–81. [Google Scholar] [CrossRef]
- Hägglöf, B. Psychological reaction by children of various ages to hospital care and invasive procedures. Acta Paediatr Suppl. 1999, 88, 72–78. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Febrile UTI (n = 86) | Fever Control (n = 32) | p Value | |
|---|---|---|---|
| Age (day) | 75.03 ± 26.07 | 76.31 ± 20.43 | 0.779 |
| Sex (F/M) | 24/65 | 13/19 | 0.113 |
| Bacteremia (n, %) | 6, 7% | 0, 0% | 0.151 |
| Fever duration at admission (day) | 0.84 ± 0.69 | 0.78 ± 0.52 | 0.676 |
| Febrile UTI (n = 86) | Fever Control (n = 32) | p Value | Logistic Regression | ||||
|---|---|---|---|---|---|---|---|
| OR (95% C.I.) | p Value | ||||||
| Blood Laboratory | * p Value | * p Value | |||||
| WBC (1000/μL) | <0.001 | 0.24 | |||||
| Before | 14.61 ± 4.80 | 8.21 ± 3.05 | <0.001 | 1.46 (1.26–1.70) | <0.001 | ||
| After | 10.27 ± 3.66 | 8.96 ± 2.79 | 0.103 | 1.14 (0.98–1.33) | 0.093 | ||
| ANC (1000/μL) | <0.001 | <0.001 | |||||
| Before | 51.97 ± 13.19 | 40.64 ± 16.50 | <0.001 | 1.06 (1.03–1.09) | <0.001 | ||
| After | 23.64 ± 8.94 | 21.65 ± 12.18 | 0.373 | 1.02 (0.97–1.07) | 0.376 | ||
| RBC (million/μL) | 0.001 | 0.176 | |||||
| Before | 3.72 ± 0.57 | 3.70 ± 0.43 | 0.833 | 1.02 (0.47–2.22) | 0.955 | ||
| After | 3.64 ± 0.48 | 3.63 ± 0.46 | 0.917 | 0.99 (0.37–2.62) | 0.986 | ||
| Hb (g/dL) | <0.001 | 0.083 | |||||
| Before | 10.48 ± 1.23 | 10.53 ± 0.86 | 0.82 | 0.94 (0.66–1.33) | 0.717 | ||
| After | 10.10 ± 0.94 | 10.18 ± 0.91 | 0.704 | 0.88 (0.54–1.44) | 0.619 | ||
| MCV (fL) | <0.001 | 0.13 | |||||
| Before | 85.66 ± 7.30 | 85.96 ± 5.79 | 0.918 | 0.99 (0.94–1.06) | 0.968 | ||
| After | 83.16 ± 6.57 | 84.80 ± 4.90 | 0.26 | 0.96 (0.89–1.04) | 0.282 | ||
| CRP (mg/L) | <0.001 | 0.12 | |||||
| Before | 42.55 ± 40.80 | 5.36 ± 6.45 | <0.001 | 1.16 (1.08–1.25) | <0.001 | ||
| After | 12.63 ± 15.52 | 4.03 ± 4.28 | <0.001 | 1.17 (1.04–1.31) | 0.007 | ||
| Procalcitonin (ng/mL) | 0.998 | 0.51 | |||||
| Before | 1.88 ± 4.81 | 0.13 ± 0.09 | 0.008 | 3522.36 (10.73–1,156,353.46) | 0.006 | ||
| After | 2.83 ± 10.91 | 0.12 ± 0.09 | 0.23 | 53.65 (0.95–3028.83) | 0.053 | ||
| Fe (ng/mL) | 25.03 ± 9.72 | 48.55 ± 25.41 | <0.001 | 0.88 (0.82–0.94) | <0.001 | ||
| Ferritin (ng/mL) | 165.38 ± 99.98 | 233.70 ± 187.56 | 0.094 | 0.99 (0.99–1.00) | 0.114 | ||
| TIBC (ug/dL) | 294.58 ± 45.85 | 295.10 ± 50.67 | 0.968 | 1.00 (0.99–1.01) | 0.967 | ||
| Hepcidin (ng/mL) | 0.907 | 0.744 | |||||
| Before | 239.01 ± 41.23 | 229.0 ± 35.66 | 0.51 | 1.00 (0.99–1.03) | 0.495 | ||
| After | 242.65 ± 52.94 | 239.49 ± 60.37 | 0.893 | 1.00 (0.99–1.02) | 1.887 | ||
| Urinary laboratory | |||||||
| WBC (/μL) | 314.57 ± 145.09 | 4.69 ± 6.81 | <0.001 | 1.16 (1.063–1.261) | 0.001 | ||
| RBC (/μL) | 87.12 ± 178.57 | 1.22 ± 2.73 | 0.001 | 1.39 (1.174–1.652) | <0.001 | ||
| Creatinine (mg/dL) | 0.257 | 0.698 | |||||
| Before | 11.06 ± 8.18 | 12.92 ± 5.88 | 0.577 | 0.97 (0.88–1.08) | 0.566 | ||
| After | 11.61 ± 7.02 | 9.31 ± 6.21 | 0.436 | 1.06 (0.91–1.24) | 0.43 | ||
| Hepcidin/Creatinine | 0.009 | 0.259 | |||||
| Before | 11.06 ± 6.93 | 4.22 ± 2.26 | 0.016 | 2.01 (1.089–3.720) | 0.026 | ||
| After | 7.49 ± 4.41 | 3.73 ± 2.77 | 0.041 | 1.37 (0.997–1.886) | 0.052 | ||
| Urinary Tract Infection | p Value | Logistic Regression | |||||
|---|---|---|---|---|---|---|---|
| E. coli (n = 69) | Non-E. coli (n = 17) | OR (95% C.I.) | p Value | ||||
| Blood laboratory | * p value | * p value | |||||
| WBC (1000/μL) | <0.001 | 0.007 | |||||
| Before | 14.96 ± 4.50 | 13.09 ± 5.83 | 0.23 | 1.09 (0.97–1.22) | 0.147 | ||
| After | 10.22 ± 3.61 | 9.66 ± 3.15 | 0.464 | 1.07 (0.91–1.26) | 0.413 | ||
| ANC (1000/μL) | <0.001 | 0.001 | |||||
| Before | 52.11 ± 13.69 | 51.42 ± 11.14 | 0.846 | 1.00 (0.96–1.05) | 0.831 | ||
| After | 24.27 ± 8.75 | 21.79 ± 9.69 | 0.116 | 1.06 (0.99–1.13) | 0.121 | ||
| RBC (million/μL) | 0.005 | 0.083 | |||||
| Before | 3.76 ± 0.55 | 3.55 ± 0.65 | 0.175 | 1.98 (0.67–5.80) | 0.214 | ||
| After | 3.69 ± 0.45 | 3.43 ± 0.55 | 0.049 | 3.63 (0.919–14.347) | 0.066 | ||
| Hb (g/dL) | <0.001 | 0.04 | |||||
| Before | 10.54 ± 1.20 | 10.22 ± 1.47 | 0.339 | 1.23 (0.77–1.97) | 0.388 | ||
| After | 10.18 ± 0.96 | 9.73 ± 0.77 | 0.079 | 1.78 (0.90–3.53) | 0.1 | ||
| MCV (fL) | <0.001 | <0.001 | |||||
| Before | 85.37 ± 7.05 | 87.72 ± 7.79 | 0.229 | 0.96 (0.88–1.03) | 0.253 | ||
| After | 82.59 ± 6.28 | 85.58 ± 7.39 | 0.101 | 0.93 (0.84–1.02) | 0.114 | ||
| CRP (mg/L) | <0.001 | 0.001 | |||||
| Before | 42.14 ± 39.79 | 44.25 ± 46.09 | 0.85 | 1.00 (0.99–1.01) | 0.797 | ||
| After | 13.31 ± 15.99 | 9.72 ± 13.41 | 0.408 | 1.02 (0.97–1.07) | 0.418 | ||
| Procalcitonin (ng/mL) | 0.996 | 0.961 | |||||
| Before | 2.11 ± 5.36 | 1.03 ± 1.31 | 0.496 | 1.08 (0.87–1.34) | 0.5 | ||
| After | 3.02 ± 11.70 | 1.61 ± 2.89 | 0.815 | 1.02 (0.88–1.18) | 0.804 | ||
| Fe (ng/mL) | 23.41 ±7.86 | 34.00 ± 15.12 | 0.257 | 0.89 (0.79–1.00) | 0.068 | ||
| Ferritin (ng/mL) | 142.86 ± 67.96 | 289.23 ± 163.70 | 0.171 | 0.99 (0.97–0.99) | 0.032 | ||
| TIBC (ug/dL) | 287.18 ± 36.23 | 335.25 ± 75.66 | 0.295 | 0.98 (0.95–1.00) | 0.078 | ||
| Hepcidin (ng/mL) | 0.839 | 0.616 | |||||
| Before | 242.26 ± 43.34 | 219.5 ± 23.33 | 0.492 | 1.02 (0.97–1.06) | 0.463 | ||
| After | 248.14 ± 54.80 | 212.40 ± 37.90 | 0.403 | 1.02 (0.98–1.06) | 0.377 | ||
| Urinary laboratory | |||||||
| WBC (/μL) | 333.21 ± 180.24 | 235.65 ± 208.50 | 0.055 | 1.00 (1.00–1.00) | 0.065 | ||
| RBC (/μL) | 103.11 ± 156.74 | 19.41 ± 27.17 | <0.001 | 1.02 (0.997–1.036) | 0.09 | ||
| Creatinine (mg/dL) | 0.838 | 0.493 | |||||
| Before | 11.15 ± 8.69 | 10.52 ±5.10 | 0.89 | 1.01 (0.88–1.16) | 0.884 | ||
| After | 10.90 ± 6.12 | 15.68 ±11.25 | 0.215 | 0.92 (0.80–1.05) | 0.224 | ||
| Hepcidin/Creatinine | 0.03 | 0.102 | |||||
| Before | 11.17 ± 7.20 | 10.42 ± 5.89 | 0.847 | 1.02 (0.86–1.20) | 0.84 | ||
| After | 7.84 ± 4.66 | 5.46 ± 1.72 | 0.329 | 1.17 (0.86–1.61) | 0.322 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, Y.-C.; Huang, H.-C.; Tang, K.-S.; Su, L.-T.; Huang, Y.-H.; Huang, H.-C.; Chen, I.-L. Elevated Urinary Hepcidin Level and Hypoferremia in Infants with Febrile Urinary Tract Infection: A Prospective Cohort Study. Children 2023, 10, 870. https://doi.org/10.3390/children10050870
Hsu Y-C, Huang H-C, Tang K-S, Su L-T, Huang Y-H, Huang H-C, Chen I-L. Elevated Urinary Hepcidin Level and Hypoferremia in Infants with Febrile Urinary Tract Infection: A Prospective Cohort Study. Children. 2023; 10(5):870. https://doi.org/10.3390/children10050870
Chicago/Turabian StyleHsu, Yu-Chen, Hsin-Chun Huang, Kuo-Su Tang, Li-Ting Su, Ying-Hsien Huang, Hui-Chen Huang, and I-Lun Chen. 2023. "Elevated Urinary Hepcidin Level and Hypoferremia in Infants with Febrile Urinary Tract Infection: A Prospective Cohort Study" Children 10, no. 5: 870. https://doi.org/10.3390/children10050870